Article Text

Statistics from Altmetric.com
Angiotensin converting enzyme 2 (ACE2) is the primary receptor for the SARS-CoV-2 virus raising concern that patients with cardiovascular disease being treated with an ACE inhibitor or angiotensin receptor blocker (ARB) drug might have altered ACE2 expression leading to increased risk of COVID-19 infection or a more severe disease course. In this issue of Heart, Hippisley-Cox and colleagues1 addressed this question using routinely collected data in a prospective cohort study in England of 8.28 million participants aged 20–99 years. COVID-19 disease was diagnosed in 19 486 patients and 1286 required treatment in the intensive care unit (ICU). Even after adjustment for confounders, ACE inhibitors were associated with a significantly reduced risk of COVID-19 disease (adjusted HR 0.71, 95% CI 0.67 to 0.74) and no increased risk of ICU care (adjusted HR 0.89, 95% CI 0.75 to 1.06). Similarly, adjusted HRs for ARBs were 0.63 (95% CI 0.59 to 0.67) for COVID-19 disease and 1.02 (95% CI 0.83 to 1.25) for ICU care. However, there were significant interactions with ethnicity for ACE inhibitors and ARB (both p<0.001) for COVID-19 RT-PCR diagnosed disease outcome (table 1).
Adjusted HRs (95% CI) for risk of COVID-19 positive test associated with ACE inhibitor and ARB exposure by ethnic group
In the accompanying editorial, Straw and Witte2 point out that ‘Observational data are challenging to work with, requiring care to avoid the pitfalls of observed and hidden interactions and biases while balancing the need to make the results accessible to non-statisticians. The reliability of conclusions drawn from observational data depends on their interpretation and on the data themselves.’ However, given the rigorous approach in this study, they that this data ‘should reassure physicians and patients that these vital medications are not implicated in COVID-19 and should not be stopped.’ This study also underscores the principles ‘that the cardiovascular system is not the same across ethnicities, that good supportive care in the absence of specific therapies is essential and that the independent scientific process based on precise peer review must be protected, even when authors and editors are under immense pressure.’
Similarly, a meta-analysis of 10 studies enrolling 9890 hypertensive subjects found that the risk of severe or lethal COVID-19 was no increased in patients on treatment with an ACE inhibitor or ARB compared with patients not on these medications (for ACE inhibitors OR: 0.90; 95% CI 0.65 to 1.26; for ARBs OR 0.92; 95% CI 0.75 to 1.12).3
These two studies in Heart complement the randomised clinical trial (RCT) recently presented at the European Society of Cardiology Annual Scientific Sessions.In the Angiotensin Receptor Blockers and Angiotensin-converting Enzyme Inhibitors and Adverse Outcomes in Patients With COVID19 (BRACE-CORONA) trial,4 659 patients hospitalized with COVID-19 infection who were chronically on an ACE inhibitor or ARB were randomised to 30-days of suspension vs continuation of these medications. The mean age was relatively young (56 years) and 40% were women, with hypertension in 100% but heart failure in only 1.4%. Overall, thehe primary outcomeof days alive and out of the hospital at 30 days was no different in those suspending or contining ACE-inhibitor or ARB therapy. The congruence between this RCT and the publications in this issue of Heart shows the power of carefully performed and analyzed oberservational studies.
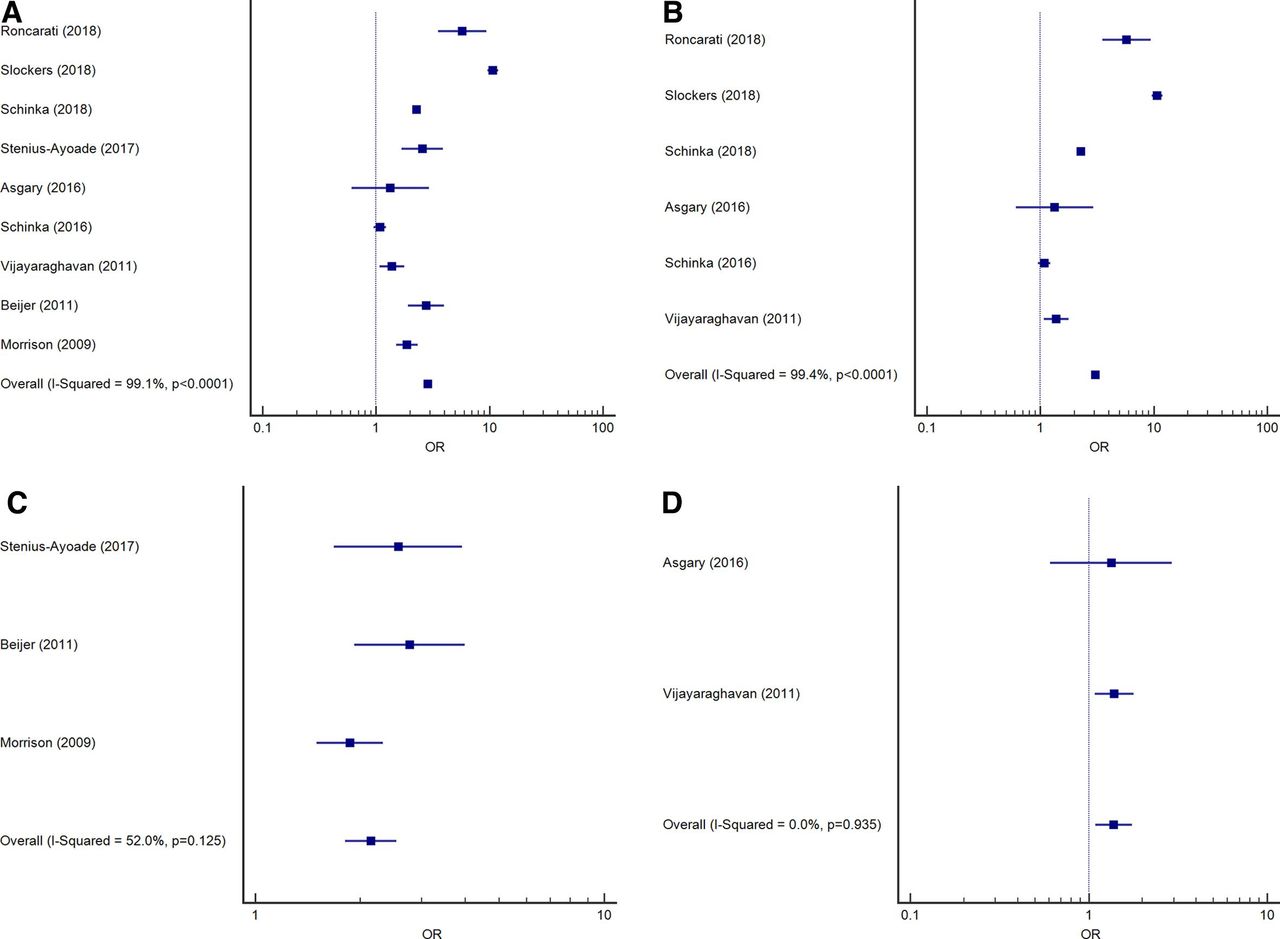
Homelessness is an often-underappreciated risk factor for cardiovascular disease (CVD). ‘Homelessness is a global crisis which has increased at an alarming rate over the last decade; worldwide it is estimated that nearly 1.6 billion people have inadequate shelter, resulting in the United Nations announcing its first-ever resolution on homelessness on 19 February 2020.’5 In a meta-analysis of 17 articles addressing both the risk of CVD and interventions for CVD in homeless populations, Al-Shakarchi and colleagues6 found an almost threefold increased risk of CVD in homeless individuals pooled (OR 2.96; 95% CI 2.80 to 3.13; p<0.0001) and a higher CVD mortality rate than non-homeless individuals(age-standardised mortality ratio range: 2.6–6.4) (figure 1).

Forest plots of ORs of cardiovascular disease (CVD) (International Classification of Diseases, Tenth Revision definition) in homeless versus housed individuals from (A) all studies in meta-analysis (n=9), (B) North American studies (n=6) and (C) European studies (n=3). (D) Forest plot of ORs of hypertension (a subset of CVD) (n=2).
As Lane concludes in her editorial,5 ‘We need to gain a better understanding of the magnitude and types of CVD among the homeless; the specific barriers to healthcare faced by homeless people; and identify effective models of care and adapt/tailor these into current CVD services and existing homeless services.’ ‘One important tangible difference healthcare professionals can implement immediately is to treat everyone with the same level of professionalism and compassion and not discriminate or stigmatise people who are homeless.’
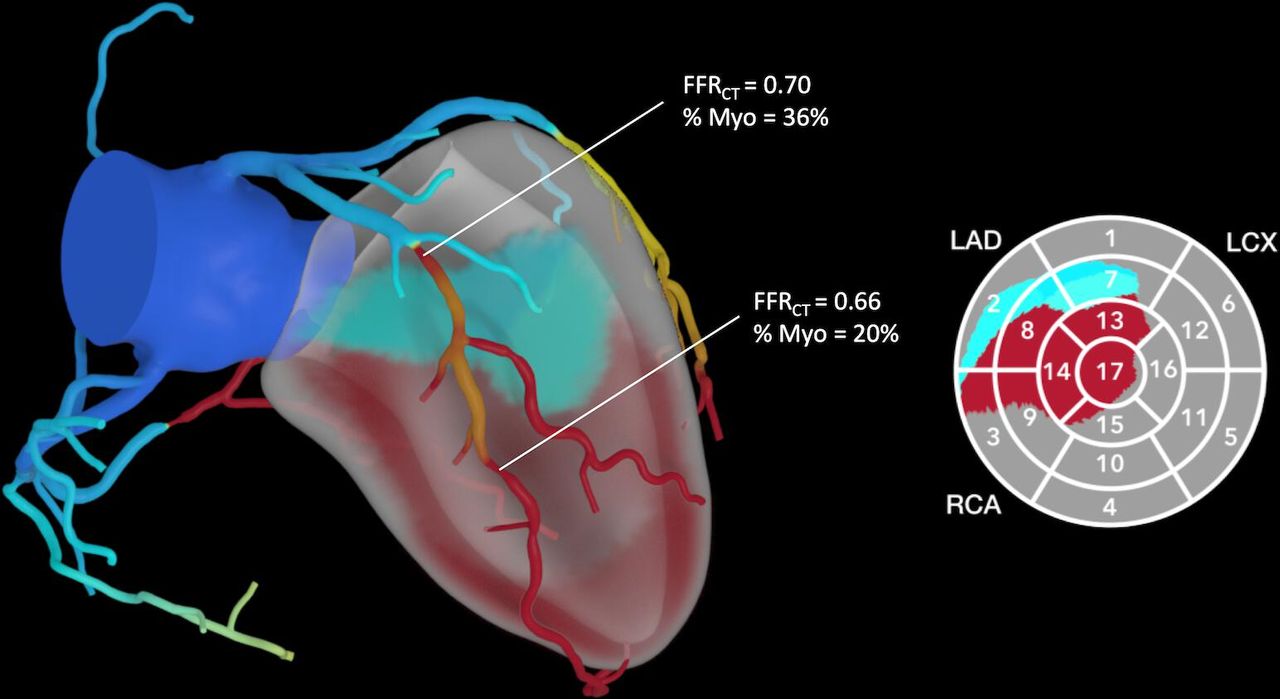
An interesting imaging study by Keulards and colleagues7 demonstrates that CT flow-based measurement of myocardial mass is closely related to invasively measured myocardial perfusion supporting the use of CT-mass for estimating the extent of myocardium-at-risk in patients with proximal coronary artery disease. The novelty of this approach is put into context by Ihdayhid and Sellers8 who discuss how fractional flow reserve measured by CT (FFRCT) techniques might allow us to ‘integrate both physiology and myocardium at risk into a single non-invasive test’ (figure 2).

Integrating fractional myocardial mass with FFRCT analysis. A conceptual image of how integrating FFRCT with myocardium at risk and myocardial blood flow could be applied in future iterations of CTCA analysis. CTCA, CT coronary angiography; FFR, fractional flow reserve; FFRCT, CT derived FFR; LAD, left anterior descending.
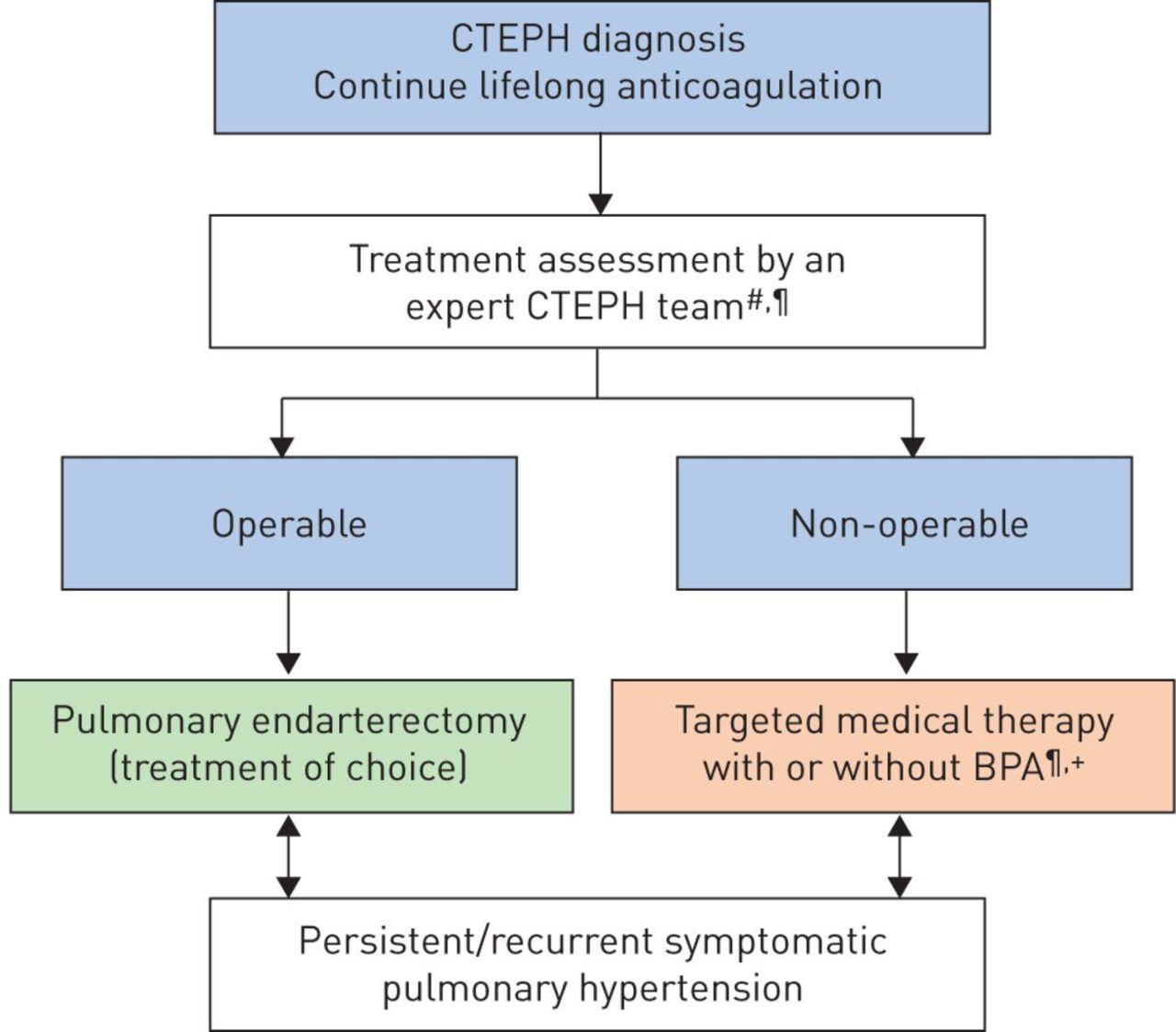
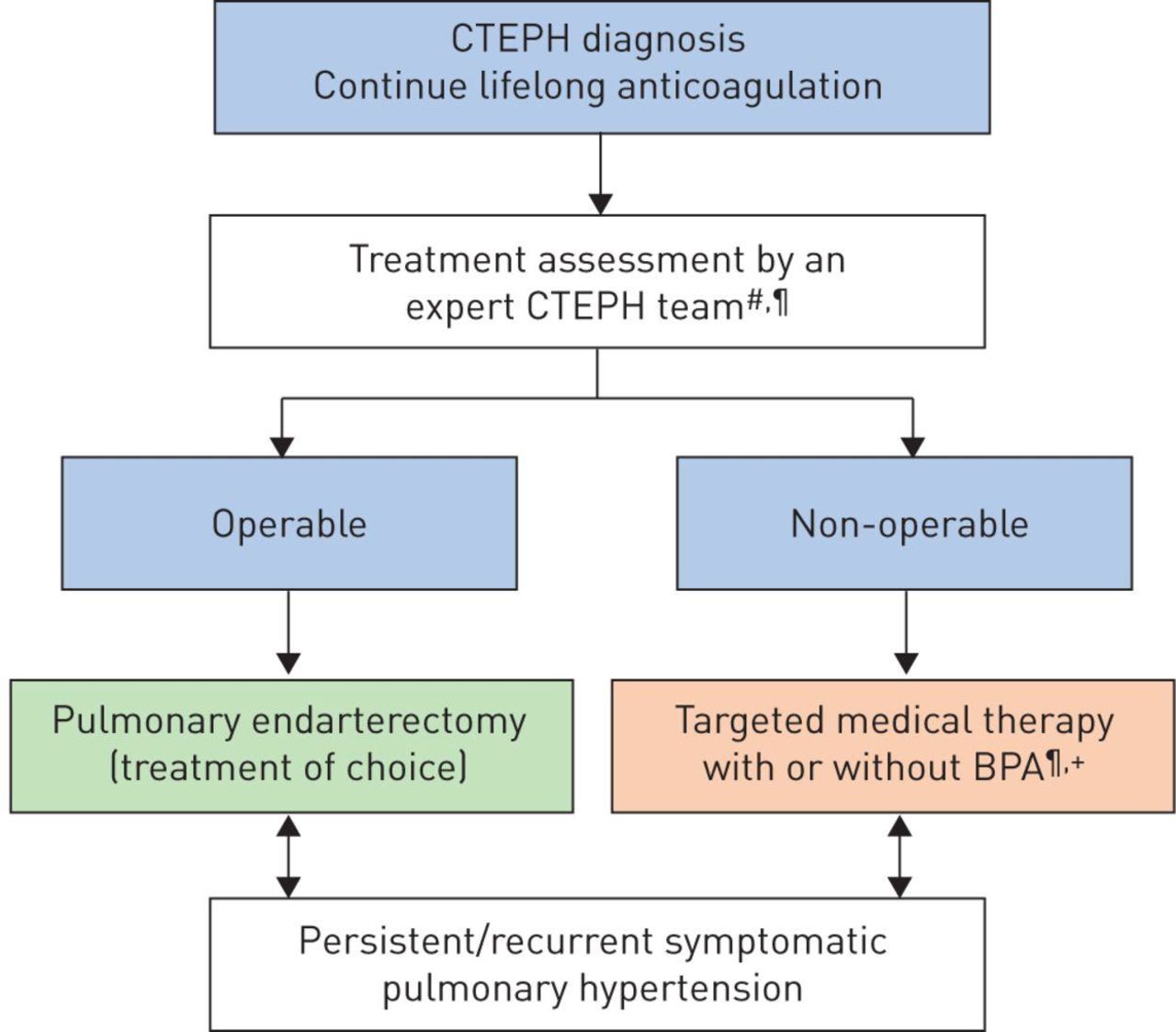
The Education in Heart article in this issue9 provides an overview of interventional approaches to treatment of chronic thromboembolic pulmonary hypertension (CTEPH), comparing surgical pulmonary endarterectomy (PEA) versus balloon pulmonary angioplasty (BPA) (figure 3). As they point out ‘BPA is now sufficiently developed that appropriately powered RCTs comparing PEA versus BPA for segmental and subsegmental (levels 3 and 4) CTEPH could be planned in centres with equivalent experience in both techniques. However, consensus in the interpretation of imaging and standardisation of the surgical and BPA approach between centres will be important to deliver meaningful comparisons.’
{kind=link}
{kind=link}
{kind=link}
Chronic thromboembolic pulmonary hypertension (CTEPH) treatment algorithm.10 #Multidisciplinary: pulmonary endarterectomy surgeon, pulmonary hypertension (PH) expert, BPA interventionist and radiologist. ¶Treatment assessment may differ depending on the level of expertise. +BPA without medical therapy can be considered in selected cases. BPA, balloon pulmonary angioplasty.
Footnotes
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Patient consent for publication Not required.
Provenance and peer review Commissioned; internally peer reviewed.