Article Text

Abstract
Introduction Sodium-glucose cotransporter 2 (SGLT2) inhibitors are known to reduce the risk of cardiovascular events in patients with type 2 diabetes (T2DM). The recent ground-breaking DAPA-HF trial has shown similar results in patients with heart failure with reduced ejection fraction (HFrEF) regardless of whether they have T2DM. Guidelines on their use in HFrEF patients are widely anticipated. Our study aims to identify the proportion of cardiology patients who may benefit from SGLT2 inhibitors in a central London teaching hospital.
Methods We retrospectively analysed two patient cohorts from August 2019 to January 2020: 1) Inpatient (IP) Cardiology referrals (452 patients), and 2) Inpatient Heart Failure Service referrals (68 patients). Using four large-scale cardiovascular outcome trials - EMPA-REG, CANVAS, DECLARE-TIMI 58 and DAPA-HF; we generated a set of screening criteria for the suitability of SGLT2 inhibitors in patients with T2DM and HFrEF, and applied them to our cohorts (Table 1).
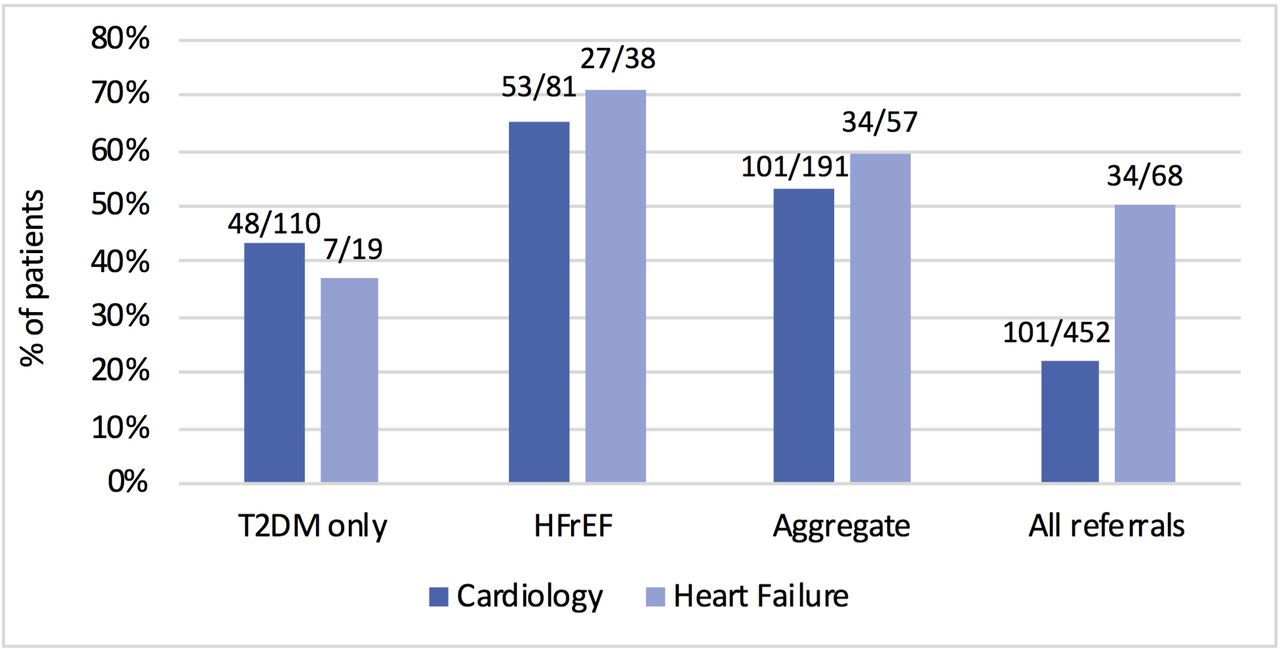
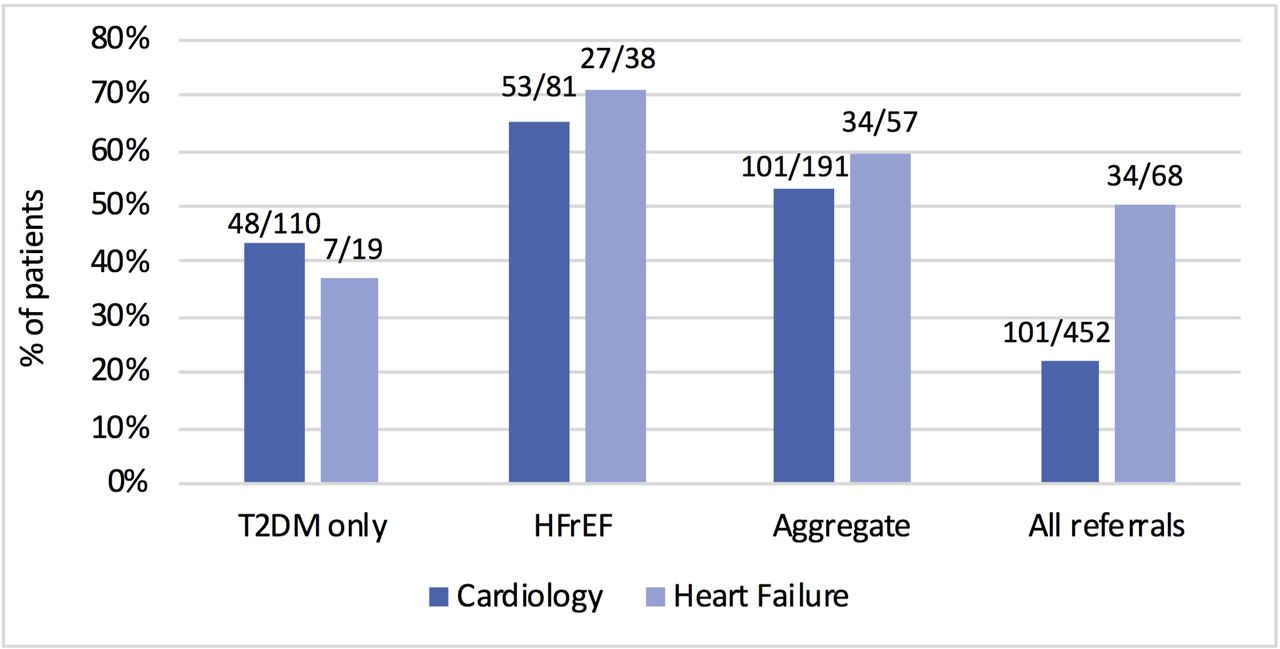
Results Over the 6 month period, 452 patients were referred for an IP Cardiology review; 191 (42%) of these patients had T2DM or HFrEF. Using our criteria, 101 (53%) of these 191 patients would be suitable, representing 22% of all Cardiology referrals. Only 5 patients were already on SGLT2 inhibitors. Looking at this more closely, 44% (48/110) of T2DM only patients were suitable for an SGLT2 inhibitor compared to 65% (53/81) of the HFrEF population. In the second patient cohort (IP Heart Failure referrals), half (34/68) of patients were suitable for SGLT2 inhibitors. The trend was broadly similar to the Cardiology referrals cohort, with 37% (7/19) of patients with T2DM only and 71% (27/38) of patients with HFrEF found to be suitable (Figure 1).
{kind=link}
Of all HFrEF patients who would be suitable for SGLT2 inhibitors, 81% (48/59) were on an angiotensin-converting-enzyme inhibitor, angiotensin-receptor blocker or sacubitril-valsartan; 92% (54/59) were on a beta-blocker; 25% (15/59) were on a mineralocorticoid receptor antagonist and 59% (35/59) were on a diuretic on admission. The main exclusion criteria in our patient cohorts was an estimated glomerular filtration (eGFR) rate below 30 mL/min/1.73m2 of body-surface area.
Conclusions Ahead of expected release of guidelines on SGLT2 inhibitor use in patients with HFrEF, we have formulated a set of screening criteria for suitability of SGLT2 inhibitors and applied them to our patient cohorts. The results show that 50% of patients referred to the IP Heart Failure Service and over 20% of patients referred to IP Cardiology may be suitable for SGLT2 inhibitors, which are much higher potential use rates than we had anticipated. This has important ramifications for cardiology services across the country when thinking about who will initiate this new heart failure therapy and in which setting.
Conflict of Interest None