Article Text

Abstract
CTFFR the SWindon Evaluation of Emerging Technology (CTFFR SWEET)
Aims To see how adding routine CT Fractional Flow Reserve (CTFFR) to CT Coronary Angiography (CTCA) altered the care pathway of patients with chest pain of recent onset.
Setting Rapid Access Chest Pain Clinic (RACPC) in a secondary care hospital in the South West of England supported by a well-established CT programme (since 2006). CTFFR was started in July 2018 as part of the NHS ITP programme, CTFFR was requested routinely for patients with CT scans of sufficient quality with visible stenoses of 30-90% in a major epicardial coronary arteries. The NICE cost model for CTFFR predicts a 50% reduction in subsequent angiography and reduced downstream costs.
Measurements Patient journey(s), costs, resource use.
Methods The RACPC database helped identify 2 consecutive 12 month patient cohorts and their initial testing strategy. Using hospital database searches the care of patients undergoing CTCA as a first test was examined in more detail. Codes of all care were obtained to estimate costs.
Results The initial testing strategy for each cohort is shown in Table 1.
Downstream testing, cath lab procedures and revascularisation by cohort that had CTCA as the first test are shown in table 2.
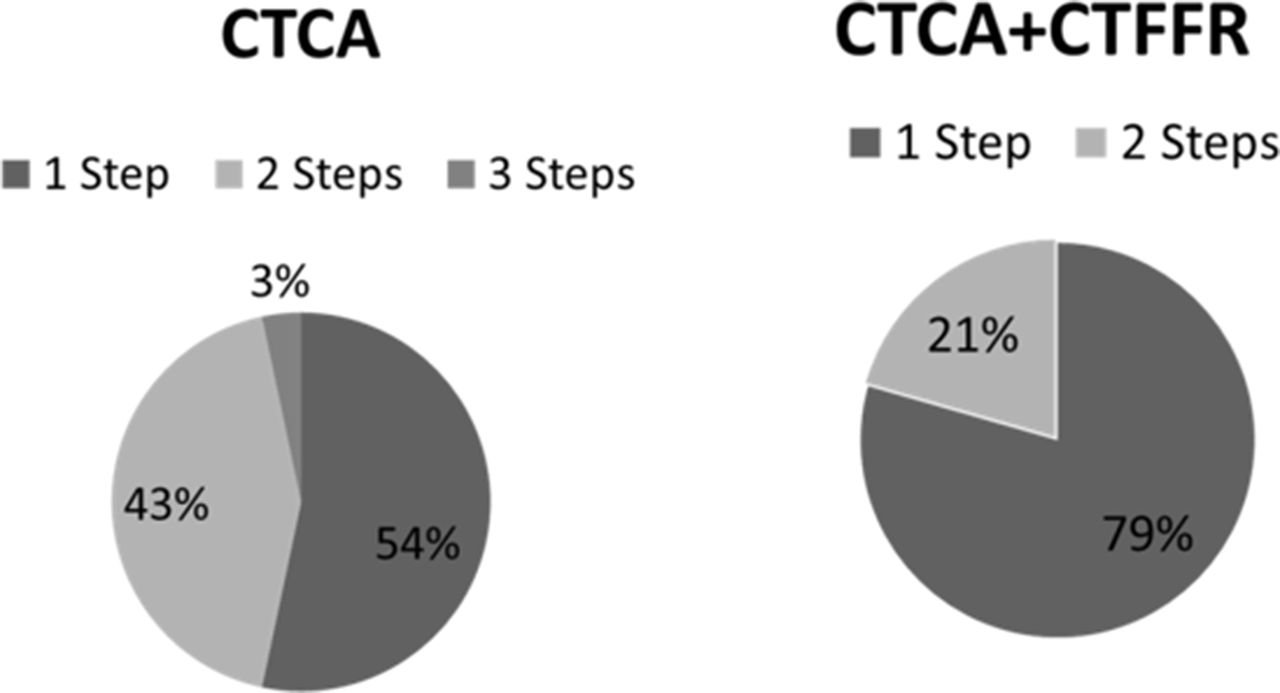
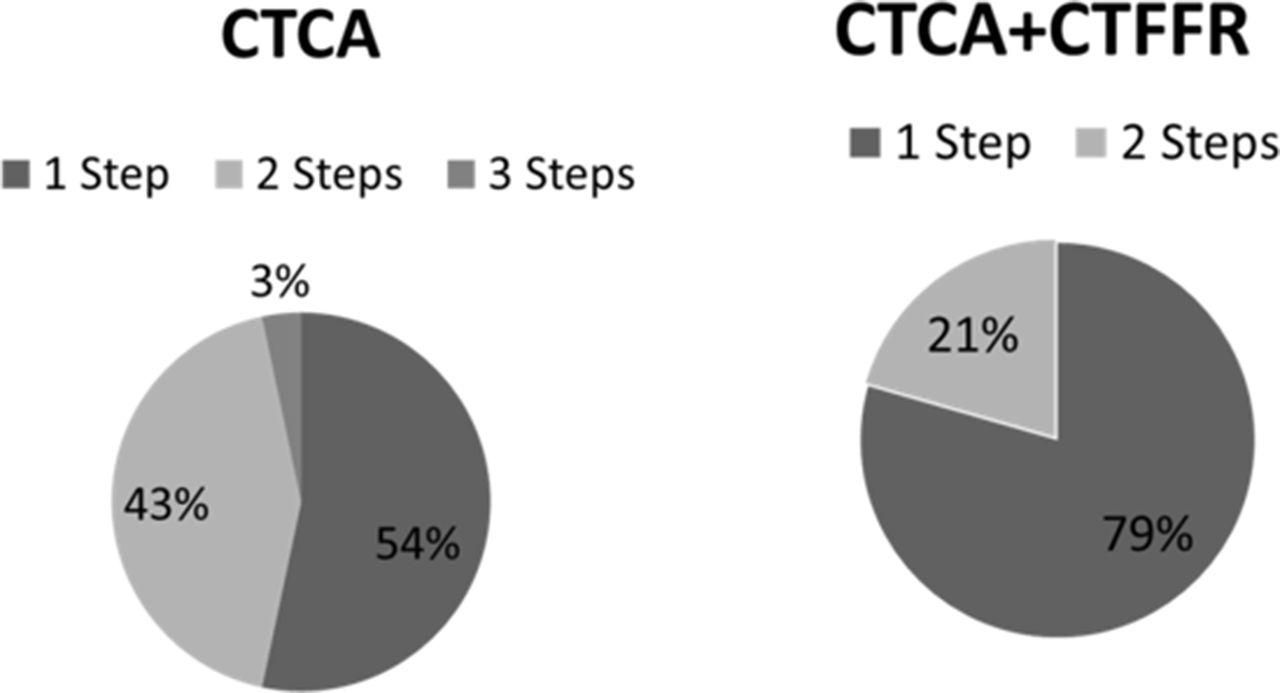
Patients who underwent CTCA as a first test had less steps (cath lab, revascularisation, stress imaging) in care following the introduction of CTFFR (Figure 1).
CTFFR helped identify patients likely to receive same day PCI, 51/276 patients had images sent for analysis. 41 were analysed successfully. 17 of these patients were scheduled for angiography. Of these there were 4 false positives. In the remaining 13, 8 underwent same day PCI and 1 was referred for CABG, Revascularisation Rate (RR) 69%. The RR was 66% in the 6/10 patients for whom CTFFR analysis was not possible referred for angiography, 1 same day PCI and 3 CABG. 12 other patients in the post CTFFR cohort were referred for angiography with a revascularisation rate of 42%, 2/4 PCI patients had same day procedures 1 had CABG.
In the CTCA only cohort 54% of PCI procedures were same day compared to 84% in the CTFFR group.
A rough estimate of costs using CTCA, DSE, CTFFR, Angiography and PCI per patient across the 2 cohorts showed £310 per patient pre and £471 per patient post CTFFR (AHSN cost model).
There was no appreciable difference in cath lab admissions in the CTCA first groups before and after the introduction of routine CTFFR, 35/363 (9.6%) vs 36/276 (13%).
{kind=link}
Conclusion This single centre observational study showed in our practice that CTFFR identified patients with significant coronary disease suitable for coronary intervention and streamlined care. The reductions in costs and angiography in the NICE model were not seen.
Conflict of Interest NIL