Article Text

Abstract
Objective To test the hypothesis that ventricular and atrial function are different between patients with transposition of the great arteries (TGA) after arterial switch operation (ASO) and healthy controls.
Methods 103 consecutive patients with TGA (median age: 16.7 years, 4.3–39.6 years, 71.8% male) were compared with 77 controls (median age: 15.4 years, 6.3–43.2 years, 66.2% male). Biventricular and biatrial function were assessed using standard cardiovascular magnetic resonance (CMR) techniques and feature tracking. Group comparison was performed with conventional non-parametrical statistics and machine learning methods to find the variables most discriminative between patients and controls. These variables were used to build a multivariable logistic regression model to assess the case–control status.
Results Markers of left and right ventricular function (LV; RV) (ejection fraction, MAPSE, TAPSE, LV long-axis strain) as well as LV global longitudinal (−20.7 (−24.1; −17.9) vs −23.7 (−26.1; −21.6), p<0.001), circumferential (−29.4 (−32.2; −26.5) vs −30.5 (−33.6; 29), p=0.001) and atrial longitudinal strain (left atrium (LA): 23.3 (18.6; 28.8) vs 36.7 (30.7; 44), p<0001; right atrium: 21.7 (18.2; 27.8) vs 34.9 (26.9; 40.3), p<0.001) were reduced in patients compared with controls using non-parametrical testing. The logistic regression model including the most discriminative variables from univariate and machine learning analysis demonstrated significant differences between patients and controls only for TAPSE and LA global longitudinal strain.
Conclusions Biventricular and biatrial function are largely preserved after ASO for TGA. Using a comprehensive CMR protocol along with statistical machine learning methods and a regression approach, only RV longitudinal function and LA function are significantly impaired.
- magnetic resonance imaging
- transposition of great vessels
- heart failure
- coronary vessels
Data availability statement
Data are available on reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
The arterial switch operation (ASO) is the standard operation for transposition of the great arteries (TGA).1 Compared with the atrial switch operation, it provides superior survival, cardiac function and better quality of life during long-term follow-up.2 3 However, complications after the ASO have been reported.1 2 Reduced left and right ventricular (LV, RV) function and atrial function has also been suggested in smaller case series using echocardiography and cardiovascular magnetic resonance (CMR).4–6
CMR is an important imaging modality in the evaluation of patients after ASO. It is well suited for the measurement of ventricular volumes and global systolic function, and also for the assessment of regional myocardial deformation using feature tracking (FT).7
The aim of this study was, first, to comprehensively assess biventricular and biatrial function in a large cohort of patients with TGA after ASO using CMR in comparison with healthy controls and, second, to test the hypothesis that ventricular and atrial function are different between patients with simple and complex TGA and between those with usual and unusual coronary artery anatomy.
Patients and methods
A general research consent was available for all participants, parents or legal guardians, as appropriate.
In total, 103 consecutive patients (median: 16.7 years, 4.3–39.6 years) with TGA after ASO who underwent a CMR examination as part of routine clinical follow-up between 2006 and 2020 were included in this study. Clinical data were retrospectively collected from medical records.
Seventy-seven healthy subjects matched for age and gender were enrolled as controls (median: 15.4 years, 6.3–43.2 years). Indications for the scans in controls were as follows: (1) participation in this study, (2) non-diagnostic echocardiography, (3) uncertainty about the cardiac anatomy on echocardiography, (3) syncope or (4) chest pain with low probability of being cardiac in origin. In all controls, a cardiac pathology could be ruled out. Controls were not on any cardiac medication. Blood pressure measurements and ECGs were available for all controls and were normal.
It was not appropriate or possible to involve patients or the public in the design, or conduct, or reporting, or dissemination plans of this research.
CMR acquisition
The CMR protocol included the acquisition of short-axis and four-chamber cine images using cine steady-state free precession or gradient echo sequences. Slice thickness and field of view varied according to patient size and were 5–8 mm and 250–420 mm, respectively. Sedation with propofol and midazolam was used in six paediatric patients with TGA. None of the controls needed sedation.
CMR analysis
CMR analysis was performed with MEDIS SUITE software (Medis Medical Imaging Systems, Leiden, The Netherlands) and cvi42 (Circle Cardiovascular Imaging, Calgary, Canada).
Biventricular volumes and mass were measured from short-axis stacks using cvi42 by drawing endocardial and epicardial borders. Endocardial and epicardial borders were drawn at end-diastole; at end-systole, only endocardial borders were drawn. Papillary muscles and trabeculations were included into the ventricular volumes. Volumes were calculated automatically and were indexed to body surface area (BSA). Ejection fraction (EF) was computed from the ventricular volumes by the analysis software. Maximum LV wall thickness was measured manually at end-diastole in short-axis stacks. To define the maximum, thickness at different ventricular levels was measured and the largest wall thickness measurement was taken for further analysis.
Mitral annular plane systolic excursion (MAPSE), tricuspid annular plane systolic excursion (TAPSE) as well as LV long-axis strain (LAS) were measured from four-chamber views with cvi42. For MAPSE and TAPSE, distance lines were drawn at end-diastole from both lateral mitral annulus and lateral tricuspid annulus through the cardiac apex to an extracardiac reference point as previously described.8 The same reference point was used for the distance line in end-systole. An extracardiac reference point was chosen to exclude apical motion from the measurements. MAPSE and TAPSE were calculated as the difference between the length of the end-diastolic and end-systolic distance lines (figure 1).
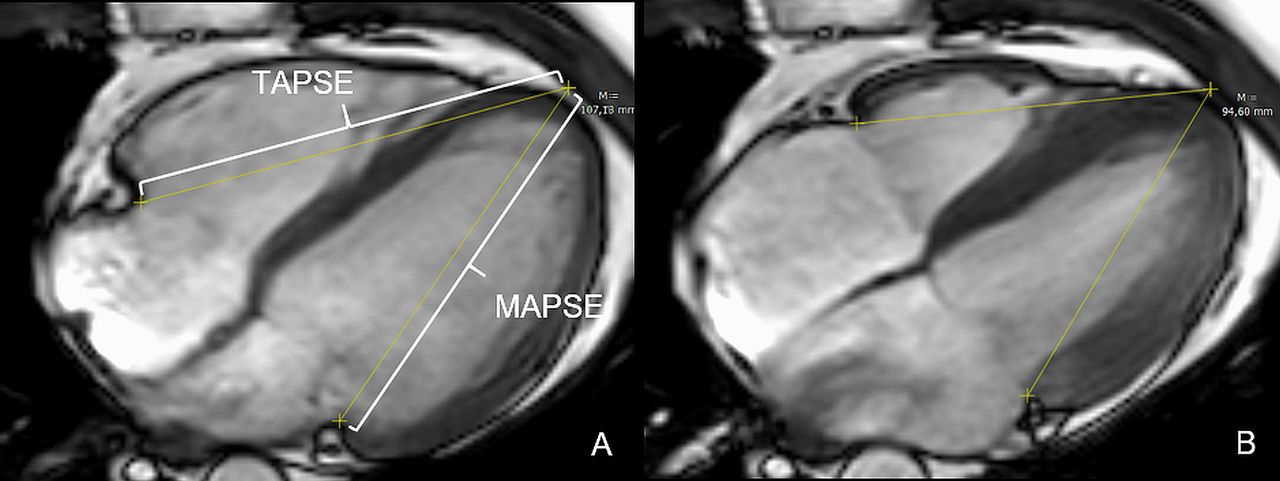
Measurement of mitral annular plane systolic excursion (MAPSE) and tricuspid annular plane systolic excursion (TAPSE) in the four-chamber view.
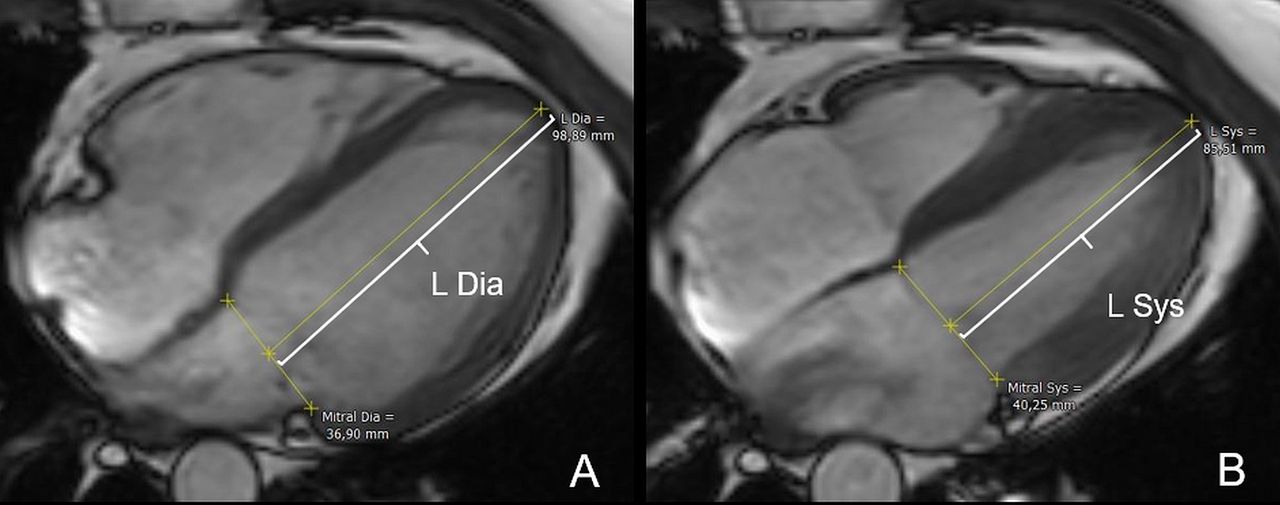
For long-axis strain (LAS), a distance line from the mitral valve annulus plane to an apical reference point was drawn in end-diastole (L Diastole) and end-systole (L Systole) as previously described (figure 2).9 LAS was measured using cvi42 and calculated according to the formula:


Cine cardiovascular magnetic resonance image illustrating the measurement of left ventricular long-axis strain.
Regional circumferential and radial strain and strain rate measurements were performed at three LV levels: (1) basal, (2) midventricular and (3) apical. Segmentation of each level followed the American Heart Association 16-segment model. The RV was divided into two segments in the four-chamber view: (1) septum and 2) free wall.
Regional and global longitudinal strain and strain rate for both ventricles and atria were measured in four-chamber views by drawing endocardial borders at end-diastole and end-systole. Global values for strain and strain rate were calculated as average of all segmental values. All regional and global strain and strain rate measurements were performed using MEDIS SUITE software (figure 3).

(A–D) Assessment of left ventricle (A), left atrium (B), right ventricle (C) and right atrium (D) longitudinal strain and strain rate from 4-chamber view. (E, F) Analysis of circumferential and radial strain from a short axis cine image.
Aortic regurgitation was assessed from phase-contrast flow measurements and was considered to be mild if the regurgitant fraction was 5% to 20%, moderate if the regurgitant fraction was 20% to 49%, and severe if the regurgitant fraction was ≥50%.
Statistical analyses
Statistical analyses were performed using MedCalc V.19.3.1 (MedCalc Software Ltd, Belgium) and R (V.3.5.0). Continuous variables are presented as mean value with SD or median with first and third quartile or with range of the lowest and highest values. Since most of the continuous variables showed deviations from the normal distribution (Shapiro-Wilk test), statistical analyses were done non-parametrically. Categorical variables were compared by Fisher’s exact test.
Due to the large number of explorative variables, a stepwise statistical analysis was performed. First, the most discriminative variables for TGA and controls groups were identified by using Mann-Whitney U tests and machine learning methods. The latter includes Boruta (R package ‘Boruta’ with 5000 replicates and default parameters from ‘Random Forest’ and ‘ranger’) which is an all-relevant feature selection wrapper algorithm for visualising variable importance measure.10 11 Second, the variables found to be most relevant were further used to build a multivariable logistic regression model including potential confounders such as gender, weight, BSA and heart rate. The final model was the result of subsequent forward selection with likelihood ratio criteria.
The same approach was used for subgroup analyses within the group of patients with TGA (simple vs complex; usual vs unusual coronary artery anatomy).
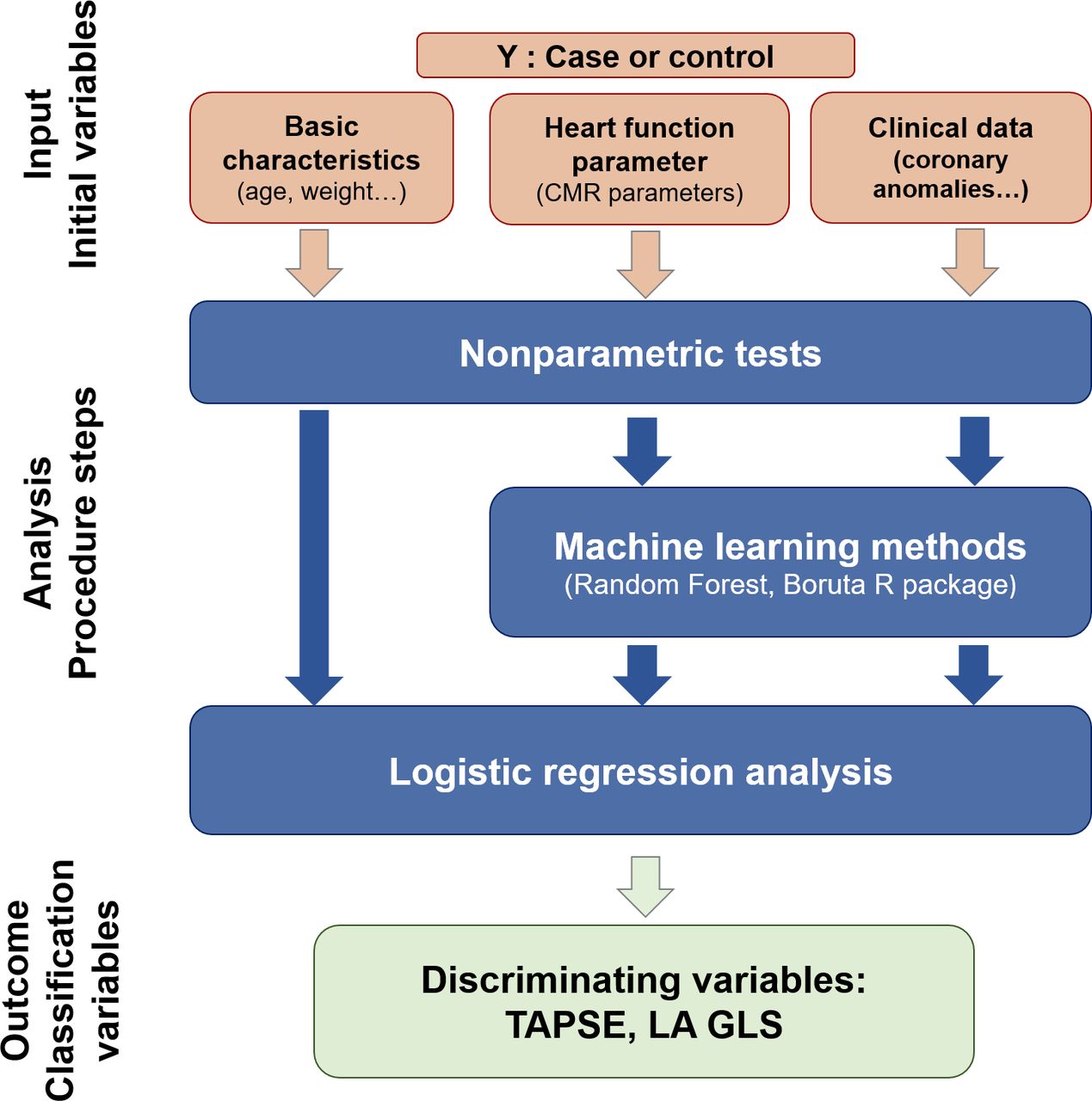
The statistical approach is summarised in figure 4.

Mann-Whitney U test together with machine learning methods were used to compare patients and controls and to identify most discriminative variables between patients and controls. The preselected variables were used for the multivariable logistic regression analysis and to build the final regression model.
For all statistical tests, p values <0.05 were considered as statistically significant.
Results
Patient characteristics
Characteristics of patients and controls are summarised in table 1. Eighty-five patients were treated with a primary ASO at a median age of 7 (1–107) days. Eighteen patients had a secondary ASO after prior pulmonary artery banding in the neonatal period (median age at ASO 1.2 (0.3–2.4) years).
Baseline characteristics of the study population
Sixty-six patients had simple TGA and 37 patients had complex TGA associated with a ventricular septal defect (n=30) and/or aortic coarctation (n=11). Forty-three patients had mild pulmonary stenosis (Doppler gradient <30 mmHg).
The majority of patients had none (n=65) or mild (n=31) aortic regurgitation. In seven patients, aortic regurgitation was moderate.
According to the Leiden classification,12 68 patients had a usual coronary anatomy (1LCx–2R). In 29 patients, the coronary anatomy was different from the usual coronary course (1L–2CxR, n=20; monocoronary system, n=7; 1RL–2Cx, n=1; LAD and LCx from different ostia, n=1). In six patients, the coronary anatomy was unclear due to incomplete records.
All patients were in New York Heart Association (NYHA) class I.
Conventional non-parametrical statistics
Ventricular volumetric measurements
Results are presented in table 2.
Cardiovascular magnetic resonance data for biventricular volumes and systolic function
In patients, left and right ventricular ejection fraction (LVEF, RVEF) were significantly reduced compared with controls. In addition, absolute and indexed LV end-diastolic and end-systolic volumes (LVEDV, LVEDVi, LVESV, LVESVi) as well as LV myocardial mass index (LVMMi) were higher in patients. RV stroke volume index (RVSVi) and RV cardiac index (RVCI) were lower in patients. Maximum LV thickness and LV cardiac index (LVCI) were not different between patients and controls.
Advanced functional CMR parameters including CMR-FT
Data are demonstrated in table 3.
CMR-FT data, TAPSE, MAPSE and LAS
MAPSE, TAPSE and LAS were significantly decreased in patients compared with controls (figure 5, table 3).

Mitral annular plane systolic excursion (MAPSE) and tricuspid annular plane systolic excursion (TAPSE) are reduced in patients with transposition of the great arteries (TGA) compared with healthy controls.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
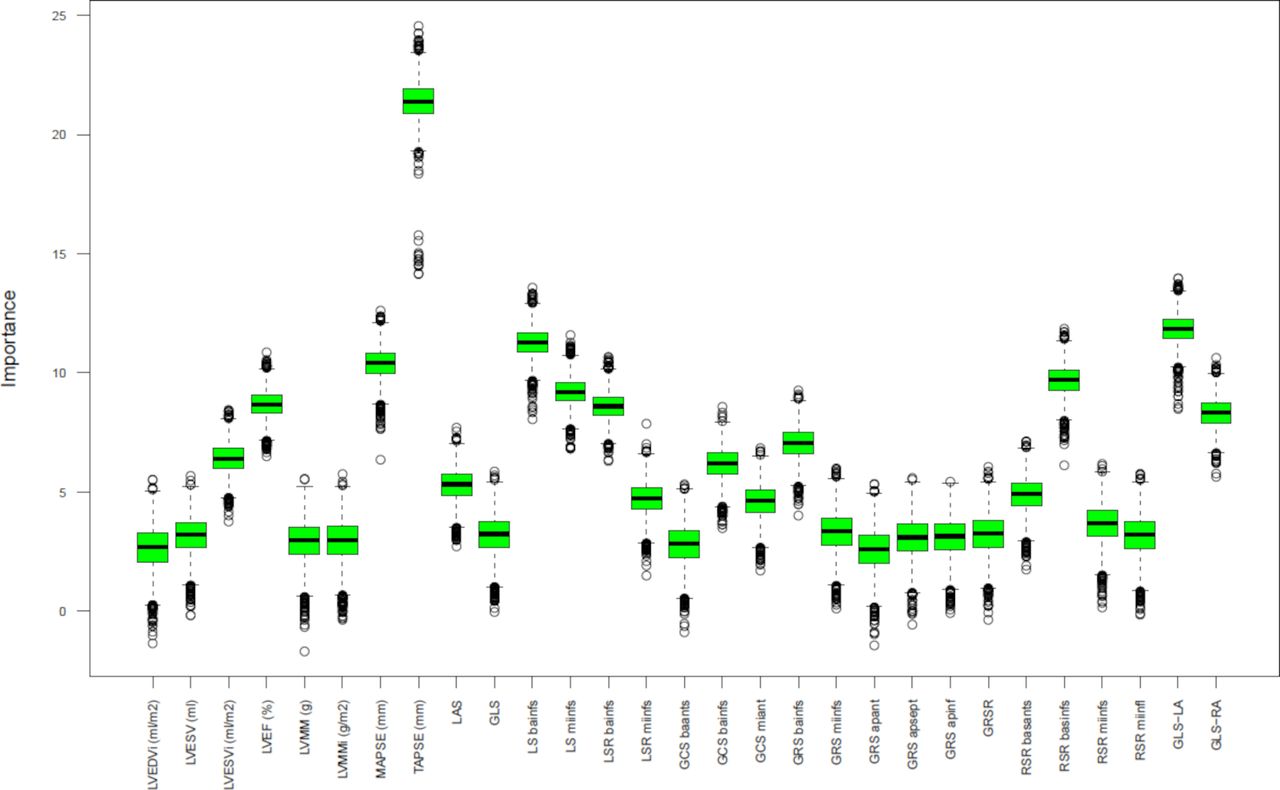
Boruta plot from machine learning analysis (random forest) demonstrating most relevant variables for differentiating the transposition of the great arteries and control group.
LV global longitudinal and circumferential strain values as well as longitudinal strain values of both atria were significantly reduced in patients. Global LV longitudinal and circumferential strain rate, global LV radial strain and strain rate, RV longitudinal strain and strain rate as well as left and right atrial (LA and RA) longitudinal strain rates were not different between patients and controls.
Machine learning methods
Preselection of variables with machine learning methods (random forest) together with Mann-Whitney U testing resulted in a list of 29 variables potentially discriminating between TGA and controls (figure 6, online supplemental figure 1). When adjusting the differences between these variables for potential confounders such as gender, height, weight, heart rate, BSA and body mass index in a multiple logistic regression analysis model, only TAPSE and LA longitudinal strain remained significantly reduced in patients compared with controls (table 4; TAPSE adjusted OR 0.52 (CI 0.39 to 0.64, p<0.001); LA longitudinal strain: adjusted OR 0.81 (CI 0.70 to 0.90, p=0.001).
Supplemental material
Logistic regression model (McFadden’s pseudo R2=0.77) adjusted for age (p=0.035), weight (p=0.03) and BSA (p=0.074)
Comparison of TGA subgroups
LV and RV volumetric and functional as well as CMR-FT parameters of the TGA subgroups are demonstrated in online supplemental tables 1–4.
Supplemental material
Discussion
Biventricular systolic and diastolic dysfunction has been reported in patients with TGA after ASO.4 13–15 Most studies, however, analysed only the LV and in relatively small cohorts often using echocardiography. With CMR imaging, it is possible to accurately assess biventricular volumes and function16 and to quantify global and regional myocardial deformation as well as atrial size. In this study, therefore, a large cohort of patients with TGA with a comprehensive and consistent CMR analysis protocol using conventional statistics combined with machine learning methods was analysed.
The present data suggest that patients with TGA in the midterm follow-up after ASO (<20 years of median follow-up) have largely preserved biventricular and biatrial function compared with controls. Only RV long-axis function (TAPSE) and LA longitudinal function were impaired in the TGA group. Furthermore, even in patients with complex TGA and in those with coronary anomalies potentially complicating repair, no major abnormalities of ventricular and atrial function were found.
Ventricular volumetric measurements
CMR studies in patients with TGA evaluating ventricular function after ASO are scarce and most include only small patient numbers. Grotenhuis et al assessed a cohort of 30 ASO patients and found normal LVEF in patients with higher LVEDVi and LVESVi compared with 28 controls.15 The same authors studied 15 patients with TGA and demonstrated reduced LVEF together with increased LV dimensions compared with 15 age-matched and sex-matched control subjects.17 The present study, however, using advanced statistical methods on a larger cohort of patients with TGA after ASO and adjusting functional data for potential confounders reassuringly suggests that these patients have a largely normal LV size and function.
Most studies available to date focused on the assessment of LV function only and only very few groups studied the RV after the ASO. Grotenhuis and co-workers used CMR to measure RV function and flow across the pulmonary valve after ASO.18 They found preserved RV systolic function whereas RV relaxation was abnormal as a result of RV hypertrophy.18 The results of the present study showed a lower RVEF in patients compared with controls; however, RVEF was not statistically significant different in the final logistic regression. Markers of diastolic RV function, however, were not analysed in this study.
A single study using echocardiography showed reduced LVEF, fractional shortening and circumferential fibre shortening in children after ASO at rest and wall motion abnormalities under dobutamine stress.4 Other echocardiographic studies, however, demonstrated preserved LVEF in this patient group.19 20
When considering potential factors that could affect LV and RV systolic function in patients with TGA, in particular perioperative and operative myocardial injury, operative strategies (eg, secondary ASO), myocardial ischaemia as well as aortic and pulmonary complications,1 2 the current findings suggest that the risk for a significant biventricular systolic contractile dysfunction from a potential complication in these patients is low.
Advanced functional CMR parameters including CMR-FT
Markers of longitudinal contractile function were only assessed in few studies after ASO. Klitsie et al found a reduced TAPSE and no difference in MAPSE in patients shortly after ASO.5 Others reported reduced values for MAPSE and TAPSE in adult patients with TGA.20 In this current study, TAPSE was significantly reduced suggesting that RV longitudinal function remains impaired after ASO. This alteration is likely not specific to ASO patients but rather represents an adverse effect of cardiac surgery itself.21 Increased RV afterload is a potential contributor to RV functional impairment after ASO, but none of the patients in the current study had a significant pulmonary artery obstruction.
To our best knowledge, this study is one of the first studies using CMR-FT for the assessment of biventricular and biatrial function in TGA after ASO. Previous studies used echocardiography to evaluate LV myocardial deformation after ASO.13 22–24 The ASO patients studied here only showed significantly reduced LA longitudinal strain. Other groups reported reduced values for LV global longitudinal strain and global circumferential strain (GCS) as well as septal and anterior segmental longitudinal strain.13 22–24 However, such abnormalities were not consistently found in ASO patients. Pettersen et al and Di Salvo and co-workers did not find differences in GCS between patients and controls13 22 and Grotenhuis’ group even reported higher GCS in ASO patients.15 Differences to this current study might be explained by the small number of patients and controls in the cited studies as well as by technical reasons (echocardiography vs CMR).
Global longitudinal strain and strain rate of the RV were normal in patients from the here presented study although TAPSE was reduced. This discrepancy might be explained by potential technical differences and limitations when using the FT techniques to assess RV deformation.7 In the setting of advanced heart failure or pulmonary hypertension, accurate TAPSE measurement might not be possible because of the rocking heart motion,25 26 whereas 2D-CMR-FT is in particular limited by its spatial resolution.7 RV strain and TAPSE are both easy to measure and suitable to assess the RV in patients with TGA, but TAPSE has the advantage that no specific CMR software is needed.
It has previously been shown that FT of the RA and LA is feasible27 and can distinguish patients with impaired LA relaxation from healthy controls.28 Recent CMR data from Voges et al 14 suggest impaired diastolic LV function in ASO patients and it can be presumed that impaired LA longitudinal strain also indicates LV diastolic dysfunction in these patients. The underlying mechanism for the impairment of LA longitudinal strain remains speculative, but it has to be considered that LA strain is likely to be affected by LV function. Increased imaging markers of diffuse myocardial fibrosis have been recently shown in patients with TGA and might contribute to LV diastolic impairment.15 In addition, myocardial hypoxia as well as reduced aortic elasticity might contribute to LV diastolic dysfunction represented by an impaired LA function.1 14 Future research on ventricular function in TGA should therefore focus on systolic and also perhaps more importantly on diastolic ventricular function.
Comparison of TGA subgroups
In the present study, global biventricular and biatrial function and deformation is not significantly different between simple and complex TGA and between those with usual and unusual coronary anatomy suggesting that there might be no significant difference in myocardial perfusion. These results are in keeping with a previous study from van Wijk et al who analysed LVEF and LV global longitudinal strain with echocardiography and did not find any differences between complex and simple TGA.23 It also supports a report from Tobler et al who used CMR to study the coronary anatomy and myocardial viability and did not find any abnormality in patients with an unusual coronary pattern.29 In keeping with Brown et al, the present data support the notion that the coronary artery anatomy is not a risk factor for longer term outcome of TGA after ASO.30
Limitations
This is a retrospective and cross-sectional study. The CMR protocol applied was however uniform and clinical data were nearly complete.
For the assessment of the longitudinal strain and strain rate, only the four-chamber view was used as two-chamber and three-chamber views were not available for all patients. Segmental strain and strain rate values have to be interpreted with caution as CMR FT is a technique that tracks features without considering certain anatomical landmarks between segments. In addition, through plane motion could have impacted on the FT results.
TAPSE measurements with the use of an extracardiac reference point could have been affected by apical rocking or dynamic LV function. However, that approach is thought to be less angle dependent.
Propofol sedation was only performed in patients but not in controls. This could have influenced the results for strain measurements and ejection fraction, but as the number of patients who needed sedation was small (n=6), the impact is probably negligible.
The cross-sectional study design does not allow to draw conclusions about the progression of LV and RV dysfunction and therefore further longitudinal studies are needed. Besides NYHA class, no further clinical information is given. However, especially data from cardiopulmonary exercise tests were only available in a subset of patients and this precluded meaningful statistical analysis. Patients with aortic regurgitation were not excluded. However, only a few patients had more than mild aortic regurgitation.
Conclusion
The data suggest that in patients with TGA after ASO, biventricular and biatrial function is largely preserved and that this applies also for patients with complex TGA and those with an unusual coronary anatomy. Using a comprehensive CMR analysis protocol along with statistical machine learning methods and a regression approach, only RV longitudinal and LA function are impaired at midterm follow-up after ASO.
Key messages
What is already known on this subject?
Reduced left and right ventricular as well as atrial function has been suggested in patients with transposition of the great arteries after arterial switch operation (ASO).
What might this study add?
A comprehensive cardiovascular magnetic resonance analysis protocol together with a statistical machine learning approach could show that only right ventricle longitudinal and left atrium function are impaired at midterm follow-up after the ASO.
How might this impact on clinical practice?
Although only minor functional abnormalities were detected, life-long monitoring of biventricular and biatrial function is required to detect potential functional deterioration late after the ASO.
Data availability statement
Data are available on reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
The study protocol was registered and approved by the local ethics committee (reference number: D562/19, date of approval: 3 Dec 2019).
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
RS and SF-W contributed equally.
PL and IV contributed equally.
Contributors IV, RS, SF-W and PL are responsible for the conceptualisation of the study. IV, RS and SF-W performed the formal analysis and wrote the initial draft. IV, RS and PL were involved in data collection. SK, DDG and AU provided critical review and helped with editing of the manuscript.
Funding This study was supported by Deutsches Zentrum für Herz-Kreislaufforschung e.V.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.