Article Text

Abstract
Objective Hypertension is the most important modifiable risk factor for stroke globally. We hypothesised that country-income level variations in knowledge, detection and treatment of hypertension may contribute to variations in the association of blood pressure with stroke.
Methods We undertook a standardised case-control study in 32 countries (INTERSTROKE). Cases were patients with acute first stroke (n=13 462) who were matched by age, sex and site to controls (n=13 483). We evaluated the associations of knowledge, awareness and treatment of hypertension with risk of stroke and its subtypes and whether this varied by gross national income (GNI) of country. We estimated OR and population attributable risk (PAR) associated with treated and untreated hypertension.
Results Hypertension was associated with a graded increase in OR by reducing GNI, ranging from OR 1.92 (99% CI 1.48 to 2.49) to OR 3.27 (2.72 to 3.93) for highest to lowest country-level GNI (p-heterogeneity<0.0001). Untreated hypertension was associated with a higher OR for stroke (OR 5.25; 4.53 to 6.10) than treated hypertension (OR 2.60; 2.32 to 2.91) and younger age of first stroke (61.4 vs 65.4 years; p<0.01). Untreated hypertension was associated with a greater risk of intracerebral haemorrhage (OR 6.95; 5.61 to 8.60) than ischaemic stroke (OR 4.76; 3.99 to 5.68). The PAR associated with untreated hypertension was higher in lower-income regions, PAR 36.3%, 26.3%, 19.8% to 10.4% by increasing GNI of countries. Lifetime non-measurement of blood pressure was associated with stroke (OR 1.80; 1.32 to 2.46).
Conclusions Deficits in knowledge, detection and treatment of hypertension contribute to higher risk of stroke, younger age of onset and larger proportion of intracerebral haemorrhage in lower-income countries.
- stroke
- hypertension
- epidemiology
Statistics from Altmetric.com
Introduction
Hypertension is an important modifiable1 risk factor for stroke.2–5 A number of international studies have reported regional and country income-level variations in awareness, treatment and control of hypertension.6–11 It is suspected that these variations in care gaps may contribute to differences in the risk, burden and pattern of strokes in countries at different economic levels.12 13 We explored whether variations in knowledge, detection (ie, awareness) and treatment of hypertension contribute to variations between countries at different economic levels in the magnitude of risk, burden and pattern of stroke and its subtypes, ischaemic and haemorrhagic stroke. Such information can assist in developing strategies to control hypertension and estimating the expected gains from improvements in hypertension detection and treatment globally and within countries of different income levels.14
Methods
INTERSTROKE is a large international case control study3 15 conducted from March 2007 to September 2015 in 142 centres from 32 countries.
Ethics
All participants, or their proxy, provided informed written consent before taking part in the study.
Participants
Cases
Cases were patients with first stroke admitted to hospitals within the preceding 72 hours, and with recent symptoms onset (<5 days), in whom neuroimaging by CT or MRI brain imaging could be completed within 1 week of presentation. Stroke was defined using the WHO clinical criteria for stroke.16 Neuroimaging was completed in 99.9% of cases. For patients unable to communicate adequately, proxy respondents were used. Key exclusions were: (1) patients unable to communicate because of severe stroke, aphasia or dementia who did not have a valid proxy respondent; (2) non-vascular causes; (3) current hospitalisation for acute coronary syndromes; 4) unable to get consent from proxy (online supplemental table 1).
Supplemental material
Controls
Controls were either community-based (54.7%) or hospital-based (45.3%). Hospital-based sources included patients admitted to hospital or attending outpatients for conditions or procedures not related to stroke or TIA or visitors or relatives of other in-patients. Detailed inclusion and exclusion criteria have been published15 (online supplemental table 2). Each control was matched for sex, age (±5 years) and site with cases, although this was extended to ±10 years for participants over 90 years of age. For the current analyses, cases and controls were matched for region and sex in all instances and age (95% within 5 years and 99.9% within 10 years).
Measurement of risk factors
Structured questionnaires were administered, and physical examinations were undertaken, in the same manner in cases and controls. Key vascular risk factors were measured in a manner consistent with the INTERHEART study17 (online supplemental appendix).
Questionnaire specific to blood pressure
Awareness of hypertension as a risk factor for stroke was recorded by asking all cases and controls whether they endorsed ‘high blood pressure’ to be ‘associated with an increased risk of stroke’. A self-reported history of hypertension was based on a direct question to patient (and/or proxy) about whether they were diagnosed with hypertension. Preadmission antihypertensive therapy was captured from the medical notes and at interview from cases and controls. During the study, we implemented supplemental questions, completed by 6143 participants, which asked participants whether they ever had a prior blood pressure measurement. Hypertension was defined as self-reported history of hypertension or the composite of self-reported hypertension or blood pressure ≥140/90 mm Hg. For cases and controls, we used blood pressure at the time of interview, which was completed by research staff in all centres. Blood pressure is cases was adjusted to account for acute phase effect and described in the online supplemental appendix. Categorisation of economic level of country was based on information from World Bank in 2010.18 As the largest proportion of countries belonged to the upper middle-income category, we divided this category into two groups separated at the mid-point of gross national income (GNI), with four categories of high-income countries (HIC), upper middle-income countries-1 (UMIC-1), upper middle-income countries-2 (UMIC-2) and lower middle and lower-income countries (LMIC/LICs), using GNI (online supplemental table 3).
Statistical analysis
Means and medians were calculated to summarise continuous variables and were compared by t tests or appropriate non-parametric tests. We evaluated the association of blood pressure with stroke risk, and the association of knowledge of hypertension, awareness of hypertension and treatment of hypertension with stroke risk (all stroke, ischaemic stroke and intracerebral haemorrhage) and by income-status of country. We also evaluated the association of hypertension awareness with prior blood pressure measurement and pre-admission treatment for hypertension.
We used conditional logistic regression for stroke outcomes and unconditional logistic regression for outcomes related to hypertension. In addition to the variables being matched within a stratum, all models were additionally adjusted for exact age, smoking, diabetes mellitus, physical activity, diet, psychosocial factors, abdominal obesity, alcohol, cardiac risk factors and apolipoproteins. We estimated population attributable risk (PAR) using the method described by Bruzzi.19 For variables with more than two categories (eg, treated and untreated hypertension), we used partitioned PAR estimators, such that the PARs for differing categories sum to the total PAR for hypertension. We estimated income-category variations in the PAR associated with treated and untreated hypertension. We also modelled the expected reduction in proportion of stroke globally, and by income status category, in different scenarios of identification and screening of known hypertension, using GIF estimators,20 which provide an estimate of the proportion of stroke that would be reduced if a risk factor was modified, based on summary estimates of association of treated and untreated hypertension with stroke risk in the current analyses. Impact fractions can be considered generalised versions of PAR percentages. Whereas a PAR percentage measures the proportional change in disease prevalence assuming a risk factor could be eliminated, impact fractions instead consider the effect of an intervention that causes a shift in the distribution of the risk factor, rather than a complete elimination. CI calculations (99%) were based on standard Wald type intervals for OR, PAR and impact fractions, with the SE of the PAR and impact fraction estimators being estimated via Bootstrap. Bootstrapping was implemented by resampling N matched case/control pairs from the overall dataset with replacement 100 times, when the original dataset consisted of N matched pairs. Tests of interaction were calculated using the likelihood ratio method, comparing likelihoods of models with and without the interaction term of interest. Statistical analyses and graphics were produced with SAS V.9.4 for UNIX (SAS, Cary, North Carolina, USA) and the open source language R, V.3.4.2.
Results
From March 2007 to September 2015, a total of 26 945 participants were recruited from 32 countries, comprising 13 462 individuals with acute first-ever stroke (cases) and 13 483 controls. The mean age was 61.7 years (SD 13.4), ischaemic stroke in 10 405 individuals (77.3%) and intracerebral haemorrhage in 3057 (22.7%). Table 1 and figure 1 describes the characteristics of cases and controls, for mean blood pressure, self-reported history of hypertension, use of antihypertensive therapy, knowledge that high blood pressure is a risk factor for stroke, prior blood pressure measurement and by income-level category of countries. The proportion of stroke due to intracerebral haemorrhage increased with reducing GNI of countries.

From left to right, figure reports proportion of cases and control that did not identify hypertension as a risk factor for stroke, proportion reporting no prior blood pressure measurement in their lifetime (subset of 6143 participants), proportion of cases and controls with a self-reported history of hypertension but not receiving preadmission antihypertensive therapy and proportion with a self-reported history of hypertension and receiving combination antihypertensive therapy. Income status of country based on gross national income. BP, blood pressure; HIC, high-income countries; LIC, lower-income countries; LMIC, lower middle-income countries.
Blood pressure, history of hypertension and pre-admission antihypertensive therapy in cases and controls
Association between history of hypertension and stroke, by preadmission use of antihypertensive therapy
Lack of knowledge that hypertension causes stroke was associated with lower rates of any lifetime blood pressure measurement (OR 1.86; 99% CI 1.47 to 2.37) and non-use of antihypertensive therapy in those with known hypertension (OR 1.60; 99% CI 1.40 to 1.83), but was not an independent risk factor for stroke (OR 1.06; 0.85–1.33 overall, and OR 1.14; 0.94–1.38 for analysis confined to cases with patient respondent only). Lack of knowledge of hypertension as a risk factor for stroke was higher in cases with intracerebral haemorrhage (34.1%) than ischaemic stroke (29.2%) and higher in LMIC/LICs than HICsfigure 1).
Of those completing supplementary questionnaire, 21.2% of participants reported no prior blood pressure measurement, which was a risk factor for stroke (OR 1.80; 99% CI 1.32 to 2.46), with non-measurement rates higher by lower-income level (figure 1). No prior measurement of blood pressure was more common in patients with intracerebral haemorrhage (33.5%) than ischaemic stroke (23.6%) (p<0.01).
Hypertension was associated with stroke in all regions, with a graded increase in OR from high to lower-income countries, (OR 1.92; 99% CI 1.48 to 2.49 for HIC, OR 2.29; 99% CI 1.73 to 3.02; for UMIC-1, OR 2.76; 99% CI 2.40 to 3.18 for UMIC-2 and OR 3.27; 99% CI 2.72 to 3.93 for LMIC/LICs; p-heterogeneity <0.0001). Among participants with a self-reported history of hypertension (table 1), preadmission antihypertensive therapy use was lower in cases (64.4%) than controls (78.0%) (p<0.001), with a gradient by income status of country, reflecting a treatment gap even among those who were aware of their hypertension (table 1, figure 1). Categorising those with a self-reported history of hypertension into those receiving, and not receiving preadmission antihypertensive therapy, revealed a stronger magnitude of association between prior history of hypertension without antihypertensive therapy (OR 5.25; 4.53–6.10) than those who reported pre-admission antihypertensive therapy (OR 2.60; 2.32–2.91) (P-interaction=0.01) (table 2, online supplemental table 4). Untreated hypertension was associated with a greater risk of intracerebral haemorrhage (OR 6.95; 5.61–8.60) than ischaemic stroke (OR 4.76; 3.99 to 5.68).
Figure 2 reports the PAR by income-level category, divided into those who were unaware of hypertension (no prior diagnosis), aware of hypertension but untreated and aware of their hypertension and treated, demonstrating a graded increase in the proportion of the PAR associated with untreated hypertension, by lower-income country category. While the prevalence of hypertension was lower in lower-income countries (compared with higher), the greater OR associated with untreated hypertension, resulted in similar PARs by income group. The PAR due to untreated hypertension (both among those detected and those undetected) was 10.4% in HICs, 19.8% in UMIC-1, 26.3% in UMIC-2 and 36.3% in LMIC/LICs (p<0.001). An analysis restricted to community-based controls demonstrated consistent findings (online supplemental figure 1). Online supplemental figure 2 report partitioned PAR for hypertension by age, sex and type of stroke (ischaemic and intracerebral haemorrhage). Use of antihypertensive therapy was lower in younger age groups, and the increased magnitude of association between hypertension and stroke in younger age groups persisted, after stratification for use of antihypertensive therapy (figure 3). Mean age of stroke was 65.4 years in those with treated hypertension and 61.4 years in those with untreated hypertension (p<0.01).
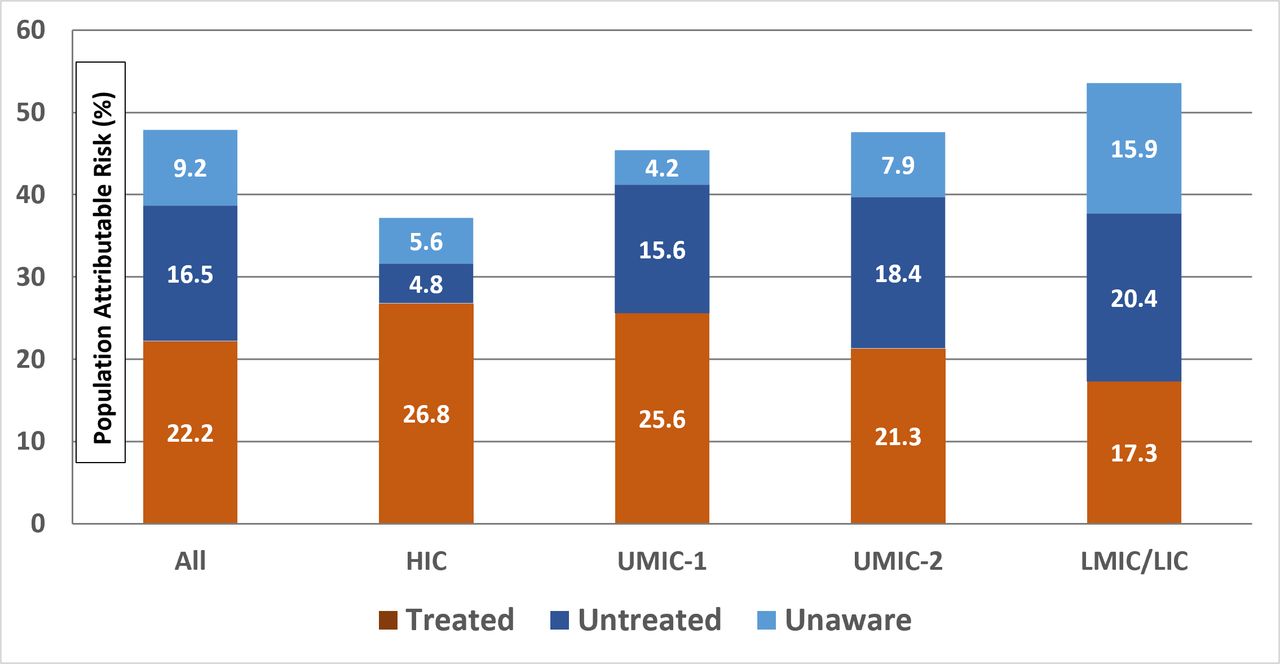
Figure reports partitioned PAR, by awareness and treatment status (ie, subdivided into proportion due to treated hypertension, known hypertension but untreated and undiagnosed hypertension). Data are shown overall and in GNI-level groups. Figure demonstrates a reduction in proportion of PAR associated with treated hypertension by income-category, with highest PAR for treated hypertension in HIC, and an increase in proportion of PAR associated with untreated hypertension in lower-income countries. Multivariable model including age, smoking, waist-to-hip ratio (WHR), diabetes, physical activity, alternate healthy eating index, alcohol intake, psychosocial factors, apolipoproteins and cardiac risk factors. GNI, gross national income; HIC, high-income countries; LIC, lower-income countries; LMIC, lower middle-income countries; PAR, population attributable risk.

{kind=link}
{kind=link}
{kind=link}
Figures report the association of hypertension with stroke by age (A) and GNI (B), demonstrating an increased slope in magnitude of association of hypertension with stroke by reducing age and reducing GNI, which is modified by treatment status. Within increasing intensity of antihypertensive therapy, there is a diminution in slope of curve. While a gradient remains for risk of stroke by age among treatment groups, there is an inversion of gradient by GNI. These figures illustrate that increased uptake of antihypertensive therapy are expected to have greatest impact in younger populations and in lower-income regions. Multivariable model including age, smoking, WHR, diabetes, physical activity, alternate healthy eating index, alcohol intake, psychosocial factors, apolipoproteins and cardiac risk factors. GNI, gross national income; PAR, population attributable risk.
Table 3 reports the association of hypertension with stroke, by number of preadmission antihypertensive medications reported. Use of combination antihypertensive therapy (two or more agents) among those with hypertension was 28.9% overall, 51.9% in HICs, 40.7% in UMIC-1, 20.7% in UMIC-2 and 17.9% in LICs. The risk association with treated hypertension was OR 2.91 (2.56–3.31) for one agent and OR 2.16 (1.86 to 2.50) for two agents or more. Non-use of antihypertensive therapy was associated with a higher OR in younger (OR 7.85; 5.84 to 10.55) than older age (OR 4.26; 3.54 to 5.12 for those >55 years). (P-interaction <0.01). Use of antihypertensive therapy and combination therapy was lower in lower-income regions (figure 1). Figure 3 reports the association of hypertension by age categories and GNI, for untreated hypertension and treated hypertension (with one or combination antihypertensive therapy). Both younger age and lower GNI are associated with higher ORs for the association of hypertension with stroke, which is attenuated with antihypertensive use. We modelled anticipated gains from improved treatment of known hypertension, using an estimate of generalised impact fraction of two scenarios. First, use of antihypertensive drugs at currently observed intensity in those known to have hypertension indicates that 10.3% of stroke globally would be avoided if known hypertensives were treated, but not necessarily controlled. This would be 3.8% (2.7%–5.0%) avoided in HIC, 10.4% (8.1%–12.7%) in UMIC-1, 11.5% (9.5%–13.5%) in UMIC-2 and 12.0% (9.6%–14.5%) in LMIC/LICs. Second is use of at least two antihypertensive agents in all known hypertensives; this indicates that 17.6% (13.6%–21.6%) of stroke globally would be eliminated, 9.1% (6.0%–12.1%) in HICs, 17.8% (12.9%–22.6%) in UMIC-1, 20.1% (15.1%–25.1%) in UMIC-2 and 18.4% (14.6%–22.1%) in LMIC/LICs. The GIF was larger for intracerebral haemorrhage (32.4%) than ischaemic stroke (13.5%), reflecting the higher prevalence of hypertension and larger OR for untreated compared with treated hypertension for intracerebral haemorrhage compared with ischaemic stroke.
Association between history of hypertension and stroke, by number of antihypertensive agents preadmission
Discussion
Hypertension is a key modifiable risk factor for stroke in all regions of the world and for both primary stroke subtypes. Poor knowledge that hypertension is a risk factor for stroke is associated with lower awareness of hypertension and non-use of antihypertensive therapy. Each of these care gaps was more common in lower-income countries, compared with higher-income countries, resulting in a higher OR associated with hypertension in lower-income countries. Hypertension, and particularly untreated hypertension, is a stronger risk factor for intracerebral haemorrhage than ischaemic stroke. Untreated hypertension, more common in lower-income countries, is associated with younger age of first stroke.
The PURE study reported major gaps in detection (46.5% of participants with hypertension were aware they had hypertension) and control (32.5%) of hypertension globally, with larger care gaps in lower-income countries, compared with higher income countries,.6 Our findings, in the current analysis of the INTERSTROKE study, extend these observations by quantifying the contribution of these gaps to the global burden, and epidemiologic pattern, of stroke. While we report a graded increase in the OR for hypertension associated with stroke by lower-income status of country, which resulted in a larger PAR for a given prevalence of hypertension, this was mostly related to a larger proportion of untreated hypertension in lower-income countries. Untreated hypertension was more strongly associated with intracerebral haemorrhage (versus ischaemic stroke) and predicted a younger age of stroke onset, meaning that care gaps in detection and treatment of hypertension result in a larger burden of stroke and differences in case mix, case-fatality (due to higher intracerebral haemorrhage) and socioeconomic consequences due to younger age of onset, which are observations consistent with other epidemiologic studies.2 5 Our data also suggest that greater population-level use of antihypertensive therapy is now favourably changing the epidemiologic association between blood pressure and stroke, whereby countries with higher use of antihypertensive therapies have a lower risk of stroke associated with hypertension, lower proportion of intracerebral haemorrhage and older age of first stroke onset.
A limitation of the PAR estimate is that it provides a theoretical estimate of the reduction in stroke associated with the complete elimination of hypertension (which is not ever likely), rather than an estimate of anticipated gains from available and potentially feasible interventions. Of greater relevance to health policy, therefore, is the anticipated gains with greater detection and control of hypertension. The impact fraction associated with treatment of hypertension is lower than the corresponding PAR. This difference between PAR and impact fraction likely reflects a number of factors. We report a residual risk associated with controlled hypertension, which is consistent with prior studies reporting have reported higher cardiovascular risk among individuals with controlled hypertension, compared with those without hypertension.21 22 This residual risk of stroke may also be due to concomitant risk factors, suboptimal treatment of hypertension, risk associated with intermediate phenotype (eg, small vessel disease) related to a period of undiagnosed hypertension or unmeasured confounders such as undetected atrial fibrillation. This implies that strategies to reduce the risk of stroke in those with hypertension needs to control blood pressure and include combined approaches such as lipid lowering,23 smoking cessation and detection and treatment of atrial fibrillation.24 Such a combined approach is more important for prevention of ischaemic stroke, compared with intracerebral haemorrhage where the impact fraction associated with hypertension is 32.4% for treating known hypertension (compared with 13.4% for ischaemic stroke) due to a larger OR related to untreated hypertension and greater relative risk reduction with hypertension control.25 In addition, our estimates of impact fractions are based on the current INTERSTROKE population, rather than population-wide efforts to prevent hypertension derived from international prospective cohort studies.
Most individuals with hypertension require combination therapy to control blood pressure.26 We observed the lowest risk of stroke associated with hypertension in the subgroup receiving two or more antihypertensive agents, particularly for intracerebral haemorrhage (table 3). While we report a graded reduction in use of combination antihypertensive regimens by lower-income-level groups, all had low rates of combination antihypertensive use, including HICs, which is also consistent with studies reporting high rates of treatment but low rates of hypertension control in HICs.3 4 We observed a sequential lowering of stroke risk association with increased treatment intensity of hypertension. Interventions that target barriers to optimal detection and treatment of hypertension, including educational programmes to increase awareness of hypertension, non-physician led screening and algorithm-based use of fixed-dose combination therapy (eg, Polycap,27 low-cost generic medications, have the potential to exact major gains in reducing stroke.28–30
Our study has some limitations. The case control nature of our study incurs unavoidable sources of bias, such as recall bias. For example, the prevalence of knowledge of hypertension as a risk factor for stroke among stroke patients may not reflect their knowledge prior to their hospital admission, which is expected to affect knowledge among cases more than controls, and which may account for a similar rate among cases and controls, despite lower rates of detection and treatment in cases. Prior assessment of blood pressure measurement was higher in controls than reported in the PURE study and other studies.6–8 This difference may be due to varying approaches to selecting controls from outpatient or general practice settings, where measurement of blood pressure may be routine, and the inclusion of a larger proportion of urban centres, as we required hospital sites to have access to neuroimaging. Additionally, the rates of treatment for hypertension among controls were also higher, but more consistent with estimates reported in the PURE study, than estimates for undetected hypertension.6 As such, our estimates for the PAR related to undetected hypertension likely represents an underestimate, but our estimates of PAR and impact fraction related to uptake of antihypertensive treatment among those with known hypertension are expected to be more reliable. Our approach to adjusting for the acute phase effect of stroke on blood pressure may have overpenalised, especially for intracerebral haemorrhage (online supplemental figures 2 and 3) and may have resulted in underestimating the frequency of undiagnosed and uncontrolled hypertension, but the direction of bias would most likely result in an underestimate of the PAR related to undiagnosed (and controlled) hypertension, and therefore, our estimates should be considered conservative. For this reason, we did not report an estimate for impact fraction for prior undiagnosed hypertension.
Summary/conclusion
In conclusion, deficits in knowledge, awareness and treatment of hypertension contribute to higher risk of stroke, younger age of onset and larger proportion of intracerebral haemorrhage in lower-income countries, compared with HICs. These data suggest that strategies to improve knowledge about hypertension in the population, access to blood pressure screening programmes and low-cost combination antihypertensive therapy could have a major impact on reducing the global burden of stroke, particularly premature stroke in LMICs.
Key messages
What is already known on this subject?
Hypertension is the leading modifiable risk factor for stroke globally. Rates of detection, treatment and control are inadequate in all regions of the world, but particularly in low-income and middle-income countries.
What might this study add?
In this paper, we report that deficits in knowledge, detection and treatment of hypertension contribute to higher risk of stroke, younger age of onset and larger proportion of intracerebral haemorrhage in lower-income countries (compared with higher income regions). Alternatively viewed, our data suggest that greater population-level use of antihypertensive therapy is now favourably changing the epidemiologic association between blood pressure and stroke, whereby countries with higher use of antihypertensive therapies have a lower risk of stroke associated with hypertension, lower proportion of intracerebral haemorrhage and older age of first stroke onset.
How might this impact on clinical practice?
These data suggest that strategies to improve knowledge about hypertension in the population, access to blood pressure screening programmes and low-cost combination antihypertensive therapy could have a major impact on reducing the global burden of stroke, particularly premature stroke in lower middle-income countries.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @Machachi2016, @conorjudge
Contributors All authors contributed to the collection of data, discussions and interpretation of the data, and to the writing of the report. All authors reviewed and approved the manuscript for submission. The study was designed, the analyses were planned and the manuscript was drafted by MO’D and SY. Statistical analyses were performed by PR-M and JF. MO’D and SY wrote the first draft of the manuscript.
Funding The INTERSTROKE study is funded by the Canadian Institutes of Health Research, Heart and Stroke Foundation of Canada, Canadian Stroke Network, Swedish Research Council, Swedish Heart and Lung Foundation, The Health & Medical Care Committee of the Regional Executive Board, Region Västra Götaland, and through unrestricted grants from several pharmaceutical companies with major contributions from Astra Zeneca, Boehringer Ingelheim (Canada), Pfizer (Canada), MERCK, Sharp and Dohme], Swedish Heart and Lung Foundation, UK Chest, and UK Heart and Stroke.
Disclaimer No medical writer or other people were involved in the design, analysis or writing of this manuscript.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval The study was approved by the ethics committees in all participating centres.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement No additional data are available.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.