Article Text

Abstract
Introduction Coronary artery calcification (CAC) is commonly seen in patients undergoing percutaneous coronary intervention (PCI) in the United Kingdom (UK). An aging population with risk factors such as diabetes and chronic kidney disease (CKD) have contributed to the rise in the prevalence of CAC. Despite advancement in PCI and alternative plaque modifying technology, rotational atherectomy (RA) remains an important adjunct to facilitate stent delivery. The UK records the highest use of RA in Europe, with a rate of 3.1% of total PCI. We report the 10-year experience of RA in a large UK tertiary hospital.
Method This was a single tertiary centre, retrospective study of prospectively collected data on 213 patients who underwent RA PCI between October 2010 to February 2020. Procedural success and complications were assessed. The clinical outcomes evaluated were: target lesion revascularisation (TLR), readmission with heart failure, acute coronary syndrome (ACS) within 1 year, 30-day mortality and 18-month mortality. Subgroup analysis of outcomes in patients aged more than 80, severe left ventricular dysfunction and chronic kidney disease was performed.
Results Patients had a mean age of 72.9 ± 8.6 years. 77.9% (n=166) were male. 67.6% (n=144) had hypertension, 35.7% (n=76) had diabetes, 9.4% (n=20) were actively smoking, 6.6% (n=14) had CKD 4-5, and 15% (n=32) had severe left ventricular systolic dysfunction (LVSD). 51.2% (n=109) had prior MI, 34.7% (n= 74) had previous PCI and 20.2% (n=43) previously had coronary artery bypass grafts. Indications were: acute coronary syndrome (52.6%), stable angina (41.3%) and bailout during STEMI (6.1%). 75% were discussed at the MDT prior to RA, and 25% were ad-hoc PCI. Predominant access was via the radial artery (74.6%), using 6F sheaths (60.6%). 1.5mm burr was most frequently used (63.4%) but in 14.6% of cases, burr upsize was required. Additional equipment such as cutting balloons (4.7%), intravascular ultrasound (13.6%), microcatheters (58.2%), temporary pacing wires (2.3%) and intra-aortic balloon pumps (1.4%) were used.Complexity of procedures ranged from RA of unprotected left main stem (14.6%), more than 1 vessel RA (2.8%), chronic total occlusions (5.2%) and in-stent restenosis cases (0.9%). Mean stent diameter was 3.5 ± 0.8mm and mean stent length was 37.6 ± 23.4mm. Stents were successfully delivered in 96.2% of cases, with a complication rate of 10.3% (table 1). At 18 months, we observed no significant difference in mortality between the age groups (p=0.26). However, patients with eGFR less than 30 (35.7%, p=0.004) and ejection fraction <35% (17%, p=0.03) undergoing RA had a significantly higher mortality rate at 18 months (figure 1,2).
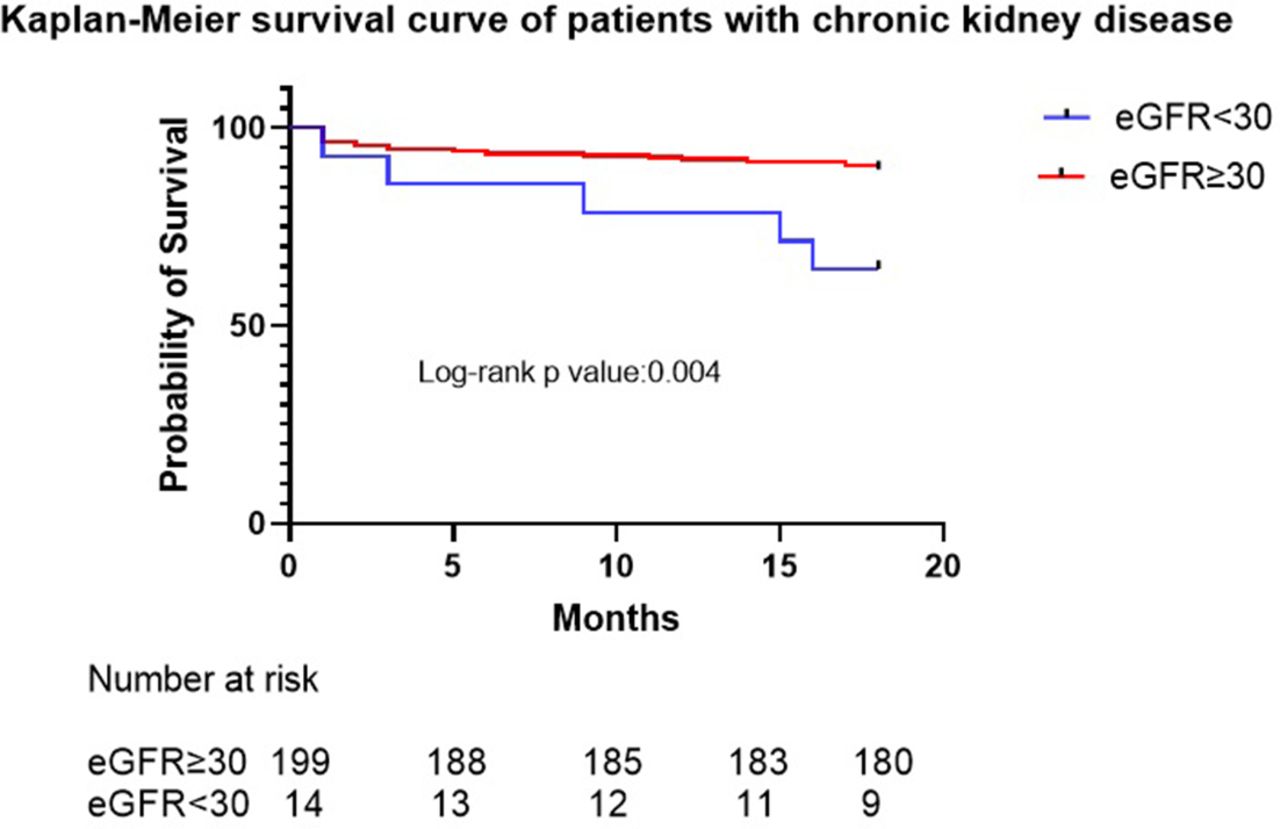
Kaplan-Meier survival curves of patients with CKD

{kind=link}
{kind=link}
Kaplan-Meier survival curves of patients with LVEF <35%
List of complications
Clinical outcomes
Conclusions Our study suggest that severe LVSD and CKD 4-5 may be a predictor for worse outcomes among rotablation patients. However, advanced age does not appear to be associated with poorer outcomes.
Conflict of Interest None