Article Text

Statistics from Altmetric.com
Introduction
The gender gap in academic medicine, including in cardiovascular medicine, is well-established with evidence on women’s under-representation as authors of research papers, editors of medical journals or in leadership positions at medical boards and institutions.1–3 There has been hardly any improvement over the past decades.4 Women’s under-representation in academic medicine may, at least partially, explain their lower participation in leading conferences.5
The COVID-19 pandemic forced many international medical conferences to move to an online environment, where participants interact remotely, with a blend of live and prerecorded events. Although, in theory, this transition to digital conferences could have removed some of the known access barriers for women,6 the actual impact on women’s representation is yet to be established.
Women’s representation at the European Society of Cardiology congress
The European Society of Cardiology (ESC) congress is well established and one of the largest medical conferences worldwide. It took place fully online in 2020 and 2021, thus providing the opportunity to investigate the impact of transition to digital conferences on women’s representation among faculty (ie, invited speakers) and abstract presenters.
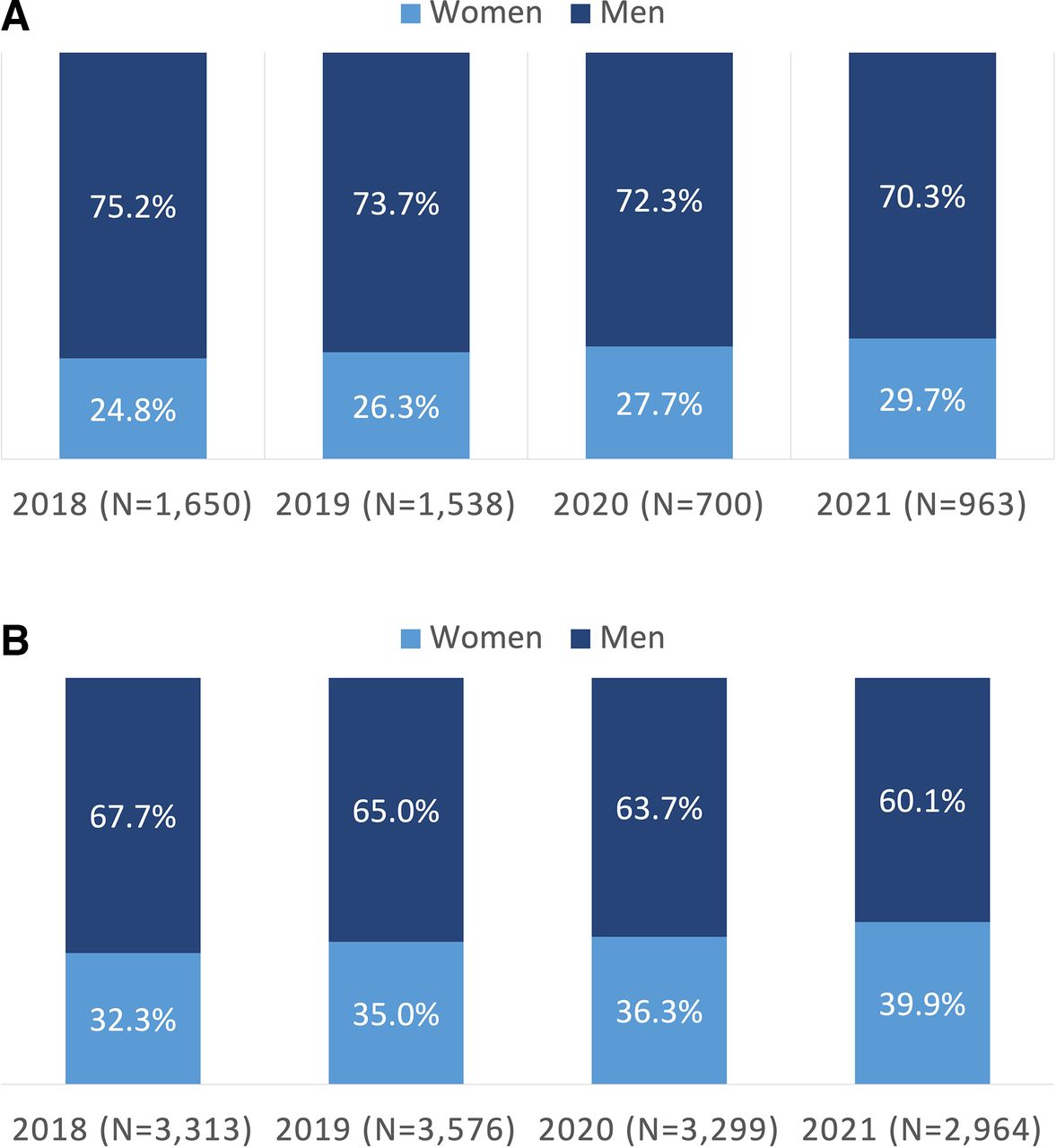
Data on self-reported gender available on registration forms were provided by the ESC congress organisers for faculty and abstract presenters. Data were not available for participants in general. Overall, there was no strong evidence that women’s representation changed substantially among faculty and abstract presenters in response to the transition from in-person to virtual conferences in 2020 and 2021 (figure 1). Taking faculty and abstract presenters combined, the percentage of women was 30% in 2018, 32% in 2019, 35% in 2020 and 37% in 2021, but the gradual increase in women’s representation appears part of an upward trend over the years, with no clear uptick that could be attributable to the digital transition. Despite a steady increase in women’s representation among faculty from 24% in 2018 to 30% in 2021, they remain under-represented. Women’s representation has always been higher among abstract presenters than faculty, with an increase from 32% in 2018 to 40% in 2021.

{kind=link}
(A) Percentage of faculty stratified by gender and year. (B) Percentage of abstract presenters stratified by gender and year.
The representation of each continent remained broadly stable between 2018 and 2021 (table 1). About three-fourths of faculty and two-thirds of abstract presenters (ie, women and men) were from Europe, particularly from Western Europe. Women’s representation among faculty ranged from 26% in Asia to 67% in Africa, and from 27% in Africa to 44% in Europe for abstract presenters in 2021, with no evidence of an increase attributable to the digital transition. In Europe, women’s representation ranged from 14% in Southern Europe to 54% in Northern Europe for faculty and from 32% in Western Europe to 54% in Eastern Europe for abstract presenters in 2021. This transition to digital conferences might have increased overall representation of abstract presenters from Southern Europe (25% in 2019 to 32% in 2021) and representation of women within Northern Europe (32% in 2019 to 61% in 2020). On the other hand, there was a substantial drop in women’s representation among faculty between 2019 and 2020 from 40% to 23% in Eastern Europe, 47% to 24% in Northern Europe and 36% to 17% in Western Europe.
Overall and women’s representation at the ESC congress between 2018 and 2021 stratified by continent and by European region
The context of women’s representation in cardiovascular medicine
Although women’s under-representation among faculty and abstract presenters is a matter of concern, it needs to be interpreted in the context of the wider representation of women among ESC members and in cardiovascular medicine in general. As of 2021, there are approximately 105 000 members of the ESC (including all association free and paying members, fellows, ESC professional members, national cardiac society members, councils, working group members), of whom 35.7% are women, 60.1% are men and 4.2% are of unknown gender. Furthermore, a recent study found that women were leaders of 30% (254/849) of cardiology departments in Europe.7 Women leaders were younger than their men counterparts (mean 52 years vs 58 years, respectively) and had significantly fewer scientific publications than men (median 16 publications vs 44 publications, respectively). Considering this evidence, the overall of 37% women as faculty and abstract presenters at the 2021 congress broadly reflects women’s general representation within the ESC and in cardiology departments in Europe. The greater under-representation of women among faculty than abstract presenters may be partially explained by their younger age and lower representation as leaders and authors of scientific publications, trials and guidelines than their male counterparts.1 4 Notwithstanding the comparable representation of women among abstract presenters and faculty at the ESC congress and among ESC members, women are under-represented in both cases, and we should strive for gender equity across the academic and clinical ladders to reflect women’s representation in the general population.
Possible explanations for persisting women’s under-representation
The lack of a marked improvement in women’s representation at the digital ESC congresses may have several explanations. The congress was only confirmed to go ahead fully online in May 2020 and the abstract submission deadline in February 2020 coincided with the first wave of the COVID-19 pandemic in Europe. The unprecedented disruption caused by lockdowns, including working from home and closure of schools and childcare facilities, meant women were more likely to have to juggle homemaking with their job.8 Entrenched social roles that still allocate to women most unpaid caring responsibilities and housework exacerbated the gendered impact of the pandemic. The consequences for women in academia may have been worse than women in clinical medicine, who qualified as key workers and hence could access childcare during lockdowns. Disruptions continued, although to a lesser yet variable extent, throughout 2021, thus limiting ability to do research, publish papers and submit abstracts to conferences, likely more so for women.8 In addition, an unequal share of teaching and administrative tasks between women and men means women had to bear the brunt of the fast transition to remote teaching and learning.8 The increased need for pastoral support alongside developing new learning resources and getting familiar with new platforms and ways of teaching, may have prevented women from dedicating time to research activities, including conferences. Finally, irrespective of the COVID-19 pandemic, women in cardiovascular medicine might have fewer research opportunities on which to write conference abstracts, which means removing physical access barriers is not a silver bullet that will fix their longstanding under-representation.3 Women may have not been able to benefit from the convenience of online conferences due to a combination of conflicting academic, social and family roles and lack of research opportunities.
The larger gender gap among faculty than abstract presenters, found in this study, may be due to a failure in supply or demand. On one hand, it may be due to lower acceptance of invitations by women. On the other hand, poor representation of women as faculty may be due to bias in invitation and a perceived lack of ‘suitable’ women in top positions to invite. It is well-established that women are poorly represented in senior or leadership positions in academic and clinical medicine, which typically grant faculty invitations for leading conferences.3 This is, thus, feeding a vicious cycle in which poor representation of women begets poor representation of women. Breaking this cycle requires concerted efforts from academic and clinical institutions, as well as medical societies and other key stakeholders, to establish more equitable systems of academic merit.6
Implications for future medical conferences
As we gradually emerge from the pandemic, it is critical to reflect on what lies ahead to avoid perpetuating or, even worse, exacerbating gender inequalities, specifically regarding international conferences. There is widespread recognition of the advantages of digital conferences in terms of accessibility, flexibility and, especially, environmental friendliness. However, the drawbacks of remote interaction are also acknowledged, particularly the lack of networking opportunities, which may be more detrimental to women than men. There is also increasing reluctance from industry to sponsor digital conferences, due to the limited ability to engage with delegates in this format. Considering their important contribution to sponsor these expensive events, fully online conferences may become unviable. Therefore, hybrid events are increasingly seen as a promising strategy to conciliate the best aspects of digital and in-person conferences. However, to what extent hybrid conferences will affect women’s representation is yet to be understood. If women preferentially attend and present virtually while men attend and present in person, hybrid conferences may exacerbate gender inequalities. The consequences of hybrid meetings on women’s representation should, thus, be closely monitored by conference organisers. All conferences should also actively support and enable women’s participation, for instance, by providing breastfeeding rooms and childcare in conference venues. In addition, conference organisers should strive to ensure gender balance among faculty, by inviting at least an equal number of women and, preferably, with adequate global representation. It is important to acknowledge the substantial progress made by the ESC congress organisers since 2015, when women comprised merely 22% (341/1541) of faculty, which may have been fuelled by an overall increase in women’s representation in cardiovascular medicine. Medical conferences are extraordinary platforms for disseminating cutting-edge research, sharing and discussing innovation, and celebrating personal and collective achievements. Missing these opportunities to showcase their research, know the most up-to-date research and network may hinder women’s career progression. Furthermore, women’s under-representation can be detrimental to the academic community, innovation and ultimately to patients, because diversity enhances the value of research and clinical care, thus emphasising the need for removing barriers and enact policies that promote gender equality and diversity in cardiovascular medicine.
Conclusion
Despite substantial progress over the past 4 years, women remain under-represented at the ESC congress, particularly among faculty, who are likely to be more senior than abstract presenters. Although this reflects the overall under-representation of women within the ESC and in academic and clinical cardiovascular medicine, it emphasises the need to ensure international conferences adopt women-friendly policies and practices to address longstanding and avoidable gender inequalities.
Ethics statements
Patient consent for publication
Acknowledgments
We would like to thank to thank Professor Barbara Casadei and the ESC congress organising committee in general for the support provided with obtaining the data required to conduct this study.
Footnotes
Twitter @cheryl_carcel
Contributors A-CP-G, SAEP, AV and MW designed this study. A-CP-G extracted and analysed the data and drafted the manuscript. All authors interpreted the results and critically reviewed the manuscript.
Funding This study was not funded. MW is supported by National Health and Medical Research Council of Australia grants APP1149987 and APP1174120. CC is funded by the National Heart Foundation of Australia (postdoctoral fellowship 102741). ACPG is funded by an Academic Clinical Fellowship by the National Institute for Health Research.
Competing interests MW is a consultant for Amgen, Kyowa Kirin and Freeline.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Commissioned; internally peer reviewed.