Article Text

Abstract
Objective Current generation left ventricular assist devices (LVADs) operate with a fixed rotation speed and no automated speed adjustment function. This study evaluates the concept of physiological pump speed optimisation based on aortic valve opening (AVO) imaging during a cardiopulmonary exercise test (CPET).
Methods This prospective crossover study (NCT05063006) enrolled patients with implanted third-generation LVADs with hydrodynamic bearing. After resting speed optimisation, patients were randomised to a fixed-modified speed or modified-fixed speed CPET sequence. Fixed speed CPET maintained baseline pump settings. During the modified speed CPET, the LVAD speed was continuously altered to preserve periodic AVO.
Results We included 22 patients, the mean age was 58.4±7 years, 4.5% were women and 54.5% had ischaemic cardiomyopathy. Exertional AVO assessment was feasible in all subjects. Maintaining periodic AVO allowed to safely raise the pump speed from 2900 (IQR 2640–3000) to 3440 revolutions per minute (RPM) (IQR 3100–3700; p<0.001). As a result, peak oxygen consumption increased from 11.1±2.4 to 12.8±2.8 mL/kg/min (p<0.001) and maximum workload from 1.1 (IQR 0.9–1.5) to 1.2 W/kg (IQR 0.9–1.7; p=0.028). The Borg scale exertion level decreased from 15.2±1.5 to 13.5±1.2 (p=0.005).
Conclusions Transthoracic AVO imaging is possible during CPETs in patients with LVAD. Dynamic echo-guided pump speed adjustment based on the AVO improves exercise tolerance and augments peak oxygen consumption and maximum workload.
- echocardiography
- heart-assist devices
- cardiomyopathy, dilated
- heart failure, systolic
Data availability statement
Data are available upon reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Left ventricular assist devices (LVADs) have greatly affected the survival and quality of life of patients with end-stage congestive heart failure (HF). Modern continuous flow pumps (CF-LVADs) have an annual survival rate of 80%, making this method competitive to heart transplantation (HTx).1 Such devices improve the survival and quality of life in end-stage HF. Moreover, third-generation pumps are relatively easier to implant and more reliable than previous generations, yet still impose limits on patient activities.1
The limitation of exercise tolerance in patients with LVAD is multifactorial and results from biventricular HF, inadequate chronotropism, multiorgan dysfunction, pulmonary hypertension, ventilatory inefficiency, anaemia and myopathy.2–6 However, an insufficient rise in cardiac output in response to increased flow demand seems to be one of the most important factors that can potentially be modified.7 The controllers of current generation LVADs do not change the rotation speed based on haemodynamic parameters, exercise load or heart rate (HR), and may not cover exertional needs. Modification of pump revolutions is made only by trained personnel, primarily based on transthoracic echocardiography (TTE) and under resting conditions.8–10 Moreover, patients cannot adjust the speed depending on their expected exercise load. Therefore, the need for designing a physiological LVAD speed controller, tailored to a specific patient’s needs and dynamically changing metabolic demand, has been suggested, despite the technical imperfections of pressure transducers.4 7 11–15
The peak exercise capacity of patients with HF, despite LVAD implantation remains severely impaired.3–5 12 13 It can be assessed by a cardiopulmonary exercise test (CPET), which is considered to be safe in patients with implanted LVADs.4 13 14 A bicycle CPET in the semirecumbent position enables simultaneous TTE, which may allow the observation of the aortic valve opening (AVO) rate, one of the markers of pump speed adequacy, and the subsequent dynamic adjustment of the pump speed.
The primary objective of the study was to evaluate the capability of ultrasound appraisal of AVO during a cycle ergometer exercise. The secondary objectives were to assess the purposefulness of dynamic LVAD speed adjustment based on the AVO rate during CPET to maximise pump performance and to determine predictors of possible oxygen consumption (VO2) increase. Thus, we aimed to evaluate the concept of dynamic CF-LVAD speed adjustment to provide the rationale for physiological pump control protocols.
Materials and methods
Study design
A prospective crossover design was chosen due to the expected small group size and high positive correlation between participant responses and pump speed adjustment. Carryover and period effects were not likely to bias this study as CPETs lasted for several minutes and were performed a day apart.
Subjects were enrolled between February 2017 and July 2020 in a single centre implanting 20 LVADs annually. Patients with implanted cardioverter-defibrillator and third-generation centrifugal CF-LVAD with hydrodynamic bearing (HVAD, Medtronic, Minnesota, USA), at least 3 months after surgery, were included. Exclusion criteria were the following: haemodynamic instability, non-therapeutic anticoagulation, device or intracardiac thrombus, inflammation and bleeding.
The study lasted for 3 consecutive days. The first day was devoted to baseline evaluation, including TTE and a resting pump speed optimisation ramp test. During the next 2 days, under comparable conditions and off beta-blockers, patients underwent two CPETs supervised by an echocardiographer (figure 1). Subjects were randomised in a 1:1 allocation to one of two sequences—fixed/modified speed CPET or modified/fixed speed CPET—according to a computer-generated list using permuted block randomisation with a block size of 2.

Study flowchart and key results. CPET, cardiopulmonary exercise test.
LVAD speed adjustment
The pump speed was optimised twice during the study. The first time was at resting conditions on day 1 to ensure comparable baseline left ventricular (LV) unloading. The fixed speed CPET was carried out with these settings, invariably. The modified speed CPET started and finished with optimal resting pump settings. Through the exercise, the speed was dynamically adjusted based on live TTE imaging.
Optimal LVAD speed settings were defined as periodic AVO while maintaining the central position of the intraventricular septum, minimising mitral regurgitation and preserving a mean systemic blood pressure above 65 mm Hg. The AVO ratio was defined as the percentage of electrocardiographic beats with a forward flow sufficient to open the aortic valve (AV). The primary aim during baseline optimisation and modified speed CPET was to achieve an AVO ratio of around 25%–33% by changing the pump speed (online supplemental figure S2). The target AVO rate was based on previous research and with the intention to promote residual LV contractility.7–9 16 When AVO rose above the target value, the pump speed was increased by 100 revolutions per minute (RPM). As the AVO decreased below 25%, the RPM was lowered by 100. There was no determined target speed, neither per time period nor maximal. The only hypothetical pump operating limits were those specified by the manufacturer (1800–4000 RPM). Resting optimisation was based on 2-minute intervals; when reaching optimal settings, smaller speed changes were required to fine-tune the pump. During the modified speed CPET, the speed increment was not greater than 100 RPM per 45 s to enable an echocardiographic analysis of resulting changes and prevent suction events. After the peak exercise of modified speed CPET, the pump speed was reduced gradually to baseline under echocardiographic guidance.
Supplemental material
Echocardiography
Two Philips systems (Philips Ultrasound, Bothell, Washington, USA) were used: a stationary iE33 for preoperative and resting LVAD echocardiography and a portable Cx50 for exercise studies (online supplemental figure S1). Both devices were equipped with 1–5 MHz sector transducers. Images were stored in the DICOM format and the Cx50 was fitted with a digital video recorder.
All TTEs were performed according to guidelines by the same cardiologist certified in echocardiography. He was experienced in both HF and LVAD domains and had a decisive role in pump speed setting. Echocardiographic measurements and image interpretations were performed independently by two cardiologists, blinded to clinical data, using ComPACS (Medimatic S.R.L., Genova, Italy) workstation.
Post-implant ejection fraction (EF) was determined using the Teichholz formula due to limited apical views. The right ventricular (RV) systolic function was assessed mainly with tricuspid annular plane systolic excursion (TAPSE), RV free wall strain (RVFWS) and fractional area change (FAC). In the absence of reference values for the LVAD population, the following were considered as ‘good’: TAPSE ≥13 mm, RVFWS≤−10% and FAC ≥28%.
Cardiopulmonary exercise tests
Tests were performed in the semirecumbent position on a bicycle ergometer. An Ergometrics ER 900 L reclining ergometer (ergoline GmbH, Bitz, Baden-Württemberg, Germany) and a stationary MES START 2000 M ergospirometer (MES Sp. Z o.o., Skawina, Malopolska, Poland) were used (online supplemental figure S1). The exercise protocol was based on workload increments of 25 watts (W) every 2 min. An Elemano ES-H55 sphygmomanometer (Terumo Corporation, Tokyo, Japan) was used.
LVAD monitoring
Due to the lack of an authorised high-frequency sampling acquisition method of the controller signal, for subsequent evaluation of LVAD operation, an EOS 600D camera (Canon, Tokyo, Japan) was used for recording of the pump monitor. The camera rested on a custom-made focusing rack (online supplemental figures S1 and S3) and was enhanced with Magic Lantern V.2.3 firmware.
Data and statistical analysis
Pilot research (unpublished data) revealed that the SD of the VO2 peak difference between the fixed and modified speed CPETs was 2.03 mL/kg/min and the expected difference in means was 2.3 mL/kg/min. Allowing for a 50% variation in the assumed SD, at least 21 patients were needed to have a 90% probability of detection of the assumed difference at the 0.05 two-sided level of significance. Participant availability, resources, the complexity of the study and group size in similar analyses were taken into account as well.3 5 10
MATLAB V.2019b (MathWorks, Natick, Massachusetts, USA) was used for numerical analyses, data mining and advanced visualisations. Custom video analytics software for the interpretation of display data was developed.
Shapiro-Wilk, Lilliefors, Kolmogorov–Smirnov and Jarque–Bera tests were used for normality assessment. When any of the selected tests rejected the hypothesis of a normal distribution, non-parametric calculations were further used.
Standard descriptive statistics were applied to basic characteristics. Continuous variables with normal distribution were presented as mean (standard deviation (SD)), non-normally distributed variables were reported as median (interquartile range (IQR)), whereas categorical variables were presented as numbers (percentages).
The paired samples t-test for normally distributed variables, the Wilcoxon signed-rank test for non-parametric variables and the McNemar test on nominal data were used to compare related samples. Unpaired samples t-test for normally distributed variables, Wilcoxon rank-sum test for non-parametric variables and Fisher’s exact test for unpaired categorical data were used to compare independent samples.
Statistical analyses were performed using Statistica V.13.3 (Tibco Software, Palo Alto, California, USA). A p value less than 0.05 was considered significant.
The investigation conforms to the principles outlined in the Declaration of Helsinki. The study was approved by the Institutional Bioethics Committee (approval number 122.6120.256.2016, dated 29 September 2016) and was registered at ClinicalTrials.gov (identifier: NCT05063006). All subjects gave written informed consent to participate in the study.
Patient and public involvement
Patients or the public were not involved in the design or conduct, or reporting or dissemination plans of this research.
Results
Twenty-two patients were included. They were predominantly overweight (26.8 kg/m2; IQR 24.5–30.8) males (21, 95.5%) with ischaemic cardiomyopathy (12, 54.5%), in their late 50s (58.4±7 years). Preoperatively, they were mostly stable but inotrope-dependent. Half of them were qualified for LVAD as a bridge to HTx and half as a bridge to candidacy. Subjects were recruited about 7 months after the surgery and showed noticeable functional improvement. More detailed characteristics are shown in table 1.
Clinical characteristics by sequence and by total
Resting pump speed optimisation was required in 16 patients (72%) to achieve intermittent AVO with an average increase of 165 RPM (6%) together with power (0.8 W, 14%) and pump flow (0.6 L/min, 14%) boost (table 2). In six subjects (28%), the pump speed remained unchanged. Most subjects had a good or mildly impaired RV systolic function, no signs of LV recovery and insignificant valvular regurgitations. No adverse events such as suction events, notable ventricular arrhythmias or RV systolic dysfunction were noted during ramp studies.
Resting pump optimisation
Periodic AVO lasted for consecutive days (p=0.789). On day 1, after speed optimisation, AVO was 33% (IQR 25–50); before CPETs on day 2 and 3 was 50% (IQR 0–100), invariably for both days. The AVO ratio and other optimal LVAD speed criteria were concordant during pump adjustments.
All 44 CPETs were adequately performed, submaximal tests (10, 22.7%) were included in the analysis. The main reason for termination was leg fatigue (table 3). Aortic valve cusps movement was noticeable in all patients in at least one view. A noticeable increase in HR, EF and absolute values of RVFWS were recorded (figures 2 and 3).
Cardiopulmonary exercise parameters

Exercise tests, comparison of vital signs. Continuous variables are represented as median (interquartile range) by boxes; p values are from Wilcoxon signed-rank test.

Exercise tests, comparison of selected echocardiographic parameters. Continuous variables are represented as mean (standard deviation) by diamonds and median (interquartile range) by boxes; p values are from paired samples t-test (normal distribution) and Wilcoxon signed-rank test (non-normal distribution). AVO, aortic valve opening; EF, ejection fraction; LVEDd, left ventricular end-diastolic dimension; LVESd, left ventricular end-systolic dimension; RVIDd1, basal right ventricular internal dimension in diastole.
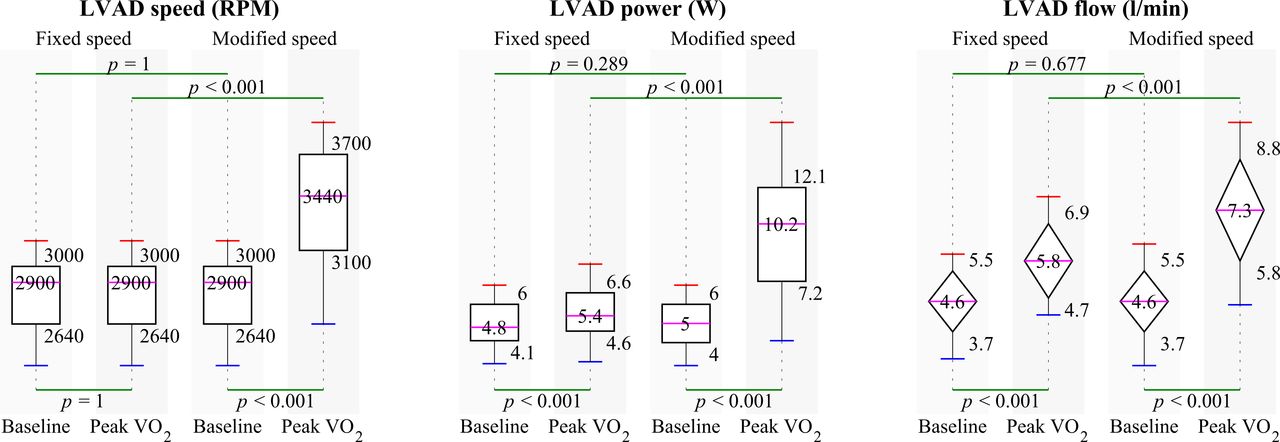
The baseline pump parameters did not differ in both CPETs. The pump speed, power and flow increased significantly during the echo-guided exercise (figure 4). Fifteen patients (68.2%) responded with more than a 5% gain of peak VO2 values. Dynamic pump speed optimisation allowed to achieve greater exercise workloads and VO2 values. Patients perceived less exertion and there was a visible trend towards longer exercise time (table 3).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Exercise tests, comparison of pump parameters. Continuous variables are represented as mean (standard deviation) by diamonds and median (interquartile range) by boxes; p values are from paired samples t-test (normal distribution) and Wilcoxon signed-rank test (non-normal distribution). LVAD, left ventricular assist device.
Responders to dynamic pump speed optimisation were identified with an arbitrary set cut-off point of 25% VO2 increase. The analysis of selected clinical, biochemical, ventilation and echocardiographic parameters is presented in table 4.
Selected predictors of achieving a 25% increase VO2 (responders) during modified speed exercise test
During the fixed pump speed exercise, a mild RV systolic dysfunction appeared in two subjects at the beginning of the test and in one case in the recovery. At the time of echo-optimised exercise, a transient episode of RV dysfunction occurred in one patient at the peak exercise. Despite this, the subject achieved a VO2 peak increase of 21%. The impairment was manifested as an increase in basal RV internal dimension and a decrease in FAC that lasted for only several cardiac cycles. Neither suction events nor significant ventricular arrhythmias were recorded. Table 3 and figures 2–4 show detailed stress test data.
Discussion
In patients with implanted assist devices, total cardiac output is the sum of LV and LVAD output. LVAD output depends on its rotational speed and the pressure difference between cannulas. LVADs operate with a fixed speed and do not have an automated speed adjustment capability. Thus, the pump output rises due to physiological exercise preload increase and theoretical afterload reduction. However, it may not be sufficient to meet the increased metabolic demand and may cause systemic hypoperfusion, therefore limiting exercise capacity.7
It was shown that rising the pump speed during a stress test increases the maximum exercise tolerance; however, in previous studies, the impeller was accelerated with no physiological feedback.11–14 17–20 Theoretically, the maximum haemodynamic support should lead to maximum exercise tolerance. Unfortunately, excessive and long-lasting LV support may result in dangerous suction events, RV overload, AV immobilisation, haemolysis, bleeding and thrombotic events. There are laboratory-proven, physiological control protocols based on pressure measurement, blood flow and flow pulsatility.21–24 Regrettably, pressure transducers, necessary for their application, have not been implemented in commercially available pumps mainly due to their technical imperfection. We show that parameters used in echocardiography can help to overcome this limitation.
Routinely, pump speed optimisation is based mainly on serial TTEs assessing the degree of LV decompression, RV function and AVO rate in proportion to electrocardiographic QRS complexes.6–8 15 17 Constant AV observation may allow evaluation of the residual LV systolic reserve and match the LVAD speed to metabolic requirements.25 Periodic AVO is one of the determinants of optimal LVAD speed settings and usually easy to assess by resting TTE. It increases during exercise even with AV closed at baseline. AVO imaging was available in all patients, despite the unfavourable exercise conditions, in at least one view. Excessive respiratory chest movement, pump-generated artefacts and tachycardia were the main imaging impediments. These observations are consistent with reports of Gross and Clifford.25 26
The novelty of our approach to exercise LVAD control was adjusting the pump speed to the current physiological demand based on real-time echocardiographic imaging. We focused on the AVO ratio as it is easy to assess with echocardiography during CPET and potentially feasible to interpret by the pump controller.27–30 Live exercise echocardiographic chamber measurements are, due to their time-consuming nature, practically impossible and burdened with a measurement error. Besides, dimensions of the ventricles, analysed offline, did not change substantially during exercise (figure 3). For these reasons, an isolated assessment of the AVO ratio seems feasible for TTE-supervised exercise tests and as input data for the next generation of controllers. This concept allowed us to safely increase pump speed by an average of 20%, augment peak VO2 consumption and maximal workload, reduce perceived exertion, and generally provide greater LVAD support than described in other studies.12 13 17–20 In vivo data on dynamic LVAD control during exercise and based on AVO have not been published in the literature so far.
The results of the conducted study do not affect the current management of patients with LVAD, as intended. The resting pump speed optimisation strategy seems optimal for non-smart controllers. The results, however, may have an impact on future work on dynamic (smart) LVAD speed management by rephrasing echocardiographic imaging into variables interpretable by the controller. There are currently applicable technical methods based on motor windings current analysis and use of an implantable aortic root ultrasound transducer for continuous AV monitoring.27–30 Furthermore, data obtained by the speed controller can be supplemented with an accelerometer and ECG signal for adjusting the pump speed.
The physiological, ‘support on-demand’ approach may reduce the exertional overload of dysfunctional LV and maximise exercise capacity. Moreover, this concept can potentially reduce the number of complications (suction events, RV failure, aortic regurgitation, bleeding, haemolysis), extend battery life, endorse residual pulsatility and enable the introduction of fully implantable systems, thus requiring additional investigation. Further studies may result in controllers upgrade or new control protocols for the next generation of pumps.
Our group tried several approaches to designate responders to dynamic exercise LVAD optimisation. Finally, due to the relatively small group size, we set an arbitrary cut-off point of 25% VO2 increase to determine six responders. This analysis showed a lower fixed speed exercise peak VO2 values and, paradoxically, better exercise tolerance to be statistically significant in the group of responders. These observations suggest the benefit of exercise pump speed tailoring in mildly symptomatic patients with objectively impaired exercise tolerance. The use of a logistic regression model to label responders was rejected due to the group size.
Study limitations
Undoubtedly, limiting factors of the study are the small sample size and the single-centre design. However, for the outcome measure, significant differences of measured parameters were found. Moreover, the sample size of such a complex, unique study does not differ from other studies in the field.
The HVAD system (Medtronic, Minnesota, USA) was withdrawn from the market during the preparation of this manuscript. However, this fact should not affect the study implications due to multiple similarities with other third-generation centrifugal pumps regarding the design, principles of operation and speed control.
The national insurer offers reimbursement for LVAD implantation only as a bridge to HTx or candidacy and does not finance LVAD as a destination therapy or bridge to recovery. Furthermore, sacubitril-valsartan and the SGLT-2 inhibitors were not used as they were not reimbursed and their price was prohibitive.
Moreover, the relatively younger age of subjects undergoing LVAD in our country, compared with Western populations, could result in higher workload and VO2 values.
Conclusion
Ultrasonographic AVO analysis is possible during cycle ergometer stress test in patients with CF-LVAD.
Dynamic LVAD speed adjustment based on AVO augments peak VO2 consumption and maximal workload, and reduces perceived exertion in patients with CF-LVADs.
An automated speed adjustment in the next generation of CF-LVAD controllers might improve functional capacity and requires further basic, technological and clinical research.
Key messages
What is already known on this subject?
Current generation left ventricular assist devices (LVADs) operate with a fixed rotation speed without the capability of automated speed adjustment.
A gradual increase of the pump speed increases the maximum exercise tolerance during a stress test.
What might this study add?
This study shows a method of LVAD speed adjustment based on real-time echocardiographic imaging.
The intermittent aortic valve opening (AVO) was considered a surrogate for left ventricular unloading.
The pump speed was continuously altered to maintain periodic AVO during the cardiopulmonary exercise test. When the AVO ratio rose, the pump speed was increased; as the ratio decreased, the speed was lowered.
How might this impact on clinical practice?
This study adds the rationale for further research on pump control protocols based on continuous AVO monitoring as the proposed physiological approach boosted exercise capacity.
Supplemental material
Data availability statement
Data are available upon reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by Bioethics Committee of Jagiellonian University Medical College, Krakow, Poland (ID: 122.6120.256.2016). Participants gave informed consent to participate in the study before taking part.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @StaporMaciej
Contributors MS: Guarantor, conceptualisation, data curation, formal analysis, funding acquisition, investigation, methodology, project administration, resources, validation, visualisation, writing–original draft. AP: Conceptualisation, data curation, formal analysis, investigation, methodology, resources, software, validation, visualisation, writing–review and editing. AG: Conceptualisation, formal analysis, methodology, resources, validation, writing–review and editing. AM: Investigation. IG-K: Investigation. MK: Investigation. PK: Writing–review and editing. KZ: Supervision. JL: Funding acquisition, supervision, writing–review and editing. BK: Funding acquisition, supervision. KW: Conceptualisation, funding acquisition, investigation, methodology, project administration, resources, validation, writing–review and editing.
Funding This work was supported by the Cor Aegrum Foundation of Cardiac Surgery Development in Cracow, by an educational grant awarded by Medtronic Poland sp. z o.o., and by the Jagiellonian University, including a grant from the Polish Ministry of Science and Higher Education (N41/DBS/000732).
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting or dissemination plans of this research.
Provenance and peer review Not commissioned; internally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.