Article Text

Abstract
Objective Although recurring coronary artery spasm (CAS) may lead to the development of fixed atherosclerotic coronary stenosis (FS), the relationship between coronary atherosclerosis and CAS is still speculative. We evaluated the incidence of FS requiring percutaneous coronary intervention (PCI) in patients with documented CAS during long-term follow-up and analysed their clinical features.
Methods Clinical data of 3556 patients during a median follow-up of 9.4 years after non-invasive ergonovine spasm provocation testing with echocardiographic monitoring of left ventricular wall motion (erg echo) were analysed.
Results Erg echo documented CAS in 830 (23.3%) patients, who had higher frequencies of coronary risk factors than those without CAS. Patients with documented CAS on erg echo showed significantly lower 10-year overall (90.5% vs 94.2%, p<0.001) and PCI-free (97.4% vs 98.4%, p=0.002) survival rates than those without CAS. Documented CAS was an independent factor associated with later PCI after adjustment by either Cox regression model or Fine-Gray competing risk model. There was no significant difference in baseline clinical characteristics between patients who needed later PCI and those who did not. Among 28 patients who needed later PCI after documentation of CAS, the original CAS and later PCI territory were concordant in 25 (89.3%), while 3 (10.7%) showed discordance.
Conclusions CAS is a risk factor for the development of FS requiring PCI during long-term follow-up, and warrants physicians’ vigilance and careful follow-up of patients with documented CAS and insignificant stenosis of major epicardial coronary arteries at the time of initial diagnosis.
- percutaneous coronary intervention
- angina pectoris
- coronary stenosis
Data availability statement
Data are available upon reasonable request.
Statistics from Altmetric.com
Coronary artery spasm (CAS) is defined as an abnormal reversible vasoconstriction of an epicardial coronary artery that results in a transient reduction in the lumen diameter of sufficient degree to produce myocardial ischaemia. CAS plays an important role in the pathogenesis of variant angina and other clinical manifestations of coronary artery disease, including acute myocardial infarction and sudden cardiac death.1–3 Thus, in addition to organic fixed stenosis (FS) of an epicardial coronary artery due to atherosclerosis, dynamic coronary artery narrowing due to CAS has been accepted as an independent and important pathogenetic mechanism of coronary artery disease. The relative theoretical contribution of fixed (due to FS) and dynamic (due to CAS) coronary artery narrowing has been suggested to explain the wide clinical spectrum of myocardial ischaemia.1 Moreover, it has been suggested that recurring CAS may lead to the development of FS.4–7 However, the relationship between coronary atherosclerosis and CAS is still speculative.8
There are several clinical studies on the long-term clinical outcomes of patients with variant angina with documented CAS, but these were mainly focused on survival rates and not on the development of significant FS requiring percutaneous coronary intervention (PCI).9–12 These studies were conducted in the era before the widespread clinical application of calcium channel antagonists,9 10 which are powerful prognostic determinants in patients with documented CAS. In addition, several studies had a relatively short follow-up duration of less than 5 years,9 10 and a significant proportion of patients (38%–92%) had both significant FS in epicardial coronary arteries and CAS.9–12 Thus, an appropriate evaluation of the potential contribution of CAS to the progression of atherosclerotic stenosis of an epicardial coronary artery was not possible. Accordingly, the purpose of the current study was to assess the frequency of the development of significant FS requiring PCI during long-term clinical follow-up in patients with documented CAS and insignificant stenosis of major epicardial coronary arteries at the time of initial diagnosis and who received appropriate medical management including calcium channel antagonists.
Methods
Subjects
Patients who underwent non-invasive ergonovine spasm provocation testing with echocardiographic monitoring of left ventricular wall motion (erg echo) between January 1991 and December 2015 at our institution were identified. In patients with clinical presentation of chest pain syndrome, aborted sudden cardiac death or syncope suggestive of significant coronary artery disease, the initial diagnostic work-up was to rule out significant FS of the major epicardial coronary artery, and if anatomic test (CT or coronary angiography) or non-invasive functional test (treadmill or myocardial perfusion scan) would not show any evidence of significant FS an erg echo is indicated to exclude the possibility of CAS (figure 1).13 The most common clinical situation or presentation for undergoing a diagnostic test for CAS is chest pain syndrome, which includes variant angina (anginal pain attack during sleep or early morning usually not associated with increased myocardial oxygen demand), effort angina and atypical angina. Other clinical diagnoses include acute coronary syndrome, syncope and aborted sudden cardiac death.14

Flow diagram of the study. CAG, coronary angiography; CAS, coronary artery spasm; erg echo, ergonovine echocardiography; PCI, percutaneous coronary intervention.
A total of 8649 patients underwent erg echo between January 1991 and December 2015 at our institution. Among them, 5093 patients who underwent functional test to rule out significant FS before erg echo were excluded as imaging data of the epicardial coronary artery were not available. Patients who underwent non-invasive CT angiography (n=1028) or invasive coronary angiography (n=2528) to rule out the possibility of significant FS of major coronary arteries before erg echo were selected (figure 1). We excluded patients with coronary lumen diameter stenosis of >50% on either non-invasive or invasive angiography, resting wall motion abnormality, or poor echocardiographic window before erg echo. The positive criteria for erg echo included the appearance of transient ST segment elevation or depression of >0.1 mV at 0.08 s after the J point and reversible regional wall motion abnormality shown on two-dimensional echocardiography. Patients with documented CAS during index erg echo were recommended to take medications, including calcium channel antagonists, with regular outpatient-based follow-up.
Data extraction
Dedicated research nurses and physicians filled a systematic case report form that included demographic information, blood test results, screening test results for ruling out significant FS of the epicardial coronary artery, clinical data of erg echo and medications. The primary endpoint was the development of significant FS requiring PCI after index erg echo during long-term follow-up. Later PCI during follow-up was clinically driven at the discretion of the caring physicians. The secondary endpoints included all-cause mortality, cardiovascular mortality, and major adverse cardiovascular events (MACE) at 10 years. Clinical follow-up data were included with special attention to hospital admission for later PCI. In addition, vital status and cause of death were cross-checked using data from the National Population Registry of the Korean National Statistical Office. There were no missing clinical data. MACE were defined as the composite of all-cause mortality, myocardial infarction, stroke and later PCI.
Statistical analysis
Continuous variables are reported as mean±SD and categorical variables are reported as counts (percentages). Group comparisons were performed with Student’s t-test and χ2 test. Survival curves were constructed using Kaplan-Meier estimates and compared with the log-rank test. The entire follow-up duration was used to analyse the time-to-event outcomes, and patients were censored at the time of later PCI or last available follow-up. The multivariable Cox proportional hazards regression model was used to determine predictors of later PCI. The model included age, sex, hypertension, diabetes mellitus, dyslipidaemia, smoking, history of PCI and documented CAS on erg echo. No relevant multicollinearity between variables assessed by the variance inflation factor values was found. The proportional hazards assumption was confirmed using Schoenfeld residual test; no relevant violations of the underlying assumption were found. Furthermore, as the number of deaths substantially exceeded the number of later PCI events, to adjust this competing event, subdistribution hazard ratio (HR) for the primary endpoint was estimated using the Fine-Gray competing risk model with all-cause death and cardiovascular death as a competing outcome. All statistical analyses were performed using IBM SPSS Statistics V.22.0 and SAS V.9.4. P<0.05 was considered statistically significant.
Results
This retrospective cohort included 3556 patients who underwent erg echo between January 1991 and December 2015 at our institution, of whom 830 (23.3%) were documented to have CAS according to the erg echo (figure 1). Patients with CAS had higher prevalence of male sex (71.1% vs 50.2%, p<0.001), dyslipidaemia (37.7% vs 29.3%, p<0.001), smoking (49.5% vs 29.0%, p<0.001) and history of PCI (4.6% vs 1.3%, p<0.001) than those without CAS (table 1).
Comparison of baseline characteristics according to the presence of coronary artery spasm
During a median clinical follow-up duration of 9.4 years (IQR: 5.8–15.1), a total of 376 patients died during follow-up (10-year mortality rate of 5.3%) and later PCI was performed in 62 (1.7%; 10-year incidence rate of 1.3%) patients at a median of 7.9 years (IQR: 2.0–10.0) after index erg echo (figure 2 and table 2). Figure 2 describes a representative case who underwent later PCI after documentation of CAS on index erg echo. The cumulative incidence of later PCI was significantly higher in patients with CAS than in those without (log-rank p=0.002; figure 3A). Documented CAS was an independent factor associated with later PCI after adjustment by either the Cox regression model or the Fine-Gray competing risk model (table 3). The 10-year cumulative incidence of the secondary endpoints was also significantly higher in patients with documented CAS (figure 3).

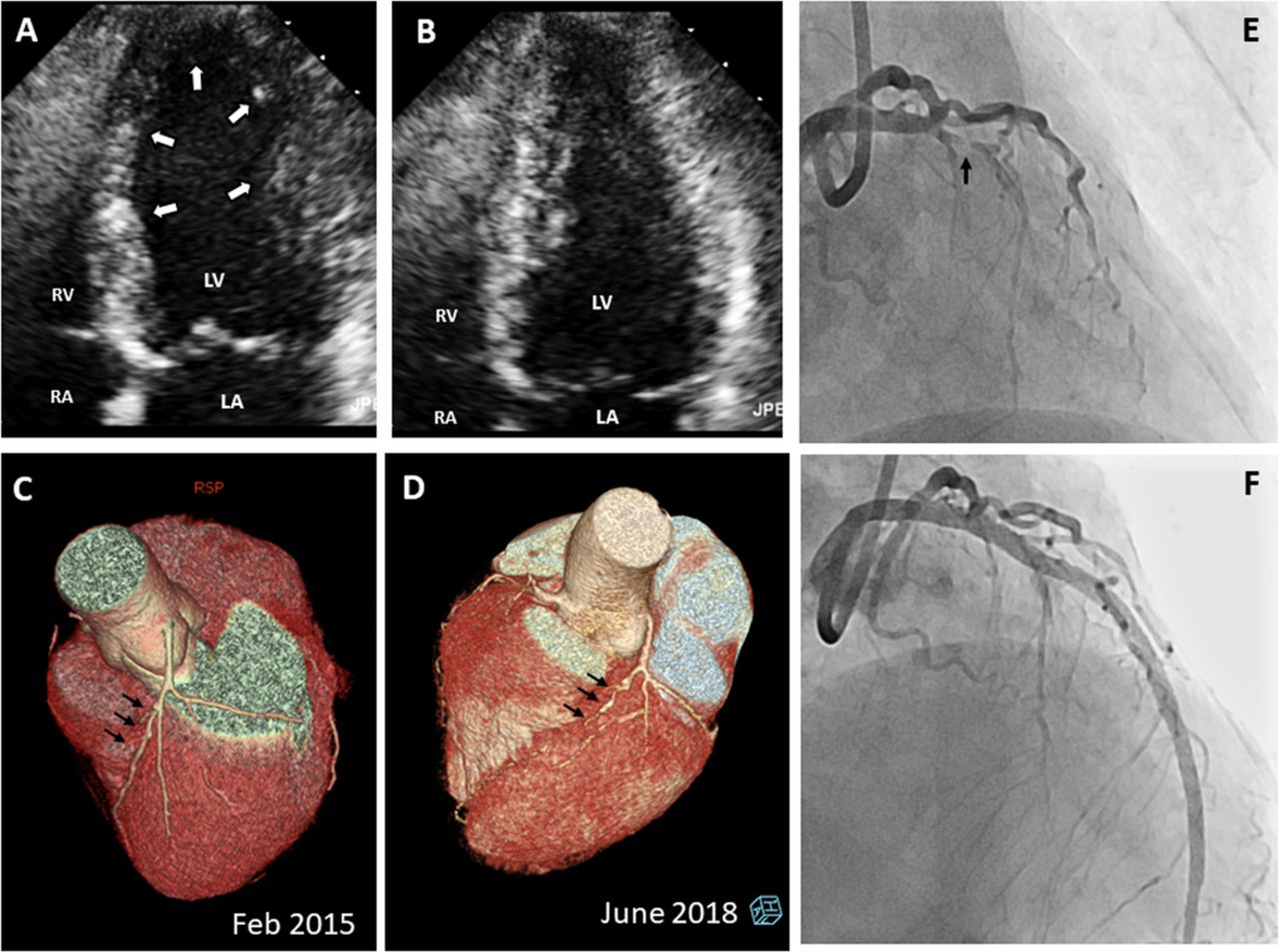
A representative case who developed significant fixed stenosis after confirmation of coronary artery spasm during clinical follow-up. This patient underwent ergonovine echocardiography, which showed the development of regional wall motion abnormality (white arrows) in the LAD territory on the end-systolic image (A) and reversal with nitroglycerin injection (B). Prior to index ergonovine echocardiography, CT coronary angiography did not show significant atherosclerotic fixed stenosis (C) at LAD (arrows). A calcium channel antagonist, statin and nitrates were prescribed and regular follow-up was recommended. Three years later, the angina had worsened despite regular medication and total occlusion of LAD (arrows) was diagnosed on CT coronary angiography (D). Percutaneous coronary intervention was successfully performed in this patient (E and F). LAD, left anterior descending coronary artery; LA, left atrium; LV, left ventricle; RA, right atrium; RV, right ventricle.

{kind=link}
{kind=link}
{kind=link}
Cumulative incidence of the primary and secondary endpoints. Cumulative incidence estimates for later PCI according to the presence of coronary artery spasm (A), for all-cause mortality (B), and for cardiovascular mortality (C). Major adverse cardiovascular events (D) were defined as all-cause mortality, myocardial infarction, stroke and later PCI. CAS, coronary artery spasm; PCI, percutaneous coronary intervention.
Summary of the primary and secondary endpoints
Crude and adjusted HR for the primary endpoint
Among patients with CAS, there was no significant difference in baseline clinical characteristics including atherosclerotic risk factors between patients who needed PCI (n=28) and those who did not (n=802; online supplemental table 1). CAS territory on erg echo (left anterior descending artery (LAD) vs non-LAD) was not significantly associated with the development of significant FS that required later PCI (HR 2.05, 95% CI 0.95 to 4.45, p=0.069). Clinically driven later PCI during follow-up was documented in 28 patients with CAS, and clinical presentation included worsening angina despite medication (n=17, 60.7%), non-ST segment elevation (n=4, 14.3%) and ST segment elevation myocardial infarction (n=2, 7.1%), and the remaining 5 (17.9%) asymptomatic patients who showed the development of FS on follow-up non-invasive CT coronary angiography without chest pain (online supplemental table 2). The most common territory of later PCI in patients with documented CAS was the LAD territory (n=14, 50.0%), followed by a non-LAD territory in 9 (32.1%); the remaining 5 (17.9%) patients needed PCI in both LAD and non-LAD territories (online supplemental table 3). In 28 patients who needed PCI during follow-up, 18 showed CAS in the LAD territory on index erg echo, whereas the remaining 10 showed CAS in the non-LAD territory. Among these 28 patients, the original CAS and PCI territory were concordant in 25 (89.3%), while 3 (10.7%) showed discordance; the concordance rate between CAS and PCI territory was not significantly different according to the territory of documented CAS on index erg echo (88.9% vs 90.0%, p=1.000).
Supplemental material
Discussion
In this retrospective cohort study characterised by the absence of significant FS at the time of spasm provocation test and the longest clinical follow-up duration in the literature, the overall prognosis was quite favourable with routine use of calcium channel blockers. However, the development of significant FS requiring later PCI was noted in a subset of patients for which documented CAS was a significant independent risk factor. Although most patients with later PCI developed chest pain suggestive of worsening angina or acute coronary syndrome despite medications, more than 10% of those who needed later PCI had developed significant FS without symptoms. As baseline risk factors could not predict the development of significant FS, careful follow-up and education of patients with documented CAS and insignificant stenosis of major epicardial coronary arteries at the time of initial diagnosis are warranted to facilitate the diagnosis of the rare development of significant FS and to achieve better clinical outcomes.
CAS and atherosclerosis progression
In the late 1970s and early 1980s, spasm provocation testing was accepted as a routine step for differential diagnosis of chest pain15–17 and numerous studies had been conducted to establish an appropriate positioning and clinical significance of CAS in the wide clinical spectrum of coronary artery disease. Particularly, the potential association between CAS and the progression of coronary atherosclerosis received significant interest. Several animal experiments demonstrated mechanical injury to the endothelium by spasm-induced platelet aggregation, thrombus formation and local release of vasoconstricting substances perpetuating vascular spasm, which ultimately leads to arterial occlusion at the spastic site.18–20 These observations supported the idea of atherosclerotic stenosis progression by CAS as a consequence of endothelial damage. Clinical cases with a rapid angiographic progression of FS at the spastic site have been reported,4 7 21 22 and intimal proliferation of smooth muscle cells superimposed on the fibrous cap of atherosclerotic plaques was also demonstrated. However, a cause–effect relationship could not be accurately assessed by histological findings alone as these lesions could be ‘innocent bystanders’ indicative of the presence of an atherosclerotic process and not necessarily responsible for the coronary hyper-reactivity that causes CAS.
Kaski et al 23 analysed repeated coronary angiography in 10 patients with typical variant angina and angiographically documented CAS and showed that stenosis progression was not frequently observed at the spastic sites despite the recurrence of focal CAS; although interesting, this study had a small number of patients with recurrent angina and a short follow-up duration (25±12 months). In addition, progression of atherosclerotic stenosis was evaluated by measurement of the arterial diameter on coronary angiogram and the progression in stenosis severity was defined using arbitrary cut-off values of luminal diameter stenosis (≥20% in a pre-existing stenosis of ≥50% or ≥30% in a stenosis <50%). Thus, the clinical significance of stenosis progression in Kaski et al’s23 study is limited, and more concrete clinical events associated with atherosclerosis progression are needed to better delineate the potential role of CAS in the progression of atherosclerotic stenosis in coronary artery diseases.
To overcome these limitations, we evaluated the development of more clearly defined clinical event (ie, FS requiring PCI) in patients with documented CAS during long-term clinical follow-up. Table 4 summarises the key findings of previous clinical studies on the long-term prognosis of patients with documented CAS.9–12 Traditionally, the survival of patients with CAS was associated with the disease activity of CAS, as determined by the frequency of anginal attack, resting left ventricular function and the degree of FS in major epicardial coronary arteries.24 Previous studies included patients with significant FS at the time of CAS diagnosis, and several studies suggested coronary artery bypass graft (CABG) surgery as a necessary treatment option in patients with documented CAS.9–11 In previous reports, the prevalence of CABG in patients with documented CAS in both the acute phase and during clinical follow-up ranged from 9.4% to 43%. These studies were mainly conducted in Western countries and represent relatively early clinical data without widespread use of calcium channel antagonists. As well demonstrated by Yasue et al,12 successful clinical introduction of calcium channel blockers significantly improved the survival rates of patients with documented CAS. It is interesting to see that CABG was no longer recommended or performed in patients with documented CAS following the widespread use of calcium channel blockers, a trend that was also evident in the current study.
Key findings of major previous studies on the long-term outcome of patients with documented coronary artery spasm
Both the Japanese study and our study showed that despite the excellent long-term prognosis of patients with CAS, later PCI was occasionally performed during long-term clinical follow-up, which warrants clinical attention. In the Japanese study, in which 60% of patients had a significant FS at the initial time of CAS diagnosis, the frequency of later PCI was 2%; in contrast, the frequency of later PCI was 3.6% in our study only including patients without any significant FS before spasm provocation test. Absence of significant FS at the time of CAS documentation did not preclude the necessity of later PCI during long-term clinical follow-up. Moreover, we showed that the prevalence of PCI was significantly higher in patients with documented CAS than in those without, which suggests that CAS itself is an independent factor associated with later PCI.
Spontaneous remission of CAS has been reported in previous clinical studies,25–27 which had been used as a rationale for short-term antianginal medication for this ‘relatively benign form of angina’. However, even in patients with CAS and normal coronary arteries without FS, the rate of early mortality has been reported to be outside an acceptable range,1 and several patients were documented to have suddenly expired after stopping their medication on their own because they thought they were cured of the ailment following a long period without attacks.28 It is not uncommon for patients with documented CAS to have prolonged remissions followed by new episodes of resting chest pain, suggesting a typical cyclic variation of symptoms.1 The development of FS requiring PCI even with calcium channel antagonists demonstrated in our study strongly supports careful clinical follow-up with special attention on the development of FS. The high concordance rate between the coronary territory with documented CAS and that with later PCI is remarkable; however, it should be noted that the territory between documented CAS and later PCI was different in about 10%. In addition, baseline characteristics at the time of CAS documentation were not useful in predicting later PCI, which emphasises the importance of the attending physicians’ vigilance during follow-up as well as the education of patients with documented CAS.
Limitations
As this is a retrospective study in a single centre without predetermined follow-up protocol and full medication information including antiplatelet medications, our observations cannot be confirmatory. Absence of angiographic comparison between the CAS site and later PCI site does not allow to conclude that CAS is the mechanism responsible for the development of FS. Racial heterogeneity in coronary vasomotor reactivity has been well demonstrated, with Japanese patients showing a higher incidence of inducible spasm after a myocardial infarction than Caucasian patients.29 In addition, a lower prevalence of FS and a higher incidence of diffuse coronary hyper-reactivity in Japanese patients have also been reported. As our study cohort is characterised by the absence of patients with significant FS at the time of CAS documentation, our findings and their clinical implication cannot be easily generalised. In addition, considering the fact that diagnosis of CAS is made less commonly now than three decades ago in Western countries, the clinical implication of our observational findings may be limited. However, despite the less frequent use of spam provocation tests in Western countries, there are several reports showing that CAS is still commonly prevalent even among Caucasians in Western countries.30 Further investigations in different populations are necessary to define the potential association between CAS and atherosclerosis progression and its clinical implication.
Clinical implications
Despite the high survival rates of contemporary patients with documented CAS with widespread usage of calcium channel antagonists, significant FS requiring later PCI occasionally occurred during long-term follow-up in patients with documented CAS and insignificant stenosis of major epicardial coronary arteries at the time of initial diagnosis. Moreover, CAS was found an independent factor associated with requirement of later PCI. As there are no solid biomarkers for the development of significant FS, careful follow-up and education of patients with documented CAS are warranted.
Key messages
What is already known on this subject?
It has been suggested that recurring coronary artery spasm (CAS) may lead to the development of atherosclerotic fixed stenosis (FS) of an epicardial coronary artery, but the relationship between coronary atherosclerosis and CAS is still speculative.
What might this study add?
Documented CAS in patients with insignificant stenosis of major epicardial coronary arteries at the time of initial diagnosis is an independent risk factor associated with the development of significant FS requiring percutaneous coronary intervention during long-term follow-up.
How might this impact on clinical practice?
As baseline risk factors could not predict the development of significant FS, physicians’ vigilance with careful follow-up and education of patients with documented CAS and insignificant stenosis of major epicardial coronary arteries at the time of initial diagnosis are warranted to facilitate the diagnosis of the rare development of significant FS and to achieve better clinical outcomes.
Data availability statement
Data are available upon reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by the Asan Medical Center IRB (2016-0509). Our institutional review board approved the protocol of this retrospective study and waived the requirement for informed consent.
Acknowledgments
The authors thank Dr Joon Seo Lim from the Scientific Publications Team at Asan Medical Center for his editorial assistance in preparing this manuscript. They also thank Dr Sung-Cheol Yun from the Department of Biomedical Statistics at Asan Medical Center for his assistance in statistical analysis.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors JHK, JP and YY participated in the study design and analysis and interpretation of the final data, as well as in the drafting and approval of the final manuscript. SL, D-HK, J-MS, S-WP, D-HK and S-JP were involved in the recruitment of participants from clinics. J-KS was the guarantor and responsible for the design and supervision of the study and revision of the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.