Article Text

Statistics from Altmetric.com
With rapidly ageing population, aortic stenosis (AS) has become one of the most common valvular heart diseases. Severe AS is clearly associated with increased mortality, and the current American College of Cardiology/American Heart Association guidelines designate a class I or IIa indication for aortic valve surgery in severe patients with AS with symptoms or with low left ventricular (LV) function.1 Historically, based on the lower risk of sudden death in moderate AS compared with severe AS, watchful observation was recommended to patients with moderate AS. In the last decade, prognostic findings on moderate AS have been gathered (table 1).2–4 A large echocardiographic national database study, including 3315 moderate AS with various LV systolic functions, suggested a poor survival rate (5-year mortality: 56%).4 Recently, two academic institutional databases, including 1245 moderate AS, also showed poor prognosis during follow-up (median follow-up: 4.3 years; mortality: 45.3%).3
Prognosis of moderate aortic stenosis
From a physiological viewpoint, narrowing of the aortic valve area leads to LV systolic/diastolic dysfunction due to LV pressure overloading. In patients with severe AS who particularly underwent transcatheter aortic valve replacement (TAVR), diastolic dysfunction (DD) has been described as an early marker of myocardial damage and an important prognostic information. Thaden et al 5 reported an association between echocardiographic data and outcomes from a retrospective single-centre study. Over a mean follow-up period of 7.3 years, increased left atrial pressure based on the American Society of Echocardiography/European Association of Cardiovascular Imaging criteria remained an independent predictor of mortality after successful aortic valve replacement (AVR) (HR: 1.45; 95% CI 1.16 to 1.81). More recently, Ong et al 6 clearly showed an association between DD grading at baseline and combined cardiovascular death/rehospitalisation at 1 year from the Placement of Aortic Transcatheter Valves (PARTNER) 2 and SAPIEN 3 registry analysed by core laboratories (n=1253). These previous studies described a consistent message of an increased risk of event with worsening grade and stage of DD in severe AS.
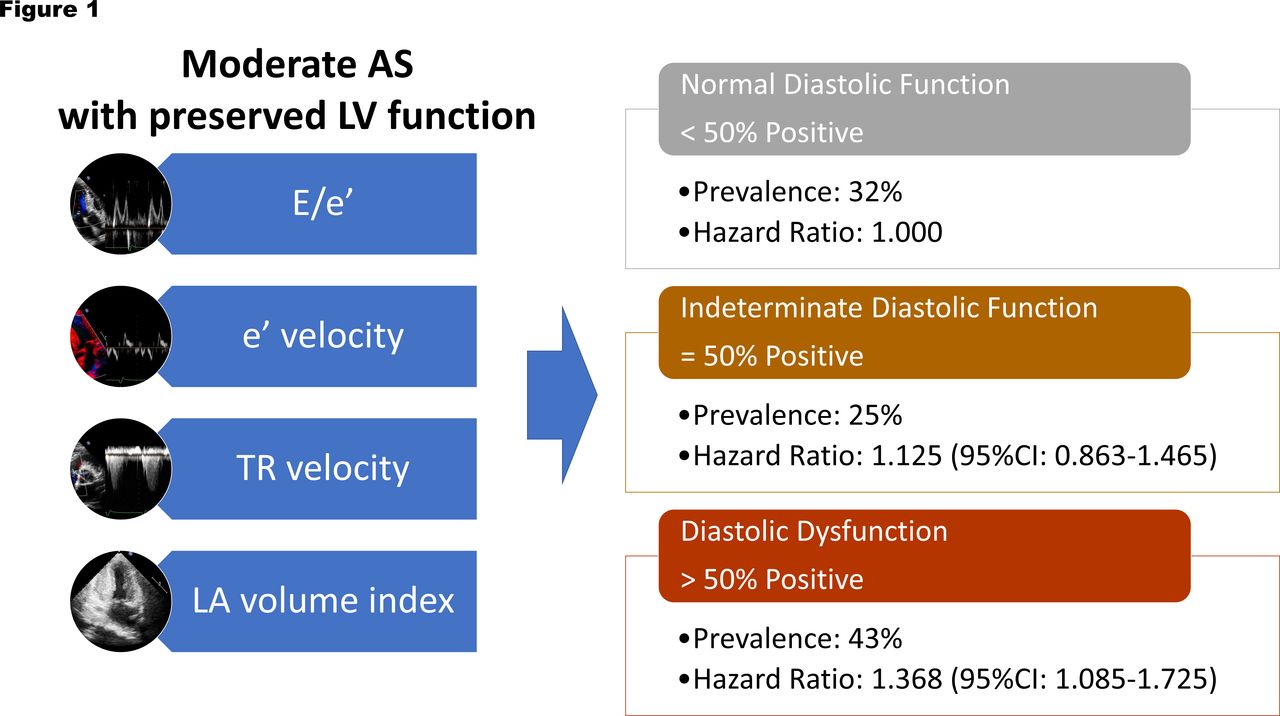
What about the association of moderate AS with DD? In their Heart article, Stassen et al 2 presented data from a large registry of patients with moderate AS and preserved LV systolic function from three academic institutions between October 2001 and December 2019. Moderate AS was defined as an aortic valve area of between 1.0 cm2 and 1.5 cm2. Finally, 1247 patients with moderate AS were retrospectively included and divided into three groups (normal diastolic function, indeterminate diastolic function and DD) based on the guidelines. The aims of the study were (1) to evaluate the prevalence of DD and (2) to examine the prognostic implications of DD in moderate AS with preserved LV systolic function. The primary outcome was all-cause mortality. The secondary outcome was a composite of all-cause mortality and surgical or transcatheter AVR. The results showed DD was frequently present in patients with moderate AS (normal diastolic function: 32%; indeterminate diastolic function: 25%; DD: 43%). Over a median follow-up of 53 months, 39% of the patients died. The survival rate was 91% at 1 year and 65% at 5 years. The presence of DD was independently associated with all-cause mortality (HR: 1.37; 95% CI 1.09 to 1.73) and the composite endpoint of all-cause mortality and AVR (HR: 1.24; 95% CI 1.04 to 1.49) after adjustment for several clinical variables (figure 1).
{kind=link}
Prevalence and HR of diastolic dysfunction in moderate AS. AS, aortic stenosis; LA, left atrial; LV, left ventricular; TR, tricuspid regurgitation.
The strengths of the study are the large sample size and the well-designed data collection. The main limitations of the study include the retrospective nature of the analysis and the lack of a validation cohort. Moreover, a major limitation in the assessment of DD is that there are many indeterminate cases using the guideline algorithm. Patients with indeterminate DD were not associated with higher event-free survival compared with patients with normal diastolic function. Moreover, individual variables for assessment of LV diastolic function (E/e’, left atrial volume index and tricuspid regurgitation velocity) were not as highly associated with the outcomes. Because there are some limitations in the guideline algorithm, we need supplementary methods to determine the presence or absence of DD. After the introduction of strain imaging, it became clear that patients with normal left ventricular ejection fraction may have mildly reduced LV systolic function by global longitudinal strain. Therefore, LV strain imaging represents a supplementary test and is useful when echocardiographic indices of diastolic function are inconclusive. Tastet et al 7 showed that the new staging system characterised the extra-aortic valve cardiac damage using several parameters, including global longitudinal strain, in AS. Strain imaging may contribute to the additional value to the DD grading system in moderate AS with preserved LV systolic function. The lack of cardiac magnetic resonance data was another limitation because of not excluding cardiac amyloidosis in this cohort. Around 30% of the patients have diuretics and around 40% were of New York Heart Association class II–IV. Around half of this cohort seem to be patients with moderate AS with high prevalence of symptoms. Atrial fibrillation (AF) was relatively prevalent in this cohort (25%) and it is unclear how patients with AF were assessed. Variation in echocardiographic examinations of patients with AF among the three institutes might affect the results. During a median follow-up of 53 months, progression of AS severity can be expected in patients with an initial diagnosis of moderate AS. Although this is a cross-sectional study evaluating the prognostic significance of different types of DD at the time of diagnosis of moderate AS, it is not clear whether progression to severe AS contributed to mortality during follow-up. The impact of AS progression on mortality needs to be clarified in future investigations.
Underlying this study is the idea that patients with DD may be eligible for early AVR intervention. Thus, further study on early AVR versus conventional approach using the definition of patients at risk based on DD should be planned. The TAVR UNLOAD (Transcatheter Aortic Valve Replacement to Unload the Left Ventricle in Patients with Advanced Heart Failure; NCT02661451) is an ongoing trial to test whether patients with moderate AS with reduced LV systolic function benefit from earlier valvular intervention compared with the current guideline-recommended medical therapy. The PROGRESS (Prospective, Randomized, Controlled Trial to Assess the Management of Moderate Aortic Stenosis by Clinical Surveillance or Transcatheter Aortic Valve Replacement; NCT04889872) trial is also ongoing and randomises patients with moderate AS with various LV systolic functions to TAVR or to clinical surveillance for composite outcomes. The results of these trials will provide information on whether AVR could have clinical usefulness in patients with moderate AS.
Surgical interventions for severe AS have improved, while treatment and prognosis of moderate AS have not changed. Traditionally considered benign, moderate AS has been associated with significant cardiovascular disease and mortality in large observational studies. Detection of higher-risk moderate AS cases may be a useful option for early intervention. Among the many clinical parameters, DD might be a red flag sign of a cohort at high risk of moderate AS. However, individual variables for assessment of LV diastolic function (E/e’, left atrial volume index and tricuspid regurgitation velocity) were not as highly associated with the outcomes. Multifactorial influences should be considered in managing moderate AS. Based on the data from Stassen et al,2 it seems important to combine multiple indicators, including image-based and biochemical parameters, when considering treatment strategies for moderate AS.
Ethics statements
Patient consent for publication
Footnotes
Contributors KK is the sole author of this editorial.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Commissioned; externally peer reviewed.