Article Text

Abstract
Objective Non-bacterial thrombotic endocarditis (NBTE) is a syndrome characterised by cardiac valve vegetations and/or thickening due to non-infective mechanisms. Nowadays, a premortem diagnosis of NBTE is possible based on echocardiographic findings. Therefore, to better characterise this disease, we performed a contemporary review of the epidemiology, demographics, diagnosis and clinical outcomes of these patients.
Methods Adults with a diagnosis of NBTE seen within the Mayo Clinic Enterprise from December 2014 to December 2021 were included. NBTE diagnosis was identified by clinicians representing at least two specialties including cardiology, infectious diseases, rheumatology and oncology. Patients with positive blood cultures, infective endocarditis, culture-negative endocarditis and denial of research authorisation were excluded. All patients had a 1-year follow-up.
Results Forty-eight cases were identified; mean age was 60.0±13.8 years, 75% were female. The most prevalent comorbidities were malignancy (52.1%) and connective tissue disease (37.5%). Valvular abnormalities included 41 (85.4%) patients with vegetations, 43 (89.6%) patients with thickening and 26 (54.2%) with moderate to severe regurgitation. Thirty-eight (79.2%) patients had an embolic event (stroke in 26 (54.2%) patients) within 1 month of NBTE diagnosis and 16 (33.3%) patients died within 1 year of NBTE diagnosis. Metastatic tumours and lung cancer were associated with 1-year all-cause mortality (p=0.0017 and p=0.0004, respectively).
Conclusions NBTE was more prevalent in females and embolic complications were the most frequent clinical finding. Overall, patients with NBTE had a poor prognosis, particularly in those with lung cancer or metastatic tumours. Further studies in patients with NBTE are needed given its morbidity and mortality.
- Echocardiography
- Endocarditis
Data availability statement
Data may be obtained from a third party and are not publicly available. The data underlying this article cannot be shared publicly because the privacy of the individuals who participated in the study must be maintained and because the data underlying this article were provided by Mayo Clinic under licence and by permission. The data will be shared at reasonable request to the corresponding author with the permission of Mayo Clinic.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Non-bacterial thrombotic endocarditis (NBTE) is a non-infectious condition characterised by thrombotic and/or inflammatory depositions involving cardiac valves.
WHAT THIS STUDY ADDS
NBTE was three times more common in females than males, and embolic events were the most frequent (79.2%) clinical finding. Malignancy (52.1%) and connective tissue disease (37.5%) were the most prevalent conditions in NBTE. Overall, 30% of patients died within 1 year of NBTE diagnosis, and those with lung cancer and metastatic disease had a higher mortality.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE AND/OR POLICY
NBTE is a challenging diagnosis which requires ruling out other diseases, particularly infective endocarditis. If NBTE is suspected, then it is crucial to assess several features that include demographics, comorbid conditions, embolic complications and echocardiographic findings. This work may facilitate an early diagnosis of NBTE to potentially prevent the common devastating sequela of stroke.
Introduction
Non-bacterial thrombotic endocarditis (NBTE), also known as marantic or Libman-Sacks endocarditis, is a syndrome characterised by cardiac valve thickening and/or vegetations due to non-infective mechanisms. The exact pathogenesis of this disease is unknown; nevertheless, it is theorised that factors such as immune complexes, hypoxia, hypercoagulability and carcinomatosis are associated with the initiation of NBTE.1 2 Concordantly, procoagulant and inflammatory conditions including advanced malignancies, systemic lupus erythematosus (SLE) and antiphospholipid antibody syndrome (AAS) have been associated with this syndrome.1–3
This disease was first described by Ziegler in 1888 as a deposition of fibrin on cadaveric cardiac valves.4 For many decades, postmortem examinations were required to diagnose NBTE. This changed in 1976, more than 20 years after the invention of M-mode echocardiography by Edler and Hertz when the first report describing the use of transthoracic echocardiogram (TTE) to diagnose NBTE was published.5 6 Currently, a premortem diagnosis of NBTE is possible based on echocardiographic findings.
Diagnosing NBTE through non-invasive techniques has positively influenced the prognosis of many patients who are now able to receive treatment.7 8 Understanding the epidemiology, demographics, diagnostics and clinical outcomes of patients with NBTE is critical in patient management, but, unfortunately, most of our understanding is based on postmortem studies which do not apply to patients currently. Moreover, a comparison of both TTE and transoesophageal echocardiography (TOE) in NBTE has been limited with only a single study published in 2008 which compared the sensitivity of TTE versus TOE in a cohort of patients with SLE.9
Therefore, the primary aim of this study is to provide an updated descriptive review of the epidemiology, demographics, diagnosis and outcomes of patients with NBTE. The secondary aim is to evaluate the ability of TTE in detecting NBTE abnormalities as compared with that of TOE.
Methods
We queried institutional databases for medical records of patients with a diagnosis of NBTE at any Mayo Clinic site (Rochester, Florida, Arizona and the Health Systems) from December 2014 to December 2021. Complete review of the medical records was performed. NBTE cases were identified if there was an agreement between two or more different specialties including cardiology, infectious diseases, rheumatology and oncology. NBTE was defined by echocardiographic abnormalities that included valvular thickening, regurgitation and/or vegetations. In addition, the diagnosis of NBTE was confirmed after excluding patients with positive blood cultures, infective endocarditis or patients with evidence of culture-negative endocarditis based on serological and/or molecular assays. Patients with denial of research authorisation, and aged <18 years old at the time of NBTE diagnosis were excluded. A total of 48 NBTE cases were eligible for inclusion (figure 1). All patients had either visits, questionnaires or script-based telephone communication after first year of NBTE diagnosis, except for those who died.

Selection flow chart demonstrating NBTE cases. NBTE, non-bacterial thrombotic endocarditis; TOE, transoesophageal echocardiogram; TTE, transthoracic echocardiogram.
Echocardiographic reports, clinical characteristics, comorbidities and outcomes (at the time of NBTE diagnosis) were collected from electronic health records.
Echocardiographic evaluation
Echocardiographic examinations were conducted according to the American Society of Echocardiography guidelines and interpreted by an experienced attending physician responsible for the report.10 11 All patients underwent TTE and/or TOE, of them, 20 had a TTE with a subsequent TOE in less than 72 hours; we used the latter patients as their own controls to compare the ability of TTE versus TOE in detecting NBTE-related abnormalities.
Statistical analyses
All data were analysed using JMP statistical software, V.14.1.0 (SAS Institute, Cary, North Carolina, USA). The Shapiro-Wilk test was used for testing the normality of the data. Patients’ characteristics are summarised for NBTE cases with mean±SDs for continuous variables and with number and percentage for categorical variables. Comparison among variables was performed with Student’s t-test or Mann-Whitney test for quantitative variables and with Χ2 test or Fisher’s exact test for qualitative variables, as appropriate. The Kaplan-Meier method was used to determine all-cause mortality event-free survival rate, and differences between groups were assessed with the log-rank test. A p value of <0.05 was considered statistically significant.
Patient and public involvement
Patients or the public were involved in the design, or conduct, or reporting, or dissemination plans of our research.
Results
Forty-eight patients with NBTE were identified and 20 (41.7%) of them had a TTE followed by a TOE within 72 hours. Overall, the mean age was 60.0±13.8 years, and 36 (75%) patients were female (table 1). The majority were white, non-Hispanic or Latino (87.5%). The most prevalent comorbidities were malignancy (52.1%), connective tissue disease (CTD) (37.5%), hypertension (37.5%), diabetes mellitus (35.4%), myocardial infarction (27.1%) and AAS (22.9%). SLE (25.0%), scleroderma (4.2%), Sjogren syndrome (4.2%), rheumatoid arthritis (2.1%) and spondylitis ankylosing (2.1%) were included as part of CTD. Cancer metastasis was identified in 10 (20.8%) patients: 8 (16.7%) originated from lung cancer and 2 (4.2%) from ovarian cancer.
Clinical characteristics and comorbidities in patients with NBTE
Clinical characteristics and comorbidities were similar for the 48 cases as compared with that of the subset of 20 patients who had undergone both TTE and TOE.
Twenty-six (54.2%) patients had a TTE, and 44 (91.7%) patients had a TOE. Reported echocardiographic measurements represent TOE findings except for four cases which only had a TTE. The reasons TOE was not performed were patient refusal (n=1), poor prognosis (n=2) and TOE was not ordered (n=1). Overall, 41 (85.4%) patients had a vegetation; the mitral valve was the most frequently affected (n=26; 54.2%), followed by the aortic valve in 20 (41.7%), tricuspid valve in 3 (6.3%) and pulmonary valve in 1 (2.1%). Valvular thickening was present in 43 (89.6%) patients and involved the mitral valve in 34 (70.8%), followed by aortic in 27 (56.3%), tricuspid in 6 (12.5%) and pulmonary in 3 (6.3%). Mild to severe regurgitation was present in 40 (83.3%) patients while moderate to severe regurgitation in 26 (54.2%) patients (online supplemental table 1). Thirty-five (72.9%) patients had a vegetation involving one valve, four (8.3%) involving two valves, one (2.1%) involving three valves and one (2.1%) involving four valves. Twenty-three (47.9%) patients had thickening involving one valve, 16 (33.3%) involving two valves, 2 (4.2%) involving three valves and 2 (4.2%) involving four valves. Nineteen (39.6%) patients had moderate to severe regurgitation involving one valve and seven (14.6%) involving two valves.
Supplemental material
Forty-one (85.4%) patients were diagnosed based on findings of valvular vegetations with/without thickening and regurgitation. Seven (14.6%) patients were diagnosed based on valvular thickening of which five (10.4%) had associated moderate to severe regurgitation of the same valve (online supplemental table 2). The remaining two patients without moderate to severe regurgitation or vegetations had a marked thickening of cusp edges and leaflet tips with ‘stuck on’ or ‘kissing appearance’ (figure 2).

Transoesophageal echocardiographic images of non-bacterial thrombotic endocarditis. (A) Zoomed mid-oesophageal four-chamber view in systole showing a thickened mitral valve with stuck-on kissing lesions on the leaflet tips (arrow). (B) Zoomed mid-oesophageal five-chamber view in diastole illustrating the stuck-on kissing lesion on the anterior mitral valve leaflet tip (arrow). (C) Zoomed mid-oesophageal two-chamber view in diastole depicting the stuck-on kissing lesion on the tip of the posterior mitral valve leaflet (arrow).
The sensitivity and specificity of TTE to detect NBTE abnormalities in 20 patients where TOE was considered gold standard are presented in table 2. TTE identified thickening in 20 (66.7%) valves out of 30 detected by TOE. Mitral valve thickening was detected in 12 (80.0%) of 15 patients and aortic valve thickening in 8 (72.7%) of 11 patients, respectively. TTE identified vegetations in 10 (47.6%) valves of 21 detected by TOE. TTE detected five (55.6%) of nine vegetations in the aortic valve and three (37.5%) of eight in the mitral valve. TTE detected a pulmonary valve vegetation in one patient in whom TOE was not able to visualise the pulmonary valve. When evaluating for mild to severe regurgitation, TTE detected regurgitation in 24 (68.6%) of 35 valves detected by TOE. Aortic regurgitation was diagnosed in 8 (88.9%) of 9 patients, mitral regurgitation in 7 (58.3%) of 12, and tricuspid in 6 (60%) of 10. When evaluating moderate to severe regurgitation, TTE detected regurgitation in 10 (71.4%) of 14 valves detected by TOE.
Echocardiographic valvular findings in 20 patients with NBTE who had a TTE followed by a TOE within 72 hours
A total of 38 (79.2%) patients had an embolic event within 1 month of NBTE diagnosis, 26 (54.2%) had a stroke, 12 (25.0%) a peripheral ischaemic event and 4 (8.3%) a transient ischaemic attack. Four (8.3%) patients had both a stroke and a peripheral ischaemic event. The clinical presentation of 10 (20.8%) patients without an embolic event is included in online supplemental table 3. Sixteen (33.3%) patients died within 1 year of NBTE diagnosis (table 3); their cause of death is described in online supplemental table 4. Malignancy, metastatic tumours and lung cancer were associated with 1-year all-cause mortality (p=0.0246, p=0.0017 and p=0.0004, respectively). A Kaplan-Meier survival curve for all patients with NBTE and 1-year all-cause mortality is presented in online supplemental figure 1. Kaplan-Meier survival curves for malignancy, lung cancer, metastasis, embolic events and 1-year all-cause mortality are presented in online supplemental figures 2–5. Hypertrophic cardiomyopathy was associated with a lower presentation of embolic events within 1 month of NBTE diagnosis (p=0.0049) (online supplemental table 5).
Outcomes in patients with NBTE
Forty-four (91.7%) patients were treated with anticoagulation; low molecular weight heparin in 22 (45.8%) patients, warfarin in 19 (39.6%), apixaban in 1 (2.1%) and unfractionated heparin in 1 (2.1%) patient.
Three (6.3%) patients underwent cardiac surgery: (1) one had a mitral valve replacement 4 years after NBTE diagnosis with no postoperative complications at 30 days, (2) the second had vegetation excisions and a left atrial appendage ligation 8 months after NBTE diagnosis with no postoperative complications at 30 days, and (3) the third patient underwent an aortic valve replacement 1 week after being diagnosed with NBTE despite being at high surgical risk; he died shortly after the intervention, determined cause of death was ‘mixed cardiogenic and vasodilatory shock with associated neurological insult’. One patient underwent transcatheter intervention and had a TOE-guided trans-septal puncture with removal of vegetation 1 year after NBTE diagnosis with no postoperative complications at 30 days.
Discussion
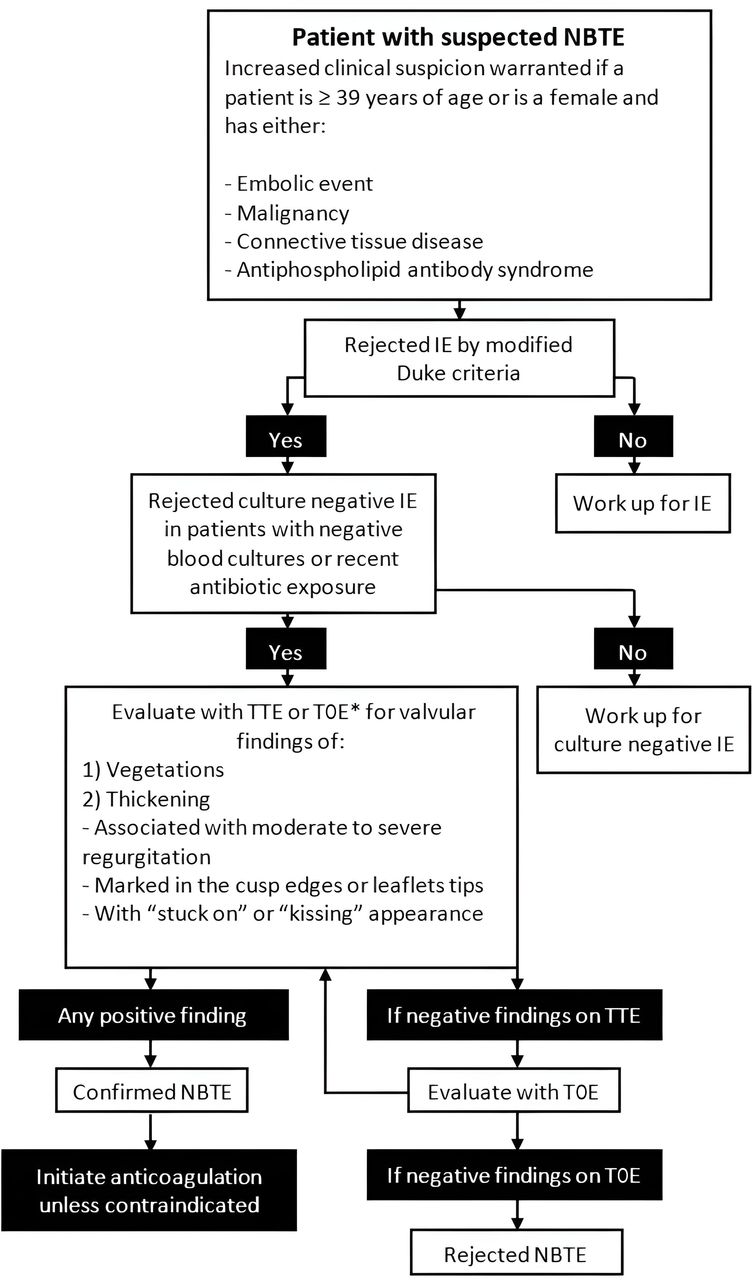
Our primary findings were: (1) NBTE was threefold more prevalent in females than males; (2) embolic complications were the most frequent clinical presentation of NBTE; (3) malignancy and CTD were the most prevalent conditions in patients with NBTE; (4) patients with NBTE have a poor prognosis, especially those with lung cancer or metastatic disease; and (5) TTE sensitivity to detect valvular vegetations was low when compared with that of TOE. Based on these findings, we propose an algorithm to facilitate an NBTE diagnosis (figure 3).

{kind=link}
{kind=link}
{kind=link}
Proposed Mayo Clinic diagnostic work-up for NBTE. *TOE is highly encouraged to evaluate for NBTE abnormalities. IE, infective endocarditis; NBTE, non-bacterial thrombotic endocarditis; TOE, transoesophageal echocardiogram; TTE, transthoracic echocardiogram.
NBTE is a complex syndrome with no pathognomonic clinical or radiographic findings, therefore, a confirmed diagnosis relies on pathological examination of either autopsy or cardiac surgical samples.4 However, acquiring valvular tissue samples in every patient in whom NBTE is considered is not feasible. Echocardiography provides the best imaging modality to detect NBTE and should be performed in every patient with suspicion of this cardiac valve condition. To secure a clinical diagnosis of NBTE, physicians should have a high index of suspicion (especially in patients with recent embolic events or procoagulant and inflammatory conditions) and should exclude alternative diagnoses, in particular infective endocarditis, including its (blood) culture-negative presentation. A similar scenario was seen in the initial proposal of the Duke criteria in 1994 which evaluated clinical, microbiological and echocardiographic findings to diagnose infective endocarditis without undergoing surgical or postmortem examinations, the latter which had been historically required for diagnosing infective endocarditis by the Beth Israel criteria.12
Several unique features characterised patients with NBTE in the current cohort. Despite some antemortem studies showing there is no sex predilection in patients with NBTE,13 14 our patients were predominantly (75%) female, as was described in a recent investigation.15 A potential explanation could be that the second most common condition in our patients, CTD, in 37.5% of cases (66.7% with SLE) affects more women than men.16 Additionally, an underdiagnosis of men with NBTE is possible considering that CTD is more likely to raise clinical suspicion of NBTE in women.
It is worth noting that despite being historically recognised as NBTE, this condition includes thrombotic, inflammatory and inflammatory with superimposed thrombotic vegetations.1 2 Patients with CTD and especially those with SLE, which constituted 25% of this cohort, are characterised by the development of Libman-Sacks vegetations which are usually inflammatory with superimposed thrombotic vegetations.
The mean age of our cohort was 60 years which are consistent with that of previous studies reporting an estimated age around 40–80 years.2 17 The advanced age in our patients could explain the high occurrence of comorbidities as hypertension, diabetes mellitus and myocardial infarction.18 Malignancy was the most prevalent condition in our cohort (52.1%) with lung cancer being its most common presentation. Concordantly, previous studies have shown that malignancy occurred in 32%–80% of NBTE cases.13 19 AAS, which has also been associated with NBTE, was another highly prevalent condition (22.9%).3
When including stroke, transient ischaemic attacks and peripheral embolic events, a total of 79.2% of NBTE cases in the current cohort had an embolic event within 1 month of diagnosis, which was independent of clinical characteristics or comorbidities. This rate is higher than that (~41%) described in postmortem examinations.13 20 This could be explained because most patients with an embolic complication are ordered an echocardiogram and this is more likely to lead to an NBTE diagnosis when compared with asymptomatic patients. To reduce the risk of embolic events complications, patients with NBTE require anticoagulation therapy unless contraindicated, and this was possible in 91.7% of patients in our cohort.7
One-third of our patients died within the first year of NBTE diagnosis. Not surprisingly, malignancy was associated with a higher mortality, particularly in patients with lung cancer or metastatic tumours. One contemporary study showed similar mortality rates with advanced malignancy being associated with the worst prognosis.15
The presence of NBTE does not establish a causal effect of outcomes including embolic complications and mortality due to underlying demographics and comorbid conditions which were not able to be adjusted for because of our small cohort.
NBTE with associated moderate to severe valvular regurgitation was seen in 54.2% of patients; the regurgitation could be related to several conditions and include: (1) thickening or vegetations leading to leaflet malcoaptation; (2) age-related degenerative valve disease; (3) high prevalence of comorbidities as hypertension, heart failure and myocardial infarction; (4) anticardiolipin antibodies in patients with SLE and AAS21; (5) therapeutic-related cardiotoxicity in patients who received chemotherapy or radiation therapy22; and (6) cardiac metastases in patients with lung cancer.23 There is limited and controversial information on surgical indications in NBTE. A few reports have shown that valvular replacement/repair and vegetation excision may be beneficial.8 15 Other investigations, however, have reported that patients with SLE may have a threefold to fivefold increased in surgical morbidity and mortality.24 25 Moreover, conventional anti-inflammatory and antithrombotic therapy may obviate the need for high-risk valvular surgery.26 Despite this, many patients in our cohort were poor surgical candidates due to advanced age and comorbid conditions. Only three (6.3%) patients underwent cardiac surgery; one of them died shortly after intervention and the others had no postoperative complications. Additionally, one (2.1%) other patient had a transcatheter removal of a vegetation with no postoperative complications.
NBTE valvular abnormalities were more frequent in the mitral valve followed by the aortic valve, findings consistent with previous studies.14 15 Both TTE and TOE are standardised techniques capable of providing high-quality images to detect NBTE abnormalities. Despite being semi-invasive, TOE is superior since it provides an improved visualisation of the posterior cardiac structures, exhibits higher resolution than TTE, and is considered more accurate in detecting valvular heart disease or masses.10 A single study has evaluated the use of TTE versus TOE to detect NBTE in a cohort of patients with SLE.9 Findings showed that when compared with TOE, TTE detected vegetations, thickening and regurgitation (mild to severe) with a sensitivity of 11%, 53% and 54%, respectively. Our study showed higher TTE sensitivities of 47.6%, 66.7% and 73.3% for vegetations, thickening and regurgitation, respectively. Differences in our findings could be explained by our patient population, which was inclusive of all NBTE cases, and not limited to patients with SLE. In addition, we speculate this can be explained due to the quality improvement of echocardiography over the past decade,27 since Roldan et al’s work was submitted in 2007.9
Although TTE accuracy to detect NBTE abnormalities has increased over time, its sensitivity remains low when compared with that of TOE, especially when assessing for valvular vegetations. One meta-analysis in patients with infective endocarditis showed that TTE has a sensitivity of 61% to detect vegetations as compared with that of TOE.28 In contrast, we found TTE performance to be lower (47.6%), probably because TOE has a higher sensitivity for small vegetations, especially those <5 mm, which are often seen in NBTE.29 Considering the prognostic implications of identifying valvular vegetations and the low sensitivity of TTE to detect them, a TOE is warranted in all patients with a high clinical suspicion of NBTE and negative or indeterminant TTE findings.30
Limitations
This work has some limitations. First, we had a limited number of NBTE-eligible cases due to our strict inclusion criteria, and the complexity of NBTE diagnosis. Our small cohort did not allow for multivariable analyses. Also, the retrospective nature of this study is a limitation. Additionally, not all patients had a TTE followed by a TOE in less than 72 hours. This could represent a selection bias, however, cases with subsequent echocardiograms were very homogeneous when compared with all NBTE-eligible cases. Moreover, interoperator variability could have been a confounder in the assessment of NBTE valvular abnormalities. Also, those performing the echocardiograms could have been aware of clinical information and previous imaging results of studied patients which could have caused an interpretation bias. Additionally, when NBTE is suspected, negative TTE findings may lead to a TOE that could cause selection bias; nevertheless, 91.7% of our cohort underwent TOE vs only 54.2% TTE. Mayo Clinic Rochester is recognised as a referral centre for infective endocarditis care; therefore, the index of suspicion for this diagnosis is high and could, in part, be responsible for the frequent use of TOE. Finally, our population was composed of adult patients who were predominantly white; thus, the generalisability of these results is not applicable to different populations. Future larger prospective studies must be performed to validate our findings.
Conclusions
The current investigation provides a contemporary evaluation of the epidemiology, demographics, diagnosis and clinical outcomes of NBTE, which was more prevalent in females and patients with conditions as malignancy or CTD. Embolic complications were the most frequent clinical finding. Overall, patients with NBTE had a poor prognosis, particularly in those with lung cancer and metastatic disease.
Data availability statement
Data may be obtained from a third party and are not publicly available. The data underlying this article cannot be shared publicly because the privacy of the individuals who participated in the study must be maintained and because the data underlying this article were provided by Mayo Clinic under licence and by permission. The data will be shared at reasonable request to the corresponding author with the permission of Mayo Clinic.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants but Mayo Clinic Institutional Review Board (ID: 20-011665) exempted this study. Participants gave informed consent to participate in the study before taking part.
Acknowledgments
The authors are extremely grateful for the philanthropic support provided by a gift from Eva and Gene Lane (LB), which was paramount in our work to advance the science of cardiovascular infections, an ongoing focus of investigation at Mayo Clinic for over 60 years.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors JAQ-M and LMB conceptualised and designed the study. JAQ-M had full access to all data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis. JAQ-M and LMB wrote the draft of the manuscript. JAQ-M designed and created all figures. J-RH, SEZ, HIM, VTN and DCD critically reviewed the paper and provided advice. All authors approved the final submitted research manuscript and agree to be personally accountable for their contribution and for the academic integrity of the work. LMB acts as the guarantor.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests LMB reports the following: UpToDate, royalty payments (authorship duties); Boston Scientific, consultant duties; Botanix Pharmaceuticals, consulting duties; Roivant Sciences, consultant duties. None of the other authors had disclosures.
Patient and public involvement Patients and/or the public were involved in the design, or conduct, or reporting, or dissemination plans of this research. Refer to the Methods section for further details.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.