Article Text

Abstract
Introduction Despite the recent inclusion of advanced chronic kidney disease (CKD) in modern heart failure (HF) trials such as DAPA-CKD, cardiorenal syndrome (CRS) remains an undertreated disorder with a paucity of evidence-based therapies. Cardiorenal clinics (CRC) have emerged as a collaborative initiative between cardiologists and nephrologists to provide a multi-disciplinary approach. To date, little data exist on the performance and outcomes of this clinic model. This study provides insight into how patient characteristics influence decisions on the choice of renal replacement therapy (RRT), and whether such decisions affect patient outcomes.
Methods This was a single-centre retrospective study of 151 consecutive patients who were referred to the CRC from primary and secondary care between January 2016 and March 2020. Criteria for referral were patients with an estimated glomerular filtration rate ≤30 mL/min/1.73 m2 and HF, regardless of ejection fraction. CRC consisted of a consultant nephrologist and cardiologist with a specialist interest in HF. All-cause mortality and hospitalisations within 12 months from the last clinic appointment were compared between patients managed conservatively and those on RRT. Morbidity outcomes before and after RRT include changes in New York Heart Association (NYHA) class, medication burden, weight and systolic blood pressure (SBP).
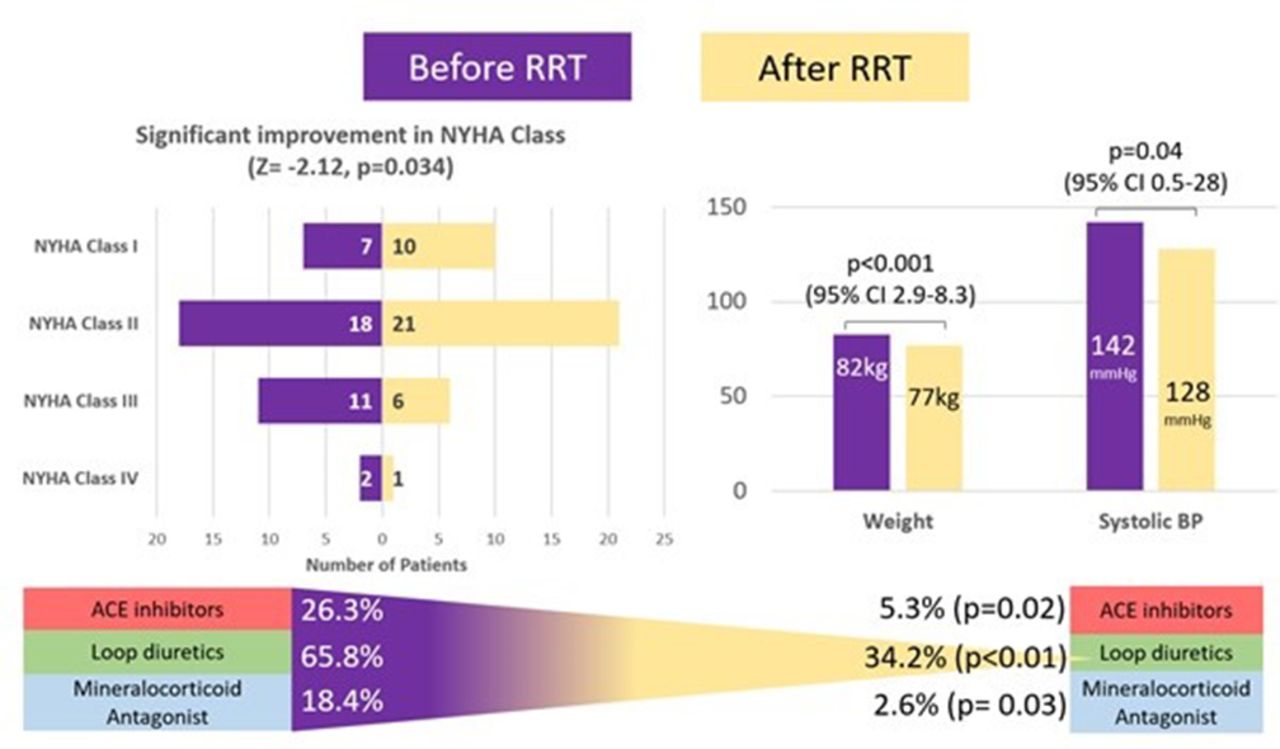
Results Within the study cohort of 151 patients, the most common form of CRS was type 2 (i.e. chronic HF induced the onset or progression of CKD). As summarized in Table 1, 113 patients (75%) were managed conservatively, of which 59% (n=67) were treated with ACE inhibitors, angiotensin-receptor blockers or Sacubitril/Valsartan (Table 2). This group was more likely to be older with a higher prevalence of renovascular and ischaemic heart disease and Type 2 CRS. In comparison, the RRT group (n=38; 25%) had a higher prevalence of diabetic nephropathy, HF with preserved ejection fraction, and Type 4 and 5 reno-cardiac syndrome. 37% (n=14) were on haemodialysis, 21% (n=8) peritoneal dialysis and 42% (n=16) had renal transplants. 63% (n=10) of transplant recipients developed CRS from an acute coronary event or sepsis. No significant differences in all-cause mortality or hospitalisation were found (Table 1), however one confounding factor was the larger number of patients on cardiac resynchronisation therapy in the conservative group. Patients on dialysis demonstrated significant reduction in weight, SBP, medication burden and an improvement in NYHA class (Figure 1).
Comparison of patient characteristics and outcomes- n (%)
Comparison of heart failure therapies- n (%)
{kind=link}
Conclusions Our study highlights specific phenotypes in CRS that are deemed more appropriate for conservative management and ones more suited for RRT. Reassuringly, RRT did not increase mortality in this high-risk cohort any more than those managed medically and so should be considered as a safe treatment, when clinically appropriate. Irrespective of treatment strategy, CRS remains a disorder with high mortality. However, RRT has been shown to improve various aspects of morbidity. The dedicated CRC enabled some patients to be optimized for bridging to renal transplant. Finally, prescriptions of guideline-directed medical therapies for HF remain under-prescribed, highlighting the need to overcome this ‘treatment-risk paradox’, whereby higher risk patients most likely to benefit are less likely to receive the recommended best medical therapy.
Conflict of Interest Nil