Article Text

Abstract
Objective To describe characteristics of patients admitted with refractory cardiac arrest for possible extracorporeal cardiopulmonary resuscitation (ECPR) and gain insight into the reasons for refraining from treatment in some.
Methods Nationwide retrospective cohort study involving all tertiary centres providing ECPR in Denmark. Consecutive patients admitted with ongoing chest compression for evaluation for ECPR treatment were enrolled. Presenting characteristics, duration of no-flow and low-flow time, end-tidal carbon dioxide (ETCO2), lactate and pH, and recording of reasons for refraining from ECPR documented by the treating team were recorded. Outcomes were survival to intensive care unit admission and survival to hospital discharge.
Results Of 579 patients admitted with refractory cardiac arrest for possible ECPR, 221 patients (38%) proceeded to ECPR and 358 patients (62%) were not considered candidates. Median prehospital low-flow time was 70 min (IQR 56 to 85) in ECPR patients and 62 min (48 to 81) in no-ECPR patients, p<0.001. Intra-arrest transport was more than 50 km in 92 (42%) ECPR patients and 135 in no-ECPR patients (38%), p=0.25. The leading causes for not initiating ECPR stated by the treating team were duration of low-flow time in 39%, severe metabolic derangement in 35%, and in 31% low ETCO2. The prevailing combination of contributing factors were non-shockable rhythm, low ETCO2, and metabolic derangement or prehospital low-flow time combined with low ETCO2. Survival to discharge was only achieved in six patients (1.7%) in the no-ECPR group.
Conclusions In this large nationwide study of patients admitted for possible ECPR, two-thirds of patients were not treated with ECPR. The most frequent reasons to abstain from ECPR were long duration of prehospital low-flow time, metabolic derangement and low ETCO2.
- EMERGENCY MEDICINE
- Ethics, Medical
- Heart-Assist Devices
Data availability statement
No data are available. Individual patient data cannot be shared due to Danish legistration.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
In selected patients with refractory cardiac arrest, survival exceeding 40% may be achieved using advanced mechanical circulatory support (MCS).
Selection of patients is based on multiple factors and not infrequently patients are evaluated but turned down for active treatment.
Understanding of factors contributing to turning down patients with refractory cardiac arrest for extracorporeal cardiopulmonary resuscitation (ECPR) is needed to improve selection and improve outcomes.
WHAT THIS STUDY ADDS
The study highlights the heterogeneity and complexity in deciding on whether or not to initiate ECPR in patients with refractory cardiac arrest.
The most frequent reasons to abstain from ECPR were long duration of prehospital treatment, metabolic derangement and low end-tidal carbon dioxide.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
Reducing low-flow times and increased focus on quality of chest compression may increase the number of patients eligible for ECPR and potentially increase the number of patients surviving refractory cardiac arrest.
Introduction
The survival of patients with out-of-hospital cardiac arrest (OHCA) depends on presenting rhythm and whether circulation can be restored.1 2 However, even with a favourable presenting rhythm and immediate bystander life support, some patients never achieve return of spontaneous circulation (ROSC) and life support is terminated at the scene of cardiac arrest.3
Initial case reports of successful resuscitation using mechanical circulatory support (MCS) despite prolonged resuscitation, have led to the concept of extracorporeal cardiopulmonary resuscitation (ECPR).4 Depending on selection criteria, survival rates of less than 10% and up to more than 40% have been reported.5–8 Recently, one randomised trial showed improved outcome with ECPR for refractory OHCA when initiated within 60 min of arrest.8
Most ECPR protocols base the patient selection on whether cardiac arrest was witnessed, immediate initiation of immediate bystander life support, initial shockable rhythm, assessment of end-tidal carbon dioxide (ETCO2), patient age and comorbidity.9 Many of these observations are not dichotomous and are not straightforward in an emergency as cardiac arrest. Previous observational studies with well-defined ECPR protocols have focused on outcomes of patients where ECPR was initiated, whereas little is known regarding patients admitted for evaluation for possible ECPR where ECPR was not initiated.
In the present study patients admitted with refractory OHCA in Denmark were identified to elucidate factors associated with turning down patients for ECPR, and to describe associated outcome.
Methods
This nationwide retrospective, observational cohort study was conducted at all tertiary cardiac arrest centres providing ECPR in Denmark (Aarhus University Hospital, Aalborg University Hospital, Odense University Hospital and Copenhagen University Hospital). These four hospitals provide ECPR treatment for the entire Danish population of 5.8 million people.
Study population
The study included consecutive patients aged ≥18 years with refractory OHCA of presumed cardiac cause admitted for potential ECPR treatment. Refractory OHCA was defined as absence of ROSC despite resuscitation efforts for more than 15 min. Patients evaluated for ECPR between January 2015 and December 2020 were identified from local MCS databases and medical records. Due to regional differences in implementation and MCS availability, initiation of data collection differed for each hospital: Aarhus University Hospital and Aalborg University Hospital: January 2015; Odense University Hospital: November 2015; and Copenhagen University Hospital: November 2016.
The cohort was divided into patients proceeding to ECPR and those where the team of treating physicians refrained from ECPR (No ECPR).
Organisation of treatment
In Denmark, patients with refractory OHCA with ongoing CPR potentially eligible for ECPR are routed directly to the catheterisation laboratory by the emergency medical service (EMS) via ambulance or helicopter. On-scene intubation was done by EMS physicians, and the decision to transfer the patient was done in agreement between the EMS physician and the attending senior cardiology registrar at the nearest centre. The EMS physician has the final decision on whether to transport the patient to the tertiary centre or terminate therapy on the scene. The decision to initiate ECPR was taken by the treating team of physicians in the catheterisation laboratory, which as a minimum consists of specialists in invasive and non-invasive cardiology and a specialist in cardiothoracic anaesthesiology. At Aarhus, Aalborg and Odense University Hospitals, a cardiac surgeon also participates in the team evaluation of the patient.
Until 2018 ECPR followed local guidelines. In 2018 a national consensus on the use of ECPR in patients with refractory OHCA was adopted based on the experience at Danish centres providing this.7 There was national consensus that patients with normothermic cardiac arrest with a presumed cardiac origin, age <65 years, an initial shockable rhythm, witnessed arrest, bystander CPR and ETCO2 >1.3 kPa on arrival at the treating heart centre were potentially eligible for ECPR. Additionally, a prehospital low-flow time of <100 min was required at two centres (Odense and Copenhagen) and lactate <15 mmol/L and pH >6.8 at three centres (Aarhus, Copenhagen and Aalborg).
Treatment algorithm
Patients selected for ECPR proceeded directly to MCS which in the vast majority was veno-arterial extracorporeal membrane oxygenation (VA-ECMO). Cannulation was done percutaneously using ultrasound-guided Seldinger technique. In most patients, a cannula was inserted antegradely in the femoral artery to ensure limb perfusion. In a minority (n=12), a transvalvular axial flow pump (Impella CP device) was initially employed during chest compression by choice of the treatment team. The transvalvular axial flow pump was placed percutaneously and correct positioning was then confirmed by fluoroscopy and echocardiography. Postresuscitation care and management was performed according to local intensive care unit (ICU) standard protocols including targeted temperature management, neurological prognostication, procedures for weaning of MCS and withdrawal of treatment.
If ROSC was achieved or if the patients were not considered a candidate for ECPR by the treating team of physicians, further advanced cardiovascular life support was either continued or terminated at the discretion of the treating team.
Data collection
Study data were entered in a national electronic RedCap database. All individual patient data were evaluated, and data recorded according to the Utstein recommendation.10 Data were recorded from the prehospital EMS systems and included time of cardiac arrest, witnessed arrest, bystander CPR, initial presenting rhythm, and prehospital care and intubation. Patient demographics and in-hospital data on clinical parameters, known comorbidities, laboratory tests, intervention and outcome data were retrospectively obtained from patient medical records. Based on patient medical records the main reasons for not initiating ECPR were recorded. This was classified as: advanced age; severe comorbidity; unshockable primary rhythm (pulseless electrical activity/asystole); unwitnessed arrest; duration of no-flow time; duration of low-flow time; low ETCO2; elevated lactate; low pH; and no visible cardiac movement on echocardiogram. These variables were recorded as binary and thus no attempts were done to qualify factors such as movement of heart on echocardiogram or signs of life.
Outcomes
The outcomes for this study were whether ECPR was initiated, and survival to ICU admission and hospital discharge.
Patient and public involvement
No patient representatives or members of the public were involved in the design, conduct or reporting plans of this research project. We aim to involve patients and members of the public in the development of an appropriate method of dissemination.
Statistical analysis
The sample size was defined by the number of patients evaluated during the 5-year period which was decided arbitrarily but ensuring a significant sample size. Continuous data are presented as median and IQR (first–third quartile) and categorical data as number and percentages. The Mann-Whitney U test and the Kruskal-Wallis H test were used for comparison of continuous data, whereas the χ2 test and Fisher’s exact test were used for categorical data. In case of missing values, patients were excluded from the statistical analysis, and no imputations were done. Association between relative contraindications for ECPR from national recommendation was tested in a logistic regression analysis with; age >65 years; ETCO2 <1.3 kPa; first rhythm asystole, unwitnessed arrest and no bystander CPR included in the model. Two-sided p values of <0.05 were considered statistically significant. Statistical tests were performed using IBM SPSS V.28.0.0.0.
Results
During the study period, 579 patients were transported with refractory cardiac arrest for evaluation for ECPR. The vast majority was intubated on site by the EMS physician (96%), and transported with mechanical chest compressions (93%). After initial evaluation 221 patients (38%) proceeded to ECPR with establishment of VA-ECMO in 208 (95%) and transvalvular axial flow pump in 12 (5%); the remaining 358 patients (62%) were not considered candidates for ECPR (table 1). As expected because of the national and regional criteria, patients rejected for ECPR were older, had more frequently non-shockable first recorded rhythm (table 1). Median prehospital low-flow time exceeded 60 min in both groups but was significantly longer in patients accepted for ECPR despite distance to centre being comparable (table 1).
Patient characteristics and prehospital data in patients with refractory cardiac arrest evaluated for possible ECPR treatment stratified according to whether treatment was initiated or not
On hospital arrival only 11% had a shockable rhythm, most prevalent among patients proceeding to ECPR; 7% developed ROSC (table 2). Proportions of patients with signs of life during resuscitation and spontaneous movement of the heart on echocardiography was higher in ECPR patients. Although patients being declined ECPR tended to be more metabolically deranged with lower pH and higher lactate, the overlap between groups was considerable and the majority of ECPR recipients were severely metabolically deranged with a median pH 6.9 and a median lactate level of 16 mmol/L (table 2).
Characteristics and management in catheterisation laboratory in patients with refractory cardiac arrest evaluated for possible ECPR treatment stratified according to whether treatment was initiated or not
Treatment decision was made by a team of minimum two cardiologists and one anaesthetist in 513 cases (97%) with no difference between groups. The most frequent cause for not initiating ECPR was duration of low flow, which was recorded in 139 patients (39%). Among these, 60 patients (43%) suffered arrest ≤50 km from an ECPR centre with a median low-flow time of 60 (53–75) min as opposed to 77 patients with >50 km with a median low-flow time of 84 (70–99) min, p<0.001. Severe metabolic derangement with high lactate and/or low pH was stated as a contributing factor in 21% and 23%, respectively (figure 1). Among patients where metabolic derangement was registered as the reason for not initiating ECPR, median lactate was 16 (14–22) mmol/L and pH 6.8 (6.7–6.9). Other contributing reasons are summarised in figure 1. In the majority of cases, two or three contributing factors were given as the reason for not initiating ECPR (figure 1).
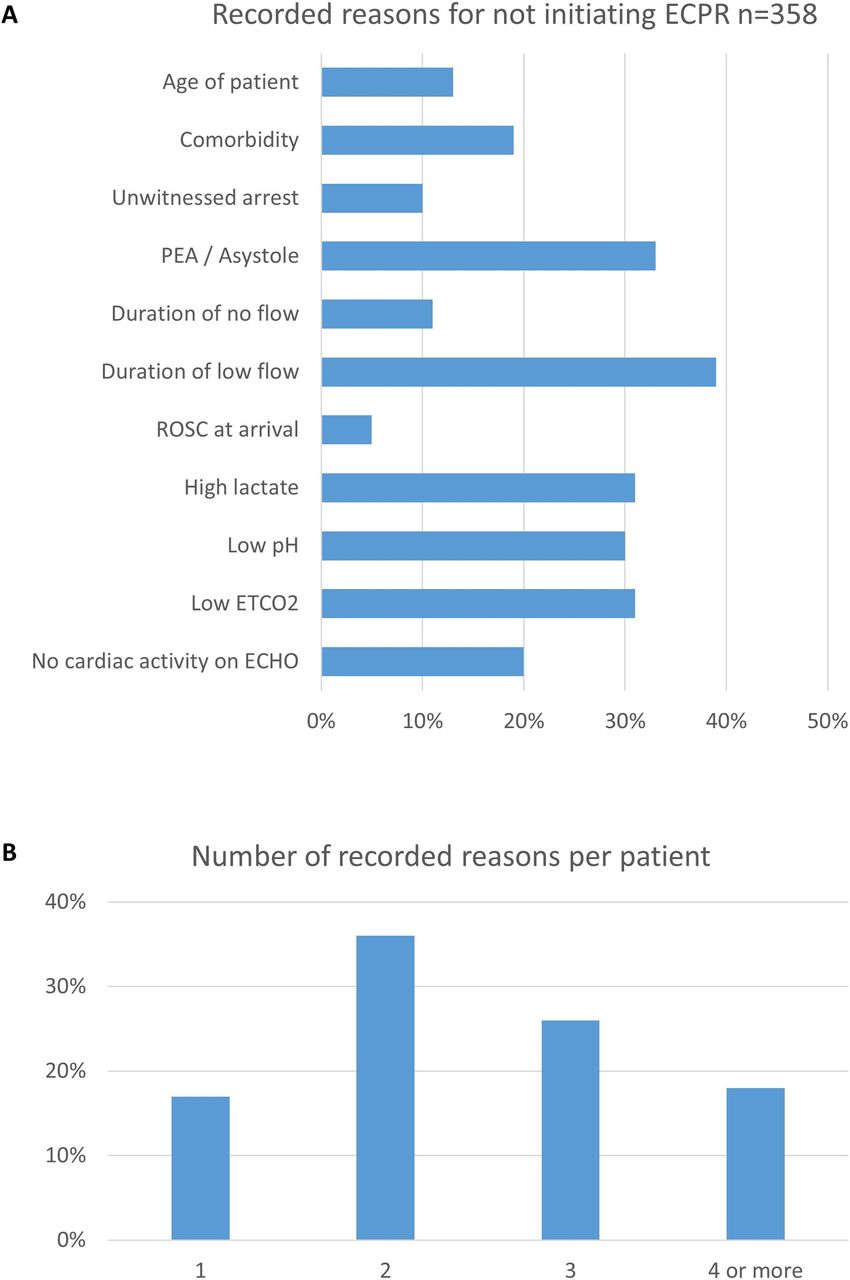
(A) Distribution of contributing factors for not initiating ECPR in refractory OHCA. (B) Frequency of the number of recorded reasons. ECHO, echocardiography; ECPR, extracorporeal cardiopulmonary resuscitation; ETCO2, end-tidal carbon dioxide; OHCA, out-of-hospital cardiac arrest; PEA, pulseless electrical activity; ROSC, return of spontaneous circulation.
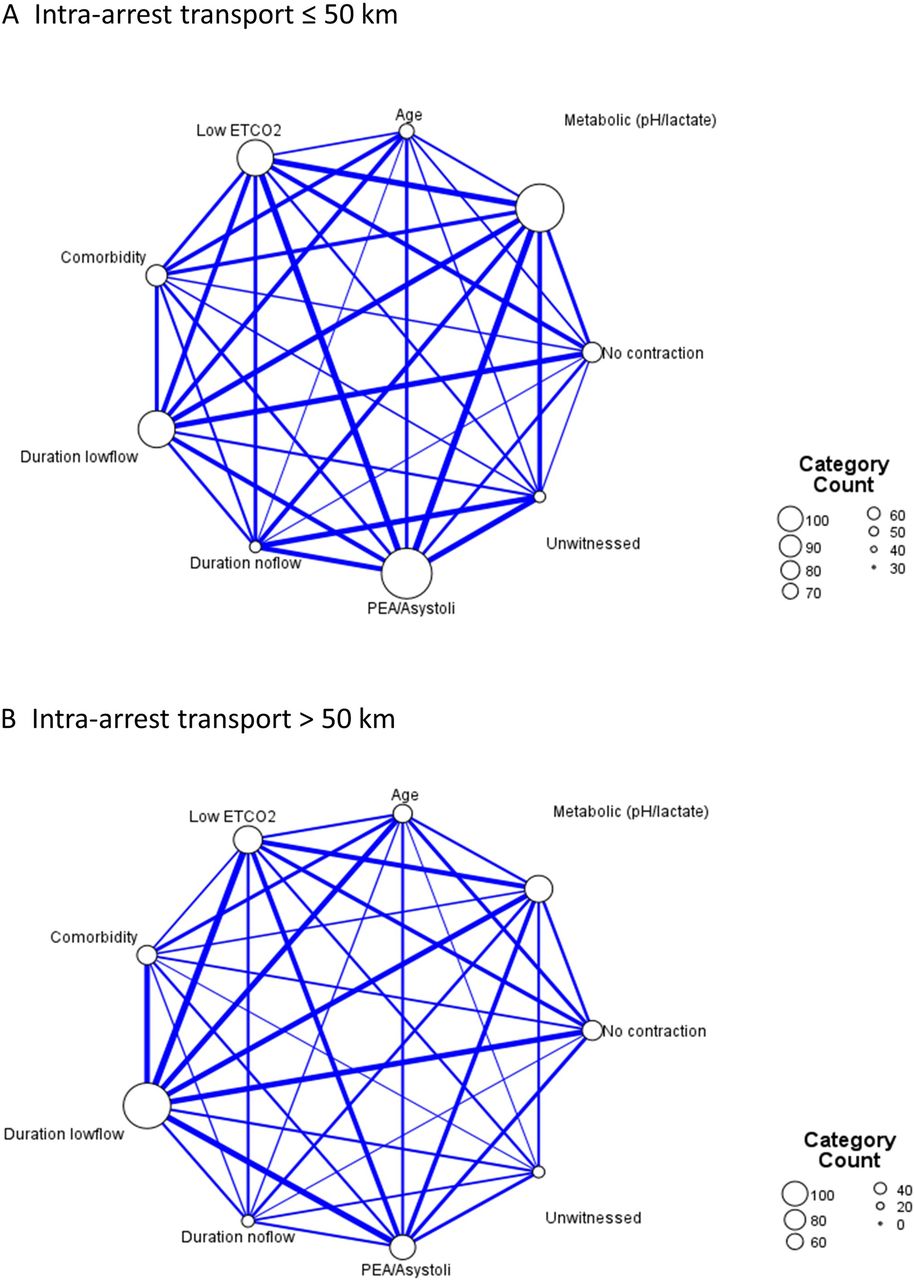
The pattern of combinations of contributing causes are summarised in figure 2 divided according to distance to centre. The prevailing contributing factors were non-shockable rhythm, low ETCO2 and metabolic derangement in those transported ≤50 km. In those transported >50 km prehospital low-flow time was the prevailing factor with low ETCO2.
{kind=link}
{kind=link}
Relationships maps of contributing factors for not initiating ECPR. Nodes represent cause for not initiating ECPR. Larger nodes and thicker lines represent stronger connections and associations whereas smaller nodes and thinner lines represent weaker connections and associations. (A) Patients with refractory OHCA less than 50 km from ECPR centre. (B) Patients with refractory OHCA more than 50 km from ECPR centre. ECPR, extracorporeal cardiopulmonary resuscitation; ETCO2, end-tidal carbon dioxide; OHCA, out-of-hospital cardiac arrest; PEA, pulseless electrical activity.
Number of patients with relative contraindications according to the national 2018 recommendation are summarised in table 3. In a logistic regression analysis with all national recommendations entered, age >65 years (OR 0.27, 95% CI 0.18 to 0.43, p<0.001); ETCO2<1.3 (OR 0.20, 95% CI 0.10 to 0.40, p<0.001); asystole (OR 0.44, 95% CI 0.25 to 0.79) were associated with less likelihood of establishing ECPR, whereas unwitnessed arrest and no bystander CPR was not.
No of patients with relative contraindications for ECPR according to the Danish national 2018 recommendation stratified according to whether treatment was initiated or not
ROSC in the catheterisation laboratory was achieved in 25 No-ECPR patients (7%), 77 No-ECPR patients (22%) underwent coronary angiography, and in 25 (7%) an attempt to perform percutaneous coronary intervention was done. Transfer to ICU was achieved in 22 patients (6%), and survival to discharge was achieved in 6 patients (1.7%). Among patients where ECPR was initiated 184 (84%) were transferred to ICU and 50 (23%) were discharged alive from hospital. In the ECPR group 22 (24%) transported more than 50 km survived to discharge and 27 (22%) of the patients transported ≤50 km survived to discharge, p=0.53. Among patients with prehospital low-flow time <60 min, 21 patients (26%) survived with was not different from 29 patients (21%) with low-flow time ≥60 min, p=0.43.
Discussion
The present study describes the pathway from refractory OHCA to the decision to establish ECPR in a large nationwide study. The study both identifies patients with unmodifiable factors turned down for ECPR but also potentially modifiable factors such as prehospital low-flow time and low ETCO2 that could potentially be candidates for ECPR by optimised identification, optimisation of chest compression and early transfer of patients with refractory cardiac arrest.
Several advanced life support algorithms have incorporated termination of resuscitation rules.11 12 There is a grey zone between patients unlikely to survive and patients eligible for ECPR. In the recent randomised Advanced Reperfusion Strategies for Patients with Out-of-hospital Cardiac Arrest and Refractory Ventricular Fibrillation (ARREST) Trial stringent inclusion criteria led to a survival rate of 43% in the ECPR group,8 consistent with recent observational studies.7 13 Conversely, in the absence of protocols for selection and management during admission, survival can be poor.6 13 However, decisions on ECPR treatment can rarely be based on a simple prognostic algorithm in a situation where the choice of refraining from ECPR in most cases will lead to termination of life support and death.8 In agreement we found a considerable number of patients not fulfilling basic prehospital criteria for ECPR. It may, from a health economic perspective, seem futile to rescue few, but for the individual patient a necessity for survival. Thus, selection of borderline cases for ECPR still seems reasonable with a final patient-centred decision-making done by multidisciplinary teams for ECPR at the hospital.
The ARREST Trial excluded patients with resuscitation lasting longer than 60 min before randomisation,8 and the Extracorporeal Life Support Organization recommend the goal of ECPR to be established within 60 min of the onset of cardiac arrest.9 The prehospital low-flow time in the present study exceeded 60 min in more than 50% of patients, and duration of prehospital low-flow time was the most frequent reason reported for not initiating ECPR. This argues for a more aggressive load-and-go strategy to reduce the prehospital arrest time. However, this must be weighed against the risks associated with intra-arrest transportation. Grunau et al recently compared intra-arrest transport with continued on-scene resuscitation in a large retrospective North American OHCA cohort.14 In a time-dependent propensity score matched analysis of more than 27 000 OHCA cases, intra-arrest transport to the hospital was associated with a lower probability of survival to hospital discharge. Further, moving a patient with refractory cardiac arrest from the scene of arrest to treating centre is logistically challenging. This may reduce quality of chest compression, and interfere with defibrillation and administration of drugs. Manual chest compression is challenging during transport where it carries serious risk for EMS when performing manual chest compression in a fast-moving vehicle. However, load-and-go with the use of mechanical chest compression during ongoing arrest has also been suggested to reduce no-flow time and improves the quality of the chest compression.15 Futile transports raise ethical concerns as they prolong suffering with no realistic chance of survival. The recently published Hyperinvasive Approach in Cardiac Arrest Study performed prehospital randomisation of 256 patients with witnessed refractory OHCA.16 The study was stopped for futility (survival with good neurological outcome was 31.5% in the hyperinvasive group and 22% in the standard of care group, p=0.09). Thus, these studies taken together suggest no overall harm when highly selected patients are routed for potential ECPR, but liberal intra-arrest transport may not be generally beneficial. Thus, early recognition of potential ECPR candidates is essential with early intra-arrest transport of potential candidates. Whether a more rapid transfer time with reduced low-flow time would have led to higher ECPR utility is speculative.
Another way of reducing low-flow time is by establishing VA-ECMO at the scene of arrest. The Service d’Aide Médicale Urgente of Paris has since 2011 implemented ECPR in the prehospital setting.13 Implementation of such a system depends on the demographics of the region where it is deployed. In a very densely populated area such as Paris, this system may be cost-effective and time-effective. In less densely populated rural areas, this may not be the case. Currently, there are ongoing randomised initiatives to compare in-hospital with prehospital ECMO for refractory cardiac arrest (ClinicalTrials.gov Identifier: NCT04620070).
In about 30% of cases, ECPR was not initiated because of low ETCO2 on arrival. The content of alveolar CO2 is determined by production, alveolar ventilation and cardiac output,17 that readily can be measured using quantitative capnography in intubated patients. During resuscitation ETCO2 reflects pulmonary blood flow, thus the quality of cardiopulmonary resuscitation.18 In patients selected for ECPR in the current study, ETCO2 was almost unchanged from intubation to hospital arrival, opposed to a significant decrease in those not selected. This is to some degree a self-fulfilling prophecy as ETCO2<1.3 kPa is a part of the contraindications for ECPR.9 However, the significant decrease in ETCO2 in some patients during resuscitation could signify a decrease in quality of chest compression during transport and extra focus on ETCO2 during these challenging transfers are warranted. However, whether this would increase the number of patients eligible for ECPR is speculative.
Strength and limitations
This study is strengthened by being nationwide and both capturing patients accepted for ECPR and turned down for ECPR. This study is also strengthened by individual assessment of medical charts and prehospital recordings and by the multidisciplinary decision of whether to treat the patient. The retrospective design is an obvious limitation, which precludes any assumptions of causality. The criteria for refraining from ECPR were extracted from medical charts. Thus, this difficult medical decision was reduced to dichotomous categories where important information and clinical judgement may have been missed. In addition the individual criteria such as duration of low-flow time or high lactate that were stated as contributing factors were not necessarily based on strict threshold values but perception of the team. There was a statistically significant median 10 min lower duration in prehospital low-flow time in the No-ECPR group. It may be speculated that cases where ECPR was selected despite extensive prehospital low-flow time had a more favourable circumstance and thus the team accepted the longer transport time. Due to selection bias, comparison of survival in patients eligible and ineligible for ECPR is not meaningful and cannot be translated into a survival benefit of the intervention, and to test the effect of national recommendation difficult is as the consensus statement was based on experience and practice in Denmark so much alike. Only 22% of patients in the group where ECPR was not pursued underwent angiography. This low number was driven by further treatment and was considered futile by the treating team. Finally, the population with refractory OHCA terminated prehospital is not available in this study.
Conclusion
The present study describes the pathway from refractory OHCA to the decision to establish ECPR in a large nationwide study. In the study, 62% of patients were not treated and most frequent reasons were long duration of prehospital low-flow time, metabolic derangement and low ETCO2 in accordance with a national selection guideline. Thus, the study identifies patients with potentially modifiable factors, which highlights importance of optimised early identification, optimisation of chest compression and early transfer of patients with refractory cardiac arrest.
Data availability statement
No data are available. Individual patient data cannot be shared due to Danish legistration.
Ethics statements
Patient consent for publication
Ethics approval
The study was conducted in accordance with the Declaration of Helsinki and approved by the Danish Data Protection Agency (Ref. 1-16-02-383-18) and the Danish Patient Safety Authority (Ref. 3-3013-2696/1). In Denmark, informed consent or ethical approval is not required for registry-based research.
References
Footnotes
Contributors Conceptualisation: JEM, CJT, CH; Methodology: LL, JEM; Formal analysis and investigation: LL, JEM, SRM, EG, JBA; Writing—original draft preparation: JEM; Writing—review and editing: all listed authors; Funding acquisition: LL, JEM; Supervision: JEM, CJT, CH. JEM is responsible for the overall content as the guarantor.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests JEM reports speaker fees and grants from Abiomed and served at the scientific advisory board for Boehringer Ingelheim, outside the submitted work. CH reports grants from the Lundbeck Foundation and speaker’s honoraria from Abiomed, outside the submitted work. JK reports non-financial participation in the advisory board for the CoCa Trial. CJT is supported by an unrestricted research grant from the Danish Heart Foundation. The remaining authors have no conflicts of interest to declare.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.