Article Text

Abstract
Background Heart valve clinics (HVC) have been introduced to manage patients with valvular heart disease within a multidisciplinary team.
Objective To determine the outcome benefit of HVC approach compared with standard of care (SOC) for patients with moderate and asymptomatic severe aortic stenosis (mAS and asAS).
Methods Single-centre, observational registry of patients with mAS and asAS with at least one cardiac ambulatory consultation at our Cardiovascular Centre. Based on the outpatient strategy, patients were divided into HVC group, if receiving at least one visit at HVC, and SOC group, if followed by routine cardiac consultations.
Results 2129 patients with mAS and asAS were divided into those followed in HVC (n=251) versus SOC group (n=1878). The mean age was 76.5±12.4 years; 919 (43.2%) had asAS. During a follow-up of 4.8±1.8 years, 822 patients (38.6%) died, 307 (14.4%) were hospitalised for heart failure and 596 (28%) underwent aortic valve replacement (AVR). After propensity score matching, the number of consultations per year, exercise stress tests, brain natriuretic peptide (BNP) determinations and CTs were higher in the HVC cohort (p<0.05 for all). A shorter time between indication of AVR and less advanced New York Heart Association class was reported in the HVC cohort (p<0.001 and p=0.032). Compared with SOC, the HVC approach was associated with reduced all-cause mortality (HR=0.63, 95% CI 0.40 to 0.98, p=0.038) and cardiovascular death (p=0.030). At multivariable analysis, the HVC remained an independent predictor of all-cause mortality (HR=0.54, 95% CI 0.34 to 0.85, p=0.007).
Conclusions In patients with mAS and asAS, the HVC approach was associated with more efficient management and outcome benefit compared with SOC.
- aortic valve stenosis
- heart valve diseases
- outcome assessment, health care
- transcatheter aortic valve replacement
Data availability statement
Data are available on reasonable request.
Statistics from Altmetric.com
- aortic valve stenosis
- heart valve diseases
- outcome assessment, health care
- transcatheter aortic valve replacement
WHAT IS ALREADY KNOWN ON THIS TOPIC
Heart valve clinics (HVC) have been introduced to evaluate and manage patients with valvular heart disease within a multidisciplinary team. Early surgical aortic valve replacement in asymptomatic patients with severe aortic stenosis (AS) and normal left ventricular ejection fraction has been recently associated with a reduction of the composite endpoint of all-cause death, acute myocardial infarction, stroke and unplanned hospitalisation for heart failure compared with conservative treatment.
WHAT THIS STUDY ADDS
Nowadays, many patients with significant AS are not recognised or not referred for evaluation and treatment. We demonstrated that patients with moderate and asymptomatic severe AS followed in the HVCs were managed more efficiently in terms of education, medical therapy and second-level diagnostic tests and experienced a lower rate of all-cause death compared with the standard-of-care group.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
Our findings provide new insights into the benefit of the HVC in the setting of AS, pointing out the potential to improve patient care and clinical outcomes. This might pave the way for the widespread organisation of the HVC structure and early referral of patients with significant AS to these organisations.
Introduction
Aortic stenosis (AS) is the most prevalent valvular heart disease (VHD) in the western world and represents a major public health burden.1 The incidence rate of clinically significant (moderate-to-severe) AS ranges from 4% to 10% among patients >65 years old.2–4 The management of patients with moderate AS (mAS) and asymptomatic severe AS (asAS), particularly the choice between early intervention versus watchful waiting, is still debated.5 A delay in reporting symptoms is common; once symptoms develop, early recognition and timely referral to intervention are critical.6 7 In this setting, the RECOVERY and AVATAR trials supported the benefit of early aortic valve replacement (AVR) versus conventional watchful waiting strategy for patients with asAS and normal left ventricular ejection fraction (LVEF).8 9 These trials are in line with the evolving clinical decision-making paradigm regarding the management of this challenging population. Similarly, no strong recommendations have been established yet for the treatment of patients with mAS, who do not have a favourable prognosis, especially in the case of concomitant reduced LVEF.10–12 The benefit of early detection of AS progression and left ventricle dysfunction prompts the interest to evaluate the outcome benefit of dedicated healthcare pathways and educational programmes.
Recently, an increasing number of patients with VHD have been managed in heart valve clinics (HVCs), which offer multidisciplinary services and fast and easy referral toward other necessary disciplines, enhancing the quality of patient care.6 However, due to the high prevalence of VHD, most patients with AS are still followed in routine cardiac care consultations. This condition allowed a direct comparison in the same institution between the usual ambulatory cardiac care (standard of care, SOC) and HVC approach. Therefore, we aimed to evaluate the outcome benefit of a HVC approach compared with SOC in patients with mAS and asAS. Moreover, a subgroup analysis was performed to assess the benefit of HVC care separately in patients with mAS and asAS.
Methods
Study population
The study population included in our single-centre, observational registry was identified according to the following criteria: (1) patients with mAS or asAS, diagnosed according to current European Society of Cardiology (ESC) Guidelines,13 (2) good quality transthoracic echocardiography (TTE) to assess AS grade and (3) at least one cardiac ambulatory consultation at our Cardiovascular Centre. Exclusion criteria included: (1) class I indications for surgical/transcatheter aortic valve replacement (SAVR/TAVR),13 (2) concomitant more than moderate aortic regurgitation and/or mitral valve disease at the time of the first echocardiography, (3) prior valve surgery or percutaneous procedure of the aortic valve and (4) severe extracardiac comorbidity limiting survival (life expectancy <12 months). Based on the type of outpatient strategy, patients were divided into the HVC group, if they underwent at least one visit to the HVC, and the SOC group, if they were followed with routine cardiac care consultations (performed by interventional cardiologists, electrophysiologists, heart failure (HF) specialists and clinical cardiologists). These patients were referred to HVC or SOC by general practitioners, outpatient care specialists in cardiology, internal medicine and resident cardiologists according to current guidelines and the availability of ambulatory slots.14 Once included in the HVC programme, the patients followed the cardiological schedule provided by this setting. The indication for AVR (SAVR/TAVR) has been assigned following the guidelines and confirmed by the Heart Team according to symptoms onset and, in the case of asymptomatic patients, in presence of any among: abnormal exercise test, LVEF <50%, markedly elevated biomarkers, rapid progression of AS severity and severe valve calcification assessed by CT.13 Patients or the public were not involved in the design, conduct, reporting or dissemination plans of our research. The present study was conducted according to the principles of the Declaration of Helsinki. All patients were informed about their participation in the registry and provided informed consent for the anonymous publication of scientific data. This registry was approved by the institutional review board (Onze-Lieve-Vrouw Clinic, Aalst, Belgium—Registration No 2022/028).
The HVC organisation
Since 2014, a Heart Valve Centre (HVCe) has been set up in our Cardiovascular Centre according to the ESC/American Heart Association Guidelines, including: (1) availability of the entire spectrum of surgical and transcatheter valve procedures with 24/7 services, (2) weekly Heart Team meetings, (3) organisation of a HVC for ambulatory management, (4) use of multimodality imaging including echocardiography, cardiac CT, cardiac magnetic resonance (CMR) and nuclear medicine and (5) yearly evaluation of patients’ outcomes with quality check and planning of educational programmes.14 15 The HVC involves cardiologists with expertise in VHD, cardiac imaging specialists, cardio-anaesthesiologists, cardiac surgeons and dedicated nurses. Specifically, the cardiologists involved have the following competencies: (1) more than 10 years of experience in VHD, (2) performance of high volume of TTE/transoesophageal echocardiograms per year, with official certifications for echocardiographic guidance of percutaneous structural valve intervention (MitraClip/TriClip), (3) continuous update on the field of VHD by periodical training courses, lead of research projects and participation in national/international congresses, (4) weekly attendance of Heart Team meetings and (5) some of them experienced in cardiac CT and CMR. The organisation of the HVC includes a reduced number of patients per session of consultations (6–8 patients vs 12–14 patients in SOC), with an average of 40 min per visit, resulting in more time dedicated to patients’ education and supplementary TTE image acquisitions if necessary. The HVC programme provides a tailored schedule of follow-up according to the severity of VHD and the overall patient clinical status. Specifically, patients with clinically significant AS managed in the HVC are followed up at least every 6 months with physical examination, EKG and TTE. Patients who develop symptoms or experience a significant worsening of symptoms/quality of life between scheduled HVC consultations could communicate with the HVC physician by telephone/email. Moreover, a dedicated team of nurses adequately trained and skilled for managing patients with VHD is available to answer HVC patients’ calls and reschedule consultations with the help of secretaries, if necessary.6 16
Study endpoints
The primary endpoint of the study was all-cause mortality. The vital status was validated in the Belgian Population Register. We also assessed cardiovascular death, hospitalisation for HF and a composite of all-cause death and non-fatal hospitalisation due to the worsening HF. Definition of each endpoint is provided in online supplemental file–extended methods.
Supplemental material
Statistical analysis
Normality distribution of continuous variables was assessed visually by histograms and Q–Q plots. Continuous variables with normal distribution were expressed as the mean±SD and non-normally distributed variables as median and IQR. Categorical variables were expressed as counts and percentages. Differences between groups were analysed using t-test and Mann-Whitney U test for continuous variables, when appropriate. The χ2 test was used to compare group differences for categorical variables. When more than 20% of the expected cell count was <5, the Fisher’s exact test was used. Propensity score matching (PSM) was used to reduce bias and differences in the patients’ baseline characteristics.17 Details are provided in the online supplemental file – extended methods. Multivariable analysis was performed using Cox proportional hazard model to determine the independent association of each risk factor with clinical outcomes. The final list of covariates was also determined by removing variables that caused high collinearity, as assessed by variance inflation factors. The correlations between variables and outcomes were assessed with either Pearson’s R or Spearman’s ρ, as appropriate. Kaplan-Meier curves and log-rank tests were used to compare the cumulative incidence of clinical events between groups. Competing risk analysis was assessed to evaluate the cumulative incidence events’ curves in the population stratified by age. P-values <0.05 was considered statistically significant. All analyses were performed using R statistical software V.4.1.0 (R Foundation for Statistical Computing, Vienna, Austria) and Statistical Package for Social Sciences, V.25.0 (SPSS, PC version, Chicago, Illinois, USA).
Results
Study population
The study population consisted of 2129 patients with mAS and asAS, divided into those followed in the SOC (n=1878) and those in the HVC (n=251). The mean age was 76.5±12.4 years, and 992 (44.2%) were women (table 1). A total of 919 (43.2%) patients had asAS (773 (41.2%) in SOC and 146 (58.2%) in HVC, p<0.001), while the remaining 1210 (56.8%) patients had mAS (1105 (58.8%) in SOC and 105 (41.8%) in the HVC) (table 2).
Baseline characteristics, comorbidities and medical therapy of matched and unmatched patients with moderate and asymptomatic severe AS, divided into heart valve clinic versus standard of care
Baseline echocardiographic indices of matched and unmatched patients with moderate and asymptomatic severe AS, divided into heart valve clinic versus standard of care
Baseline, clinical and echocardiographic characteristics
Baseline characteristics, cardiovascular risk factors, comorbidities and medical therapy are reported in table 1. Patients in SOC were older (p<0.001), with a higher prevalence of arterial hypertension (p=0.041), coronary artery disease (p=0.003) and lower glomerular filtration rate (GFR) (p<0.001) (table 1 –unmatched columns). Medical therapy was also similar between the two cohorts (table 1). At echocardiogram, LVEF and Vmax were lower in the SOC group (p<0.01 for both; table 2). After 1:1 PSM, no differences were observed in baseline and echocardiographic characteristics between the two groups (tables 1 and 2 –matched columns). Details of PSM are reported in online supplemental figures S1 and S2.
Outcomes in the unmatched population
Mean follow-up was 4.8±1.8 years (4.8±1.7 years in HVC and 4.7±2 years in SOC, p=0.123). During the study period, a total of 822 patients (38.6%) died, 307 (14.4%) had HF hospitalisation and 596 patients (28%) underwent AVR, of whom 85.1% SAVR and 14.9% TAVR (online supplemental table ST1). Compared with SOC, Kaplan-Meier estimates showed a lower rate of unadjusted all-cause death and the composite endpoint in the HVC cohort (p<0.001 for both—figure 1A,C).

Kaplan-Meier survival curves for all-cause death and composite endpoint (all-cause death and heart failure hospitalisation) in patients with moderate and asymptomatic severe aortic stenosis. (A) All-cause death in unmatched population; (B) all-cause death in matched cohorts; (C) composite endpoint (all-cause death and heart failure hospitalisation) in unmatched population; (D): composite endpoint (all-cause death and heart failure hospitalisation) in matched cohorts. Blue curve: Heart Valve Clinic; red line: standard of care.
Findings and outcomes in the matched population
The number of cardiac consultations per year, exercise stress tests and BNP determinations were higher in the HVC cohort (p<0.001 for all). Moreover, a higher number of CTs was requested in the HVC group (p=0.002), with numerically higher values of calcium score, even though not statistically significant (table 3). Significant correlations were observed between number of visits and outcomes in HVC patients (r=−0.283, p=0.021 and r=−0.263, p=0.004 for all-cause and cardiovascular death, respectively) but not in SOC group (r=−0.164, p=0.112 and r=−0.016, p=0.918 for all-cause and cardiovascular death, respectively).
Main findings and outcomes of matched patients with mAS and asAS, divided into HVC versus SOC
Similar incidences of asAS and referral to AVR were reported between the two cohorts, with a shorter time between indication to AVR and less advanced New York Heart Association class in HVC (p<0.001 and p=0.032, respectively) (table 3). Compared with SOC, a lower rate of all-cause death, but not of the composite endpoint, was observed in the HVC cohort (HR=0.63, 95% CI 0.40 to 0.98, p=0.038; figure 1 B,D). This benefit was also observed for cardiovascular death (52.9% vs 76.1%, p=0.030) and all ranges of age (online supplemental table ST2). Stratifying the population by LVEF (< or >50%), there was a significantly lower survival in SOC patients when LVEF was reduced (p=0.005) (online supplemental figure S3). In the multivariable Cox regression model, after adjusting for confounding factors, the HVC was an independent predictor of reduced all-cause death (HR=0.54, 95% CI 0.34 to 0.85, p=0.007), together with younger age, absence of chronic obstructive pulmonary disease (COPD and higher LVEF (table 4, matched columns). In the competing risk regression analysis, stratifying the population by age (<70, 70–80, >80 years), the HVC approach was a significant predictor of all-cause mortality (p=0.011), but not of HF hospitalisation (p=0.275) (figure 2).
Predictors of all-cause death for patients with moderate and asymptomatic severe AS at univariable and multivariable analyses
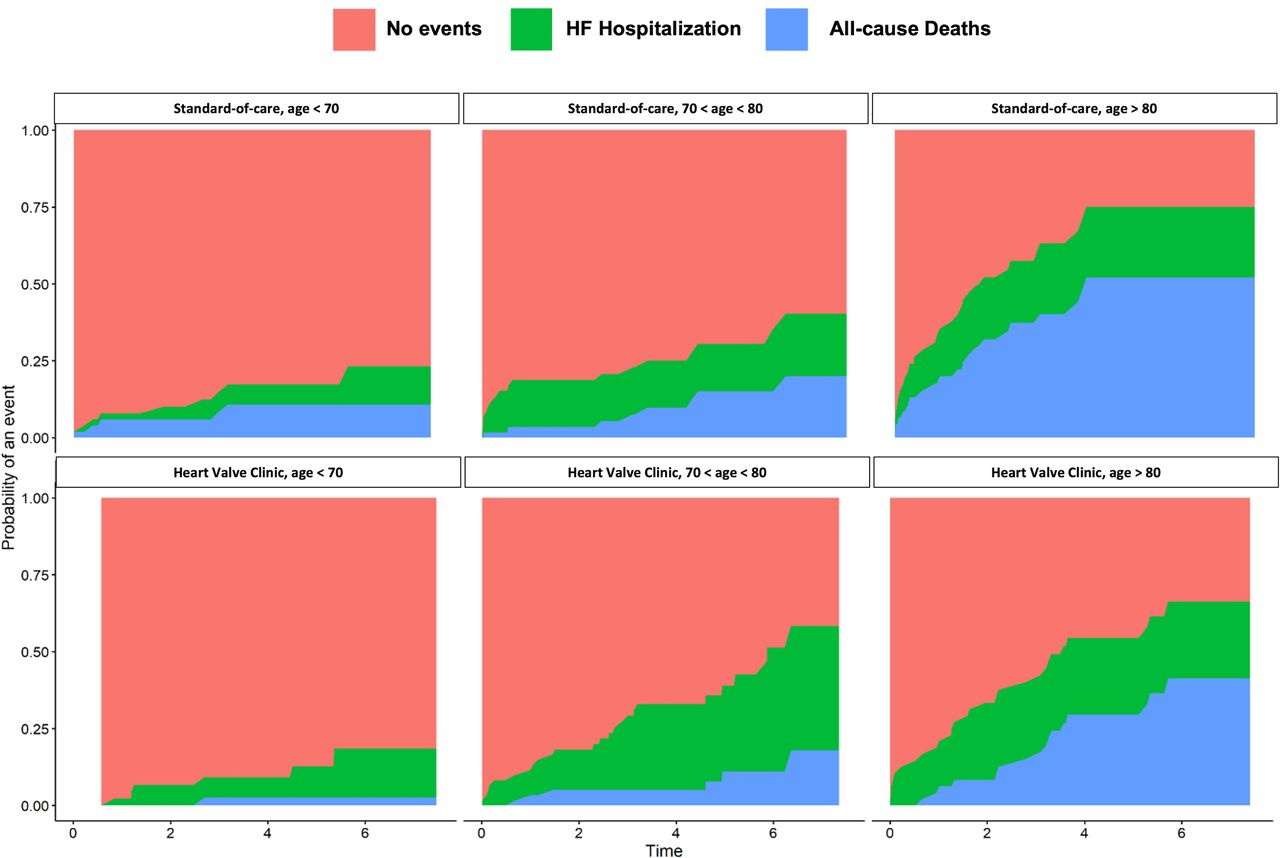
Competing risk analysis for all-cause death and heart failure (HF) hospitalisation with cumulative incidence curves, stratified by age (<70, 70–80, >80 years). The cumulative incidence curves were not significantly different for HF hospitalisation (p=0.275) but were significantly different for all-cause death (p=0.011).

Kaplan-Meier survival curves for all-cause death in patients with moderate and asymptomatic severe aortic stenosis (AS), separately. (A) All-cause death in patients with moderate AS—unmatched population; (B) all-cause death in patients with moderate AS—matched cohorts. (C) All-cause death in patients with asymptomatic severe AS—unmatched population; (D) all-cause death in patients with asymptomatic severe AS—matched cohorts. Blue curve: heart valve clinic; red line: standard-of-care group.
Impact of HVC in patients with mAS
Overall, 1210 (56.8%) patients had mAS (1105 (58.8%) in SOC and 105 (41.8%) in HVC, p<0.001). Baseline characteristics and echocardiographic parameters of crude and matched patients are reported in online supplemental tables ST3 and ST4. Details of PSM are reported in online supplemental figures S4 and S5. In patients with mAS, the HVC approach showed a higher survival rate (unadjusted p<0.001 vs adjusted p=0.003, figure 3 A,B). In the multivariable analysis, the HVC strategy was an independent predictor of reduced all-cause of death, together with younger age, higher GFR and absence of COPD (online supplemental table ST5).
Impact of HVC in patients with asAS
Overall, 919 (43.2%) patients had asAS (773 (41.2%) in SOC and 146 (58.2%) in HVC, p<0.001). Baseline characteristics and echocardiographic parameters of crude and matched patients with asAS are reported in online supplemental tables ST6 and ST7. Details of PSM are reported in online supplemental figures S6 and S7. In the Kaplan-Meier curve analysis, the higher survival of the HVC approach, compared with SOC, turned out to be non-significant after PSM (unadjusted p<0.001 vs adjusted p=0.25, figure 3 C,D). In the multivariable analysis, the HVC was not an independent predictor of reduced all-cause of death, unlike the use of beta-blockers, ACE inhibitors, lower age, lower tricuspid regurgitation gradient and higher LVEF (online supplemental table ST8).
Discussion
This is the first study investigating the outcome benefit of the HVC approach, compared with SOC, in patients with mAS and asAS. The main findings of our study include: (1) lower rate of adjusted all-cause and cardiovascular death in HVC compared with SOC; (2) the HVC approach was an independent predictor of reduced all-cause death after adjusting for all confounding factors; (3) the same benefit was not observed for the composite endpoint (all-cause death and HF hospitalisation); (4) the outcome benefit of HVC persisted in all groups of age and (5) in the subgroup analysis, the HVC was associated with reduced all-cause death in patients with mAS but not in those with asAS.
Benefits of HVC for patients with clinically significant AS
Over the last years, a deeper understanding of pathophysiology of VHD, refinements in multimodality imaging and improvements in surgical techniques and technology have resulted in the development of HVCes.18 Several data have been published on the organisation and requirements of HVC/HVCe.6 19–21 However, the outcome benefit of the HVC approach, compared with SOC, has never been investigated.
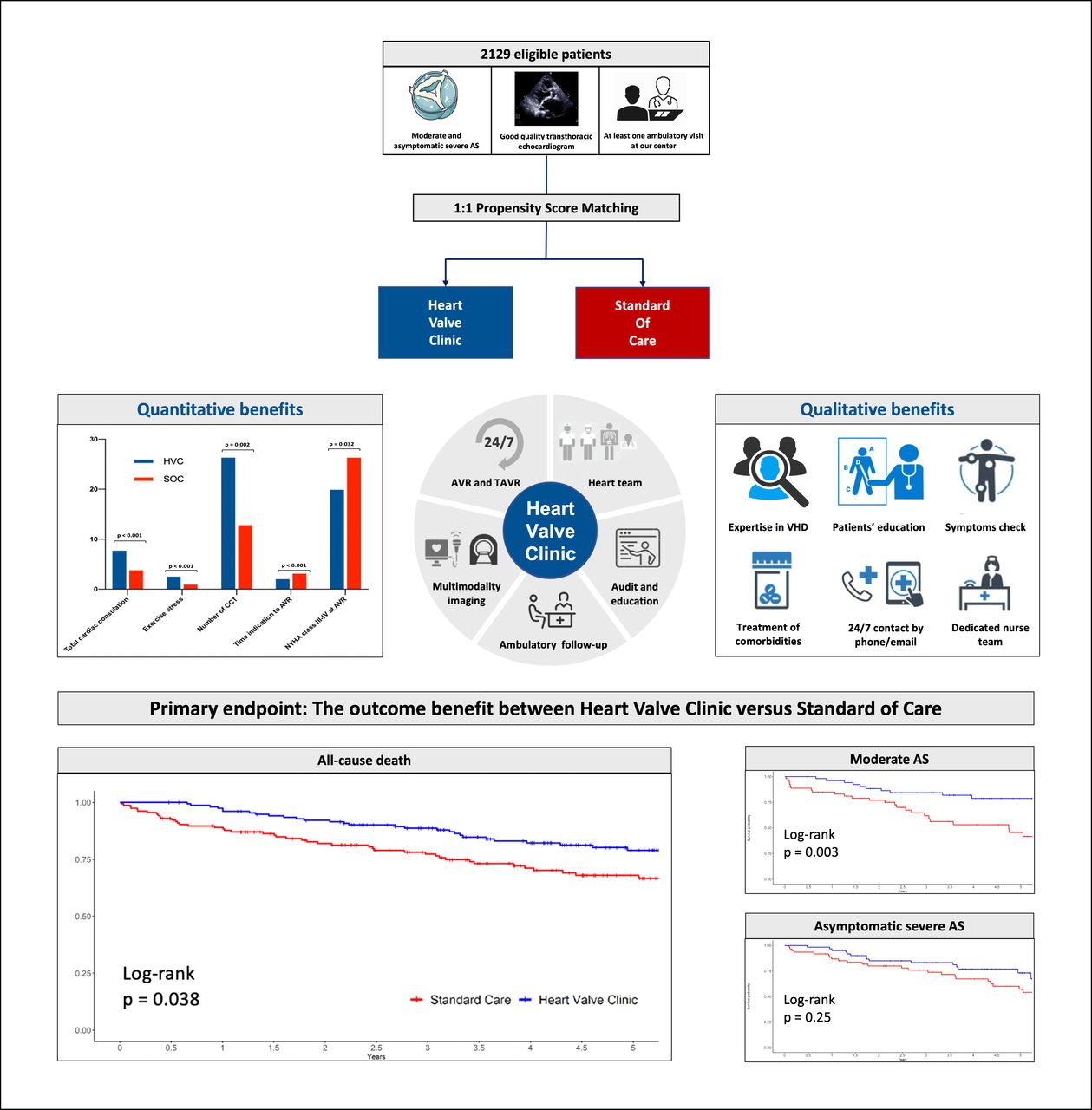
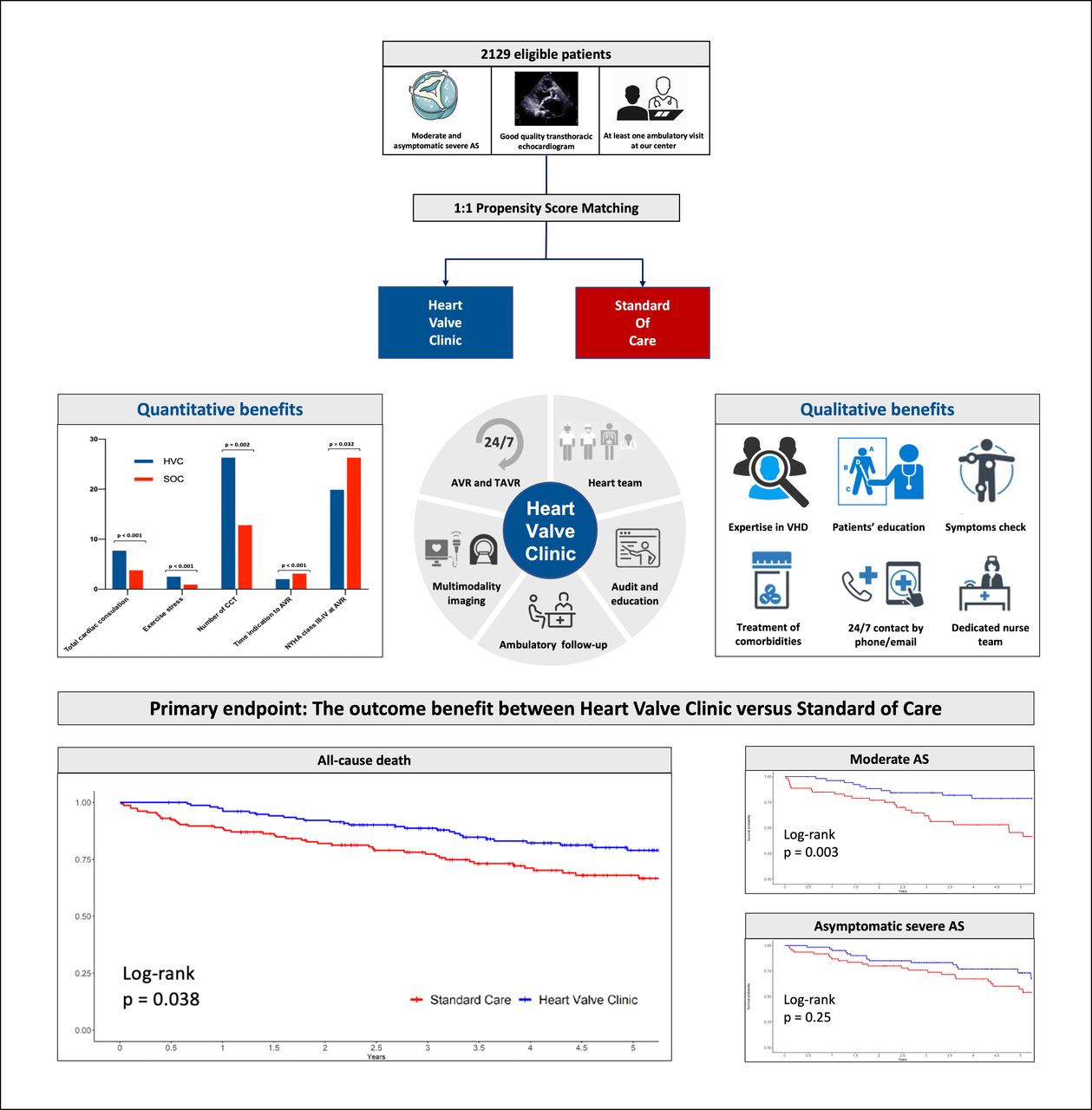
In the present study, we performed a direct comparison in the same institution between HVC and SOC for patients with mAS and asAS. This setting allowed a reduction of potential ‘environmental’ biases (same hospital, healthcare providers, and period). Moreover, biases related to baseline patients’ characteristics were reduced by PSM.17 Thus, for the first time, a benefit in outcome for HVC was demonstrated and confirmed for all age groups. These results could be explained by quantitative and qualitative differences in the healthcare service provided in HVC versus SOC (figure 4).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Summary of the main findings of the study. AS, aortic stenosis; AVR, aortic valve replacement; HVC, heart valve clinic; SOC, standard-of-care group; TAVR, transcatheter aortic valve replacement; VHD, valvular heart disease.
Quantitative benefits of HVC
In the present study, we observed a double number of consultations per year in HVC. Accordingly, HVC patients underwent a higher number (more than double) of exercise tests compared with SOC, allowing the early identification of exercise-induced symptoms. Moreover, a higher number of CT scans was requested in the HVC group, which provides further evidence of the closer follow-up and earlier detection of severe aortic valve calcification. The latter is one of the criteria considered to indicate AVR in asymptomatic patients with normal LVEF and exercise test.22–24 The same applies for BNP determinations, which were more frequent in HVC (p<0.001). Significant correlations were observed between number of visits and outcomes in HVC, but not in SOC. Although statistically significant, the correlation is not that ‘strong’, suggesting an equal importance of qualitative aspects related to the HVC strategy.
Qualitative benefits of HVC
The strength of HVCs versus SOC does not lie in the merely higher number of consultations/medical services in the former, but in the delivery of high-quality medical care and patient education by a dedicated team of experts. Indeed, the greater amount of time-per-visit in HVC (40 vs 20 min) allows the involved cardiologist to thoroughly review the echocardiographic findings; complete the TTE examination with supplementary images and data measurements, if necessary; interpret them in the overall patient clinical context and, more importantly, to share and explain the information to each patient. This results in patients’ education, a pivotal element of the HVC, which consists in: explaining the natural history of the disease, raising awareness on the signs and symptoms that could occur in follow-up, stressing the importance of prompt referral at their onset, providing means to inform the physician about changes in clinical status in the time between the scheduled consultations, and more generally the importance of controlling cardiovascular risk factors and adherence to medical indications/prescriptions. During consultations, the physician inquiries about the onset of AS-related symptoms and tries to determine their duration. The ‘educational strategy’ leads to benefits for both the patient and the physician. Due to a deeper awareness of the disease, the patient feels more involved in the decision-making process and is more prone to follow the given medical indications/prescriptions. Closer medical contact allows better risk stratification, optimisation of follow-up planning and tailoring of comorbidities treatment, which could have prognostic implications. Moreover, experience in VHD implies a deeper understanding of the echocardiographic examination, detection of details or unreported findings, which could be missed by other cardiologist specialists, allowing a ‘patient-tailored’ follow-up planning.
Management of patients with clinically significant AS
The HVC approach might play a pivotal role in managing patients with mAS and asAS, optimising the timing of indication to AVR.5 19 Indeed, symptoms could be recognised at an earlier and less severe stage before the occurrence of LV dysfunction.19 This evidence is further supported by the significantly lower survival of SOC patients with LVEF <50% and the shortened duration of symptoms before AVR in the HVC group (almost half-time than the SOC group; table 3). Indeed, the severity of preoperative symptoms is a marker of increased operative risk, with worse survival rates for patients with severe symptoms.6 25 Patients managed in HVC underwent AVR in a less advanced stage, with less waiting time between indications and AVR. This is crucial considering a mortality risk on the waiting list for surgery of about 15% per year.26
In the natural history of AS, HF occurrence adversely impacts prognosis. This is clearly shown in the competing risk analysis and supported by the similar rate of the composite endpoint, including HF hospitalisation between the two groups. These results could be driven by the similar number of HF hospitalisation and referral to AVR in patients with asAS included in both cohorts. Moreover, due to closer medical relationship with the referring physician, patients followed in HVC are more likely to undergo hospitalisations in case of clinical deterioration to optimise medical therapy and to reassess the progression and severity of AS. Therefore, comprehensive management would be beneficial, especially for patients with mAS, for whom the appropriate follow-up timing to prevent the onset of symptoms and HF occurrence might be challenging, compared with those with asAS, who are more directly referred to AVR. Accordingly, the outcome benefit of the HVC in the overall population is mainly driven by the outcome benefit of the subgroup of patients with mAS.
Study limitations
Our results should be interpreted considering some limitations. First, due to the observational study design, the study results should be considered hypothesis-generating. Second, the assessment of myocardial strain to identify subclinical LV dysfunction was not systematically performed. Third, no quality-of-life questionnaires at baseline and during follow-up were administered. Fourth, among patients fulfilling the inclusion criteria, nine were excluded because of more than 20% of missing values in the collected data to reduce potential bias.
Conclusions
In patients with AS, the HVC approach was associated with a lower risk of all-cause and cardiovascular mortality at long-term follow-up compared with SOC. HVC was associated with more efficient patient management in terms of education, treatment and second-level diagnostic tests and was an independent predictor of reduced all-cause death. Our findings are hypothesis-generating and provide new insights into the benefit of HVC in VHD setting, highlighting the potential to improve patient care and clinical outcomes.
Data availability statement
Data are available on reasonable request.
Ethics approval
This study involves human participants. This registry was approved by the institutional review board of the Onze-Lieve-Vrouw Clinic in Aalst, Belgium, with the registration no 2022/028. Participants gave informed consent to participate in the study before taking part.
Acknowledgments
The authors thank the physicians and patients of involved institutions.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @EGallinoro, @EricWyffels
Contributors MBele and PP carried out the statistical analysis. PP and MBelm wrote the first draft of the manuscript. EG, CDC, NM, DTB, CD, JS and SB collated data. JS, SB, ID, FC, BS, FVP, MP, CC, EW, MV, EB, JB and GVC corrected and approved the revisions and final version of the manuscript. GVC, PP and MBelm are responsible for the conception, funding and design of the study. GVC is the guarantor of this work.
Funding PP, MBelm and DTB report receiving a research grant from the CardioPaTh PhD Program.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, conduct, reporting or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.
Linked Articles
- Editorial
- Correspondence
- Correspondence