Article Text

Abstract
Objective: Progression of neointimal stent coverage (NSC) and changes in thrombus were evaluated serially by coronary angioscopy for up to 2 years after sirolimus-eluting stent (SES) implantation.
Design: Serial angioscopic observations were performed in 20 segments of 20 patients at baseline, and at 6 months and 2 years after SES implantation. NSC was classified as follows: 0, uncovered struts; 1, visible struts through thin neointima; or 2, no visible struts. In each patient, maximum and minimum NSC was evaluated. Existence of thrombus was also examined.
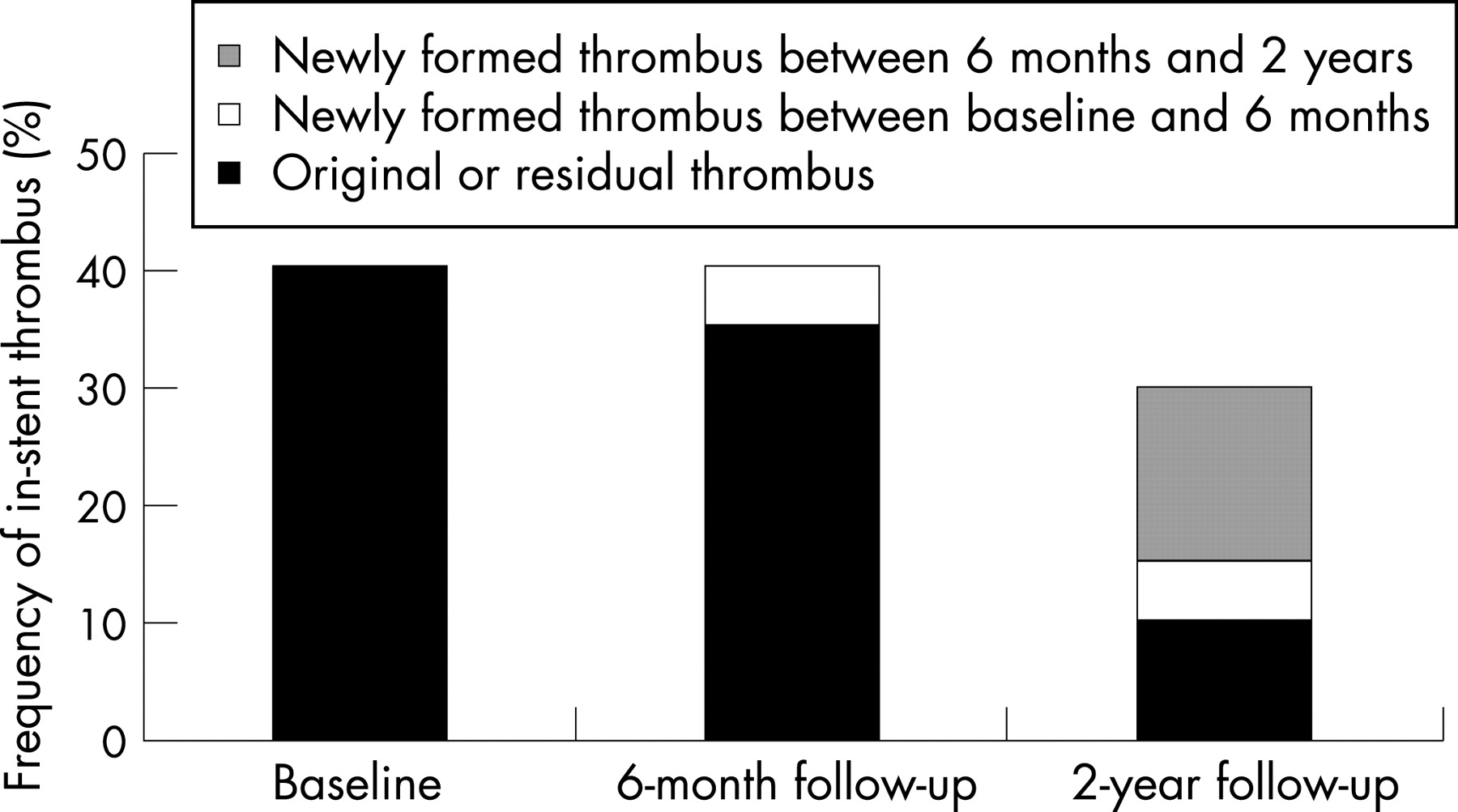
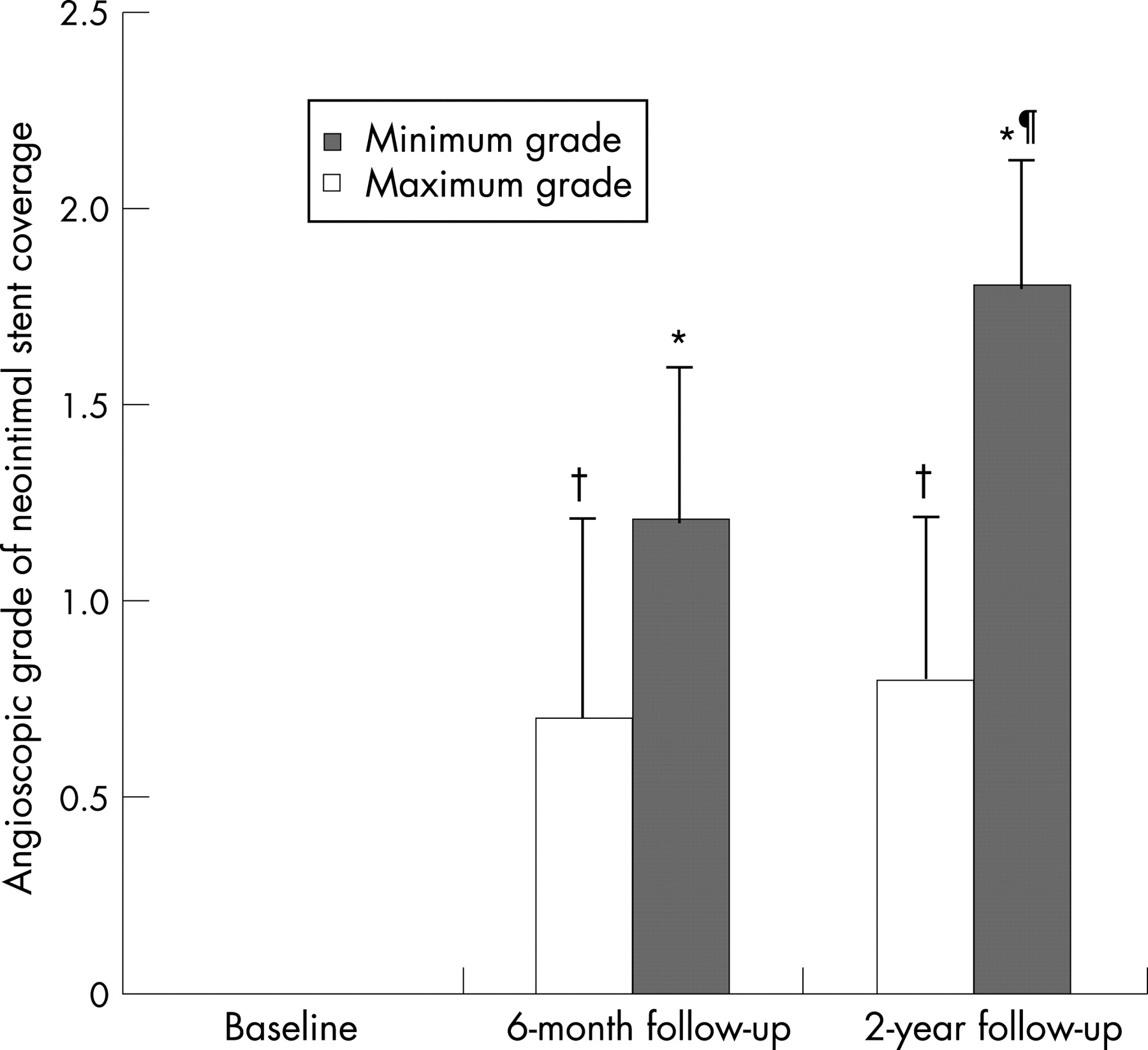
Results: The maximum NSC increased from 6 months to 2 years (1.2 (0.4) vs 1.8 (0.4), respectively, p = 0.005), while the minimum NSC did not change (0.7 (0.5) vs 0.8 (0.4), respectively, p = 0.25). The prevalence of patients with uncovered struts did not decrease from 6 months to 2 years (35% vs 20%, respectively, p = 0.29). Although there were no thrombus-related adverse events, new thrombus formation was found in one patient (5%) at the 6-month, and in four patients (20%) at the 2-year follow-up evaluations. Frequencies of thrombus inside the SES at baseline, 6 months and 2 years did not differ one from another (40%, 40% and 30%, respectively; p = NS).
Conclusions: Neointimal growth inside the SES progressed heterogeneously. Uncovered struts persisted in 20% of the patients for up to 2 years and subclinical thrombus formation was not a rare phenomenon.
Statistics from Altmetric.com
Recently, occurrence of late stent thrombosis (LST) after drug-eluting stent implantation has became a major clinical concern.1–3 A long-term follow-up study demonstrated that LST occurs at a constant rate of 0.6% a year for up to 3 years after drug-eluting stent implantation.3 Pathological investigation shows that delayed arterial healing, characterised by an incomplete endothelialisation and persistence of fibrin, has a key role in the occurrence of LST.4 5 Moreover, a powerful predictor of LST is the existence of uncovered struts without endothelialisation.5 We therefore proposed the hypothesis that the uncovered struts of a sirolimus-eluting stent (SES) remain for an extended period of time.
Coronary angioscopy provides a direct visualisation of the lumen and detailed information on the condition of neointimal stent coverage (NSC) and thrombus.6–8 This imaging modality has the advantage of allowing the identification of an intracoronary thrombus.8 Presently, no long-term angioscopic follow-up data after SES implantation are available. We herein present our findings as derived from angioscopic examination, focusing on the long-term serial changes in the NSC, especially the uncovered stent struts, and the presence of thrombus inside the SES.
PATIENTS AND METHODS
Patient group
Serial angiographic and angioscopic follow-up examinations after SES (Cypher, Cordis Corp, Miami Lakes, Florida, USA) implantation were performed for 20 segments in 20 patients. Exclusion criteria were (a) acute myocardial infarction within 48 hours from onset; (b) contraindication to aggressive antiplatelet treatment; (c) restenotic lesions; (d) lesions of coronary bypass grafts; (e) low ejection fraction of the left ventricle (<30%); (f) unprotected left main disease or ostial lesions; and (g) tortuous vessels or heavily calcified vessels proximal to the target lesions. All patients received dual antiplatelet treatment (aspirin + ticlopidine) for more than 48 hours before the stenting for the prevention of acute or subacute thrombosis. During this study period, clopidogrel had not been approved for clinical use in Japan. The medical ethics committee at our hospital approved this study, and written informed consent was obtained from all patients before catheterisation.
Clinical demographics
Patient demographics were obtained by hospital chart review. Culprit lesions (target lesions of the stenting) were identified by a combination of electrocardiographic findings, wall motion abnormalities on left ventriculography or echocardiographic findings, and angiographic lesion morphology. A serum creatinine value ⩾180 μmol/l or regular haemodialysis qualified for the definition of chronic renal failure. Ejection fraction of the left ventricle was measured by ventriculography or echocardiography.
Coronary angioscopic imaging
The coronary angioscopic procedure has been previously reported.7 Serial angioscopic examinations were scheduled immediately, 6 months and 2 years after the SES. Culprit lesions and the entire stented segments were observed with an angioscopic catheter. Angioscopic images were recorded on digital videotape for later analysis and the exact position of the angioscopic catheter at the observed segment was recorded by fluoroscopy to ensure a reliable comparison.
Definition and analysis of angioscopic findings
A thrombus was defined as a coalescent red or white superficial or protruding mass, but clearly a separate structure that remained despite being flushed with a saline solution.7 The extent of the NSC was evaluated by a grading system according to our previous report.6 In brief, NSC was classified as follows: 0, uncovered struts; 1, visible struts through thin neointima; or 2, no visible struts under the neointima (complete coverage). Stent struts located at the orifice of the side branches were excluded from this evaluation. In each patient, the grade of the best-covered segment was defined as the maximum NSC and that of the worst-covered segment was defined as the minimum NSC. Based on the position of the angioscopic catheter on fluoroscopy, the same segments were evaluated at a 6-month and 2-year follow-up. Two observers who were unaware of the patients’ information analysed the angioscopic images, and intra- and interobserver agreements were evaluated.
Clinical follow-up
Regular clinical follow-up visits occurred every month or every other month for up to 2 years after stenting. Major adverse cardiac events were defined as acute coronary syndrome, cardiac sudden death and repeat target lesion revascularisation.
Statistical analysis
Data are presented as mean (SD). Categorical variables are presented as frequencies and they were analysed by either χ2 test or Fisher exact test. Discontinuous data (grade of the NSC) were tested by the Mann-Whitney U test with Bonferroni’s correction after a Kruskal–Wallis test. A p value of <0.05 was considered to be significant.
RESULTS
Clinical demographics
Table 1 summarises the clinical demographics. Dual antiplatelet treatment was discontinued in two patients 6 months after the SES implantation based on the angioscopic confirmation of complete NSC. These two patients thereafter received aspirin monotherapy while the other 18 patients continued with the administration of dual antiplatelet treatment. The reference diameter of the target lesions was 2.82 (0.24) mm. Stent deployment pressure was 17.8 (3.6) atm, and dilatation after stenting was added in all procedures.
Major adverse cardiac events
There were no abnormal qualitative angiographic findings such as filling defect, haziness or wall irregularity within the SES segment at the follow-ups. One patient received target lesion revascularisation (repeat SES implantation) at the 2-year follow-up owing to angiographic late restenosis. No other major adverse cardiac events occurred during the 2-year follow-up.
Neointimal stent coverage on angioscopy
The values of maximum NSC at baseline, 6-month and 2-year evaluations were 0 (0), 1.2 (0.4), and 1.8 (0.4), respectively. The maximum NSC increased significantly from baseline to 6-month evaluation, and from 6-month to 2-year evaluation (p<0.001 and p = 0.005, respectively). The values of minimum NSC at baseline, 6-month and 2-year evaluations were 0 (0), 0.7 (0.5), and 0.8 (0.4), respectively. At 6-month and 2-year follow-ups, the minimum NSC was higher than at baseline (baseline vs 6-month; p<0.001, and baseline vs 2-year follow-up; p<0.001). The minimum NSC did not increase significantly from the 6-month to 2-year follow-up (p = 0.25) (fig 1). Uncovered struts, grade 0 of the NSC, were found in 20 patients (100%) at baseline, seven patients (35%) at the 6-month follow-up and four patients (20%) at the 2-year follow-up. The prevalence of patients with uncovered struts did not decrease from the 6-month to 2-year follow-up (p = 0.29). Intra- and interobserver agreements of the grade of the NSC were 95% and 90%, respectively.

Thrombus on angioscopy
At baseline, intracoronary thrombi were observed in 40% of patients. During the follow-up period, residual thrombi were found in seven patients (35%) at 6 months and in two patients (10%) at 2 years. One thrombus in one patient (5%) was newly recognised at 6 months and persisted up to 2 years. Additionally, three thrombi in three patients (15%) were newly found at the 2-year follow-up. New thrombus formation was recognised in 1/7 (14%) patients with uncovered struts at 6 months and in 3/4 (75%) patients with uncovered struts at 2 years. Three of four (75%) of the new thrombi attached to the uncovered struts. All four patients who had newly formed thrombi received dual antiplatelet treatment for up to 2 years. As a result, the frequencies of thrombi at baseline, 6-month follow-up and 2-year follow-up were 40%, 40% and 30%, respectively (fig 2), and they did not differ one from another (p = 0.51). Intra- and interobserver agreements of thrombus were 100% and 95%, respectively.
{kind=link}
{kind=link}
DISCUSSION
This investigation demonstrated that incomplete NSC persisted in 20% of the patients for up to 2 years, and six (30%) patients had subclinical thrombi within the SES segments at the 2-year follow-up.
In our series, the maximum NSC increased gradually from baseline to the 2-year follow-up. From this perspective, the angioscopic NSC after SES implantation advanced steadily for up to 2 years. In contrast, the minimum NSC almost reached its peak at the 6-month follow-up and did not significantly increase between 6 months and 2 years. These findings imply that the NSC within the SES segment progressed unequally and support recent pathological finding.5 Moreover, the prevalence of patients with uncovered struts did not decrease from 6 months to 2 years. Our results suggest that struts which have difficulty in achieving coverage by the neointima may still remain as uncovered struts for an extended period of time. The uncovered struts, the most important measure of the angioscopic findings, persisted in 20% of the patients for up to 2 years. Nevertheless, no thrombus-related adverse events occurred in this study group. Possibly, the existence of the uncovered stent struts is not an absolute condition, but a necessary condition for the occurrence of LST. In other words, when uncovered struts are present, additional special factors, such as discontinuation of antiplatelet treatment,1 antiplatelet resistance,9 intrinsic thrombogenicity or coronary flow problems, may trigger the development of LST.
The prevalence of thrombus including original, residual and newly developed thrombus did not decrease from baseline to 2 years. In previous postmortem research, dual antiplatelet treatment was continued in 18/23 (78%) patients who died of LST after drug-eluting stent implantation.5 Our angioscopic observation also demonstrated that in-stent thrombus within the SES segments could arise during dual antiplatelet treatment. In this study, 75% of newly formed thrombi attached to the uncovered struts. These angioscopic findings suggested that in-stent thrombus formation in the late phase was caused by the existence of uncovered struts without neointima. In one case, the uncovered struts could not be identified around the thrombus. Possibly, detection of uncovered struts by angioscopy was limited because the thrombus might have concealed them. Although none of the thrombi identified by angioscopy contributed to the occurrence of LST, our angioscopic investigation supported the premise that the uncovered struts of the SES persisted for a long time and that in-stent thrombus formation originated in the uncovered struts without neointima. Our results suggest that patients with uncovered struts may have a potential risk for the occurrence of LST.
The US Food and Drug Administration recommends the continuation of dual antiplatelet treatment for longer than 12 months after drug-eluting stent implantation. Nevertheless, there is no scientific evidence for the discontinuation of dual antiplatelet treatment at 12 months after drug-eluting stent implantation. In this study, analysis of the clinical factors affecting persistent uncovered struts or thrombus formation could not be achieved because of the small number of patients. Further large-scale studies are necessary to determine what factors influence the persistence of uncovered struts or thrombus formation. The cause of LST is probably multifactorial. Furthermore, patient-related factors (variability from patient to patient) may contribute to the persistence of uncovered struts or thrombus formation. Results of this study do not confirm the optimal duration of antiplatelet treatment after SES implantation. However, although this follow-up study had no direct linkage with LST, our angioscopic findings indicate that prolonged dual antiplatelet treatment for the prevention of LST is required for some patients who undergo drug-eluting stent implantation, especially for those patients with uncovered stent struts or in-stent thrombus.
There were several limitations to this study. Our findings were based on observations in a relatively small number of patients, but serial angioscopic observation demonstrated detailed features inside the SES. In general, the angioscopic evaluation was not quantitative. Nevertheless, the most important findings in this study were the qualitative identification of the uncovered struts and thrombi.
In conclusion, the serial angioscopic follow-up observations after the SES implantation demonstrated that an incomplete NSC, recognised as uncovered stent struts, persisted for a long time, and that thrombus formation within the SES segment originated in the uncovered struts. Subclinical thrombus identified by angioscopy was not a rare phenomenon. Further careful attention to the occurrence of LST in patients with uncovered stent struts and in-stent thrombi is thus required.
Acknowledgments
We thank Shunsuke Shimada and Yoshihiro Abe for their excellent assistance in our catheter laboratory.
REFERENCES
Footnotes
This study was supported in part by a research grant (to Dr Xie) from Japan-China Sasakawa Medical Fellowship.
Competing interests: None.
- Abbreviations:
- LST
- late stent thrombosis
- NSC
- neointimal stent coverage
- SES
- late stent thrombosis