Article Text

Statistics from Altmetric.com
001 THE REACT (RESCUE ANGIOPLASTY VS CONSERVATIVE TREATMENT OR REPEAT THROMBOLYSIS) TRIAL: LONGER-TERM FOLLOW-UP
A. Gershlick, K. Fairbrother, A. Carver, S. Stevens, G. Richardson. University Hospitals of Leicester, Leicester, UK
Introduction: Although primary PCI is increasingly used to treat patients with STEMI, logistic reasons dictate that thrombolysis remains an important reperfusion option. However in up to 40% of patients lysis fails (defined as either TIMI flow grade <3 or <50% ST-segment resolution at 90 min). Until the REACT trial there was little evidence to support rescue-PCI (R-PCI) as a treatment option. REACT, reporting in 2005, showed in 427 patients presenting with failed lysis randomised to repeat lysis (R-Lysis), conservative therapy (C) or R-PCI, that R-PCI improved outcome affecting all composites MACCE at 6 months; event-free survival rates were RPCI 84.6%; R-Lysis 68.7%; C 70.1% (p = 0.004). Hazard ratio (HR) RPCI vs R-Lysis 0.45 (95% CI 0.27–0.75, p = 0.002) and vs C 0.47 (0.28–0.79, p = 0.004). The data according to last treatment received within the 12 h following randomisation were analysed to ensure that it was the R-PCI rather than the randomisation to that group that was beneficial. Results were further improved. Of 142 patients who actually received R-Lysis, 44 (31.0%) suffered at least one component of the composite end-point as did 46 (29.2%) of 154 who were treated conservatively compared to only 18 (13.7%) of 131 who actually received R-PCI. HR for R-PCI vs R-Lysis was 0.40 (0.23–0.70, p<0.001) and vs C 0.42 (0.24–0.72, p = 0.0018). The current abstract also addresses whether these shorter-term benefits are maintained.
Methods and Results: A total 91% of trial patients were contacted by telephone/seen at 12 months follow-up. Event-free survival curves at this time showed an interaction (p = 0.004). The HR for R-PCI vs R-Lysis was 0.47 (0.29–0.75, p = 0.002), and vs C 0.51 (0.32–0.83, p = 0.007). The need for subsequent revascularisation (a secondary end-point that was not significantly different at 6 months) was required significantly less in the R-PCI group at one year—HR for R-PCI vs R-Lysis 0.52 (0.32–0.86, p = 0.010) and vs C 0.53 (0.32–0.88, p = 0.014). While difference in mortality between the groups at one year did not reach sigificance, early analysis of late (median 4.6 year) mortality suggests significant benefit in those treated with R-PCI out to this time: death for R-Lysis 21% (67% data collected), C 27% (66% data) and R-PCI 11% (71% data), p = 0.015.
Conclusions: Rescue PCI after failed lysis should be mandated in protocols of AMI mangement. Early benefits appear to be maintained.
acute myocardial infarction; rescue angioplasty; percutaneous coronary intervention
002 DELAYS IN DELIVERING PRIMARY ANGIOPLASTY WITH INTERHOSPITAL TRANSFER RESULT IN LIMITED MORTALITY BENEFIT IN REAL-WORLD PRACTICE IN THE CONTEXT OF A HIGH-QUALITY THROMBOLYSIS SERVICE
M. Dalby1, R. Kharbanda1, G. Ghimire1, J. Spiro1, E. Hutchison1, M. Teoh2, R. Grocott-Mason2, M. Roughton1, A. Mitchell1, M. Mason1, C. Ilsley1. 1Royal Brompton & Harefield NHS Trust, London, UK; 2Hillingdon Hospital NHS Trust, London, UK
Introduction: Primary percutaneous coronary intervention (PPCI) is regarded as the preferred reperfusion therapy in ST elevation myocardial infarction even if interhospital transfer (IHT) is required. We introduced PPCI for both direct and interhospital admissions in a region with a well-developed, high-quality thrombolysis service. We tested the hypothesis that the inevitable delays imposed by IHT would limit the benefit of PPCI.
Method: We prospectively analysed in consecutive cases our time-interval and 30 day mortality for 24 months from April 2004–March 2006, and made a retrospective comparison with thrombolysis era data from the previous two years using Kaplan-Meir methodology to enhance analysis of performance. There was no age limit.
Results: With direct admission door to balloon times were similar to the door to needle thrombolytic era data and <60 min in all cases. First professional contact-balloon times were <90 min in 90% of patients. Mortality with direct admission PPCI was significantly lower than in the thrombolysis era (table; χ2 p<0.001). With IHT door-balloon times were <90 minutes in 40% and first professional contact-balloon times were <90 minutes in 7% of cases. IHT PPCI mortality was similar to the thrombolysis era. Total length of stay was reduced from 8.1 days in the thrombolysis group to 3.7 days for the PPCI group.
Conclusion: Direct transfer for PPCI with very rapid door to balloon times can yield a large and significant mortality benefit. However, real-world interhospital transfer for PPCI limits the mortality benefit of this strategy over rapid thrombolysis.
myocardial infarction; primary angioplasty; interhospital transfer
003 ASSOCIATION BETWEEN THE PURINERGIC RECEPTORS P2X4, P2X6 AND P2X7 GENETIC VARIATION AND BLOOD PRESSURE IN A BRITISH POPULATION
J. Palomino Doza, B. Keavney, T. Rahman, J. Eden, R. Hussain. Institute of Human Genetics, University of Newcastle upon Tyne, Newcastle upon Tyne, UK
Introduction: Blood pressure is a quantitative trait clustered in families with heritability estimated at 30–60% in the literature. The P2X receptor family has been implicated in neural impulse transmission, ion exchange, renal function, vasomotor response, and possibly in mediating the effect of aldosterone. The physiological role of this group of receptors and previous linkage data suggest them as strong candidate genes in hypertension. The hypothesis of this study is that blood pressure variation is a trait associated with genetic variation in the purinergic receptors P2X4, P2X6 and P2X7.
Methods: Based on the hapmap project data from the CEU population 28 SNPs were chosen in total, using a tagging strategy. Five SNPs in P2X4, 9 in P2X6 and 14 in P2X7 were genotyped. SNPs with a minimum allele frequency of 0.05 and a LD threshold of 0.85 were included. The population, comprising 1248 European individuals from 248 families, was recruited based on one hypertensive subject in each family. Office and ambulatory 24 h BP measurements were performed. The SNPs were genotyped using homogeneous mass extension reactions and mass spectrometry. Categorical analysis calculating odds ratio, confidence intervals and significance level were performed based on the diagnosis of hypertension. Quantitative trait analysis was performed using the QTDT software, testing additive genetic models and controlling for significant clinical covariates.
Results: The allele and haplotype frequencies in the sample are in close similarity to the hapmap data. In the analysis for hypertension affection status the major allele in the markers rs9625334 and rs2255371 confers an OR of 1.27 and 0.77 respectively (p = 0.02). The homozygous state of these markers confers and OR of 1.42 and 0.7 respectively (p = 0.04 and 0.02). In the quantitative analysis, the marker rs8141816 in the P2X6 receptor was significantly associated (p = 0.01–0.03) with both SBP and DBP in office readings and SBP in both daytime and night-time ambulatory readings. The marker rs591874 in the P2X7 receptor was significantly associated (p = 0.002–0.02) with both SBP and DBP in office readings and both daytime and night-time ambulatory readings. The marker rs503720 in the same gene was significantly associated (p = 0.03) with SBP and DBP during the day and SBP in office readings. The P2X4 SNP rs2303998 was significantly associated with SBP and DBP during both office and day ambulatory readings.
Conclusions: This study suggests that the P2X receptors P2X4, P2X6 and P2X7 are involved in the regulation of blood pressure and susceptibility to hypertension. Further functional analyses are required to elucidate the functional implications of these genetic findings.
purinergic receptor; genetic variation; hypertension
004 INTEGRATED GENETIC LINKAGE ANALYSIS AND EXPRESSION PROFILING IN THE RAT HEART TO IDENTIFY PRIMARY DRIVERS OF CARDIAC HYPERTROPHY
R. Sarwar1, E. Petretto1, H. Lu1, M. Kumaran1, B. Schroen2, J. Fischer3, N. Hubner3, J. Mangion1, Y. Pinto2, M. Pravenec4, T. Aitman1, S. Cook1. 1MRC-CSC Imperial College, London, UK; 2CARIM Maastricht University, Maastricht, Netherlands; 3Max Delbrück Center, Berlin, Germany; 4Czech Academy of Sciences, Prague, Czech Republic
Introduction: Although the environmental regulation of left ventricular mass (LVM) has been extensively investigated, the genetic components of this clinically important phenotype remain unclear. LVM is a quantitative trait, and its genetic determinants can be mapped to distinct chromosomal regions as physiological quantitative trait loci (pQTLs).
Hypothesis: Genes whose cardiac expression is genetically determined are strong candidates for primary drivers of cardiac phenotypes, such as LVM.
Methods: We used linkage analysis combined with genome-wide expression profiling in the largest recombinant inbred (RI) rat strain panel to map the genetic determinants of cardiac gene expression, taking into account naturally occurring variation in blood pressure. The LVs were harvested and RNA was extracted from the 30 RI rat strains (n = 4 males/strain) and quantified with individual Affymetrix RAE 230 2.0 microarrays (31 099 probesets/array) and gene expression was mapped to the genome using published approaches with correction for multiple testing. Candidate genes for LVM were defined as a gene whose genetic regulation was due to a sequence polymorphism near its own genomic location (cis-regulated expression QTL, eQTL) that also coincided with a previously described LVM pQTLs. Candidate genes identified in the rat were then prioritised by assessing whether their human orthologues were dynamically regulated in human heart biopsies from patients with cardiac hypertrophy undergoing surgery for aortic stenosis (n = 20) compared to controls (n = 7). Genes prioritised in human studies were further examined in 2 models of hypertrophy in vitro and in vivo.
Results: We showed that the genetic regulation of cardiac transcription is predominant when compared to environmental effects. This enabled us to map 4587 eQTLs to the genome (genome-wide p<0.05) as the major inherited control points for gene expression in the rat heart. A subset of ∼50 cis-regulated eQTL genes that colocalised with previously described LVM pQTLs are candidate genes for cardiac hypertrophy. Orthologues of 7 of these candidate genes were found to be dynamically regulated in human heart hypertrophy. We went on to refine the map location of a rat LVM pQTL in the RI strain panel and identified sequence polymorphisms in 2 of the 7 prioritised candidate genes that were encoded within this genomic location. We showed that one of these candidate genes (mimecan or osteoglycin precursor) is dynamically regulated in in vitro and in vivo models of hypertrophy.
Conclusion: eQTLs provide a new and powerful systems approach to dissecting the pathophysiology of genetically complex traits. This is the first study of this kind in the heart and has provided new data on the genes and pathways that determine LVM in rodents and humans. These data stand to advance significantly our understanding of LVM, cardiac biology and systems approaches.
genetical genomics; microarray; hypertrophy
005 MUTATIONS IN THE CARDIAC TRANSCRIPTION FACTOR TBX1 MAY CONTRIBUTE TO SUSCEPTIBILITY TO TETRALOGY OF FALLOT IN PATIENTS WITHOUT 22Q11 DELETION
H. Griffin, B. Keavney, J. Goodship, TheChange Study Group. Institute of Human Genetics, Newcastle upon Tyne, UK
Introduction: Tetralogy of Fallot (TOF) is a relatively common form of congenital heart disease that affects the cardiac outflow tract. Previous studies have demonstrated a strong genetic component to disease risk (Calcagni et al. 2006, Burn et al. 1998). TOF can occur as part of 22q11 Deletion syndrome (22q11DS). Mouse models have implicated TBX1 as the likely haploinsufficient gene within the deleted region responsible for cardiac outflow tract defects (Merscher et al. 2001, Lindsay et al. 2001, Jerome and Papaioannou 2001). TBX1 is a transcription factor expressed in the secondary heart field. Signalling by TBX1 to downstream fibroblast growth factors (FGFs) regulates cellular proliferation, differentiation and migration, and leads to development of the outflow tract region of the heart. TBX1 is a candidate gene for non-sydromic cases of TOF.
Methods: We sequenced the exonic regions of TBX1 in a panel of 93 TOF probands, using fluorescence-based technology. Probands were confirmed not to have 22q11 deletion by FISH or MLPA approaches. Seven previously unreported variants of TBX1 were identified in the panel of 93 TOF probands. Two of the variants, each seen in an individual proband, were not present in over 1000 control chromosomes. Both these variants alter the protein sequence of TBX1 and are present in an evolutionarily conserved region of TBX1. Of the five other variants four were seen in more than one proband and the other was seen in a single proband. These five variants did not alter the protein sequence of TBX1, were present in the panel of 1000 control chromosomes and may represent rare population variation or possible contributing factors to TOF in a complex multifactorial model of disease susceptibility.
Results: The two novel variants could affect the ability of TBX1 to activate transcription of the downstream FGFs, affecting cellular proliferation, differentiation, migration and development of the outflow tract of the heart. In vitro assay are currently underway to investigate the functionality of the novel TBX1 variants.
Conclusions: TOF is a complex disease, most likely heterogeneous in nature with environmental influences. Potential mutations in TBX1 may only account for a small proportion of cases. However identification of novel TBX1 variants will lead to a greater understanding of gene function and implicates other candidate genes acting in the same genetic pathways as TBX1 in the pathogenesis of TOF.
tetralogy of Fallot; TBX1; complex genetics
006 ENDOTHELIAL PROGENITOR CELLS IN ADULTS WITH AND WITHOUT CORONARY ARTERY DISEASE AND THEIR HEALTHY ADULT OFFSPRING: EVIDENCE FOR POTENTIAL GENETIC REGULATION
A. Whittaker, J. Moore, M. Vasa, S. Stevens, N. Samani. Department of Cardiovascular Sciences, University of Leicester, Leicester, UK
Introduction: Endothelial progenitor cells (EPCs) represent a circulating pool of precursor cells that are capable of endothelial repair and neovascularisation. Their number and activity is impaired in patients with coronary artery disease (CAD). The factors regulating EPC activity are poorly understood. We hypothesised that EPC activity may be partly genetically determined. We examined this possibility by comparing EPC numbers in parents (both with and without CAD) and their healthy adult offspring.
Methods: 102 subjects, comprising 51 non-diabetic adults (45–65 years) plus one of their healthy adult offspring (age range 19–43 years) were studied. The parental generation included both subjects with severe premature CAD (n = 27, age range 46–65 years) confirmed by coronary angiography and healthy subjects (n = 24, age range 45–59 years) identified from the general population. Circulating EPCs were quantified in the lymphocyte fraction of 100 μl peripheral venous blood by fluorescent activated cell sorting after labelling with antibodies to surface receptors AC133, CD34, and KDR. 100 000 total events per CD34+KDR+ sample and 200 000 total events per AC133+KDR+ sample were recorded. EPC adherence and differentiation in vitro was also examined by culture of isolated peripheral blood mononuclear cells on fibronectin coated plates in endothelial basal medium supplemented with EGM SingleQuots and 20% FCS. On day 4 the adherent cell fraction was stained with 1,1-dioctadecyl-3,3,3,3-tetramethylindocarbocyanine-labeled acetylated (DiL-ac-LDL) and FITC-labeled Ulex europaeus agglutinin I. Dual-stained cells were judged to be EPCs, and counted in six random high-power fields (hpf).
Results: There was wide variation (15–40-fold) in the number of cultured and circulating EPCs in both parents and offspring. There was a significant positive correlation between parents and offspring in cultured EPC number (all subjects: r = 0.642, p<0.001; cases: r = 0.751, p<0.001; controls: r = 0.492, p = 0.015 (graphs 1–3)) and circulating AC133+KDR+ cells (all subjects: p = 0.023). On adjusted regression analysis including other demographic variables, parent’s cultured EPC number was the only significant predictor of offspring cultured EPC number. (All subjects: p<0.001; cases: p = 0.005; controls: p = 0.046.)
Conclusions: Our results suggest that EPC number and activity are partly genetically regulated. Given the emerging role of EPCs in endothelial repair and their association with CAD, our findings have interesting implications for understanding the role of EPCs in atherosclerosis and in contributing to the genetic basis of CAD.
endothelial progenitor cells; hereditary; coronary artery disease
007 GENETIC DISSECTION OF A BLOOD PRESSURE QUANTITATIVE TRAIT LOCUS ON RAT CHROMOSOME 1 AND GENE EXPRESSION ANALYSIS IDENTIFIES SPON1 AS A NOVEL CANDIDATE HYPERTENSION GENE
A. Bingham1, J. Clemitson1, R. Dixon1, S. Haines1, B. Patel1, L. Hall1, M. Lo2, J. Sassard2, F. Charchar1, N. Samani1. 1University of Leicester, Leicester, UK; 2Faculte de Pharmacie, Lyon, France
Introduction and Aims: A region with a major effect on blood pressure (BP) is located on rat chromosome 1. We previously confirmed the BP effect of this region by constructing reciprocal congenic strains (WKY.SHR-Sa and SHR.WKY-Sa) derived from a cross of the spontaneously hypertensive rat (SHR) with the Wistar-Kyoto rat (WKY), showing that it contains two distinct BP quantitative trait loci (QTLs), BP1 and BP2. Using kidney cross-transplantation experiments the BP effect of these QTLs was shown to be mediated through the kidney. A congenic substrain containing only BP1 (Sisa1) and carrying a 4.3 Mb introgressed region, was constructed from SHR.WKY-Sa animals. In this study our aims were to carry out further genetic dissection of BP1 and to identify positional candidate genes through transcriptome analysis.
Methods: We fine mapped the BP1 region by systemic construction of two mutually exclusive congenic substrains, Sisa1a and Sisa1b, from the Sisa1 strain. To interrogate candidate genes, targeted transcript sequencing was carried out. In addition, genome-wide microarray expression profiling in whole kidney was undertaken to identify differentially expressed genes that lie within the BP1 region.
Results and Conclusion: Genetic dissection of BP1 showed that only the Sisa1a congenic substrain continued to demonstrate a BP difference but with a reduced introgressed segment of 3Mb. Exonic sequencing of the 17 renally-expressed and 3 novel genes located in the Sisa1a region did not identify any major differences between SHR and WKY. However, microarray expression profiling identified a single gene (Spon1) that mapped within the boundaries of our Sisa1a minimal congenic region, and that exhibited significant differential expression between the WKY and SHR genotypes, at both 6 and 24 weeks of age. Differential expression of Spon1 was confirmed by performing quantitative RT-PCR. Furthermore, western blot analysis also confirmed an increased level of the Spon1 gene product in the SHR. Spon1 belongs to a family of genes with anti-angiogenic properties and has not previously been identified as a hypertension candidate gene. Our findings justify further investigation of this novel positional candidate gene in BP control in hypertensive rat models and humans.
hypertension; genetics; gene expression
008 INTERLEUKIN 1 IS SIGNIFICANTLY ASSOCIATED WITH CAD IN A LARGE UK DISCORDANT SIBSHIP COLLECTION
B. Brown1, A. Balmforth2, J. Nsengimana3, J. Barret3, R. Lawrence1, A. Hall2. 1Leeds General Infirmary, Leeds, UK; 2Institute for Cardiovascular Research, Leeds, UK; 3Cancer Research, Leeds, UK
Background: Family history is a major risk factor for CAD. Although traditional risk factors show heritability a family history remains an independent predictor of disease driven by genetic variation. Inflammation is central to the development and complications of coronary atheroma and interleukin 1 (IL1) is one of the most potent mediators of inflammation. We sought to identify if genetic variation of IL1 might explain disease development.
Methods: We evaluated the UK’s largest collection of discordant sibships consisting of families in which at least one family member was affected by premature CAD (<66 years; MI/PCI/Angina/CABG). Three cohorts were studied: (1) all CAD phenotypes (2) individuals having MI and (3) disease onset <50 years. DNA was evaluated by means of a multilocus assay evaluating 35 candidate genes of inflammation. Data were checked and genotypes analysed with PEDIGREE and “family based association test” (FBAT) software respectively.
Results: 2871 individuals of 930 families were analysed. Mean age was 50 and 59 for affected and unaffected family members respectively (80% of unaffecteds had surpassed the age at which affected siblings had their event). Three polymorphisms of IL1 were studied; IL1α T549C IL1β C1423T C4336T. We observed a highly significant relation between all specified groups and the frequent (41.2–42.7%) IL1 hapotype CCC (all CAD p = 0.009305; MI only p = 0.001745; <50 years p<0.000037). The effect of this haplotype was then estimated using conditional regression but adapted to families by adding weights in the regression of the haplotypes to disease status. Considering age firstly shows that the CCC haplotpye has a disease causing effect across all ages but is more marked in those with younger onset disease (odds ratio 1.47 (CI 1.05–2.05) vs 2.26 (1.41–3.62) respectively). Adjusting for covariates (sex, smoking and hypertension) the CCC haplotype remains significantly associated with disease status (see table) and is again most evident in those with younger onset disease.
Conclusion: Our family-based design avoids error due to population stratification. Considering IL1 haplotypes in our study we have observed a highly significant effect and contrary to other major discoveries (FLAP and LTA4) this is in both CAD and MI populations. Ideally this study needs replicating in further populations and we await with interest the outcome of IL1 intervention studies as a measure of biological plausability.
genetics; interleukin 1; coronary artery disease
009 THE STENT OR SURGERY LONG-TERM FOLLOW-UP
R. Stables1, J. Booth2, J. Pepper2, T. Clayton3, M. Flather2, F. Nugara2, U. Sigwart4. 1Liverpool Cardiothoracic Centre, Liverpool, UK; 2Royal Brompton & Harefield NHS Trust, London, UK; 3London School of Hygiene & Tropical Medicine, London, UK; 4University Hospital, Geneva, Switzerland
Introduction: The Stent or Surgery Trial was a randomised controlled trial comparing percutaneous coronary intervention with coronary artery bypass grafting for patients with multi-vessel disease. Initial results at an average follow up of 2 years showed a survival advantage for patients randomised to CABG. This paper reports survival outcome at a mean follow up of 5.8 years.
Methods: A total of 988 (n = 488 PCI, n = 500 CABG) patients were initially randomised from 53 centres in 11 European countries and Canada. Investigators were asked to evaluate survival status from hospital or community medical records, national databases or by direct contact with patients. Investigators reported cause of death where known. For individual patients, the date of death or the last date of contact at which the patient was known to be alive was used in the statistical analysis. A comparison was made of all cause mortality and the hazard ratios and CI calculated from Cox proportional hazards model. All-cause mortality was also analysed after adjustment for age, angina grade, diabetes mellitus, left ventricular ejection fraction and angiographic severity of coronary disease at baseline. A subgroup analysis of diabetes mellitus, angina grade and angiographic severity of coronary disease at baseline was performed using tests for interaction.
Results: The mean follow-up for mortality was 5.8 years with a maximum of 8 years. At 5 years the mortality status of 9 patients in the PCI group and 15 patients in the CABG group were unknown. At a mean follow-up of 5.8 years 53 (10.9%) patients died in the PCI group compared to 34 (6.8%) patients in the CABG group, hazard ratio 1.66 (95% CI 1.08 to 2.55, p = 0.022). An analysis adjusted for specified baseline variables yield similar results. There was no significant difference in the subgroup analysis for diabetes mellitus (p = 0.15), angina grade (p = 0.52) and severity of coronary disease (p = 0.92).
Conclusion: Mortality rate for both groups has increased over time; however at a mean follow-up of 5.8 years we found that patients managed with CABG have an apparent survival advantage.
CABG; stent; coronary artery disease
010 EFFECT OF INCOMPLETE REVASCULARISATION ON OUTCOME FOLLOWING PERCUTANEOUS CORONARY INTERVENTION FOR MULTI-VESSEL DISEASE: SCOTTISH CORONARY REVASCULARISATION REGISTER
J. Pell1, K. Oldroyd2, R. Slack3, A. Pell4, H. Eteiba5, A. Flapan6, S. Hillis2, J. Irving7, K. Jennings8, R. Northcote9, I. Starkey6. 1BHF Glasgow Cardiovascular Research Centre, University of Glasgow, Glasgow, UK; 2Western Infirmary, Glasgow, UK; 3Greater Glasgow NHS Board, Glasgow, UK; 4Monklands Hospital, Airdrie, UK; 5Glasgow Royal Infirmary, Glasgow, UK; 6Royal Infirmary, Edinburgh, UK; 7Ninewells Hospital, Dundee, UK; 8Aberdeen Royal Infirmary, Aberdeen, UK; 9Victoria Infirmary, Glasgow, UK
Introduction: Revascularisation can be achieved through either percutaneous coronary intervention (PCI) or coronary artery bypass grafting (CABG). Patients with multi-vessel disease (MVD) are increasingly treated by PCI. Compared with CABG, PCI carries a higher risk of incomplete revascularisation.
Methods: The Scottish Coronary Revascularisation Register collects data on all patients undergoing PCI in Scotland. Comprehensive information is collected prospectively on clinical presentation, comorbidity and procedural details. Linkage to routine hospital and death certificate data provides long-term follow-up. We undertook a retrospective cohort study of PCIs undertaken in 2003/4 on whom we had up to 2 years’ follow-up. We excluded patients with single vessel disease or a history of previous revascularisation and PCIs undertaken as the first part of a staged procedure.
Results: Of the 1198 PCIs eligible for inclusion, 902 (75%) resulted in complete revascularisation (post procedure Duke jeopardy score 0–2) and 289 (24%) produced incomplete revascularisation (Duke score >2). On binary logistic regression analysis, both the pre PCI Duke score (p<0.001) and the presence of a chronic total occlusion (CTO) (OR 2.19, 95% CI 1.36 to 3.53, p = 0.001) predicted incomplete revascularisation after adjustment for potential confounders. We used Cox proportional hazards models to determine whether incomplete revascularisation was associated with outcome post PCI. There were no statistically significant interactions with either CTO or pre PCI Duke score. On univariate analysis, incomplete revascularisation was associated with an increased risk of all-cause death, myocardial infarction (MI), CABG and repeat PCI (table). In the multivariate model, we adjusted for age, sex, urgency, diabetes, cerebrovascular disease, renal impairment, hypertension, hyperlipidaemia, obesity, smoking status and past history of MI. Incomplete revascularisation remained a significant independent predictor of death, CABG and repeat PCI (table).
Conclusions: In determining whether a patient with MVD is suitable for PCI, consideration needs to be given to the likelihood of achieving complete revascularisation as this, in turn, will significantly impact on prognosis and the need for further intervention.
percutaneous coronary intervention; incomplete revascularisation; outcomes
011 REMOTE ISCHAEMIC PRECONDITIONING PROTECTS THE HEART AT TIME OF CABG SURGERY
P. Mwamure1, D. Hausenloy1, J. Harris1, M. Barnard2, E. Grundy2, E. Ashley2, C. Di Salvo2, S. Vichare2, S. Kolvekar2, M. Hayward2, B. Keogh2, R. MacAllister3, D. Yellon1. 1The Hatter Cardiovascular Institute, UCL, London, UK; 2The UCLH Heart Hospital, London, UK; 3Centre for Clinical Pharmacology and Therapeutics, UCL, London, UK
Introduction: Remote ischaemic preconditioning (RIPC) describes the phenomenon in which brief ischaemia of one tissue or organ protects remote organs from a sustained episode of ischaemia. Myocardial injury in patients undergoing coronary artery bypass surgery (CABG), as measured by the release of cardiac enzymes, is associated with postoperative morbidity and mortality. We conducted a single-blinded randomised controlled trial to determine whether RIPC, using transient upper limb ischaemia, protects patients undergoing elective CABG against this myocardial injury.
Methods: Thirty consenting patients undergoing elective CABG were randomised to receive either RIPC (n = 15) or control (n = 15) following induction of anaesthesia. RIPC comprised three 5-min cycles of right upper limb ischaemia, induced by an automated cuff-inflator placed on the right upper arm and inflated to 200 mmHg, with an intervening 5 min of reperfusion during which time the cuff was deflated. Control patients had a deflated cuff placed on their right upper arm for 30 min. Serum troponin-T was measured preoperatively and at 6, 12, 24, 48 and 72 h post-surgery.
Results: There were no significant differences in the patient characteristics or the details of cardiac surgery between the two treatment groups. RIPC significantly reduced serum troponin-T release in patients undergoing elective CABG, at 6 h (0.31 (0.24) µg/l with RIPC vs 0.61 (0.52) µg/l with control: p<0.05), 12 h (0.33 (0.16) µg/l with RIPC vs 0.82 (0.54) µg/l with control: p = 0.002), 24 h (0.32 (0.12) µg/l with RIPC vs 0.62 (0.37) µg/l with control: p = 0.006) and 48 h (0.31 (0.18) µg/l with RIPC vs 0.54 (0.34) µg/l with control: p = 0.036) following surgery. The total area under the curve (over 72 h) was reduced by 49% with RIPC compared to control (19.87 (7.82) µg/l in RIPC vs 39.25 (20.97) µg/l in control: 95% CI 7.55 to 31.22 µg/l: p = 0.002).
Conclusions: Remote ischaemic preconditioning induced by transient upper limb ischaemia, reduces myocardial injury in patients undergoing elective CABG surgery, as evidenced by a 49% reduction in troponin-T release over the perioperative 72-h period, a finding which may be associated with an improvement in clinical outcomes in this patient group. These findings provide an easily applied non-invasive and non-pharmacological novel strategy for protecting the myocardium against ischaemia-reperfusion injury, which could be investigated in patients undergoing myocardial reperfusion using either thrombolysis or primary coronary angioplasty for an acute myocardial infarction.
coronary artery bypass graft surgery; remote preconditioning; troponin
012 STRESS ECHOCARDIOGRAPHY CAN SAFELY, RAPIDLY AND ACCURATELY RISK STRATIFY PATIENTS WITH SUSPECTED ACUTE CORONARY SYNDROME AND AN INITIAL (12 H) NEGATIVE TROPONIN: IMPLICATIONS FOR EARLY USE OF STRESS ECHOCARDIOGRAPHY IN THE EMERGENCY DEPARTMENT
P. Jeetley, L. Burden, R. Senior. Northwick Park Hospital, Harrow, UK
Background: Patients presenting to hospital with suspected acute coronary syndrome (ACS) and an initial negative troponin (Tn) require further investigation. We hypothesised that stress echocardiography (SE) was both safe and accurate for the risk stratification of patients with suspected ACS but a negative 12-h troponin.
Methods: Patients with cardiac risk factors presenting with suspected ACS and a negative Tn measured 12 h from onset of pain underwent SE. A further Tn measure was taken after admission before SE. A positive SE was defined as presence of a new or inducible wall motion abnormality in any one of the 16 left ventricular segments. Patients were followed up for hard cardiac events (cardiac death and acute myocardial infarction (AMI)).
Results: Of the 190 patients who underwent SE, 16 (8.4%) suffered cardiac events (1 cardiac death and 15 AMI) over a follow-up period of 18 (9) months. Of the 40 patients with positive SE, cardiac events occurred in 10 (25%) as opposed to only 6 cardiac events out of 150 patients (4%) with a negative SE (p<0.001). Kaplan-Meier survival curves (fig) illustrate outcomes for positive versus negative SE. The majority of cardiac events (11/16) occurred early after admission. A positive SE predicted 8 (20%) out of 40 patients while only 3 (2%) out of 150 patients with negative SE suffered cardiac events.
Conclusions: SE is a safe effective and rapid method of risk stratifying patients with suspected ACS and an initially negative Tn. A negative SE is associated with excellent long-term prognosis.
stress echocardiography; prognosis; risk prediction
013 ISCHAEMIC AND THROMBOTIC EFFECTS OF DILUTE DIESEL EXHAUST INHALATION IN PATIENTS WITH CORONARY HEART DISEASE: MECHANISMS FOR THE ADVERSE CARDIOVASCULAR EFFECTS OF AIR POLLUTION
N. Mills1, H. Törnqvist2, M. Gonzalez2, E. Vink1, S. Robinson3, S. Söderberg2, K. Donaldson4, T. Sandström2, A. Blomberg2, N. Boon1, D. Newby1. 1Edinburgh Royal Infirmary, Edinburgh, UK; 2Umeå University, Umeå, Sweden; 3James Cook University Hospital, Middlesbrough, UK; 4The University of Edinburgh, Edinburgh, UK
Background: Exposure to traffic-derived air pollution is associated with adverse cardiovascular events. The mechanisms for this association are unknown. We conducted a controlled exposure to dilute diesel exhaust in patients with stable coronary heart disease to determine the direct effect of air pollution on myocardial, vascular and fibrinolytic function.
Methods: In a double blind randomised crossover study, 20 patients with prior myocardial infarction were exposed to dilute diesel exhaust (300 µg/m3) or filtered air during periods of rest and moderate exercise in a controlled exposure facility. During the exposure, myocardial ischaemia was quantified by ST-segment analysis using continuous 12-lead electrocardiography. Six hours following exposure, vascular vasomotor and fibrinolytic function were assessed by means of intra-arterial agonist infusions.
Results: During both exposures, heart rate increased with exercise (p<0.001 for both) to a similar extent (p = NS; diesel exhaust versus filtered air). Exercise induced ST-segment depression was present in all patients but there was a greater increase in ischaemic burden during exposure to diesel exhaust (−22 (4) vs −8 (6) mVs, p<0.001; fig). Exposure to diesel exhaust did not aggravate pre-existing vasomotor dysfunction, but did reduce acute endothelial tissue plasminogen activator release (p<0.05; area under the curve decreased by 35%).
Conclusions: Brief exposure to dilute diesel exhaust promotes myocardial ischaemia and inhibits endogenous fibrinolytic capacity in patients with stable coronary heart disease. Our findings have identified ischaemic and thrombotic mechanisms for the observations that exposure to combustion-derived air pollution is associated with adverse cardiovascular events including acute myocardial infarction.
myocardial ischaemia; fibrinolysis; air pollution
014 ARE THERE ETHNIC DIFFERENCES IN THE DIAGNOSTIC AND PROGNOSTIC VALUE OF ANGINA SYMPTOM DESCRIPTORS? A 3-YEAR PROSPECTIVE STUDY OF 2189 SOUTH ASIANS
M. Zaman1, C. Junghans1, N. Sekhri2, G. Feder3, A. Timmis3, H. Hemingway1. 1University College London, London, UK; 2Newham University Hospital, London, UK; 3Queen Mary’s School of Medicine and Dentistry, London, UK
Introduction: Classic symptom descriptors of stable angina pectoris were derived largely in white men, and their diagnostic and prognostic validity in South Asian women and men is unknown. South Asians may be misdiagnosed, and therefore inequitably treated, if their description of symptoms is not classic.
Objective: To determine in South Asians compared with whites the value of chest pain descriptors in making a diagnosis of angina and in determining prognosis.
Methods: Prospective, multicentre cohort study of consecutive, test-naive patients attending six rapid access chest pain clinics in the UK (980 South Asian women, 1209 South Asian men, 2676 white women, 2929 white men). Patients with three or more descriptors (location, duration, quality and provocation) being typical were defined as having typical angina. The composite endpoint was death due to coronary disease or admission with acute coronary syndrome, over mean follow-up of 3.0 years (164 events in South Asians, 374 in whites).
Results: For each of the four chest pain descriptors, South Asian women and men were more likely to report atypical responses, compared to whites (p<0.001 for all comparisons). However typical angina symptoms in South Asian women and men were as strong a predictor of angina diagnosis as they were in white women and men. Furthermore, in Cox regression models adjusting for age, sex, diabetes, smoking and hypertension there were no differences between ethnic groups in the probability of sustaining the composite event in both those with typical (HR 1.04 (95% CI 0.80 to 1.34)) and atypical/non-cardiac pain (HR 1.23 (95% CI 0.88 to 1.71)). The Kaplan–Meier curves indicate that there is no ethnic difference in the prognostic validity of symptom classification (fig).
Conclusion: South Asians attending chest pain clinic had an excess of atypical chest pain descriptors, and this may reflect a low threshold for referral. However, there were no ethnic differences in the diagnostic or prognostic validity of anginal symptom classification. These findings suggest that clinicians can trust their history taking, and do not support the hypothesis that ethnic differences in symptom descriptors lead to inequalities in health care.
stable angina pectoris; ethnic differences; prognosis
015 IMPLICATIONS OF GUIDELINES FOR STATIN TREATMENT FOR SECONDARY PREVENTION OF CARDIOVASCULAR DISEASE: RISK FACTOR ANALYSIS OF THE SCOTTISH HEALTH SURVEY 2003
I. Haq1, J. Hill2, J. Craig3, L. Ritchie4. 1Royal Victoria Infirmary, Newcastle upon Tyne, UK; 2Quality Improvement Scotland, Edinburgh, UK; 3Quality Improvement Scotland, Glasgow, UK; 4Unversity of Aberdeen, Aberdeen, UK
Objective: To determine the proportion of the population aged 40 years or over with clinical apparent cardiovascular disease (CVD) who might benefit from statin therapy for secondary prevention.
Methodology: Risk factor information was extracted on adults from data from the Scottish Health Survey 2003. The survey used a multi-stage stratified probability sampling design, with postcode sectors. Over 8000 interviews were conducted with individuals over 18 and over and over 4250 gave blood samples to be analysed for factors which included total and HDL-cholesterol. Individuals were classified as having CVD if they reported having any of the following conditions confirmed by a doctor: myocardial infarction (MI), angina, stroke. Peripheral vascular disease (PVD) was diagnosed by a symptom questionnaire for claudication. Only those with “definite claudication” were included. Those with a history of MI were identified; then those with angina but no MI; then those with stroke but no MI or angina; and finally those with PVD but no MI, angina or stroke.
Results: The total number sampled with any cholesterol reading was 2966. The table shows the estimates of prevalence of disease in that group for 5-year age bands. Treating all individuals with CVD will result in 14.0% of the population being offered a statin. This comprises 16.4% of men and 12.0% of women. Reserving treatment to those with total cholesterol ⩾4 mmol/l reduces the percentage marginally from 14.0% to 13.8%, and to 12.3% for those with total cholesterol ⩾5 mmol/l.
Conclusions: Approximately 14% of the Scottish population aged 40 years or over are potential candidates for treatment with statins for secondary prevention of cardiovascular disease. Even discounting those for treatment for primary prevention, this is a major undertaking with large resource implications.
secondary prevention; statin; epidemiology
016 AGING DIMINISHES THE PUMPING CAPACITY OF HEALTHY HUMAN MALE BUT NOT FEMALE HEARTS
N. T. Lewis1, D. F. Goldspink2, R. E. Clements2, L. Sharp2, P. D. Chantler2, A. Patwala3, K. George2, C. Stephenson2, L. B. Tan1. 1Leeds General Infirmary, Leeds, UK; 2Research Institute For Sports & Exercise Sciences, Liverpool John Moores University, Liverpool, UK; 3The Cardiothoracic Centre In Liverpool, Liverpool, UK
Introduction: Previous autopsy observations indicated that with aging the male myocardium loses about 35% of its myocytes over the adult lifespan, whereas the female heart retains both its myocyte number and LV mass. We tested the hypothesis that this striking gender difference in morphology has cardiovascular functional correlates.
Methods: LV mass via echocardiography and central hemodynamics were studied during maximal treadmill cardiopulmonary exercise testing by non-invasively measuring cardiac output (Q) and mean arterial pressure (MAP) in healthy men (n = 101) and women (n = 140) between the ages of 19 and 76 years. Overall cardiac function, represented by cardiac power output (CPO = Q × MAP), was determined at rest and at maximal exercise.
Results: Over the 50+ years of adult lifespan studied, LV mass was found to be preserved in women, but reduced by over 4% per decade of aging in men (p<0.001). Cardiac power was also preserved in aging women, but diminished both at rest and during volitional maximal exercise by around 5% per decade in men (p<10–6). The cardiac flow-generating capacity was also preserved in aging women, but not in men. In contrast, both sexes showed higher pressure-generating capacities with aging, but this was greater in women despite similar age-related changes in systemic vascular resistances during exercise.
Conclusions: These experimental data support the hypothesis that in aging women preservation of LV mass correlates with preserved cardiac pump function, contrasting with the loss of cardiac mass and function in aging men. Hence, gender differences in cardiac aging extend beyond mere morphological features, and impact on cardiovascular function.
sex; cardiac function; ageing
017 DIFFERENCES BETWEEN THE EUROPEAN AND AMERICAN SOCIETY GUIDELINES INFLUENCE THE NUMBER AND DURATION OF CHEST PAIN ADMISSIONS
R. Good, M. Pollock, A. Carrick, A. Murphy, K. Oldroyd, S. Robb. Western Infirmary, Glasgow, UK
Background: Admission rates, in developed countries, of patients with suspected acute coronary syndrome continue to increase. Consequently, efficient screening, risk stratification and management of chest pain patients is critical. In this regard the AHA/ACC and ESC guidelines differ in a number of areas. In particular, the ESC guidelines suggest that, for patients attending hospital with suspected ischaemic cardiac chest pain, myocardial enzymes, in the form of troponin, should be checked >12 h following resolution of chest pain symptoms or >12 h following attendance. In contrast, the AHA/ACC guidelines suggest that troponin assessment >12 h following the onset of suspected cardiac chest pain is sufficient to risk stratify these patients. We sought to investigate how adherence to the ACC/AHA criteria might impact upon chest pain admissions.
Methods: We prospectively audited all patients admitted to the acute medical receiving unit (AMRU) in our hospital over a 10-week period with suspected cardiac chest pain. Time of onset of chest pain symptoms, time of A&E arrival, length of stay in AMRU, time to troponin assessment, final diagnosis and outcome from AMRU were recorded. High-risk patients admitted directly to the coronary care unit were excluded.
Results: 220 patients were admitted to the AMRU with suspected cardiac chest pain in this period. Patients attended throughout the 24-h period (fig). 56/220 patients (25%) had chest pain symptoms for more than 12 h (table). Of these patients 40/56 were subsequently discharged directly from the AMRU following troponin assessment. Mean time to troponin estimation in these patients was 9.9 h (range 0.5–22.5 h). There was no significant difference in the length of hospital stay between patients with chest pain symptoms >12 h (mean 23.3, SD 7.4 h) and those <12 h (mean 25.3, SD 9.8 h) (p = 0.25).
Conclusion: The onset of chest pain symptoms plays a critical role in determining the treatment of patients presenting with ST-elevation myocardial infarction. However, in patients with suspected acute coronary syndrome, the onset of their symptoms has much less impact. The majority of chest pain patients present between 08:00 and 20:00 h. We found that 40/220 (18%) of patients admitted with suspected ischaemic chest pain and discharged directly from AMRU had symptoms for >12 h prior to attending hospital. Adopting the ACC/AHA criteria for the timing of myocardial enzyme estimation together with rapid and efficient assessment of these patients could significantly reduce hospital admissions.
chest pain; acute coronary syndrome; troponin
018 MANUAL ASSESSMENT OF QRS DURATION: IMPORTANCE OF ECG FORMAT AND CLINICAL IMPLICATIONS IN LIGHT OF NICE ICD IMPLANTATION GUIDELINES
D. Tomlinson, J. Timperley, J. Ehtisham, N. Sabharwal, S. Myerson, A. Ryding, C. Shirodaria, Y. Bashir, T. Betts. Department of Cardiology, John Radcliffe Hospital, Oxford, UK
Background: In patients with ischaemic cardiomyopathy a prolonged QRS duration (QRSd) on the surface ECG is a marker of sudden death risk. Current UK NICE primary prevention guidelines recommend ICDs for patients with left ventricular ejection fraction <30% and QRSd ⩾120 ms. When the QRSd is close to 120 ms the decision to undertake further investigations or recommend ICD implantation is critically dependent on the ECG interpretation. However, clinical trials differ in their methods of assessment of QRSd in this setting and current UK NICE guidelines do not specify a preferred measurement technique.
Methods: The effect of ECG format and paper speed on manual QRSd measurement was investigated using ECGs recorded on Fukuda Denshi FX-4101U/FX-4010 machines. Standard 12-lead, 6-limb and 6-precordial lead tracings were recorded at both 25 and 50 mm/s; extended analysis calculated QRSd for all individual leads as well as the mean QRSd. Five cardiology specialist registrars and 1 consultant undertook blinded manual QRSd analysis. Intraobserver variability was determined from 4 identical sets of ECGs of each format. The agreement between measurement techniques at dichotomising ECG QRSd as <120 ms or ⩾120 ms was studied.
Results: The range of calculated mean QRSd among study ECGs was 98–121 ms. Intraobserver variability was greatest at 25 mm/s to 40 ms, compared to 20 ms at 50 mm/s (fig). The interobserver variability was no different between ECG formats. The accuracy of manual dichotomisation of ECGs varied according to the reference used for calculated QRSd; significantly fewer ECGs were identified as having QRSd ⩾120 ms manually when the maximum QRSd in any lead was taken as the reference.
Conclusions: Manual assessment of QRSd is subject to significant intraobserver variability that may be improved by changing the paper speed to 50 mm/s. However, this may result in greater inaccuracy when undertaking manual QRSd measurement, particularly if the lead with the greatest QRSd is used as a reference. In patients with QRSd at the upper limit of normal, calculated measurements may be a useful tool to guide patient selection for ICD implantation. Furthermore, UK NICE guidelines should include specific recommendations on QRSd measurement in this clinical setting.
implantable cardioverter defibrillator; electrocardiogram; QRS duration
019 EUROACTION: A EUROPEAN SOCIETY OF CARDIOLOGY DEMONSTRATION PROJECT IN PREVENTIVE CARDIOLOGY: ONE-YEAR RESULTS FOR CORONARY PATIENTS AND THEIR PARTNERS
S. Connolly1, K. Kotseva1, C. Jennings1, A. Mead1, J. Jones1, A. Holden1, G. De Backer2, D. DeBacquer2, T. Collier3, D. Wood1. 1Imperial College, London, UK; 2University of Ghent, Ghent, Belgium; 3London School of Hygiene and Tropical Medicine, London, UK
Objectives: EUROACTION is a cluster randomised controlled trial of a nurse-led multidisciplinary preventive cardiology programme which aims to manage coronary patients and their families to the European lifestyle, risk factor and therapeutic targets for cardiovascular disease prevention.
Methods: In each of 6 European countries, a pair of comparable general hospitals was randomised to receive the EUROACTION intervention programme or to be monitored for usual care. Consecutive coronary patients were proactively identified by the study nurse and invited with their partners to attend the 16-week EUROACTION programme with a repeat assessment at one year.
Results: In intervention (INT) hospitals, 1589 eligible coronary patients were identified and 946 (60% of all eligible) patients attended at 1 year. 703 partners in INT were identified, of whom 401 (57%) attended at one year. In usual care (UC), 1499 eligible coronary patients were identified and 994 (66% of all eligible) patients attended at one year. 745 partners were identified in usual care, of whom 335 (45%) attended the one year assessment. Tables 1 and 2 show the proportions of patients and their partners achieving the European lifestyle (table 1), risk factor and therapeutic targets (table 2).
Abstract 002
Abstract 008
Conclusions: The EUROACTION programme helped coronary patients and their families to achieve a reduction in central obesity, to make healthier food choices and also to increase their physical activity levels in comparison with usual care. In addition, there was an improvement in blood pressure control and lipid control although significant for blood pressure only. There was a substantial improvement in the use of cardioprotective medication particularly antiplatelet therapy, beta-blockers and statins. Therefore EUROACTION achieved its overall aim in raising standards of preventive cardiology care for coronary patients and their partners in everyday clinical practice.
cardiovascular disease; risk factors; prevention
020 ATRIAL FIBRILLATION IN A PRIMARY CARE POPULATION: HOW CLOSE TO NICE GUIDELINES ARE WE?
B. Loo1, C. Parnell1, G. Brook2, E. Southall3, I. Mahy1. 1Torbay General Hospital, Torquay, UK; 2Barton Sugery, Dawlish, UK; 3Mayfield Surgery, Torquay, UK
Introduction: In anticipation of the publication of the new NICE clinical guideline for atrial fibrillation we sought to document existing management of patients with atrial fibrillation (AF) in the primary care population, to determine whether additional resources or education would be required to meet the standards set.
Methods: All practices in the South Devon area were invited to take part in a systematic audit of a random population sample during 2006. 27 of 35 practices agreed to take part, serving a population of 189 261 patients. Of these 3347 were identified as having AF through practice registers. Four patients were selected at random from each practice register for detailed study, providing a study population of 107 (55 males, mean age 69 (15) years). The audit addressed documentation, investigation, comorbidity, thromboemblism prophylaxis, and whether patients had been referred to secondary care.
Results: 59% of the population had primary care documentation of an ECG confirming the diagnosis of AF, in 39 patients (36%) the diagnosis was of paroxysmal AF and in 63 patients (59%) permanent AF. 51% had been referred to secondary care. 17% of the population had undergone at least one DC cardioversion. 44% had undergone echocardiography (23% of those managed only in primary care). Of patients diagnosed since 2000, 65% had echocardiography compared with 18% of patients diagnosed before 2000. 83% of the total population were taking either aspirin or warfarin as thromboembolism prophylaxis. According to NICE classification of thromboembolic risk 46% were high risk, 42% intermediate risk and 12% low risk. 49% of high risk patients were taking warfarin or had an explicit contraindication, 56% of intermediate risk, 23% of low risk.
Conclusion: Almost half of patients with diagnosed atrial fibrillation are currently managed exclusively in primary care. A minority of patients had undergone echocardiography but this reflects low investigation rates in patients with a longstanding diagnosis. The need for thromboembolism prophylaxis was recognised but warfarin usage did not closely reflect the thromboembolic risk of patients.
primary care; atrial fibrillation; NICE
021 ETHNIC DIFFERENCES IN RATES OF MYOCARDIAL INFARCTION IN PATIENTS WITH HYPERTENSION ARE EXPLAINED BY AN EXCESS OF DIABETES
H. Lim1, J. Patel1, G. Lip1, I. Tracey2, A. Gunarathne2, E. Hughes2. 1City Hospital, Birmingham, UK; 2Sandwell Medical Research Unit, West Bromwich, UK
Background: South Asians living in the UK have a higher prevalence of, and mortality from coronary heart disease (CHD) than the general British population. The causes of this excess CHD risk are unclear. Data from longitudinal studies are lacking to provide an evidence-based approach for ethnicity-specific CHD management in Britain. Diabetes is common among South Asian populations, and we hypothesised that this susceptibility would explain the higher rates of myocardial infarction (MI) in South Asian hypertension patients compared to white contemporaries.
Abstract 010 Cox proportional hazards model of risks associated with incomplete revascularisation
Abstract 015 Prevalence of CVD in people aged 40 years or over who had a total cholesterol concentration in the Scottish Health Survey
Abstract 017
Abstract 019 Table 1
Abstract 019 Table 2
Abstract 021
Methods: We investigated the relation between CHD risk factors measured among patients with hypertension (attending Sandwell and West Birmingham Hospitals, inner city UK, between January 1998–September 2000) and cardiovascular events over 5-year follow-up. Biochemical tests were performed with routine automated assays. Diabetes was diagnosed by history and fasting plasma glucose measurement at baseline. Blood pressure was standardised to British Hypertension Society guidelines with an automated sphynomanometer (Omron HEM 705-CP, Netherlands).
Results: A total of 350 white (83.7% male) and 104 South Asian (66.3% male) patients with hypertension were followed up for a mean (SD) follow-up period of 64.7 (12.1) months. On comparison of risk factors at initial assessment (table), white patients with hypertension were older (p<0.001), had higher systolic blood pressure (p<0.001), were more likely to be on two or more blood pressure therapies (p<0.001) and more hyperlipidaemic (p<0.001), but were less likely to have diabetes (p<0.001).There were no ethnic differences in HDL cholesterol concentrations, the use of statin therapy or anti-platelet therapies among patients (table). Despite higher blood pressure and cholesterol in the white group, there were fewer cases of MI in white (11 (6.4/1000 patient years)) compared to in South Asian patients (11 (17.8/1000 patient years)). Event-free survival time was lower in the South Asian group (log rank test p = 0.04). On Cox regression analysis of all independent cardiovascular risk variables, associated treatments and ethnicity, MI was associated with diabetes (odds ratio, 95% CI 3.77, 1.55–9.15, p = 0.003) and anti-platelet therapy at baseline (3.9, 1.5–10.3, p = 0.07).
Conclusion: In this study, South Asian patients with hypertension had a higher incidence of myocardial infarction compared to their white counterpart (despite lower blood pressure and cholesterol) due to a higher prevalence of diabetes. These differences in cardiovascular risk profile calls for an ethnicity-specific risk assessment and treatment targets. Our data support routine screening for diabetes among South Asian patients with hypertension.
diabetes; ethnicity; myocardial infarction
022 SINGLE CENTRE UK EXPERIENCE OF CRYOABLATION BALLOON FOR PAROXYSMAL ATRIAL FIBRILLATION
A. Sandilands, K. Woodburn, P. Boreham, T. Cripps. Bristol Royal Infirmary, Bristol, UK
Background: Radiofrequency ablation (RFA) for paroxysmal atrial fibrillation (AF) has developed into an effective and safe procedure. However, the efficacy of balloon cryoablation (Arctic Front, CryoCath) has not yet been established.
Methods and Results: We report the first 20 consecutive patients (16 male, mean age 54 years) undergoing balloon cryoablation between December 2005 and November 2006. Each patient had documented symptomatic paroxysmal atrial fibrillation (AF) with failure of at least 1 anti-arrythmic (mean 2, range 1–4) and 2 patients had AF suppression pacemakers. Following transeptal puncture, pulmonary vein (PV) anatomy was identified using contrast injection and PV potentials (PVPs) were mapped with a circular catheter. Balloon cryoablation was performed (12 patients 28 mm, 7 patients 23 mm with 1 patient both 23 and 28 mm balloons) in each active PV ostia for up to 5 min, mean procedure time 154 min, mean screening time 47.2 min. Post ablation mapping demonstrated 86/90 PVs were electrically isolated (1 already silent, persistent PVPs in the remaining 3). Four patients also underwent typical right atrial flutter ablation (2 as repeat procedure). A single patient had RFA to a single PV. Complications included 3 mechanical balloon failures necessitating new balloons, 4 phrenic nerve palsies (2 minor which reversed, 2 partially reversed but patients asymptomatic), 1 tamponade requiring drainage and a single patient with lobar collapse following general anaesthetic. With a mean follow-up of 7 months, 9 (45%) patients were AF-free on no medication, 3 (15%) patients had minor symptoms on no medication and 4 (20%) had minor symptoms on medication. Four (20%) patients had minor or no improvement in symptomology and are awaiting re-do. Patients were generally satisfied with the outcome using a postal questionnaire with mean scoring 4/5 (range 0–5).
Conclusion: It would therefore appear that balloon cryoablation for PAF is a safe and promising alternative to RF ablation.
atrial fibrillation; cryoablation; pulmonary vein potentials.
023 THROMBOEMBOLISM RISK REDUCTION IN PATIENTS UNDERGOING CATHETER ABLATION PROCEDURES FOR PERSISTENT AND PAROXYSMAL ATRIAL FIBRILLATION: A COMPARISON OF UK AND INTERNATIONAL PROTOCOLS
D. Tomlinson, T. Betts, Y. Bashir. Department of Cardiology, John Radcliffe Hospital, Oxford, UK
Abstract 023
Background: Left atrial catheter ablation is now an established technique for the treatment of symptomatic patients with atrial fibrillation (AF). Thromboembolism may complicate approximately 1% of such procedures, however there is no consensus regarding optimal preoperative investigations and anti-thrombotic regimes to minimise this risk. Moreover, concerns regarding the risk of postoperative cardiac tamponade may lead to significant differences in anticoagulation practices. To further investigate this issue, an audit of protocols currently employed in UK was undertaken. These data were then compared with those international centres undertaking AF ablation.
Method: Email-based questionnaire of UK Consultant Cardiac Electrophysiologists and comparison with international protocols obtained from publications, or by direct telephone enquiry.
Results: Anticoagulation protocols were obtained from 30 UK consultants, representing 21 institutions. International protocols were obtained from the following centres: Cleveland Clinic (Natale et al), University Hospital of Bordeaux (Haissaguerre et al), University of Michigan (Oral, Morady et al), San Raffaele University Hospital, Milan, (Pappone et al), Klinik St Georg, Hamburg (Kuch et al), University of Oklahoma (Jackmann et al) and Pacific Rim EP Center (Nademanee et al). Comparison with UK practice was made in three key areas: pre and post-ablation anticoagulation, transoesophageal echocardiography (TOE) and peri-procedural activated clotting time (ACT) (table).
Conclusions: There are significant differences in anti-thrombotic regimes between UK centres undertaking catheter ablation of paroxysmal and persistent AF. Furthermore, UK protocols for persistent AF employ a more intensive anti-thrombotic regime and a greater use of pre-ablation TOE than those for paroxysmal AF. In comparison with international centres, UK protocols have a lower rate of heparin administration pre and post-ablation and a lower rate of pre-procedural TOE. The effects of these differences is unknown, but an important function of the planned Electrophysiology Central Cardiac Audit Database should be the monitoring of both bleeding and thromboembolic complications following AF ablation procedures.
atrial fibrillation ablation; anticoagulation; protocols
024 A STUDY TO IDENTIFY THE PREVALENCE AND TIMING OF PERICARDIAL EFFUSIONS AFTER LEFT ATRIAL CATHETER ABLATION FOR ATRIAL FIBRILLATION AND ATRIAL TACHYCARDIA
M. Kalla, K. Rajappan, S. Kalra, S. Sporton, R. Schilling. Department of Cardiology, St Bartholomew’s Hospital and Queen Mary University, London, UK
Introduction: A potential complication of left atrial (LA) catheter ablation procedures is tamponade. This risk is normally quoted as 1–2% in patients undergoing LA ablation. However little is known about the incidence and timing of reactive pericardial effusions developing in the absence of tamponade and whether echocardiography should be routinely performed in these patients post procedure.
Methods: Forty consecutive patients (33 male, age 57 (10) years) undergoing LA catheter ablation for persistent atrial fibrillation (AF) (23 patients), paroxysmal AF (14 patients) or atrial tachycardia (AT) (3 patients) underwent on-table transthoracic echocardiography (TTE) at the end of the procedure, and pre-discharge TTE (12–24 h post-procedure). Catheter ablation was guided by electroanatomic mapping and CT image integration. A double trans-septal puncture technique was used in all cases, followed by radiofrequency ablation to isolate pulmonary vein pairs. Further LA and coronary sinus ablation was carried out in some AF cases. ATs were mapped and ablated as appropriate.
Results: Thirty eight patients (95%) underwent on-table TTE and this identified pericardial effusions in 19 patients (50%, range 0.4–0.75 cm). None had either echocardiographic or clinical signs of tamponade. Discharge TTE was carried out on 39 patients (98%) and identified effusions in 67% of patients (26/39). There were still no echocardiographic or clinical signs of tamponade. Of the 19 patients in whom on-table TTE identified a pericardial effusion, 13 (68%) showed an increase in size prior to discharge (range of increase 0.1–1.54 cm, median 0.2 cm, SD 0.40), and 4 showed a decrease (21%). Seventeen patients had no pericardial effusion on table but 8 of these (47%) went on to develop pericardial effusions at the time of discharge (range 0.19–1.3 cm, median 0.59 cm, SD 0.41). No patients required treatment for these pericardial collections.
Conclusion: Pericardial collections that are detectable on TTE are seen in a significant number of patients after LA catheter ablation for AF. However, in this group of patients this was not associated with any adverse outcome. Discharge TTE identified more pericardial effusions than on-table TTE, and importantly identified effusions that were not present immediately post-procedure. Discharge TTE also identified patients in whom there had been an increase in the size of the effusion. This suggests that discharge rather than on-table TTE would allow more accurate identification of reactive pericardial effusions and therefore identify potentially problematic effusions early. On-table TTE clearly still has a role if the clinical setting warrants this. Ongoing studies in larger numbers of patients will hopefully further validate these findings.
catheter ablation; atrial fibrillation; pericardial effusion
025 THE IMPACT OF LINEAR ABLATION ALONG THE CORONARY SINUS ON THE OUTCOMES OF CATHETER ABLATION FOR PERMANENT ATRIAL FIBRILLATION
K. Rajappan, S. Kalra, M. Kalla, M. Earley, S. Harris, D. Gupta, D. Abrams, S. Sporton, R. Schilling. The Department of Cardiology, St Bartholomew’s Hospital and Queen Mary University, London, UK
Introduction: The success of catheter ablation (CA) in permanent atrial fibrillation (AF) is inferior to paroxysmal AF. The appropriate strategy for additional atrial ablation following wide encirclement of pulmonary vein (PV) pairs in patients with chronic AF remains to be determined. We report the single procedure outcomes of adding linear ablation along the coronary sinus (CS) to the ablation strategy in patients with chronic AF.
Methods and Results: Seventy one consecutive patients (55 male, mean age 60 (10) years) with permanent AF underwent first-time CA guided by electroanatomic mapping and CT integration. Following double trans-septal puncture wide encirclement of PV pairs was performed using irrigated radiofrequency ablation with the endpoint of electrical isolation. In the first 34 patients (control group) linear ablation was performed at the left atrial (LA) roof, right atrial isthmus and complex fractionated LA electrical activity was targeted. In the subsequent 37 patients (study group) ablation along the inferior LA parallel to the CS catheter and ablation within the CS (30 Watts) was performed with the endpoint of electrical disconnection. If AF persisted on completion of the lesion set internal DC cardioversion was performed. Procedure times were similar in both groups (268 (61) (control) vs 270 (71) min (study); p = NS). There were no additional complications from CS ablation. There was no difference in the number of patients who needed DC cardioversion at the end of the procedure (22 control vs 25 study). All patients were in SR at the end of the procedure and on the first day afterwards. At follow-up (19 (12) weeks) 16/34 patients (47%) were free of AF in the control group compared with 16/37 patients (43%) in the study group (χ2 = 0.10; p = NS). Of those with recurrence 26 had AF (15 control vs 11 study) and 13 had atrial tachycardia (3 control vs 10 study) (AF vs atrial tachycardia for the two groups χ2 = 4.18; p<0.05).
Conclusions: The addition of CS linear ablation for CA of permanent AF did not improve acute or medium term outcomes. There was a lower recurrence of AF and more atrial tachycardia in the linear CS ablation group. Atrial tachycardia may be more amenable to further ablation and hence improve outcome in the longer term.
atrial fibrillation; catheter ablation; coronary sinus
026 CATHETER ABLATION FOR PERMANENT ATRIAL FIBRILLATION: ARE OUTCOMES IMPROVED BY ABLATION RESTORING SINUS RHYTHM WITHOUT ELECTRICAL CARDIOVERSION?
K. Rajappan, P. Kistler, M. Kalla, S. Kalra, L. Richmond, M. Earley, S. Harris, D. Gupta, D. Abrams, S. Sporton, R. Schilling. The Department of Cardiology, St Bartholomew’s Hospital and Queen Mary University, London, UK
Introduction: Catheter ablation (CA) is successful in restoring sinus rhythm (SR) in patients with long standing persistent atrial fibrillation (AF). However whether AF which terminates as a direct result of CA translates to an improved clinical outcome is yet to be determined. The aim of the study was to determine if clinical outcomes were improved in patients where SR was restored in response to CA.
Abstract 026
Methods and Results: 71 consecutive patients (55 male, mean age 60 (10) years) with chronic AF underwent first-time CA guided by electroanatomic mapping and CT integration. Following double trans-septal puncture wide encirclement of pulmonary vein (PV) pairs was performed with the endpoint of electrical isolation. If AF persisted linear ablation was performed at the LA roof (55 patients), inferior LA and CS (37 patients) and RA isthmus (34 patients). Complex fractionated left atrial electrical activity was targeted in 46 patients. If AF persisted following the standard lesion set DCCV was performed (DCCV group; n = 48). CA restored SR in 23 patients (ABL group). During CA if SR was restored (n = 9) the lesion set was not completed. If AF organised activation mapping was performed (14 patients). All patients were in SR at the end of the procedure and on the 1st day afterwards. Based on absence of symptoms and freedom from AF on 7-day Holter monitor, success after a single procedure off antiarrhythmic drugs was achieved in 20/48 patients (42%) in the DCCV group vs 12/23 patients (52%) in the ABL group (χ2 = 0.69; p = NS) at a median follow-up of 16 (12) weeks. Recurrent arrhythmias (n = 39) were AF (19 DCCV vs 8 ABL) and atrial tachycardia (AT) (9 DCCV vs 3 ABL) (χ2 = 0.09 for AF vs AT in each group; p = NS). These results were not affected by ablation within the CS (see table).
Conclusions: Permanent AF which terminates as a direct result of CA was not associated with an improvement in clinical outcomes at medium term follow up in this group of patients. Whether this result is reproduced in a larger group of patients with longer-term follow-up remains to be seen. Following completion of a standardised lesion set, DCCV was successful in restoring sinus rhythm.
catheter ablation; atrial fibrillation; electrical cardioversion
027 SIMPLE DOSE LIMITATION MANOEUVRES CAN SIGNIFICANTLY REDUCE RADIATION EXPOSURE DOSE DURING RADIOFREQUENCY ABLATION
D. Rogers, F. England, A. Ahmed, M. Dhinoja, M. Lowe, P. Lambiase, A. Chow. The Heart Hospital, London, UK
Introduction: Fluoroscopy guided catheter ablation is increasingly used for the treatment of both simple and complex arrhythmias. Radiation exposure during ablation procedures poses a risk to both patient and operators. We examined the effects of practical dose reduction manoeuvres in the electrophysiology lab.
Methods: The following changes were instigated for all ablation procedures: (1) reduced pulsed fluoroscopy dose; (2) removal of secondary radiation (scatter) grids; (3) optimising use of collimation; (4) maximising field of view; (5) halving frame rate for acquisitions to 6.25 frames per second. Radiation dose and screening time were analysed for the periods 16 months before and 15 months after these dose reduction manoeuvres. Ablations were classified as simple (AV nodal re-entrant tachycardias, right atrial flutters and accessory pathway procedures) or complex (left atrial fibrillation and ventricular tachycardia).
Results: A total of 759 ablation procedures (544 simple, 215 complex) were analysed. Screening times were unchanged before and after dose reduction manoeuvres (simple 26.4 (1.5) vs 23.6 (1.3) min, p = NS; complex 47.5 (3.0) vs 51.1 (1.9) min, p = NS). There were 68% and 39% reductions in radiation exposure after dose reduction interventions for simple and complex ablation procedures respectively (fig).
Conclusion: The safety of ablation procedures can be improved by simple radiation protection manoeuvres. These measures can significantly reduce radiation doses for both simple and complex ablations.
radiofrequency ablation; x ray radiation; dose reduction
028 THE IMPACT OF IMAGE INTEGRATION ON CATHETER ABLATION OF ATRIAL FIBRILLATION USING ELECTROANATOMIC MAPPING: A PROSPECTIVE RANDOMISED STUDY
P. Kistler, K. Rajappan, S. Harris, D. Gupta, L. Richmond, S. Ellis, S. Sporton, R. Schilling. 1The Department of Cardiology, St Bartholomew’s Hospital and Queen Mary University, London, UK; 2The Department of Radiology, St Bartholomew’s Hospital and Queen Mary University, London, UK
Background: A detailed appreciation of left atrial/pulmonary vein (LA/PV) anatomy may be important in improving the safety and success of catheter ablation (CA) for atrial fibrillation (AF). The aim of the study was to determine the impact of CT image integration into a 3D electroanatomical mapping system (EAM) on acute procedural outcomes and duration in patients undergoing CA for AF.
Abstract 028
Methods: Eighty patients with AF were randomised to undergo first time wide encirclement of ipsilateral PV pairs using EAM alone or with additional CT image integration (Cartomerge). Wide encirclement of the PVs was performed using irrigated radiofrequency ablation (RFA) with the electrophysiological endpoint of electrical isolation (EI). Patients in persistent AF underwent additional CA (line at roof, CS and RA isthmus and complex fractionated electrograms) in an attempt to restore SR with RFA. Acute procedural outcomes and procedure durations were determined (see table).
Results: Acute procedural outcomes (EI, PV reconnection, SR restored by ablation in persistent AF, fluoroscopy time) and procedure durations (EI of right PVs, EI of left PVs, total) did not differ significantly between EAM and CTI groups (see table). PV stenosis was not demonstrated in either group.
Conclusion: Image integration to guide catheter ablation for AF did not significantly improve intraprocedural outcomes or duration. The impact of image integration on clinical outcomes awaits long-term follow-up.
catheter ablation; atrial fibrillation; image integration
029 EFFICIENT CARDIAC GENE DELIVERY TO RAT HEART BY INTRAVASCULAR INJECTION OF ADENO-ASSOCIATED VIRUS 6
R. Masson1, L. Work1, S. Nicklin1, P. Gregorevic2, J. Allen2, J. Chamberlain2, A. Baker1. 1BHF Glasgow Cardiovascular Research Centre, University of Glasgow, Glasgow, UK; 2Senator Paul D Wellstone Muscular Dystrophy Cooperative Research Centre, University of Washington, Seattle, USA
Introduction: A major challenge to overcome in cardiac gene delivery is the limited availability of vectors that provide efficient delivery via a minimally invasive route. Adeno-assocatied viruses (AAVs) are promising vectors for gene therapy and to date 11 serotypes of AAV have been identified. Therefore, exploitation of alternative AAV isolates with differing tissue tropisms could overcome this limitation. Recombinant AAV vectors pseudotyped with serotype 6 capsid proteins (rAAV6) have been shown to transduce skeletal muscle at levels >500-fold higher than rAAV2 vectors in mice, with extensive transgene expression throughout the entire musculature including cardiac muscle.1 Expression was dependent on co-administration with a vascular permeabilising agent (VEGF) for the lower dose vectors. We investigated rAAV6 vectors and their validity as systemic gene transfer vectors in an established disease model in rats; stroke prone spontaneously hypertensive rats (SHRSP).
Methods: To study transduction we administered a single intravenous injection of rAAV6-CMV-lacZ vectors at three different doses (2×1011, 1.5×1012 and 3×1012 vp/rat) ± rVEGF into 6-week-old SHRSP rats. Striated muscle was examined after 14 days or 3 months and β-galactosidase activity compared to that of untreated rats. Immunohistochemistry (IHC) was also performed to confirm the expression of lacZ within the myocardium. Taqman was used to compare lacZ presence between different tissue types and animals.
Results: The LacZ gene and its product were located in the heart and various skeletal muscle beds as determined by X-gal staining, Taqman and IHC. X-gal staining results showed that gene expression had occurred throughout the musculature but not within other tissues (kidney, liver, spleen and lung). At the highest dose, Taqman revealed viral accumulation in the heart, muscle, liver and spleen (1300, 1100, 1100 and 45 vg/100 ng DNA, respectively). IHC showed a dose-dependent response with the highest β-galactosidase staining in the hearts of the highest dose animals. β-galactosidase activity was present in the heart 3 months post-injection demonstrating the longevity of transgene expression. Results indicate that β-galactosidase activity levels are independent of VEGF co-administration.
Conclusions: Due to the extensive transduction of cardiac muscle observed in this investigation, this vector may be suitable as a systemic vector for cardiac gene delivery. As rAAV6 also targets striated muscle inclusion of a cardiac transcriptional-regulator may further improve selectivity.
AAV-6; gene delivery; myocardium
1
030 THE ADIPOCYTOKINE, VISFATIN, REDUCES MYOCARDIAL INFARCT SIZE, WHEN GIVEN AT TIME OF REPERFUSION, BY INHIBITING THE MITOCHONDRIAL PERMEABILITY TRANSITION PORE
D. Hausenloy, L. Shiang-Yong, A. Paramanathan, S. Davidson, C. Smith, D. Yellon. The Hatter Cardiovascular Institute, UCL, London, UK
Introduction: Adipose tissue, formerly regarded as purely an energy storage site, is now recognised as an active endocrine organ, producing various hormones, which include “adipocytokines”. In this study we investigated the cardioprotective potential of the recently discovered adipocytokine, visfatin, which has been demonstrated to act as an insulin-mimetic and activate Akt, a protein kinase which has been implicated in cardioprotection. The mitochondrial permeability transition pore (mPTP), a non-specific mitochondrial channel whose opening at the time of myocardial reperfusion increases myocardial infarct size is also a viable target for cardioprotection. In this study we hypothesised that visfatin protects the ischaemic heart through the inhibition of mPTP opening.
Methods: Three different experimental models were used: (1) C57BL/6 male mice were anaesthetised and subjected to in situ 30 min of regional myocardial ischaemia and 120 min of reperfusion at the end of which myocardial infarct size was determined by tetrazolium staining. Visfatin (50 pmol) or normal saline vehicle were given as an intravenous bolus at time of myocardial reperfusion. (2) Isolated Wistar rat ventricular cardiomyocytes were subjected to an 60 min of hypoxia followed by 30 min of reoxygenation, at the end of which cell viability was determined by staining with propidium iodide. Visfatin (100 ng/ml) or normal saline vehicle were given at the time of reoxygenation. (3) Isolated C57BL/6 murine ventricular cardiomyocytes loaded with the fluorescent dye, TMRM, were incubated in either visfatin (100 ng/ml) or normal saline vehicle, for 15 min before being subjected to confocal laser-induced oxidative stress to provoke mPTP opening.
Results: (1) Visfatin given at time of myocardial reperfusion was found to reduce myocardial infarct size from 43.0 (5.0)% in control animals to 27.3 (4.0)% (n>9/group: p<0.05). (2) Visfatin given at time of reoxygenation was also found to reduce % cell death from 30.7 (2.9)% in control to 11.4 (0.7)% (n>60 cells/group from 4 animals: p<0.05). (3) Finally, visfatin was found to increase the time taken to induce mPTP opening from 90 (16) seconds in control to 231 (23) seconds (n>10/group: p<0.05).
Conclusions: This study demonstrates for the first time that the recently discovered adipocytokine, visfatin, reduces myocardial infarct size when given at time of myocardial reperfusion, and improves cell viability when given at time of reoxygenation. The protection appears to be mediated through the inhibition of mPTP opening. The clinical implications of these findings are that visfatin or its pharmacological analogue may provide a novel treatment for diabetes mellitus, while also conferring a powerful cardioprotective effect.
visfatin; adipocytokine; cardioprotection
031 METFORMIN GIVEN AT TIME OF REPERFUSION REDUCES MYOCARDIAL INFARCT SIZE THROUGH THE AKT-MEDIATED INHIBITION OF MITOCHONDRIAL PERMEABILITY TRANSITION PORE OPENING
D. Hausenloy, G. Bhamra, S. Davidson, R. Carr, M. Mocanu, D. Yellon. The Hatter Cardiovascular Institute, UCL, London, UK
Introduction: In addition to its hypoglycaemic actions, metformin has been demonstrated in clinical studies to be cardioprotective, the mechanism of which is unclear. Previous studies have demonstrated in the non-diabetic heart, that the activation of the survival kinase, Akt, and the subsequent inhibition of mitochondrial permeability transition pore (mPTP) opening at time of reperfusion, reduces myocardial infarct size. The mPTP is a non-specific channel of the inner mitochondrial membrane whose opening at the time of myocardial reperfusion mediates cardiomyocyte death. Interestingly, previous studies suggest that metformin can inhibit the opening of the mPTP. Therefore, we hypothesised that metformin given at time of reperfusion protects the ischaemic diabetic heart through the inhibition of mPTP opening, and that this effect is mediated via Akt.
Methods: Hearts were excised from diabetic Goto-Kakizaki rats and non-diabetic Wistar control rats and were subjected to 35 min ischaemia followed by either (1) 120 min of reperfusion, at the end of which myocardial infarct size was determined by tetrazolium staining or (2) 15 min of reperfusion after which a myocardial sample was taken for determination of Akt and PTEN phosphorylation (the phosphatase which negatively regulates Akt, which becomes inactivated on phosphorylation) by western blotting. Metformin (50 μmol/l) was given for the first 15 min of reperfusion in the presence or absence of the PI3K inhibitor, LY294002 (15 μmol/l). In a separate set of experiments, the effect of metformin in the presence or absence of LY294002 on the susceptibility to mPTP opening was determined in both diabetic and non-diabetic ventricular cardiomyocytes subjected to oxidative stress.
Results: Metformin given at the time of reperfusion, significantly reduced myocardial infarct size in both non-diabetic Wistar rat hearts (35 (2.7)% metformin vs 62 (3.0)% control: n>6/group; p<0.05) and Goto-Kakizaki diabetic rat hearts (43 (4.7)% metformin vs 60 (3.8)% control: n>6/group; p<0.05). This protective effect of metformin was accompanied by a significant increase in phosphorylation of both Akt and PTEN. Both the Akt phosphorylation and the infarct limiting-effect of metformin were abolished by LY294002 in both the non-diabetic heart (61 (6.7)% metformin+LY294002 vs 35 (2.7)% metformin: p<0.05) and diabetic heart (56 (5.7)% metformin+LY294008 vs 43 (4.7)% metformin: p<0.05). Metformin was demonstrated to inhibit mPTP opening in both non-diabetic and diabetic myocytes subjected to oxidative stress, in a LY294002 sensitive manner.
Conclusions: We demonstrate for the first time that metformin given at time of reperfusion reduces myocardial infarct size in the diabetic heart. Furthermore, this protection appears to be executed through the Akt-mediated inhibition of mitochondrial permeability transition pore opening, a finding which may in part explain the cardioprotective properties of metformin observed in clinical studies.
metformin; reperfusion injury; mitochondrial permeability transition pore
032 DIFFERENTIAL ROLE OF NNOS IN HEART RATE REGULATION BETWEEN REST AND EXERCISE
D. Adlam1, J. de Bono1, B. Casadei1, D. Paterson2, K. Channon1. 1Department of Cardiovascular Medicine, University of Oxford, Oxford, UK; 2Department of Physiology, Anatomy and Genetics, University of Oxford, Oxford, UK
Introduction: Nitric oxide produced by neuronal nitric oxide synthase (nNOS) regulates vagal nerve function in vitro. Upregulation of nNOS appears to be one mechanism underlying the development of resting bradycardia with exercise training. Our understanding of the role of nNOS in heart rate control during different spontaneous activity states, and how this is modulated by exercise training remains limited. Accordingly, we used continuous radiotelemetry combined with detailed analysis of physical activity to investigate changes in heart rate in nNOS knockout (nNOS-KO) mice during different spontaneous activity states and in response to exercise training.
Methods: Radiotelemeters were implanted in nNOS-KO mice and wild type littermates (WT), to provide continuous haemodynamic monitoring. After recovery, mice were placed in cages containing freely rotating voluntary running wheels. Heart rate was measured on a beat to beat basis. Activity state of the mouse for each individual heart beat was determined by logging individual wheel rotations and detecting movement of the animal within the cage. The following activity states were defined: wheel running, cage activity, and rest.
Results: Mice increased both running time and speed over the first 14 days of exercise training. In untrained mice (days 1–5) there was no overall difference in mean daily heart rate between nNOS-KO (574 (8) bpm) and WT mice (592 (8) bpm, p = 0.13). Exercise training led to a fall in mean heart rate in both nNOS-KO (days 25–40: 540 (5) bpm) and WT mice (534 (13) bpm), although there was still no effect of genotype. However analysis of heart rate according to activity state revealed clear differences. Untrained nNOS-KO mice were bradycardic at rest compared with WT mice (nNOS 523 (7) bpm, WT 552 (8) bpm, p = 0.02), but there was no difference in their heart rate during cage activity (nNOS 624 (9) bpm, WT 635 (11) bpm, p = 0.5) or while running on the wheel (nNOS 732 (13) bpm, WT 730 (15) bpm, p = 0.9). During exercise training, heart rate at rest (nNOS 490 (6) bpm, p = 0.002; WT 494 (14) bpm, p = 0.009) and during activity (nNOS 596 (9) bpm, p = 0.007; WT 575 (15) bpm, p = 0.008) decreased in both WT and nNOS-KO mice. The decrease was greater in WT mice, so that in trained mice there was no longer any genotype difference in resting heart rate (p = 0.8). In contrast, heart rate during wheel running decreased in the WT animals (692 (13) bpm, p = 0.03) but not in the nNOS-KO (733 (10) bpm, p = 0.92).
Conclusions: Important differences in heart rate regulation resulting from nNOS gene deletion are revealed only by continuous beat to beat analysis according to activity and exercise state. An important role for nNOS in heart rate control is demonstrated by a resting bradycardia in nNOS-KO mice that is abolished by exercise training. However, a fall in resting heart rate in both wild type and nNOS-KO mice suggests that nNOS is not the sole mediator of exercise induced bradycardia.
neuronal nitric oxide synthase; autonomic function; exercise training
033 IS INCREASED MYOCARDIAL OXIDATIVE STRESS AN EARLY EVENT IN THE NATURAL HISTORY OF ATRIAL FIBRILLATION?
S. Reilly1, W. Idigo1, M. Zhang2, A. Hale2, U. Schotten3, N. Alp1, B. Casadei1. 1University of Oxford, Department of Cardiovascular Medicine, John Radcliffe Hospital, Oxford, UK; 2Department of Cardiovascular Medicine, Wellcome Trust Centre of Human Genetics, Oxford, UK; 3Department of Physiology, Cardiovascular Research Institute Maastricht, Maastricht University, Maastricht, Netherlands
Background: Atrial fibrillation (AF) is known to induce progressive myocardial remodelling, which in turn promotes AF maintenance and increases vulnerability to relapse. Although these features have been extensively documented both in animal models and in humans, the mechanisms triggering electrical and structural remodelling in the fibrillating atrial myocardium have remained largely unexplored. Emerging evidence indicates that myocardial oxidative stress and NADPH oxidase activity are increased in the fibrillating human atrial myocardium; however, it remains unclear whether this is an early event in the natural history of AF, contributing to AF-induced remodelling, or a late by-product of this process.
Methods and Results: Here we evaluated basal and NADPH stimulated superoxide (O2-) production in the left (LA) and right (RA) atria of goats with pacing-induced AF for 2 weeks (LA-AF: n = 18; RA-AF: n = 11) and control goats in sinus rhythm (LA-C: n = 19, RA-C: n = 13), using lucigenin (5 μmol/l)-enhanced chemiluminescence. Since uncoupled NOS contributes to atrial O2- generation in sustained human AF, we compared the effect of L-NAME on O2- generation and the level of the NOS cofactor tetrahydrobiopterin (BH4) and its oxidized products (by high-performance liquid chromatography) in atrial tissue from AF and C goats. eNOS and nNOS expression was evaluated by immunoblotting. AF caused a significant shortening of the left atrial effective refractory period (C: 148 (7.5) ms vs AF: 81 (12) ms, p<0.01), confirming that electrical remodelling had occurred at this stage. O2- production was significantly higher in LA compared with RA, both in C and AF goats (fig). There was no difference in basal O2- production between AF and C groups; however, NADPH-stimulated O2- production was significantly enhanced in the LA of goats with AF (fig). Inhibition of NOS by L-NAME did not affect NADPH-stimulated O2- production in the LA and RA of either AF or C. Neither atrial biopterin levels nor the ratio of BH4 to oxidized biopterins differed between groups (BH4/oxidized biopterin ratio: LA-C: 0.75±0.25; LA-AF: 0.64 (0.10), RA-C: 0.73 (0.05); RA-AF: 0.64 (0.10)). eNOS expression remained unchanged but nNOS protein level was significantly increased in the LA from goats in AF.
Conclusions: Our findings indicate that LA NAD(P)H oxidase activity is already significantly increased after 2 weeks of AF. However, at this early stage, NOS activity is not yet uncoupled, suggesting that this phenomenon occurs later in the natural history of AF. Increased nNOS expression in AF suggests that this isoform may also be involved in the early remodelling process—for example, in mediating calcium current (ICa) downregulation which is a hallmark of AF.
atrial fibrillation; superoxide; nitric oxide synthase
034 CARDIAC AND SYSTEMS BIOLOGY OF ISOFORM 4 OF THE PLASMA MEMBRANE CALCIUM ATPASE
E. Cartwright, F. Baudoin, D. Oceandy, S. Prehar, M. Zi, L. Neyses. University of Manchester, Manchester, UK
Introduction: The plasma membrane calcium/calmodulin dependent ATPase (PMCA) is a ubiquitously expressed calcium-extruding enzymatic pump which is the only system to extrude calcium from the cytosol of the majority of cells. In the heart, however, the sodium/calcium exchange is responsible for bulk calcium removal, leaving the role of PMCA unclear. To determine the functional role of the ubiquitous isoform PMCA4, and the effect of its deletion on the whole mouse we have employed systems biology. In analysing over 100 parameters we have carried out the most complete phenotyping of any calcium transporter gene knockout mouse.
Methods: We have previously generated a PMCA4 null mutant mouse line (PMCA4 KO); these mice are viable, have a normal lifespan, and although the females display normal fertility the males are completely infertile due to the sperm being immotile or having no directed or progressive motility. Analysis of the heart by echocardiography revealed no differences in heart rate, wall and septum thicknesses and fractional shortening between PMCA4 KO and wild type (WT) controls, and blood pressure remained unaltered. Invasive haemodynamic analysis did, however, reveal that both contractility and speed of relaxation were significantly elevated in PMCA4 KO mice. To determine the pathophysiological relevance of PMCA4 in the heart hypertrophy was induced by chronic beta-adrenergic stimulation. PMCA4 KO and WT mice showed the same hypertrophic response leading to increased cardiac mass and wall thickness, however, PMCA4 KO mice did not display the normal deleterious delay in diastolic relaxation.
Results: We determined that there was no deleterious effect due to the deletion of this calcium pump on skeletal formation; x ray analysis and dexascan showed no changes in bone density, structure and mineral content. No significant difference in plasma chemistry parameters such as urea, creatinine, sodium, potassium, chloride, bicarbonates, total proteins, albumin, phosphorus and magnesium was observed between WT and PMCA4 KO mice. Notably, no significant differences in calcium levels were observed. Behavioural tests designed to investigate a wide range of nervous system functions or their pathologies showed essentially no differences between PMCA4 KO and WT mice, although the mutant males did show a tendency to increased anxiety. Auditory and visual functions remained unaffected; auditory brainstem responses suggested normal function of the inner ear and electroretinography and optomotor response showed that retina function was unaltered. Deletion of PMCA4 also had no impact on calorimetric analysis, a standard clinical measure of well-being.
Conclusions: This analysis has shown that although PMCA4 is ubiquitously expressed its function is highly tissue specific, with physiological/pathophysiological relevance in the sperm and cardiovascular system. It identifies PMCA4 as a novel target for developing inhibitors for the treatment of diastolic dysfunction.
plasma membrane calcium pump; systems biology; diastolic dysfunction
035 PLASMA MEMBRANE CALCIUM ATPASE PUMP ISOFORMS 1 AND 4 DIFFERENTIALLY REGULATE HEART CONTRACTILITY
T. Mohamed, D. Oceandy, N. Alatwi, F. Baudoin, E. Cartwright, L. Neyses. University of Manchester, Manchester, UK
Introduction: The role of plasma membrane calcium ATPase (PMCA), a calcium extruding enzyme, in cardiac physiology is not entirely clear. Two isoforms of PMCA, PMCA1 and 4, are expressed in the myocardium. Previously, we and others have suggested a new function for PMCA4 as a modulator of signal transduction pathways through modulation of neuronal nitric oxide synthase (NOS-1) activity but the differential role of the isoform 1 and 4 remains enigmatic. Myocardial contractility and relaxation were known to be highly affected by the degree of phospholamban (PLB) phosphorylation.
Aim: To investigate the role of PMCA1 and whether it is also involved in cellular signalling or in excitation-contraction coupling.
Methods: In vitro studies in transfected HEK293 cells showed that either PMCA1 or 4 forms a complex with NOS-1; these interaction complexes were also present in cardiac tissue. These complexes were found to modulate NOS-1 activity; however, the functionality of the interactions varied with PMCA4 inhibiting NOS-1 activity twice as much as PMCA1.
Results: To study the differential effect in vivo we generated transgenic mice (tg) overexpressing PMCA1 or PMCA4 in the heart. In PMCA1 tg the in vivo α-inotropic response, as assessed by left ventricular pressure/volume measurements, was augmented, whereas it was reduced in PMCA4 tg. In wild type animals (WT) isoproterenol increased the load-independent contractility index (end systolic elastance) by 47 (13)% compared to only 11 (5)% in PMCA4 tg littermates; in contrast, in PMCA1 tg the response was greatly increased to 159 (32)% (n = 8 in each group, p<0.05 for WT vs both tgs). Using isolated adult cardiomyocytes from the transgenic animals immunoblotting showed a higher ratio of ser-16 phosphorylation of phospholamban in PMCA1 tg animals after stimulation with isoproterenol (ser-16 PLB/PLB ratio: 29.21 (3.64) in WT vs 50.28 (8.3) in PMCA1 tg, n = 7 each, p<0.05).
Conclusions: Increased PLB phosphorylation after isoproterenol stimulation in PMCA1 tg animals indicated that PMCA1 may be involved in excitation-contraction coupling specifically after α-adrenergic stimulation. In contrast, the subdued response to β-adrenergic stimulation in PMCA4 tg was mediated by the inhibition of NOS-1. These findings show that both PMCA1 and 4 have a relevant although different physiological function in the heart.
plasma membrane calcium atpase; neuronal nitric oxide synthase; phospholamban
036 GLIMEPIRIDE TREATMENT FACILITATES THE PROTECTIVE EFFECT OF ISCHAEMIC PRECONDITIONING IN THE DIABETIC HEART
D. Hausenloy, A. Wynne, M. Mocanu, D. Yellon. The Hatter Cardiovascular Institute, UCL, London, UK
Introduction: Ischaemic preconditioning (IPC) describes the reduction in myocardial infarct size obtained from applying one or more episodes of transient myocardial ischaemia/reperfusion prior to the index ischaemic event. Our previous studies suggest that the diabetic heart may be resistant to IPC when compared to the non-diabetic heart, such that three cycles of IPC, instead of the normal one cycle of IPC, are required to reduce myocardial infarct size. The aim of the present study was to determine whether treatment with the anti-diabetic sulphonylurea, glimepiride, is able to normalise the response of the diabetic heart to IPC, by reducing the threshold of IPC required to confer cardioprotection.
Abstract 036 Infarct size expressed as a percentage of the risk zone (I/R%)
Methods: Diabetic GK rats were randomised to receive three different glimepiride treatment protocols: rats received either glimepiride (20 mg/kg/day, by oral gavage) or methylcellulose vehicle for either (1) 12 weeks or (2) 24 hours, following which the hearts were excised and mounted on a Langendorff apparatus. In the third group (3) the hearts were excised and mounted on a Langendorff apparatus and glimepiride (20 μmol/l) was given immediately prior to IPC. Rat hearts were subjected to 35 min ischaemia and 120 min reperfusion, at the end of which infarct size was determined by tetrazolium staining. Preconditioned hearts received either 1 or 3 cycles of IPC (each cycle comprising 5 min ischaemia with an intervening 10 min reperfusion) prior to the index ischaemic period.
Results: Hearts taken from diabetic GK rats that had not received glimepiride treatment were not protected by 1 cycle of IPC and required 3 cycles of IPC to reduce myocardial infarct size (see table). However, in hearts taken from diabetic GK rats that had been treated glimepiride, irrespective of the treatment protocol, both 1 cycle as well as 3 cycles of IPC reduced myocardial infarct size (see table). This effect of glimepiride was not mediated by its hypoglycaemic effect, as no change was observed in serum glucose levels in rats given glimepiride.
Conclusions: We confirm that the diabetic heart is resistant to IPC, such that they require 3 cycles instead of 1 cycle of IPC to reduce myocardial infarct size. Importantly, treatment with glimepiride appears to normalise the response to IPC, permitting 1 cycle of IPC to reduce myocardial infarct size. These findings suggest that the resistance of the diabetic patients to the cardioprotective effects of IPC may be overcome by treatment with glimepiride.
diabetic; preconditioning; glimepiride
037 PRECONDITIONING AND POSTCONDITIONING: THE MITOCHONDRIAL PERMEABLITY TRANSITION PORE AS THE COMMON END-EFFECTOR
L. Shiang-Yong, D. Hausenloy, S. Davidson, D. Yellon. The Hatter Cardiovascular Institute, UCL, London, UK
Introduction: The mitochondrial permeability transition pore (mPTP) is a non-specific channel of the inner mitochondrial membrane whose opening at the time of myocardial reperfusion mediates cardiomyocyte death. Mitochondrial cyclophilin D (CYP-D) has been demonstrated in recent studies to be a component of the mPTP. Emerging studies suggest that the phenomena of ischaemic preconditioning (IPC) and ischaemic postconditioning (IPost) may confer cardioprotection through the inhibition of mPTP opening. In order to determine the importance of the mPTP to cardioprotection in these settings, we investigated whether the hearts of CYP-D −/− mice (which lack a functional mPTP) can be protected by ischaemic and pharmacological preconditioning and postconditioning.
Methods: CYP-D −/− and B6Sv129F1 (wild type) male mice were anaesthetised and subjected to in situ 30 min of regional myocardial ischaemia and 120 min of reperfusion at the end of which myocardial infarct size was determined by tetrazolium staining. Mice were randomised to the following treatment groups: (1) vehicle controls; (2) IPC: which comprised 5 min of ischaemia followed by 5 min of reperfusion; (3) IPost-1: which comprised 10 sec of ischaemia followed by 10 secs of reperfusion repeated three times applied at the end of the index ischaemic period; (4) IPost-2: the ischaemia-reperfusion algorithm described above repeated six times; (5) Dzx: pharmacological preconditioning with diazoxide (5 mg/kg) given 10 min before the index ischaemic period; (6) Bradykinin: pharmacological post-conditioning using bradykinin (40 mg/kg) given at reperfusion; (7) CsA: Ciclosporin-A (10 mg/kg) was given at reperfusion; (8) SfA: Sanglifehrin-A (25 mg/kg) was given at reperfusion.
Results: As expected, wild type hearts were protected by both IPC and IPost and all the pharmacological agents. Interestingly however, CYP-D −/− hearts were not protected by either IPC, IPost or any of the pharmacological agents.
Conclusions: This study demonstrates for the first time that cardioprotection elicited by ischaemic and pharmacological preconditioning and post-conditioning requires the presence of a functional mPTP. This confirms the crucial role of the mPTP in the mechanistic pathway of preconditioning and post-conditioning, therefore positioning the mPTP as a target for cardioprotection in patients presenting with acute myocardial infarction or undergoing cardiac bypass surgery.
mitochondrial permeability transition pore; preconditioning; post-conditioning
038 C-TERMINAL PRO-ENDOTHELIN-1 OFFERS ADDITIONAL PROGNOSTIC INFORMATION WITH NTPROBNP IN PATIENTS FOLLOWING ACUTE MYOCARDIAL INFARCTION. THE LEICESTER ACUTE MYOCARDIAL INFARCTION PEPTIDE STUDY
S. Khan1, O. Dhillon1, J. Struck2, P. Quinn1, N. Morgenthaler2, I. Squire3, J. Davies1, A. Bergmann2, L. Ng1. 1University of Leicester, Leicester, UK; 2BRAHMS AG, Hennigsdorf/Berlin, Germany; 3University of Leicester, Leicester, Germany
Introduction: Endothelin levels are elevated in heart failure (HF) and after an acute myocardial infarction (AMI) give prognostic information on mortality. C-terminal Pro-Endothelin-1 (CT-proET-1) a precursor of ET is more stable in circulation and ex-vivo. We investigated the cardiovascular prognostic value post-AMI of CT-proET-1 and compared it to N-terminal B-type natriuretic peptide (NTproBNP), a marker of death and HF.
Abstract 038 Infarct size expressed as a percentage of the risk zone (I/R%)
Methods: We measured plasma CT-proET-1 and NTproBNP in 983 consecutive post-AMI patients (721 men, mean age 65.0 (SD 12.2) years), 3–5 days after chest pain onset. NTproBNP was determined using an in-house non-competitive immunoassay and ProET was detected using a novel commercial assay (BRAHMS AG). Patients were followed up for the combined endpoint of death or heart failure.
Results: There were 101 deaths and 49 readmissions with HF during follow up (median 343, range 0–764 days). CT-proET-1 was raised in patients with death or HF compared to survivors (median (range) pmol/l, 119.0 (14.0–671.0) vs 73.0 (4.6–431.0); p<0.0001). Using a Cox proportional hazards logistic model, log CT-proET-1 (HR 6.82) and log NTproBNP (HR 2.62) were significant independent predictors of death or HF (along with age, gender, past history of AMI and therapy with beta blockers). The areas under the receiver-operating curve (AUC) for CT-proET-1, NTproBNP and the logistic model with both markers were 0.76, 0.76 and 0.81 respectively for predicting death or HF at 60 days. CT-proET-1 provided further risk stratification in those patients who had NTproBNP level above the median (log rank for trend 40.29, p<0.001). Findings were similar for death and HF as individual endpoints.
Conclusion: The endothelin system is known to be activated post-AMI. CT-proET-1 is a powerful predictor of adverse outcome especially in those with an elevated NTproBNP. CT-proET-1 may represent a clinically useful marker of prognosis after AMI.
heart failure; peptides; prognosis
039 PLASMA MMP-9 AND TIMP-1: NOVEL MARKERS OF LEFT VENTRICULAR DYSFUNCTION AND ADVERSE PROGNOSIS AFTER ACUTE MYOCARDIAL INFARCTION IN MAN
D. Kelly1, M. Thompson2, N. Samani1, S. Khan1, G. Cockerill2, L. Ng1, I. Squire1. 1University Hospitals Leicester, Leicester, UK; 2St George’s Hospital Medical School, London, UK
Aims: To investigate the association of plasma MMP-9 and TIMP-1 with ventricular function, remodelling and prognosis after AMI in man.
Methods: We enrolled 404 patients with AMI (81.4% STEMI).Blood was sampled for MMP-9 at 0–12 h post-symptom onset and 24 h intervals and for TIMP-1 immediately prior to discharge. Left ventricular (LV) function and volumes were assessed (echocardiography) pre-discharge and at a median of 148 days. Remodelling was assessed by change in LV volumes (ΔLVEDV) between examinations. The pre-specified primary end-point was a composite of death or heart failure during follow-up (median 314 days, range 1–619).
Results: MMP-9 and TIMP-1 were associated with more severe LV impairment and greater ventricular volumes. MMP-9 correlated with ΔLVEDV (r = 0.173, p = 0.004). In the 65 (16.1%) individuals who reached the primary end point, MMP-9 (106.5 ng/ml vs 66.4, p<0.001) at 0–12 h and TIMP-1 (116.7 ng/ml vs 107.8, p<0.001) were higher compared to survivors. In multivariate analysis each retained independent predictive value for death or heart failure (MMP-9, p = 0.004, TIMP-1, p<0.001). The area under the ROC curves for the prediction of primary end-point were 0.633 for MMP-9, 0.815 for TIMP-1 and 0.828 for a combination. Concentrations above 76 ng/ml for MMP-9 (OR = 1.89, p = 0.003) and 124 ng/ml for TIMP-1 (OR 10.9, p<0.001) were associated with increased risk of death or heart failure. The risk of adverse outcome was greatest if both TIMP-1 and MMP-9 were above these values, lowest if both MMP-9 and TIMP-1 below, with intermediate risk if either TIMP-1 or MMP-9 were above (KM plot).
Conclusion: Following AMI elevated plasma MMP-9 and TIMP-1 are associated with more severe LV impairment, greater LV remodelling and increased risk of death or heart failure. Although TIMP-1 is the more powerful marker of prognosis, the combination of elevated MMP-9 and TIMP-1 increases predictive power.
myocardial infarction; metalloproteinase; MACE
040 THE CRITICAL ROLE OF ERBB2 IN HUMAN LEFT VENTRICULAR REMODELLING DUE TO PRESSURE OR VOLUME OVERLOAD
X. Jin1, J. Hu2, F. Pezzella2, J. Pepper3. 1John Radcliffe Hospital, Oxford, UK; 2NDCLS, Oxford University, Oxford, UK; 3Royal Brompton Hospital, London, UK
Background and Aim: Left ventricular (LV) pressure or volume overload leads to ventricular geometrical remodelling underlined by differential myocardial gene expression. In this study we aimed to determine the key genes that play critical roles in ventricular remodelling, and their physiological functions.
Methods: Intraoperative TOE along with LV pressure and cardiac output recordings were performed in 19 patients (mean age 69 (10) years, 12 males) before starting cardiopulmonary bypass during valve surgery for aortic stenosis (AS, n = 11) or mitral regurgitation (MR, n = 8). Detailed LV structure and function was quantified. Endomyocardial biopsy was obtained immediately after cardioplegia. Using complementary DNA micro-array chip, gene expression profiling data of 11 AS and 8 MR were compared (parametric t test combined with Young permutation multiple test correction, using GeneSpring 6.0). Differentially expressed genes were further analysed using PathwayAssist (Stratagene, incorporated with biomedical literature database), and genes having direct interactions were identified. The predictive values of these key genes’ expression level with respect to LV geometry, muscle mass and contractile function were determined using stepwise regression analysis.
Results: Of 65 genes differentially expressed between AS and MR groups, 9 genes (IRS-1, ERBB2, SMAD3, CPB2, ERBB3, SCAP1, SCAP2, PAI-1 and uPAR) were identified as having direct interactions in cellular molecular biology based on biomedical literature (PathwayAssist). These interactions were indeed confirmed by the significant correlations among 9 genes’ actual expression level by stepwise regression analysis (mean r2 = 61%, p<0.01). ERBB2 was significantly upregulated in AS group (p = 0.004) and had direct correlations with 6 other key genes. Of particularly interesting, ERBB2 was the sole predictor of LV geometry (wall thickness to cavity radius ratio, r2 = 56%, p<0.001), while the other 8 key genes had predicted 50% variations of LV pressure, volume, muscle mass, and ejection time (mean r2 = 50%, p<0.01).
Conclusion: Combined echo-physiology and gene expression profiling provides a unique framework for elucidating clinical cardiac functional genomics. The critical roles that ERBB2 and other key genes have played in human LV remodelling will have profound implications for better understanding and thus more effectively treating heart failure patients, in particularly for those secondary to anti-cancer therapy, by targeting the ERBB receptors.
gene expression profiling; ventricular remodelling; echocardiography
041 THE EFFECT OF INTRODUCING DIURETICS IN COMPENSATED PATIENTS WITH LEFT VENTRICULAR DYSFUNCTION ON QUALITY OF LIFE, PLASMA BNP LEVELS, NBNP LEVELS AND PEAK OXYGEN CONSUMPTION: RESULTS FROM A DOUBLE BLIND, PLACEBO CONTROLLED CROSSOVER STUDY
S. Gupta1, N. Gandhi1, C. Waywell1, N. Clayton1, T. Coppinger1, L. Ng2, N. Brooks1, L. Neyses3. 1Wythenshawe Hospital, Manchester, UK; 2Leicester Royal Infirmary, Leicester, UK; 3University of Manchester, Manchester, UK
Background: Diuretics are used to treat congestion in patients with chronic heart failure (CHF), which improves symptoms and perhaps prognosis based on small trials. In the non-congested patient with left ventricular dysfunction (LVD), little information is available. Two hypotheses appear possible: (1) chronic diuretic therapy causes persistent neuroendocrine activation which is harmful; (2) alternatively, in patients whose neuroendocrine activation is blocked with Angiotensin converting enzyme inhibitors (ACEI) and beta blockers (BB), diuretics may potentially be beneficial—for example, through a decrease in end-diastolic pressures or prevention of incipient congestion. We, therefore, performed a pilot trial to assess the effect of diuretics on quality of life (QOL) measures and surrogate markers of prognosis in non-congested patients with LVD.
Methods: The Manchester Water Study was a randomised, double-blind, placebo controlled, crossover study. 30 patients with stable LVD (ejection fraction <45%) not taking diuretics were recruited. None of the patients had clinical signs of fluid overload and all were on maximally tolerated doses of ACEI and BB. Minnesota QOL score, symptom limited cardiopulmonary exercise tests (pVO2, that is, O2 consumption per minute), plasma BNP and NBNP levels were measured before and after each phase. Patients were randomised to either Torasemide 5 mg/d or placebo for 3 months (Phase A) and after a washout phase of 2 months, crossover performed for 3 months (Phase B).
Results: Twenty eight patients completed the study. Mean age was 59.4 years. No significant statistical carry-over effect from phase A to B was found. Mean BNP levels at the beginning of phase A and B were 13.93 fmol/ml and 14.00 fmol/ml respectively. Mean BNP levels fell by 2.94 fmol/ml on placebo and 3.43 fmol/ml on the diuretic (NS). Mean NBNP levels fell by 5.5 fmol/ml on placebo and 22.6 fmol/ml on diuretic (NS). Mean QOL score at beginning of Phase A was 25.7 (19.6) and at beginning of Phase B was 22.2 (16.1) and remained unaltered. Mean pVO2 at the beginning of Phase A and phase B were 16.6 (3.4) ml/kg/min and 17.1 (4.0) ml/kg/min respectively. Mean pVO2 fell by 0.04 ml/kg/min on placebo and by 0.13 ml/kg/min on diuretic (NS).
Conclusion: Diuretics are not superior to placebo in improving QOL or surrogate parameters of prognosis in patients with LVD who are not clinically congested.
diuretics; heart failure; prognosis
042 IS DIASTOLIC HEART FAILURE A MYTH?
M. Townsend1, D. MacIver2. 1Bristol Royal Infirmary, North Somerset, UK; 2Taunton and Somerset NHS Trust, Taunton, UK
Introduction: Many patients who present with heart failure (HF) have a normal ejection fraction (EF) and left ventricular hypertrophy (LVH). This poorly understood syndrome is often described as diastolic HF or HF with preserved ejection fraction (HFPEF). Long axis shortening is a measure of systolic function. Many HFPEF patients have significantly reduced long axis shortening despite the normal EF. We propose a mechanism which would explain this apparent contradiction and propose that HFPEF may be explained by a reduced stroke volume (SV) rather than diastolic dysfunction.
Abstract 042 Table 1
Abstract 042 Table 2
Methods: We examined the effect of changes in left ventricular wall thickness (LVWT) on EF and SV in non-dilated ventricles using a mathematical model. The model used the truncated ellipsoid method to calculate external and internal LV ventricular volumes and the ventricular muscle volume. The effect of LVWT was then adjusted for changes in long axis displacement. EF and SV were then recalculated.
Results: With normal long axis displacement and increasing LVH the EF increased but the SV was unchanged (table 1). When the LVWT is normal (0.9 cm) a decrease in long axis displacement correlates with a drop in EF and SV (table 2). Importantly, when LVH (LV wall thickness 1.3 cm) is present there is a less significant fall in the EF with a decrease in long axis displacement when compared to the abscence of LVH. (table 2). When LVH is present the EF remains in the normal range until the long axis displacement is markedly reduced to less than 0.5 cm.
Conclusions: The model predicts that patients with heart failure and normal ejection fraction may have significant LV systolic dysfunction as assessed by long axis shortening and this correlates with a fall in the stroke volume. The preserved ejection fraction is directly related to the presence of LVH and the effect of increased muscle mass resulting in increased displacement of the cavity in systole. This study provides an important explanation for the syndrome of heart failure with a normal ejection fraction and LVH. We propose that heart failure with a preserved ejection fraction may be caused by a reduced (systolic) long axis function and reduction in stroke volume rather than diastolic dysfunction.
heart failure; ejection fraction; long axis function
043 PREVALENCE OF HEART FAILURE PRESERVED EJECTION FRACTION IN THE COMMUNITY
G. Mahadevan, L. Williams, R. Campbell, T. Palin, R. Weaver, A. Marsh, F. Hobbs, M. Frenneaux. University of Birmingham, Birmingham, UK
Introduction: Large cross sectional population studies have estimated the prevalence of HFpEF within the population varies from 1.14% to 5.5% depending on the age of the population. The means of identification of clinical heart failure and the threshold used to differentiate reduced from preserved ejection fraction have resulted in vastly differing prevalence of HFpEF. Resting diastolic function appears to be a poor predictor for clinical heart failure. By using metabolic exercise testing as the gold standard we have attempted to define the mechanism of limitation in patients with breathlessness and a preserved ejection fraction.
Methods: 364 subjects over the age of 60 were randomly selected from primary care practice. All participants were asked to complete a questionnaire relating to symptoms of breathlessness and underwent and a transthoracic echocardiogram. A left ventricular ejection fraction (LVEF) >50% was defined as normal. All subjects with a preserved LVEF and NYHA class IIb or worse breathlessness were subsequently invited to undergo metabolic exercise testing using a ramp protocol and full lung function testing to establish the mechanism of limitation.
Results: 348 subjects were found to have a preserved LVEF, of which 52 reported symptoms of at least NYHA Class IIb. Eight patients were unwilling or unable to undergo exercise testing due to concurrent medical illness. Six patients with valvular or ischaemic heart disease as a cause for their symptoms were excluded from further testing. Of the remaining 38 patients, 9 were found to have no objective limitation, 11 were cardiac limited, 11 were lung limited, and 7 patients were unable to perform a diagnostic exercise test (unable to reach anaerobic threshold). In this study 11 patients were found to have HFpEF, resulting in a prevalence in the community of 3%. Of the 52 patients with a preserved LVEF and breathlessness, only 22% were found to have HFpEF.
Conclusion: This study demonstrated that not all patients with a preserved LVEF and breathlessness have cardiac limitation. Metabolic exercise testing is a feasible diagnostic tool in this age group, as the test was non-diagnostic in only 18% of patients.
heart failure; metabolic exercise testing; preserved ejection fraction
044 CARDIORESPIRATORY CONTROL INSTABILITY IN HEART FAILURE: DOES THE CHEMOREFLEX SHOW ADAPTATION OR ARE WE MISSING THE POINT?
C. Manisty1, S. Jaisval2, J. Davies1, N. Hadjiloizou1, A. Hughes1, J. Mayet1, K. Willson1, D. Francis1. 1International Centre for Circulatory Health, Imperial College and St Mary’s Hospital, London, UK; 2Imperial College, London, UK
Introduction: Unstable cardiorespiratory control in heart failure leads to periodic breathing (cyclical oscillations in cardiac and respiratory parameters with a period of about a minute) with accompanying symptomatology and poor prognosis. The principal determinant of cardiorespiratory stability in heart failure patients is chemoreflex gain—the ventilatory sensitivity to changes in carbon dioxide levels. Chemoreflex gain is measured using the rebreathing technique, whereby subjects breathe in a closed loop system, and the slope of the linear relation between ventilation and ETCO2 is measured as the chemoreflex gain. In this method, there is a gradually-rising stimulus of CO2, whereas in periodic breathing there is an oscillatory CO2 stimulus. Most physiological reflexes show adaptation with time, whereby a more gradual onset of a stimulus results in a smaller response (for the same stimulus magnitude). Therefore the rebreathing technique may not be accurately measuring the physiological chemoreflex gain relevant to periodic breathing. We tested the hypothesis that chemoreflex gain shows adaptation—that is, with longer cycle times of oscillatory CO2 stimuli, the gain will reduce.
Methods and Results: We measured chemoreflex gain using our custom-designed method for delivering variable oscillations of inspired CO2 in 24 subjects (17 heart failure subjects: 8 with unstable cardiorespiratory control and 9 with stable control, and 7 age-matched controls). We administered oscillations of inspired CO2 at different stimulus periods: 30, 60, 120 and 240 seconds. Chemoreflex gain was calculated as the amplitude of oscillations in ventilation divided by the amplitude of oscillations in ETCO2, using Fourier analysis to measure the amplitudes. We found that chemoreflex gain is strongly influenced by the cycle time of the stimuli, but in the opposite direction to that expected for adaptation: gain is highest with the longest stimulus cycle length (136, 212, 279, 412 l/min/atm for cycle times of 30, 60, 120 and 240 seconds respectively across all patients: p<0.05 for all paired comparisons, fig 1). Within individual subjects the relationship between cycle length and chemoreflex gain was linear (fig 2).
Conclusions: We conclude that over these clinically-relevant timescales, the chemoreflex shows not adaptation but an entirely opposite phenomenon: it has a greater gain when the cycle time of the oscillatory CO2 stimuli is longer. This is an unusual pattern for a cardiorespiratory reflex, and means that the rebreathing technique for calculation of chemoreflex gain which uses a single slowly-rising stimulus of CO2 cannot be measuring the relevant gain in periodic breathing. Our new technique allows measurements of chemoreflex gain to be made over the physiological cycle time seen in periodic breathing.
periodic breathing; chemoreflex; heart failure
045 CARDIOVASCULAR MAGNETIC RESONANCE PERFUSION IMAGING AT 3 TESLA FOR THE DETECTION OF CORONARY ARTERY DISEASE: A COMPARISON WITH 1.5 TESLA
A. Cheng1, T. Pegg1, T. Karamitsos1, M. Robson1, N. Searle1, M. Jerosch-Herold2, R. Choudhury1, A. Banning1, J. Selvanayagam1. 1John Radcliffe Hospital/Department of Cardiovascular Medicine, Oxford, UK; 2Advanced Imaging Research Center, Oregon Health & Science University, Portland, Oregon, US
Introduction: Myocardial perfusion imaging is one of the most compelling applications for cardiovascular magnetic resonance (CMR) at 3 Tesla (T). 3 T systems provide increased signal-to-noise ratio (SNR) and contrast enhancement (compared with 1.5 T) which can improve spatial resolution and image quality. We aimed to establish the diagnostic accuracy of CMR perfusion imaging at 3 T in patients with suspected coronary artery disease (CAD).
Abstract 045
Methods: Sixty one patients (mean age 64 (8) years) referred for elective diagnostic coronary angiography for investigation of exertional chest pain were studied (pre-angiogram) with first-pass perfusion CMR at both 1.5 T and 3 T, and at stress (140 μg/kg/min intravenous adenosine) and rest. Perfusion imaging on each system was performed at least an hour apart and in randomised order. Four short axis images were acquired during every heartbeat using a saturation recovery fast gradient echo sequence and 0.04 mmol/kg Gd-DTPA bolus injection. Quantitative coronary angiography served as the reference standard. Perfusion analysis of each myocardial segment (except the apex) was performed by visual interpretation by two blinded observers, using the 17-segment model recommended by the American Heart Association. CAD was defined angiographically as the presence of ⩾1 stenosis of ⩾50% diameter in any of the main epicardial coronary arteries or their branches with a diameter of ⩾2 mm. Continuous data were compared using t tests, paired where appropriate. Discrete data were compared using χ2 tests or the Fisher exact test as appropriate. Receiver operating characteristic (ROC) curve analyses were performed to compare the diagnostic performance of perfusion CMR at each field strength. Statistical tests were two-tailed and p<0.05 was considered to be significant.
Results: The prevalence of CAD was 66%. All perfusion images were visually interpretable for diagnosis. 3 T CMR perfusion imaging provided a higher diagnostic accuracy (90% vs 82%), sensitivity (98% vs 90%), specificity (76% vs 67%), positive predictive value (89% vs 84%) and negative predictive value (94% vs 78%) for detection of significant coronary stenoses, compared to 1.5 T. The diagnostic performance of 3 T perfusion imaging was significantly greater than that of 1.5 T in identifying both single vessel disease (area under ROC curve: 0.89 (0.05) vs 0.70 (0.08)) and multi-vessel disease (area under ROC curve: 0.95 (0.03) vs 0.82 (0.06)); p<0.05 for both. 3 T perfusion imaging provided a significant increase in both SNR (17 (6) vs 11 (2) respectively) and contrast-to-noise ratio (17 (10) vs 11 (4) respectively), compared to 1.5 T; p<0.01 for both.
Conclusion: 3 T CMR perfusion imaging is superior to 1.5 T for prediction of significant single and multivessel coronary disease, and may become the preferred CMR field strength for myocardial perfusion assessment in clinical practice.
magnetic resonance imaging; perfusion imaging; coronary artery disease
046 CAN FALSE POSITIVE AND NEGATIVE FIRST PASS MYOCARDIAL PERFUSION MRI SCANS BE EXPLAINED BY CORONARY PHYSIOLOGICAL MEASUREMENTS?
S. Watkins1, T. Steedman1, J. Lyne2, J. Foster1, I. Ford3, H. Dargie1, K. Oldroyd1. 1Western Infirmary, Glasgow, UK; 2Royal Brompton Hospital, London, UK; 3University of Glasgow, Glasgow, UK
Introduction: An ideal screening test for the reliable diagnosis of significant coronary heart disease (CHD) will have a low percentage of false positive and negative results. Stress first pass myocardial perfusion MRI (MPMRI) has a sensitivity and specificity of 80–90%. Artefacts caused by the need for rapid data acquisition are felt to be partially responsible for some loss of accuracy. We have measured fractional flow reserve (FFR), coronary flow reserve (CFR) and the index of microcirculatory resistance (IMR) in a group of patients found to have false positive or negative MPMRI.
Abstract 046
Methods: Eighty six patients with suspected ischaemic cardiac chest pain who were scheduled for coronary angiography/intervention had MPMRI during the week prior to their angiogram. Studies were performed on a Siemens Sonata 1.5 T scanner (Erlangen, Germany) using intravenous adenosine as the stress agent (140 µg/kg/min). During coronary angiography a high fidelity pressure wire with two temperature sensors (Pressure Wire 5, RADI, Uppsala, Sweden) was inserted into the distal third of all major patent epicardial coronary arteries. FFR and CFR were measured during maximal hyperaemia induced by intravenous adenosine. A coronary stenosis was defined as significant if the FFR was <0.75. MPMRI data for each coronary territory was compared with the FFR to identify false positive and negative scans.
Results: Of 258 coronary artery territories there were 11(4%) false positives and 5(2%) false negatives. The table shows a number of potential explanations. An FFR of 0.75–0.8 in the supplying coronary artery is considered to be equivocal and may be functionally significant. A low CFR (<2.5) may indicate microvascular dysfunction and may have contributed to the appearance of a perfusion abnormality. An IMR value of <20 was considered to indicate normal microvascular function in the false negative territories.
Conclusion: The occurrence of false positive and negative MPMRI scans is low using an FFR<0.75 as the cut-off for defining significant coronary disease. Misinterpretations can be partially explained by assessment of the microcirculation in the artery supplying that area. The status of the adjacent coronary arteries may also be important in terms of vascular territory overlap in the false positives, and adjacent coronary occlusions in the false negatives. Ensuring adequate haemodynamic stress is essential and can contribute to false negative results. Artefacts are therefore not always to blame for false positive MPMRI scans.
first pass myocardial perfusion MRI; coronary heart disease; fractional flow reserve
047 ISCAHEMIA AND SCAR BURDEN AFTER ACUTE MYOCARDIAL INFARCTION
S. Plein, J. Younger, P. Sparrow, J. Ridgway, M. Sivananthan, S. Ball, J. Greenwood. University of Leeds, Leeds, UK
Background: Despite a common underlying pathophysiological substrate (the vulnerable plaque), different types of myocardial infarction have diverse morphological consequences as well as different early and late outcomes. These differences are likely to occur as a consequence of the different ratio of permanently damaged (scar) tissue and myocardium remaining at ischemic risk after the acute event. In this study we measured ischaemia and scar burden in patients with Q-wave ST-elevation myocardial infarction (Q-STEMI), non-Q-wave ST-elevation myocardial infarction (NQ-STEMI) and Non-ST-elevation myocardial infarction (NSTEMI) to test the hypothesis that the ratio of scar and ischaemia burden differs between these different types of myocardial infarction.
Methods: Seventy five subjects presenting with acute coronary syndromes were recruited: 25 consecutive patients with NSTEMI, 25 with thrombolysed Q-STEMI and 25 with NQ-STEMI. All patients underwent CMR imaging of myocardial function, perfusion (rest and adenosine-stress) and viability (by late gadolinium-enhancement) 2–7 days after presentation and before any invasive procedures.
Results: Scar burden was highest in Q-STEMI, followed by NQ-STEMI and NSTEMI (24.1%, 15.2% and 3.3% of LV mass, respectively; p<0.001). Ischaemia burden showed a reverse correlation and was lowest in Q-STEMI, followed by NQ-STEMI and NSTEMI (6.9%, 14.7% and 19.9% of LV mass, respectively; p<0.001). The combined burden of scar plus ischaemia was similar between the three groups. Left ventricular ejection fraction was lowest in Q-STEMI and highest in NSTEMI.
Conclusions: The ratio of scar versus ischaemia burden differs significantly between NSTEMI and STEMI as well as between NQ-STEMI and Q-STEMI. These differences may explain the diverse early and late prognosis following different types of myocardial infarction. The higher scar mass in STEMI is a probable substrate for early haemodynamic complications while the ischaemia burden in NSTEMI may be responsible for delayed events in this group.
MRI; coronary heart disease; ischaemia
048 31P CARDIAC MAGNETIC RESONANCE SPECTROSCOPY DURING PHYSIOLOGICAL LEG EXERCISE AT 3 TESLA
L. Hudsmith1, D. Tyler1, Y. Emmanuel1, J. Francis1, S. Petersen1, K. Clarke2, H. Watkins1, M. Robson1, S. Neubauer1. 1Department of Cardiovascular Medicine, University of Oxford, Oxford, UK; 2Department of Physiology, Anatomy, and Genetics, University of Oxford, Oxford, UK
Introduction: The use of phosphorus (31P) magnetic resonance spectroscopy (MRS) provides a unique non-invasive tool to investigate myocardial high-energy phosphate metabolism. Impaired resting energetics have been demonstrated in a number of disease states including hypertension and cardiomyopathies. In many situations, alterations in cardiac energetics will only be unmasked, or in some cases exacerbated, when the heart is stressed. However, exercise 31P MRS spectral acquisition at field strengths of <2 Tesla has been limited by low spatial and temporal resolution requiring the achievement and maintenance of a modest level of exercise for long scan durations (up to 30 min). We aimed to establish cardiac 31P MR spectroscopy during leg exercise at 3T, which, due to the higher signal to noise ratio compared with 1.5T, should allow improvements in temporal (8 min 29 seconds) and spatial (15 ml voxel) resolution in healthy volunteers.
Materials and Methods: 31P MR cardiac spectra were obtained at 3 Tesla in 20 healthy volunteers (10 male and 10 female, mean age 28 (3) years) with no history of cardiac disease, hypertension or cardiac risk factors and a normal baseline electrocardiogram (ECG) at rest, during dynamic physiological leg exercise and after recovery. Exercise consisted of repetitive knee flexion with 0.5 kg weights applied to each ankle with an elastic cord providing additional resistance. All spectra were acquired with a 3D acquisition weighted chemical shift imaging sequence with the acquisition matrix aligned perpendicular to the septum, minimising skeletal muscle contamination. To prevent confounding saturation issues with changing heart rates during exercise, the repetition time was fixed at 1.0 ms, without ECG gating, resulting in a total acquisition time of 8 minutes 29 seconds. Haemodynamic measurements were taken every 2 min and the rate pressure product calculated (product of heart rate and systolic blood pressure).
Results: With exercise in the healthy volunteers, the mean heart rate increased by 73% and the rate pressure product showed an increase of 115%. All datasets were of sufficient quality to be analysed (fig). The mean corrected PCr/ATP ratio for healthy subjects at rest was 2.02 (0.43), exercise 2.14 (0.67) (p = 0.54 vs rest) and at recovery 2.03 (0.52) (p = 0.91 vs rest and p = 0.62 vs exercise).
Conclusion: A cardiac 31P MR spectroscopy physiological exercise-recovery protocol is feasible at 3T, resulting in haemodynamic parameters comparable with pharmacological stress and allowing substantial improvement in temporal and spatial resolution compared to lower field strengths. There was no significant difference in high-energy cardiac phosphate metabolite concentrations in healthy volunteers at rest, during physiological leg exercise or during recovery. This protocol can now be applied to patients to provide new insights into pathophysiological changes in cardiac metabolism in response to exercise.
exercise; cardiac spectroscopy; cardiac energetics
049 NEGATIVE MULTIDETECTOR CORONARY CTA IN SYMPTOMATIC PATIENTS CONFERS A GOOD ONE-YEAR PROGNOSIS
R. van Lingen, N. Manghat, N. Kakani, C. Roobottom, G. Morgan-Hughes. Derriford Hospital, Plymouth, UK
Background: Symptomatic patients with an intermediate risk of coronary artery disease (CAD) have a good prognosis if they have a negative myocardial perfusion scan or stress echocardiogram. Recently multidetector CT coronary angiography (coronary CTA) has been proposed as an alternative strategy for investigating such patients and there are data to suggest that coronary CTA is accurate in comparison to invasive coronary angiography. As yet the prognostic value of a “negative” coronary CTA is not known.
Methods: A database search identified 355 symptomatic patients who had undergone coronary CTA as part of routine clinical care, to evaluate possible or known CAD, over a 44-month period up until October 2006. The coronary CTA scans were performed before September 2005 with 16-detector CT and 64-detector CT thereafter. Out of the 355 patients, 179 were identified who firstly had an intermediate risk of CAD following clinical assessment +/− uninterpretable or equivocal stress testing (exercise or perfusion) and secondly a coronary CTA deemed “negative” in view of the absence of a severe coronary artery stenosis (170 with normal coronary arteries/mild coronary artery stenosis and 9 with moderate coronary artery stenosis). These 179 patients represented the study group. The hospital database and patient records were reviewed to identify deaths, myocardial infarction (MI), unstable angina (UA) or revascularisation for all patients in this group.
Results: The 179 negative patients had a mean age of 56 years (27–83 years) and 102 (57%) were female. Mean duration of patient follow-up was 366 days (range 51–1113 days). At follow-up all 179 patients were alive (0% mortality) and no patients episodes of either MI or UA were identified. In total two revascularisation procedures had subsequently been performed (1.1%), both elective PCI procedures carried out on females from the group of 9 patients with one or more moderate coronary artery stenosis detected at the original coronary CTA.
Conclusion: Approximately half (50%) of the patients referred for CAD assessment using coronary CTA were symptomatic intermediate risk chest pain patients who were deemed to have a negative scan. The finding of a negative coronary CTA in this group of patients appears to confer a good prognosis, at mean follow-up of one year, with no deaths and no episodes of UA or MI. The need for subsequent elective PCI procedures in this patient cohort appears very low and confined to the patients with the largest plaque burden. The data suggest that the prognostic value of a negative coronary CTA may be similar to that conferred by a negative myocardial perfusion scan or stress echocardiogram. Larger studies with longer follow-up are needed to confirm this.
coronary CTA; negative; prognosis
050 LONG-TERM CORONARY ARTERY BYPASS GRAFT PATENCY AS ASSESSED BY MULTISLICE COMPUTED TOMOGRAPHY, QUALITY OF LIFE AND ADVERSE EVENTS IN PATIENTS RANDOMISED TO ON- AND OFF-PUMP SURGERY
D. Smith1, G. Murphy2, B. Reeves3, L. Culliford3, C. Rogers3, D. Coles4, A. Baumbach3, G. Angelini3. 1Gloucestershire Royal Hospital NHS Trust, Gloucester, UK; 2Bristol Royal Infirmary, Bristol, UK; 3Bristol Heart Institute, Bristol, UK; 4Barnstaple Hospital, Barnstaple, UK
Objectives: Off-pump coronary artery bypass grafting (OPCAB) has short-term benefits over conventional on-pump surgery (CABG-CPB). However, there is conflicting evidence about early graft patency and concern remains that long-term outcome may be compromised. Several recent studies have reported sensitivities and specificities of multislice computed coronary angiography of 100% in assessing bypass graft patency after comparison with the gold standard, invasive coronary angiography. We assessed graft patency, quality of life (QoL) and adverse event rates in two randomised trials of OPCAB vs CABG-CPB 6–7 years after surgery.
Abstract 050
Methods: Surviving participants were sent four QoL questionnaires (SF-36, Seattle Angina Questionnaire, EuroQol and Coronary Revascularisation Outcome Questionnaire) and were invited to have Multislice Computed Tomography Coronary Angiography (MSCT-CA). Exclusion criteria were known contrast allergy and serum creatinine >130 mmol/l. Consenting patients underwent the following scan protocol: if the heart rate was >65 bpm consideration was given to the administration of up to 100 mg of oral metoprolol tartrate. Patients were scanned using a Siemens Sensation 16 (Siemens, Forchheim, Germany) software Version 70A with retrospective electrocardiogram gated reconstruction. Each patient had a topogram, calcium scoring scan and angiogram, scanning caudocranially up to the level of the sternoclavicular joint in order to include any IMA origins with arms held above the head. The timing of this main injection (105 ml Iomeron at 4 ml/second) was determined by a test bolus scan. Scans were dual-reported by a cardiologist and a radiologist blinded to the surgical technique. Major adverse cardiac events were identified from the patient, GP and hospital notes.
Results: Of 401 original participants, 52 had died. Of the remaining 349, 298 (85.4%) returned questionnaires (149 OPCAB; 149 CABG-CPB); 216 agreed to have MSCT-CA though 17 were found to be ineligible leaving 199 (OPCABG 98 vs CABG-CPB 101). Patency rates were similar in both groups (table). Median length of follow-up for survival was 83 months. Scores on each QoL dimension were similar across groups and none of the differences between groups was significant (p>0.1 for all comparisons). Survival, and survival free from cardiac events and death, were similar in both groups (hazard ratios OPCAB vs CABG-CPB 1.25 (95% CI 0.72 to 2.17) p = 0.42 and 0.82 (95% CI 0.56 to 1.20) p = 0.30, respectively).
Conclusions: Six to seven years after surgery, graft patency rates, QoL and adverse event rates were similar in patients randomised to OPCAB and CABG-CPB.
off-pump coronary artery bypass surgery; multislice computed tomography; graft patency
051 TWO-YEAR FOLLOW-UP OF 410 PATIENTS PRESENTING TO A DISTRICT GENERAL HOSPITAL WITH CHEST PAIN AND A CT CORONARY CALCIUM SCORE OF ZERO
T. Keeble1, A. Hague1, S. Powles1, A. Thain1, E. Smith2, R. Prasad1, S. Mazhar1, T. Nageh1, P. Kelly1, A. Khokhar1. 1Southend Hospital, Southend, UK; 2London Chest Hospital, Bethnal Green, UK
Introduction: CT coronary calcium scoring (CTCCS) has been developed over the last few years as an independent risk factor for coronary heart disease, with even low coronary calcium scores doubling the risk of coronary events. Calcification in the coronary artery vessel walls is a very sensitive marker for the presence of atherosclerosis and shows moderate correlation between its extent and the likelihood of coronary obstruction. There is considerable controversy as to the ability of calcium scoring to detect early yet potentially prognostically important “soft plaques”.
Objective: To evaluate the event rates within a mean follow-up period of 2 years for 410 patients presenting to hospital with chest pain and a CTCCS of zero.
Methods: Southend Hospital commenced a CT calcium scoring programme using a GE 16 slice CT scanner in September 2003. 1100 CT coronary calcium scores were carried out between September 2003 and October 2005 to risk stratify patients presenting with chest pain and potential obstructive coronary disease. This retrospective observational study reports the 2-year mean follow-up of 410 patients with CTCCS of zero. Patients with a zero CTCCS were databased and their hospital electronic and paper records analysed to ascertain event rates, number of presentations to hospital, non-cardiac causes of presentation, and the number of patients who went on to have other ischaemic heart disease investigations.
Results: The mean age of this zero CTCCS group was 49 years (23–73 years) and 51% were male. Patients were followed up for a mean of 2 years (minimum 13 to maximum 37 months). Of the 410 patients with a zero CTCCS over the follow-up period, there were no deaths, and no troponin positive acute coronary syndromes. 38 patients re-presented to Hospital—30 with symptoms of chest pain, 8 with other medical complaints. The average age of those re-presenting with chest pain was 49 years (30–68 years). No patients had dynamic ECG changes, and none stayed more than 24 h in hospital. Nine patients had a confirmed upper GI diagnosis made, based on OGD examination. Seven patients had a diagnosis of, or were being treated for a psychological illness—mainly anxiety/depression. Within this group of 38 patients re-presenting, 3 went on to have a negative exercise test, 2 had a normal dobutmaine stress echocardiogram (DSE), 1 had a normal adenosine MIBI scan, and no patients progressed to coronary angiography.
Conclusion: In a cohort of 410 patients with a mean age of 49 years presenting to a district general hospital with chest pain, a CT coronary calcium score of zero confers an excellent short term prognosis with no deaths or troponin positive acute coronary syndromes within a mean 2-year follow-up period.
CT coronary calcium score; 2-year mean follow-up; prognosis
052 A POTENTIAL ROLE FOR OSTEOPROTEGERIN IN IDIOPATHIC PULMONARY ARTERIAL HYPERTENSION
A. Lawrie1, J. Suntharalingham2, M. Southwood2, S. Francis1, D. Crossman1, N. Morrell2, C. Newman1. 1University of Sheffield, Sheffield, UK; 2University of Cambridge, Cambridge, UK
Introduction: Pulmonary arterial hypertension (PAH) is characterised by the narrowing and occlusion of small pulmonary arteries driven by the proliferation and migration of pulmonary artery smooth muscle cell (PA-SMC). Mutations in the bone morphogenetic protein receptor 2 (BMP-R2), and a polymorphism in the serotonin transporter (SERT) genes, and inflammation have all been implicated with the pathogenesis of idiopathic PAH (IPH). Despite this information, we are still unaware of how these molecules and pathways interact to cause disease. Osteoprotegerin (OPG), a member of the TNF superfamily, is widely expressed and secreted by a variety of tissues including arteries and veins, as well as haematopoietic and immune cells. OPG has an emerging role in vascular biology, in particular in the calcification of atherosclerotic lesions. Interestingly from the context of PAH, BMPs, serotonin and IL-1 all modulate OPG expression in other cell types. We hypothesised that OPG expression and secretion is regulated by BMP-R2, SERT and inflammation, and that once secreted, OPG induces a pro-migratory and/or anti-apoptotic/pro-mitotic phenotype in PA-SMC, consistent with a role in the pathogenesis of PAH.
Methods: These studies used a combination of primary human PA-SMC, BMP-R2 siRNA, and stimulation with recombinant proteins. OPG gene expression was also measured in PA-SMC RNA isolated from IPH patients. Secreted OPG was measured by ELISA in both cell culture media and in IPH patient serum, and immunohistochemistry was performed on lung sections. Proliferation was assessed by tritiated thymidine and migration by a transwell chamber assay.
Results: BMP-R2 siRNA increased OPG secretion fivefold compared to control oligos (n = 4, p<0.05). Serotonin stimulated OPG release from human PA-SMC compared to 0.1% FCS in a SERT-dependent manner (n = 4, p<0.05) and IL-1 also increased OPG secretion (n = 4, p<0.05). Recombinant OPG (50 ng/ml) was pro-mitogenic (n = 4, p<0.05) and pro-migratory (n = 4, p<0.05) for PA-SMC in vitro. Analysis of microarray data performed on PA-SMC, isolated from either control or IPH patients with BMP-R2 mutations, demonstrated a twofold higher level of OPG gene expression in IPH patients compared to controls. Analysis of serum samples collected from IPH patients of mixed BMP-R2 genotype revealed a significantly elevated level of OPG compared to control subjects. Immunohistochemical analysis of human lung tissue samples showed a low level of OPG expression in sections of control lung, localised mainly in the perilumenal endothelium. In the IPH lung sections, stronger medial staining was observed within both concentric and plexiform lesions of remodelled pulmonary arteries.
Conclusion: These data suggest that OPG may be a central molecule in the pathogenesis of pulmonary hypertension and provide a common link to the different pathways associated with disease.
pulmonary hypertension; osteoprotegerin; VSMC
053 THE NOVEL PEPTIDE, APELIN, IS A VASODILATOR IN VIVO IN MAN
A. Japp1, V. Li1, N. Cruden2, A. Flapan3, D. Newby1. 1University of Edinburgh, Edinburgh, UK; 2Western General Hospital, Edinburgh, UK; 3Royal Infirmary of Edinburgh, Edinburgh, UK
Introduction: Apelin is the endogenous ligand for the orphan G-protein coupled APJ receptor. In preclinical models, apelin is a powerful vasodilator and the most potent inotrope studied to date. It increases cardiac output in normal and failing hearts without inducing left ventricular hypertrophy. This unique profile of cardiovascular effects suggests potential therapeutic applications, such as in patients with heart failure. To date, there have been no reports on the in vivo effects of apelin in man. The aim of this study was to determine the effects of apelin on vascular tone in human forearm resistance vessels using full length apelin-36 and (Pyr1)apelin-13, a naturally occurring, shorter C-terminal fragment with reportedly greater potency.
Methods: Forearm blood flow (FBF) was measured using venous occlusion plethysmography in 6 healthy male volunteers on 4 occasions during intrabrachial infusions of apelin-36 or (Pyr1)apelin-13 (0.1–30 nmol/min). On 2 of the 4 occasions (Protocol 1), doses were given as a continuous dose escalation followed by a 42 min saline washout. On the remaining 2 occasions (Protocol 2) each dose was followed by an 18 min infusion of saline. FBF in the infused and non-infused arm was compared using two-way ANOVA with repeated measures and Bonferroni post-tests.
Results: Both apelin-36 and (Pyr1)apelin-13 caused dose-dependent vasodilatation (p<0.001) with peak increases in FBF of 222% and 103% respectively. In both cases the effect was prolonged with vasodilatation still apparent 42 min after cessation of infusion. The response to (Pyr1)apelin-13 was greater than apelin-36 at lower doses (<3 nmol/min) peaking at 1 nmol/min before declining at higher doses (fig 1). In contrast the response to apelin-36 increased progressively, peaking at the maximum dose of 30 nmol/min (data not shown). With both peptides there was a small increase in FBF in the non-infused arm from 10 nmol/min (p<0.05) suggesting systemic spillover. In protocol 2 there was also a dose-dependent increase in forearm blood flow in the infused arm with both apelin-36 and (Pyr1)apelin-13 (p<0.001; fig 2). The response was greatest during peptide infusion and declined steadily during washout periods, although never returning to baseline. There were no significant changes in heart rate or blood pressure during infusion of either peptide.
Conclusions: Apelin causes sustained, dose-dependent vasodilatation in resistance vessels of the human forearm. The apelin-APJ system merits further detailed clinical investigation to characterise its effects on cardiovascular homeostasis and determine its therapeutic potential.
apelin; APJ receptor; forearm blood flow
054 NF-κB INHIBITION BY BLOCKADE OF IKK-2 AND MYD88 IN VEIN GRAFT SMOOTH MUSCLE CELLS REDUCES THE EXPRESSION OF KEY MEDIATORS OF INTIMAL HYPERPLASIA
J. Finch1, T. Navin2, S. Gregan2, B. Foxwell3, D. Haskard1, C. Monaco2, P. Hornick4. 1NHLI, Imperial College London, London, UK; 2Cytokine Biology of Vessels, Kennedy Institute of Rheumatology, Imperial College London, London, UK; 3Kennedy Institute of Rheumatology, Imperial College London, London, UK; 4Department of Cardiothoracic Surgery, Hammersmith Hospital, London, UK
Introduction: 100 years after its discovery, accelerated intimal hyperplasia (AIH) remains the leading cause of failure of invasive vascular interventions such as bypass grafting with saphenous vein. No successful preventative therapy currently exists for vein graft AIH, a condition which causes 40–50% of grafts to be occluded by 10 years. AIH leads to recurrent ischaemia and risk of death from myocardial infarction and necessitates revision surgery in 10% of patients. Inflammatory signalling is pivotal in AIH pathogenesis and mediators such as transcription factor NF-κB represent potential therapeutic targets. We hypothesise that genetic manipulation of specific upstream NF-κB signalling pathways in vein VSMCs in vitro will identify a leading therapeutic target to ameliorate AIH in vivo. We anticipate that this approach, as opposed to non-specific inhibition, will reduce deleterious effects on vascular cell viability.
Methods: A porcine jugular vein to carotid artery interposition model was used to generate vein graft AIH at varying durations up to 56 days. Diseased grafts and control veins were obtained at intervals for histological and immunoconfocal analysis and cell culture studies. Analysis of NF-κB activation in AIH lesions was carried out by confocal analysis of snap frozen grafts stained with immunofluorescent anti-p65 antibody. VSMCs were isolated from control and diseased vein segments and cultures established. Cells were infected with adenoviruses expressing mutated forms of the main kinases within the NF-κB pathway (IKK1 and 2) or toll-like receptor (TLR) adaptor molecules (such as the shared IL-1/TLR adaptor protein MyD88). Transfected cells were incubated with proinflammatory cytokines and TLR ligands. Expression of NF-κB-dependant AIH mediators such as cytokines, MMPs and tissue factor, were assessed with Q-PCR and ELISA.
Results: Immunoconfocal analysis confirmed NF-κB nuclear translocation within the endothelial cells and neointima of explanted vein grafts whereas minimal activation was seen in control vein segments. In vitro stimulation of vein graft VSMCs with IL-1 and ligands for TLR-2,-3 and-4 induced upregulation of IL-6 and MMP-3. For TLRs-3/-4 a significantly greater response was seen in diseased as opposed to control cells (TLR-3: 13.4-fold vs 5-fold, TLR-4: 5.4-fold vs 1.8-fold increase in IL-6) suggesting upregulation of these TLRs in the diseased state. Overexpression of mutated IKK-2 inhibited expression of IL-6 by 95%, MMP-3 by 80% and tissue factor by 50% (p.<0.05 vs control). Mutated MyD88 inhibited expression of IL-6 by 80% and MMP-3 by 90% (p.<0.05 vs control).
Conclusions: Activation of NF-κB was confirmed within vein graft ECs and neointimal VSMCs at the earliest stages of AIH development. In vitro inhibition of upstream NF-κB signalling in VSMCs with mutated IKK-2 or MyD88 significantly reduced the expression of AIH mediators highlighting promising targets for inhibition in vivo.
NF-κB; vein graft; intimal hyperplasia
055 HYPERGLYCAEMIA REDUCES ENDOTHELIAL PROGENITOR CELL ADHERENCE AND DIFFERENTIATION IN VITRO
J. Moore, A. Whittaker, M. Vasa, N. Samani. Department of Cardiovascular Sciences, University of Leicester, Leicester, UK
Introduction: Hyperglycaemia is a major risk factor for the development of atherosclerosis. Reduced numbers of endothelial progenitor cells (EPCs) have been associated with an increased risk of coronary artery disease. In the present study we compared the effects of glucose alone, insulin alone and the combination of insulin plus glucose on the ability of mononuclear cells to adhere and differentiate into EPCs in vitro.
Methods: Mononuclear cells (MNCs) were separated from peripheral blood of 15 healthy donors by Ficoll density gradient centrifugation. Isolated MNCs were suspended in endothelial basal medium supplemented with SingleQuots and 20% FCS and plated into fibronectin-coated 24-well plates. Cells were treated with either glucose (7,12, or 22 mmol/l), insulin (0.01,0.5, or 20 µg/ml) or glucose plus insulin (12 mmol/l glucose plus either 0.001 or 0.01 µg/ml insulin) and incubated for 7 days. Control wells received no treatment. Non-adherent cells were removed by thorough washing with PBS on days 3, 6 and 7. Adherent cells were provided with fresh media (containing the relevant treatment) on days 3 and 6. Adherent cells were stained with 1,1-dioctadecyl-3,3,3,3-tetramethylindocarbocyanine-labelled acetylated LDL and FITC-labelled Ulex europaeus agglutinin I and Ulex Agglutinin on day 7. Dual stained cells were judged to represent EPCs and counted in 5 high-powered fields (hpfs) per well.
Results: We found a significant reduction in EPC number (values expressed as mean cells per hpf per 106 plated mononuclear cells (SEM)) with increasing doses of glucose (7 mmol/l: 22.3 (6.4), p = NS; 12 mmol/l: 19.4 (4.9), p<0.001; 22 mmol/l: 14.9 (3.9), p<0.001) compared to control (24.7 (5.8)). Increasing doses of insulin led to a significant increase in EPC number even at low doses (0.01 µg/ml: 28.3 (7.2), p<0.001; 0.5µg/ml: 33.5 (6.7), p<0.001; 20 µg/ml: 35.7 (7.7), p<0.001) compared to control (19.8 (5.3)). The combination treatments showed no effect of insulin (0.001 µg/ml or 0.01 µg/ml) on the reduction in EPC numbers caused by 12 mmol/l glucose (glucose alone 14 (2.7), plus 0.001 µg/ml 13.4 (3), plus 0.01 µg/ml 13.7 (3.8)).
Conclusions: Our study shows that MNCs cultured in hyperglycaemic conditions exhibited impaired formation and adherence of EPCs. This effect was not reversed with the addition of insulin. Insulin treatment alone led to enhancement of EPC adherence and formation in vitro. Reduced formation and adherence of EPCs in vitro with hyperglycaemia may reflect poor endothelial repair in vivo, which in turn could contribute to the increased risk of atherosclerosis seen in diabetes mellitus.
endothelial progenitor cells; hyperglycaemia; insulin
056 DISCORDANT RESPONSE TO EXERCISE TRAINING IN NNOS KNOCKOUT MICE: DIFFERENTIAL ROLE OF NNOS ON EXERCISE PERFORMANCE VERSUS CARDIAC HYPERTROPHY
J. de Bono1, D. Adlam1, M. Zhang1, D. Paterson2, B. Casadei1, K. Channon1. 1Department of Cardiovascular Medicine, University of Oxford, Oxford, UK; 2Department of Physiology, Anatomy and Genetics, University of Oxford, Oxford, UK
Introduction: Neuronal nitric oxide synthase (nNOS) appears to play important roles in the regulation of both autonomic and myocardial function in physiological conditions and disease states. Multiple cardiovascular adaptations occur during exercise training. We aimed to investigate the importance of nNOS in exercise performance and in the cardiac response to exercise, using nNOS knockout mice.
Methods: 11-week-old male nNOS knockout (nNOS-KO) mice and their wild type (WT) littermates on a C57Bl/6 background were randomised to either sedentary and exercise groups. All mice were singly housed. The exercise group were place in cages with running wheel for 6 weeks. Exercise performance was quantified by continuous logging of individual wheel rotations and analysed using Spike 2 software to derive indices of running distance, modal running speed and duration of exercise bouts in each 24-h period.
Results: Male nNOS-KO mice ran at the same speeds as WT littermates (modal speed in trained animals: WT 3.0 +/− 0.2, nNOS-KO 3.1 +/− 0.1 km/h), but for considerably shorter periods each day, resulting in a significant reduction in running distance by 50–60% compared with WT mice (see fig (A)). In contrast to the impaired exercise performance of nNOS-KO mice, lack of the nNOS gene was associated with an enhanced myocardial response to exercise. After 6 weeks’ training mice were sacrificed and the left ventricular (LV) mass measured. There was no difference in body weight between nNOS-KO mice and WT littermates in either the sedentary of exercise trained groups. However, sedentary nNOS-KOS mice had significantly lighter hearts than their WT littermates. WT animals only showed a small (6%) non-significant increase in LV mass in response to exercise training (see fig (B)). In contrast, nNOS-KO mice developed substantial (17%) and highly significant LV hypertrophy following exercise training (LV mass: Sedentary nNOS-KO mice 108 (6) mg, Exercise nNOS-KO mice 126 (2) mg, p = 0.017), despite running less distance each day than WT littermates.
Conclusion: Targeted deletion of the neuronal nitric oxide synthase gene impairs voluntary running performance in mice, but despite reduced exercise performance leads to enhanced myocardial hypertrophy in response to exercise training. nNOS plays important and divergent roles in regulating exercise capacity and the cardiac response to exercise.
neuronal nitric oxide synthase; exercise; physiological hypertrophy
057 WHITE BLOOD CELL TELOMERE LENGTH IS ASSOCIATED WITH LEFT VENTRICULAR FUNCTION IN THE OLDEST OLD: THE NEWCASTLE 85+ STUDY
J. Collerton1, C. Martin-Ruiz1, M. Kenny2, K. Barrass1, T. von Zglinicki1, T. Kirkwood1, B. Keavney1. 1Newcastle University, Newcastle upon Tyne, UK; 2Freeman Hospital, Newcastle upon Tyne, UK
Aims: Heart failure is a condition increasingly prevalent at older ages; however, mechanisms by which the ageing process affects cardiac function are largely unknown. White blood cell telomere length is a biomarker of ageing that may be associated with a variety of diseases of late onset, but its relation with cardiac function has not previously been studied. We measured telomere length in peripheral blood mononuclear cells (PBMCs) and carried out echocardiography in a group of 85-year-old subjects recruited from the community as part of the Newcastle 85+ Study.
Methods and Results: Eighty nine subjects whose 85th birthday occurred in the year 2004 were recruited through local family practitioners. They were visited in their homes for clinical assessment and echocardiography, which was performed using a handheld device. Telomere length was measured by a real-time PCR method. High sensitivity CRP was measured using ELISA. Echocardiographic M-mode ejection fraction (EF) was strongly associated with telomere length (p = 0.006) in subjects without evidence of previous MI. In multivariate analyses, sex and telomere length were significant predictors of EF while current smoking, blood pressure, plasma hsCRP and use of cardiovascular medications were not. One standard deviation longer telomeres were associated with a 5% higher EF. Telomere length accounted for 12% of the observed variability in EF.
Conclusions: These data show influences of the ageing process on myocardial function in the oldest old, apparently independent of other specific disease processes. This may be of importance in the aetiology of heart failure in this age group.
heart failure; telomeres; ageing
058 A PROSPECTIVE, MULTICENTRE CLINICAL TRIAL TO EVALUATE THE BIOSTAR BIOABSORBABLE SEPTAL REPAIR IMPLANT FOR THE CLOSURE OF ATRIAL LEVEL SHUNTS (1-YEAR FOLLOW-UP)
M. Mullen1, D. Hildick-Smith2, J. De Giovanni3, C. Duke4, S. Hillis5, L. Morrison6, C. Jux7. 1Royal Brompton Hospital, London, UK; 2Royal Sussex Country Hospital, Brighton, UK; 3Children’s Hospital Birmingham, Birmingham, UK; 4Glenfield Road Hospital, Leicester, UK; 5Western Infirmary, Glasgow, UK; 6Cardiothoracic Centre, Liverpool, UK; 7Georg-August University, Goettingen, Germany
Background: The BioSTAR Septal Repair Implant is a novel heparin coated bioabsorbable device specifically designed for the closure of atrial level shunts. The device has an acellular collagen matrix, mounted on a low-profile alloy framework, which is gradually absorbed and replaced with host tissue. This study assessed, for the first time in man, the safety and effectiveness of the BioSTAR device in percutaneous closure of patent foramen ovale (PFO) and atrial septal defects (ASD).
Methods: We conducted a prospective, non-randomised, open-label, multicentre, clinical study in 57 patients with evidence of a clinically, or haemodynamically significant atrial level shunt. The defect had to be amenable to percutaneous closure with the BioSTAR Bioabsorbable Septal Repair Implant. All patients were subjected to clinical follow-up evaluations comprised of echocardiography assessments and serum assays.
Results: All devices were successfully deployed. In one patient with a large ASD the defect was not adequately closed and the device was withdrawn. There were no major procedural complications. Closure rates at 30 days and six months were 88.5% and 96.4%. One-year follow-up data will be available for presentation at the British Cardiac Society.
Conclusions: BioSTAR is the first bioabsorbable septal repair implant to provide biological closure of atrial septal defects. 90–95% of the implant is bioabsorbed and is replaced with patient’s native tissue. It appears to be a safe and effective implant providing edge-to-edge sealing with rapid complete closure.
1Royal Brompton Hospital, London, UK; 2Royal Sussex County Hospital, Brighton, UK; 3Children’s Hospital Birmingham, Birmingham, UK; 4Glenfield Road Hospital, Leicetser, UK; 5Western Infirmary, Glasgow, UK; 6Cardiothoracic Centre, Liverpool, Uk; 7Georg-August University, Goettingen, Germany
patent foramen ovale; bioabsorbable; congenital heart disease
059 A PROSPECTIVE, MULTICENTRE, RANDOMISED, DOUBLE BLIND, PLACEBO-CONTROLLED TRIAL TO EVALUATE THE EFFICACY OF PATENT FORAMEN OVALE CLOSURE WITH THE STARFLEX SEPTAL REPAIR IMPLANT TO PREVENT REFRACTORY MIGRAINE HEADACHES: THE MIST TRIAL
A. Dowson. King’s College Hospital, London, UK
Aim: Observational studies demonstrated that patent foramen ovale (PFO) closure in stroke and decompression sickness patients led to the improvement or resolution of migraine in 65–90% of patients. The MIST (Migraine Intervention with STARFlex Technology) Trial is the first trial to attempt to investigate these observations with a prospective, double blind, placebo-controlled design.
Materials and Methods: Patients with frequent migraine (and some aura) that was not controlled with two or more classes of prophylactic medications were recruited. Transthoracic contrast echocardiography was used to detect right-to-left shunts and to semiquantitatively assess their size. Patients with a large or medium size PFO were randomised to PFO closure with the STARFlex septal repair implant or to a sham procedure. Patients and their headache specialist remained blind to randomisation during an initial 180-day follow-up period. After unblinding, patients whose PFOs had been closed continued to be followed. Patients from the sham arm were offered PFO closure and those who chose to have the procedure were followed for one year.
Results: 432 patients were recruited and screened for shunts. 260 (60.2%) had a shunt, of which 163 (37.7% of total patients and 62.7% of those with shunts) had a large PFO. The mean diameter of the PFOs among the patient population was 9.21 (3.27) mm. 73 patients were randomised to the sham procedure and 74 to the closure procedure with STARFlex. Preliminary results announced in March 2006 demonstrated that 42% of patients who had their PFOs closed with STARFlex had a 50% reduction in migraine headache days compared to 23% in the control arm. Full data from the initial follow-up period (MIST I) and findings from subsequent follow-up of this patient population (MIST III) will be available for presentation at British Cardiac Society 2006.
Conclusion: Large right-to-left shunts (mostly PFOs) are 6 times more common in migraine with aura patients than in the general population. The average diameter of the PFO in this patient population is similar to that seen in patients with paradoxical embolism. Preliminary results from MIST I have successfully demonstrated that closure of PFO with STARFlex provides a significant treatment effect in some patients. Longer follow-up of this patient population (MIST III) and future trials (MIST II is currently recruiting in the US) will improve our understanding.
STARFlex; migraine with aura; patent foramen ovale
060 COREVALVE PERCUTANEOUS AORTIC VALVE REPLACEMENT: NORTH AMERICAN EXPERIENCE
C. Berry1, A. Asgar2, B. Marcheix2, Y. Lamarche2, A. Denault2, A. Basmadjian2, A. Ducharme2, J. Laborde2, R. Bonan2. 1University of Glasgow, Glasgow, UK; 2Montreal Heart Institute, Montreal, Canada
Introduction: Percutaneous aortic valve replacement (PAVR) is an emerging alternative to medical therapy for non-surgical patients with severe aortic stenosis (AS). We describe the North American PAVR experience with the CoreValve Revalving system which includes a self-expandable porcine bioprosthesis in a nitinol frame.
Methods: Inoperable patients with symptomatic, severe (area <0.6 cm2/m2) AS were enrolled. Exclusion criteria included severe peripheral vascular disease and major comorbidity (life expectancy <1 year). Aortic balloon valvuloplasty was performed first, then retrograde CoreValve PAVR with general anaesthesia and circulatory support.
Results: Ten women and 9 men (mean (SD) age 84 (6) years) gave informed consent. Two of these patients had non-permissive vascular access therefore 9 women and 8 men underwent PAVR. Their baseline characteristics included: mean AV area = 0.62 (0.14) cm2; mean AV gradient = 53 (20) mmHg; mean left ventricular ejection fraction (LVEF) = 45 (17) %; median (IQR) NYHA class was 3 (3–4); and median (interquartile range) logistic EuroScore = 29% (14–42%). One patient had a 70% stenosis of the mid-left anterior descending coronary artery and underwent percutaneous coronary intervention (PCI) combined with simultaneous PAVR. Two male patients needed left iliac artery balloon dilatation (7 mm balloon) to permit device advancement. The first 11 patients underwent PAVR with the 21 Fr Generation II system and the following 6 patients had the 18 Fr Generation III system. Ten patients had fem-fem cardiopulmonary bypass and the median (interquartile range) CPB duration was 30 (26–50) min. Seven patients had left heart support with a percutaneous assist device (median (IQR) duration was 39 (29–60) min). The post-PAVR aortic bioprosthetic valve area was >1.2 cm2 and paravalvular regurgitation was ⩽Grade 2 in all cases. Six patients (35%) died. One man experienced a fatal peri-procedural stroke 5 days post-PAVR. All other patients died following discharge from comorbidity-related problems, and autopsies confirmed satisfactory valve function. Five patients required permanent pacemaker implantation. Follow-up of survivors (n = 11 (65%); range 1–11 months) confirmed haemodynamic and functional improvements in all PAVR cases. Compared with pre-PAVR observations, the one month mean (SD) aortic valve area was 1.3 (0.4) cm2, the mean AV gradient was 19 (26) mmHg, the mean LVEF was 56 (11) %, and the median NYHA was 2 (2–3) (all p<0.001). The mean N-terminal brain natriuretic peptide conc fell from 7825 (9549) pg/ml pre-PAVR to 5420 (8462) pg/ml 1 month post-PAVR (p = 0.05). Five referred patients who were waiting for PAVR died during the study period.
Conclusions: CoreValve PAVR is feasible and may be performed with percutaneous circulatory support. PAVR may be combined with PCI and may need peripheral angioplasty. A multidisciplinary approach in this high-risk population is necessary to ensure optimal procedural outcomes.
aortic stenosis; valve replacement; percutaneous
061 INCIDENCE OF RADIAL ARTERY ANATOMICAL VARIATION IN PATIENTS UNDERGOING TRANSRADIAL CORONARY ANGIOGRAPHY AND INTERVENTION: INFLUENCE ON PROCEDURAL OUTCOME
T. Lo1, E. Fountzopoulos1, R. Butler1, S. Hetherington2, A. Zaman2, D. Perera3, J. Nolan1, D. Hildick-Smith3. 1University Hospital of North Staffordshire, Stoke-on-Trent, UK; 2Freeman Hospital, Newcastle upon Tyne, UK; 3Brighton and Sussex University Hospital, Brighton, UK
Introduction: The radial artery (RA) is increasingly used as a preferred access site for percutaneous coronary procedures. It has the advantages of minimal access site complications, immediate ambulation and better patient comfort post procedure but is associated with a longer learning curve. Variation in forearm vascular anatomy may have an adverse effect on procedure success, but there are currently limited data on the incidence of anatomical variations and their effects on transradial coronary procedures. This multicentre prospective study aims systematically to establish the incidence and significance of RA anomalous anatomy in patients undergoing transradial coronary procedures.
Methods: Retrograde radial arteriography using a short introducing sheath was performed in all patients presenting for a first-time radial procedure. Patient characteristics, procedural data, radial artery anomalous anatomy and local vascular complications were analysed.
Results: 612 consecutive patients were studied. Patients were predominantly male (68.1%) with a mean age of 67.4 (10.3) years. The overall incidence of RA anomalous variation was 13.4% (82 patients)—42 patients (6.9%) had a high-bifurcating radial origin, 13 patients (2.1%) had a radial loop and recurrent RA, 6 patients (1%) had a significant recurrent RA alone and 21 patients (3.4%) had other anomalies which included extreme radial tortuosity, radial calcification and a high ulnar origin. Overall transradial procedural success was 96.2%. Procedure failures were due to inability to cannulate the RA (3 patients, 0.5%), RA anomalies (12 patients, 2%) and tortuosity of subclavian artery/brachiocephalic artery (8 patients, 1.3%). When a radial loop was present, procedure failure was common (8 out of 12 patients). There were no major vascular complications and only 7 patients (1.1%) had minor vascular complications treated conservatively.
Conclusion: Anomalous RA anatomy is common and in the majority of cases does not affect the outcome of a transradial procedure. The commonest variation is high bifurcating radial origin. The presence of a radial loop is associated with frequent procedure failure. Retrograde radial arteriography before the intended transradial procedure helps to identify such anomalies and identify patients with potentially unfavourable RA anatomy. It should be incooperated into routine practice for transradial procedures.
radial artery; anatomical variation; transradial coronary procedures
062 PHYSIOLOGICAL ADAPTATION TO ACUTE RELIEF OF ADVERSE RIGHT VENTRICULAR LOADING CONDITIONS
L. Coats, S. Khambadone, G. Derrick, J. Deanfield, P. Bonhoeffer, A. Taylor. Great Ormond Street Hospital for Children, London, UK
Introduction: Percutaneous pulmonary valve insertion (PPVI) is a unique model to study the cardiac response to relief of right ventricular (RV) pressure and volume overload as it is not confounded by pulmonary regurgitation (PR) and cardiopulmonary bypass that respectively accompany bare stenting and surgical valve replacement.
Methods: We selected 18 subjects with RV outflow tract obstruction (regurgition <10% on magnetic resonance (MR) and gradient >50 mmHg on echo) and 16 with PR (regurgitation >25% and gradient <50 mmHg). Haemodynamics were recorded before and after PPVI. Assessment of NYHA class, exercise testing, tissue Doppler and MR were performed before and 3 months after PPVI.
Results: Patients with RV outflow tract obstruction improved NYHA (2 to 1, p<0.001) and exercise capacity (VO2:25.7 to 28.9 ml/kg/min, p = 0.002). RV systolic (72.8 to 47.3 mmHg, p = 0.001) and end diastolic pressure (11.3 to 9.6 mmHg, p = 0.04) fell. Pulmonary systolic pressure increased (21.4 to 25.7 mmHg, p<0.001). On tissue Doppler, systolic velocity improved (tricuspid:4.8 to 5.3 cm/s, p = 0.05; mitral 4.7 to 5.5 cm/s, p = 0.01). Isovolumic acceleration did not change. Regurgitation remained trivial (3.6 to 1.4%, p = 0.06). RV end diastolic (99.9 to 89.7 ml/m2, p = 0.001) and end systolic volume (54.2 to 40.6 ml/m2, p = 0.001) fell. Effective stroke volume (43.7 to 48.3 ml/m2, p = 0.06) and ejection fraction increased (48.0 to 56.8%, p = 0.01). Left ventricular (LV) end diastolic volume (72.5 to 77.4 ml/m2, p = 0.145), stroke volume (45.3 to 50.6 ml/m2, p = 0.02) and ejection fraction (62.6% to 65.8%, p = 0.03) rose. Patients with PR improved NYHA (2 to 1, p = 0.001) but not exercise capacity. RV systolic pressure fell (51.3 to 42.0 mmHg, p = 0.003) and pulmonary diastolic pressure rose (8.9 to 11.9 mmHg, p = 0.041). Systolic velocity and isovolumic acceleration did not change. Regurgitant fraction (40.7 to 4.1%, p<0.001) and RV end diastolic volume (115.4 to 98.9 ml/m2, p = 0.001) fell; end systolic volume did not change. Effective RV stroke volume increased (34.3 to 44.4 ml/m2, p<0.001) but ejection fraction did not change. LV end diastolic volume (66.6 to 73.4 ml/m2, p = 0.014), stroke volume (38.4 to 46.4 ml/m2, p = 0.001), ejection fraction (57.8 to 63.5%, p = 0.001) and cardiac output (4.3 to 4.8 ml/m2/min, p<0.001) increased.
Discussion: Improved effective stroke volume following PPVI suggests that pressure and volume overloaded RVs, in this setting, work on the decompensatory limb of the Starling curve. When abnormal loading conditions are relieved, the pressure-volume loop shifts leftwards to the compensatory limb. In the LV, end diastolic volume, stroke volume and ejection fraction improve implying a rightward shift on the compensatory limb of the Starling curve. Higher preload and restoration of better septal behaviour are the likely mechanisms. In those with PR, VO2max does not reflect the MR improvements. We conclude that pressure-overloaded myocardium has a contractile reserve that is recruitable with reduction in afterload, whereas the volume loaded RV does not.
physiology; right ventricle; percutaneous pulmonary valve implantation
063 EFFECTS OF GLYCERYL TRINITRATE TO LOWER CENTRAL ARTERIAL PRESSURE RELATE TO ARTERIAL VASODILATION RATHER THAN REDUCTION IN PRE-LOAD
M. Seddon, B. Liu, B. Jiang, P. Chowienczyk. Cardiovascular Division, King’s College School of Medicine at Guy’s, King’s College and St Thomas’ Hospitals, London, UK
Background: Glyceryl trinitrate (GTN) produces a characteristic change in the form of the arterial pulse wave with a reduction in augmentation index (AI) and reduces central systolic blood pressure (cSBP) to a greater extent than peripheral systolic blood pressure. These actions of GTN could be due to arterial vasodilation and/or a reduction in pre-load. To determine which of these mechanisms predominates, we compared effects of GTN on measures of central and peripheral blood pressure with those of lower body negative pressure (LBNP), which selectively reduces pre-load.
Methods: Ten healthy men (mean age 35 years) were studied. Subjects were placed in a LBNP chamber, and serial measurements were taken at baseline and at increasingly negative pressures (−10, −20 and −30 mmHg). At these levels of LBNP, cardiac filling pressure decreases with minimal change in arterial pressure, and change in preload can be assessed from the amplitude of the systolic (s) wave in the superior vena cava (SVC) doppler trace. Following return of haemodynamic measurements to baseline, subjects underwent repeat measurements during a cumulative dose intravenous infusion of GTN (10, 30 and 60 µg/min, each dose for 10 min). Brachial blood pressure was measured by a validated oscillometric method and transthoracic echocardiography performed to assess SVC flow, and to calculate stroke volume (SV) and cardiac output (CO). A SphygmoCor tonometry system was used to measure the radial pulse waveform and derive, via a validated transfer function, the aortic pressure waveform and hence cSBP and AI.
Results: LBNP (−30 mmHg) significantly reduced preload, with a decrease in the SVC s wave from 0.58 (0.04) to 0.37 (0.02) m/s (p<0.001), reduced SV from 86 (5.3) to 64 (5.1) ml (p<0.001) and CO from 5.2 (0.9) to 4.3 (0.87) l/min (p<0.005). Heart rate increased from 61 (2.3) to 67 (3.3) beats/min (p<0.01). There was no significant effect on peripheral mean arterial pressure (MAP), a small but significant change in cSBP from 101 (1.9) to 98 (2.0) mmHg (p<0.05), and no significant change in AI (50 (4.9) to 51 (6.4)%). Compared to LBNP (−30 mmHg), GTN (60 µg/min) similarly reduced preload (SVC s wave 0.55 (0.04) to 0.40 (0.02) m/s), SV (85 (6.0) to 75 (6.8) ml), CO (5.1 (0.86) to 4.6 (0.90) l/min) and increased heart rate (58 (2.2) to 65 (2.4) beats/min). However compared to LBNP, GTN produced a significantly greater reduction in MAP (85 (1.7) to 71 (2.1) mmHg; p<0.001 for comparison with change for LBNP), cSBP (102 (2.1) to 88 (2.3); p <0.005 compared to LBNP) and AI (55 (3.6) to 29 (2.4)%, p<0.005 compared to LBNP).
Conclusion: For a similar degree of pre-load reduction, GTN and LBNP have differential effects on AI and cSBP. This suggests that GTN reduces cSBP by arterial vasodilation and reduction in pressure waveform reflection rather than by reduction in pre-load.
GTN; blood pressure; preload
064 AUDIT OF RATE OF RECURRENCE OF ATRIAL FIBRILLATION FOLLOWING DC CARDIOVERSION
D. Sevant, A. Khokhar. Southend Hospital, Southend, UK
Introduction: Atrial fibrillation (AF) is an independent predictor of stroke, with an annual risk that is 5–6 times higher than in patients with sinus rhythm. When stroke occurs in association with AF, patients suffer substantial mortality, morbidity, disability and longer hospital stays compared with stroke patients without AF, (NICE, 2006). The benefits of thromboprophylaxis in patients with AF are well established and most guidelines recommend the use of warfarin for high-risk patients pre- and post-cardioversion. Cardioversion is performed as part of a rhythm control strategy and if successful restores sinus rhythm. Patients’ INR is required to be within therapeutic range for a minimum of 3 weeks before and 4 weeks after cardioversion to reduce the additional risk of thromboembolism due to cardioversion. ACC/AHA/ESC Guidelines 2006 for management of AF suggest discontinuation of warfarin 4 weeks after cardioversion if sinus rhythm is maintained. However, not all attempts at cardioversion are successful long term and at one year post-cardioversion approximately 50% of patients are back in atrial fibrillation (Lim et al 2004). There is growing evidence that warfarin should continue long term despite reversion to sinus rhythm.
Aim: Our practice has been to stop warfarin 6 weeks post-cardioversion for most patients remaining in sinus rhythm following successful chemical or DC cardioversion. With a known high recurrence rate of AF and growing support for all patients to remain on warfarin long term, it was proposed to audit our recurrence rates from our 2004 cohort of patients.
Method: In 2005 an audit was carried out of all patients who had been successfully cardioverted in 2004 and had remained in sinus rhythm at 6 weeks follow-up. One year after that follow-up they were all sent a request to have an ECG and asked to complete a questionnaire regarding current medications and symptoms.
Results: Sixty four patients were called for repeat ECG and 57 responded. Of these, 46% were in sinus rhythm at 1 year and 54% in AF. Of the patients in AF, only 5 were continuing to take warfarin, leaving the majority of patients off warfarin and exposed to significant stroke risk. 32 patients reported feeling better and 19 feeling “no worse”.
Conclusion: Those patients with AF not taking anticoagulation therapy were at increased risk of stroke. Results also confirm that patients are often not aware they have reverted to AF and require recommencement of anticoagulation.
Changes to Practice: Patients remain on warfarin longer post-cardioversion and the frequency of follow-up has been increased to 3 and 6 months and 1 year. This work further supports the AF management NICE recommendations, for rigorous follow-up post-cardioversion. Our audit is continuing to inform future practice.
cardioversion; atrial fibrillation; follow-up
065 CARDIAC REHABIILITATION AND PATIENT EDUCATION FOLLOWING PRIMARY PERCUTANEOUS CORONARY INTERVENTION
A. Thornley1, B. Kunadian1, A. Lister1, A. Turley1, A. Moffitt1, J. Close2, M. Cave2, J. Hall1, M. de Belder1. 1The James Cook University Hospital, Middlesbrough, UK; 2University Hospital of North Durham, Durham, UK
Background: Primary percutaneous coronary intervention (PPCI) has been shown to improve outcomes in terms of morbidity and mortality for patients presenting with acute ST elevation myocardial infarction (STEMI). There is also good evidence that selected patients who undergo Primary Angioplasty can be discharged at an earlier stage than those who receive thrombolysis. This has led to concerns that decreased hospital stays following PPCI may have a negative impact on patient education and subsequent involvement in cardiac rehabilitation programmes.
Aims: We investigated patient experience in two cohorts undergoing treatment for STEMI: the first underwent PPCI at a tertiary cardiothoracic centre and the second received thrombolysis at a district general hospital.
Methods: A written patient questionnaire was sent to patients more than 3 months after they presented with a STEMI to the two centres. The questionnaire consisted of 14 questions with a mix of free text responses and closed questions. Results were tabulated and the responses to closed questions were compared using the χ2 statistic. A p value of less than 0.05 was taken to be significant.
Results: Questionnaires were distributed to patients that underwent PPCI and thrombolysed patients. There were 118 response from the PPCI group and 52 from the thrombolysed group. There were no significant differences between the two groups in terms of patient recall of dietary advice (91/118 (77%) vs 44/52 (85%)), exercise advice (98/118 (83%) vs 47/52 (90%)), information about medications (112/118 (95%) vs 49/52 (94%)), advice about returning to work (19/46 (41%) vs 9/16 (56%)) or provision of an emergency helpline number (96/118 (81%) vs 47/52 (90%)). Patients that underwent PPCI were more likely to state that their condition and treatment was “understandably explained” than those that received thrombolysis (“definitely” or “to some extent” 114/118 (97%) vs 45/52 (87%), p = 0.03). There was no difference in patient reported rates of readmission between the two groups (24/118 (20%) vs 8/52 (15%), p = 0.17). Patient involvement in cardiac rehabilitation was no different with 80/118 (68%) and 32/59 (67%) reporting either current or past attendance at rehabilitation classes or that they were awaiting a place. Overall patient satisfaction was high with 114/118 (97%) and 51/52 (99%) rating their treatment as either good or excellent.
Conclusions: Patient involvement in cardiac rehabilitation following STEMI does not seem to be affected by the mode of reperfusion treatment received. Patient education is not impaired by the potential for shorter hospital stays associated with PPCI.
cardiac rehabilitation; patient education; primary PCI
066 CORONARY HEART DISEASE PATIENTS’ PERCEPTION OF THEIR SYMPTOMS AND SENSE OF CONTROL BEFORE HOSPITAL DISCHARGE PREDICTS THEIR QUALITY OF LIFE IN THE LONG TERM
M. Lau-Walker, M. Cowie. Imperial College, London, UK
Introduction: Recent intervention studies have attempted to address cardiac rehabilitation patients’ illness beliefs to improve care. However, these research findings are mainly limited to short-term behaviour changes such as return to work or attendance on rehabilitation programmes. Evidence available about what aspects of the patients’ illness beliefs would influence their long-term health outcomes in cardiac rehabilitation remains sparse. A more precise understanding of the relationship between specific illness beliefs that influence health status in the long term could provide clinicians with evidence to develop an effective individualised care approach and to promote quality of life.
Objective: To examine the association between coronary heart disease patients’ illness beliefs and their quality of life 3 years following hospital discharge.
Design: A cohort study of 300 patients who were admitted to hospital with a diagnosis of coronary heart disease; measuring their illness beliefs twice, before hospital discharge and nine months after discharge, using the Illness Perception Questionnaire. Patients’ demographics, illness characteristics and attendance at cardiac rehabilitation were also included in the multiple regression analyses.
Outcome measures: Quality of life was measured using the Health Survey SF36v2 questionnaire with eight domains and two summary scores (physical and mental health) 3 years after hospital discharge.
Results: Average age of enrolled patients was 65 years, 79% male, 50% acute myocardial infarction and 50% angina, 61% had no previous history of cardiac illness, 55% had index admission as emergency and 57% subsequently attended cardiac rehabilitation. Two multiple regression analyses were performed with each of the SF-36v2 physical and mental health summary scores as dependent variables. Analysis of baseline data showed that 43% of the variance in the physical health summary score at three years after index admission was accounted for by a perceived lower number of symptoms, belief that the illness was controllable, index admission as an emergency and no previous history of cardiac illness; 22% of the variance in the mental health summary score was accounted for by perceived lower number of symptoms and no previous history of cardiac illness. Analysis of data collected 9 months after discharge showed similar findings.
Conclusion: Coronary heart disease patients’ perception of their symptoms and disease “controllability” are significantly associated with their quality of life 3 years after admission to hospital. Interventions designed to address patients’ sense of control and symptom management are likely to improve their quality of life in the long term.
patient beliefs; cardiac rehabilitation; quality of life
067 NURSE-LED CHEST PAIN TRIAGE: MEETING THE CHALLENGE OF ACUTE CORONARY SYNDROMES
L. O’Neill, D. Elder, N. Dewhurst, P. Currie. Perth Royal Infirmary, Perth, UK
Background: Patients admitted to hospital with acute coronary syndromes (ACS) are at high risk of early death and poor outcome. This may be reduced by prompt therapeutic intervention. While the effectiveness of nurse-initiated thrombolysis for patients with ST elevation myocardial infarction (STEMI) has been established, data on nurse-led chest pain triage for other ACS patients are lacking.
Aim: To evaluate the existing standard of care of patients presenting with non-ST elevation myocardial infarction/unstable angina (NSTEMI/UA) at a district general hospital and to assess the impact of the introduction of nurse-led chest pain triage.
Methods: A 12-week, prospective case note review of 282 patients admitted with chest pain was undertaken to examine time to assessment or treatment and delivery of evidence-based ACS drug therapy. A new model of CCU-based, chest pain triage was then introduced which involved nurse-led assessment, risk stratification and treatment initiation. A further, 6-month retrospective case note audit of chest pain patients admitted through triage was carried out. NSTEMI/UA patients were deemed high risk with a TIMI score ⩾4 or TIMI score <4 but with dynamic ECG changes.
Results: The prospective audit identified 157 possible ACS cases (30 STEMI). 105 patients (5 STEMI) were admitted through the triage service operational on a weekday, 9 to 5 basis. Nurse-led triage brought about improvements in the time to initial assessment with 104 patients (99%) seen within 10 min of arrival, time to initial ECG (101/105 (96%) within 10 minutes vs 76/157 (48%), p<0.001*). The use of antiplatelet therapy and heparin for high-risk patients also improved. 80% (28/35) received clopidogrel compared to 45% (36/80) pre-triage (p<0.001*) and 97% (34/35) received heparin compared to 80% (36/80) pre-triage (p<0.001*). An unexpected reduction in the use of beta-blockers was noted (74% vs 93% (p<0.01*)). A non-significant trend for high-risk patients to be either managed by or referred to a cardiologist during triage was noted (18/35 (52%) compared to 27/80 (34%) p = NS*). No differences in the prescription of aspirin, clopidogrel, heparin or beta-blocker for low risk patients were noted.
Conclusion: A CCU based, nurse-led chest pain triage service may be an effective means of providing accurate and prompt assessment and improved clinical management of ACS patients presenting to district general hospitals.
*By χ2.
acute coronary syndromes; triage; nurse-led assessment
068 THE CARDIAC EDUCATIONAL NEEDS AND COMPETENCIES OF EMERGENCY CARE NURSES
H. Cox. University of the West of England, Bristol, UK
Introduction: The management of patients presenting with chest pain has changed dramatically. In order to achieve national standards, there has been an operational shift of focus from coronary care to the emergency department (ED). It is estimated approximately 700 000 patients per annum present to hospital with chest pain (Goodacre, 2005). Although the change in management has resulted in achieving set targets, the inappropriate discharge of patients is still an area for concern (Masoudi et al 2006). Nurses now need a more refined knowledge of cardiac conditions in order to triage this group of patients effectively (Arslanian-Engoren, 2005). Therefore this study aims to explore the cardiac educational needs of ED nurses.
Methods: Ethical approval was gained and a convenience sample of trained nursing staff from two local EDs were approached to participate. The methodology used taped focus group discussions, semistructured with a clinical scenario and the completion of a questionnaire based on the national clinical competencies. The tapes were transcribed and thematic analysis ensued.
Results: Five focus group interviews were conducted with 19 staff from a variety of clinical grades. Themes generated from the data reflected the national core professional, clinical and specialist competencies which provided an analytical framework
Core professional: Communication skills were viewed as vital, disparity arose within their current role remit regarding patient education in respect of time and knowledge. Education of clinical staff was on an ad hoc basis, predominately by the use of role modelling. Changing roles within the ED caused a degree of conflict.
Core clinical: ABC assessment, history taking skills and pharmacological knowledge were identified as essential; advanced assessment skills were considered not within their role remit. Education of staff in the triage of patients was not consistent. The Manchester triage tool was commonly used although its specific application for this client was questioned.
Core specialist: Although chest pain assessment and recording an ECG were viewed as essential the interpretation was not considered part of the nurses’ triage process.
Conclusion: Education was viewed as important with staff learning through in-house courses or role modelling. Concern was raised by senior staff to the level of standardisation or quality in adhering to this system. ECG interpretation and patient education were viewed by some as beyond their role remit. Chest pain assessment and differential diagnosis was considered although gender or ethnicity was not acknowledged. Patient education featured strongly to be not within the remit of the ED. The use of cardiac protocols was evident as was the ability of senior staff to manipulate their application. Therefore, based on an individual’s knowledge patients’ care and management thereafter could differ. Changing roles within the ED continues to cause concern.
chest pain assessment; emergency care; educational needs
069 CARDIAC ARRHYTHMIAS IN WOMEN WITH PALPITATIONS OF PREGNANCY ASSOCIATED WITH SYMPTOMS
A. Dhawan, J. Singh, P. Lewis. Stepping Hill Hospital, Stockport, UK
Introduction: Palpitations are one of the most common reasons for cardiac consultations during pregnancy and are generally attributed to benign cardiac arrhythmias of pregnancy. The commonest complaint in these women is an awareness of fast heartbeat without any associated symptoms. However there is a small proportion of pregnant women in whom palpitations are associated with significant symptoms such as chest tightness, sweaty, dizzy, syncope, sob, faint, and light-headedness. We compared symptomatic palpitations with asymptomatic palpitations.
Methods: We studied 180 pregnant women referred for further assessment of palpitations during pregnancy. Of these, 118 women had associated symptoms and 62 were asymptomatic. Both groups had no evidence of any prior known structural abnormalities of the heart. All women were extensively investigated for potential underlying causes of palpitations. All had detailed history, examination, baseline blood tests including thyroid function test, 12-lead electrocardiogram, echocardiogram, holter monitor, and regular follow-ups.
Results: Women with symptoms were older in age (33.1 (4.2) vs 30.1 (6.0), p = 0.005) and had significantly higher incidence of anaemia (p = 0.014). Women with symptoms were more likely to have a significant cardiac arrhythmia noted on Holter recording, (22/118 vs 2/62, p = 0.008). Using a multivariate binary logistic model including age, symptoms and presence of anaemia; only age (OR 1.14, 95% CI 1.03–1.27, p = 0.011) and symptoms (OR 0.022, 95% CI 1.30–26.3, p = 0.022) were significant independent contributors to the final diagnosis.
Conclusion: This study shows that not all palpitations of pregnancy are due to benign cardiac arrhythmias and that the presence of symptoms is associated with a higher incidence of significant cardiac arrhythmias. Anaemia significantly contributes towards symptoms but not towards final diagnosis.
palpitations; pregnancy; arrhythmias
070 IMPROVING PROGNOSIS IN HEART FAILURE: TRENDS IN INCIDENT HOSPITALISATION FOR HEART FAILURE AND SUBSEQUENT SURVIVAL BETWEEN 1986 AND 2003
P. Jhund1, K. MacIntyre1, J. Bishop2, A. Redpath2, J. Chalmers2, S. Capewell3, J. McMurray1. 1University of Glasgow, Glasgow, UK; 2ISD Scotland, Edinburgh, UK; 3University of Liverpool, Liverpool, UK
Introduction: The secondary prevention of cardiovascular diseases and treatment for heart failure (HF) has progressed markedly over the past two decades. Whether this progress has translated into improvements in the incidence of hospitalisations with a first episode of HF, and survival after discharge, is unknown in the UK at a population level.
Methods: Using the Scottish Linked Morbidity Record Database we identified all patients with a first episode of HF hospitalised between 1986 and 2003. They were followed to the end of 2005. We used multivariable modelling at 30 days (logistic regression), 1 and 5 years (Cox proportional hazards) to examine factors affecting prognosis in men and women and to determine trends over time after adjusting for age, comorbidities and socioeconomic deprivation.
Results: Between 1986 and 2003 116 556 individuals (55 173 men and 61 383 women) were discharged with a first (incident) admission for HF. From 1986 to 2003 the age standardised rate of incident hospitalisation for HF (per 10 000 inhabitants) fell from 12.4 (95% CI 11.9–12.9) to 10.5 (10.1–10.9) in men. In women the rate fell from 12.8 (12.3–13.2) to 10.1 (9.7–10.5). From 1986 to 2003 median survival following discharge increased from 1.23 years (1.08–1.39) to ⩾2.9 years in men and from 1.22 years (1.1–1.35) to 1.74 years (1.56–1.93) in women. Mean age at death in men also increased, from 73.9 years (73.5–74.3) to 77.3 years (76.8–77.8) and in women, from 79.1 years (78.7–79.5) to 81.4 years (80.9–81.9). The odds of death at 30 days, following discharge from an incident hospitalisation in 2003 (vs an incident admission in 1986), was 0.59 (0.45–0.63) in men and in women, 0.77(0.67–0.88), after adjustment for other prognostic variables. The adjusted hazard of death at 1 year following discharge from an incident hospitalisation for HF in 2003 (vs 1986) was 0.66 (0.57–0.68) in men and 0.77 (0.71–0.84) in women. The adjusted hazard of death at 5 years in 1999 (vs 1986) was 0.71 (0.67–0.75) in men and 0.78 (0.74–0.83) in women.
Conclusion: The rate of incident hospitalisation for HF fell between 1986 and 2003. Survival following hospitalisation improved in men and women at 30 days, 1 year and 5 years. These findings would suggest that improvements in the prevention and treatment of HF have had an effect at a population level. However, despite these advances, short- and long-term prognosis remains poor in HF.
heart failure; epidemiology; survival
071 MULTIMODEL DIAGNOSTIC TESTS TO ASSESS HEART FAILURE USING ECG, CHEST X RAY AND ECHOCARDIOGRAM IN PATIENTS WITH SUSPECTED HEART FAILURE
N. Khan1, K. Goode1, A. Rigby1, A. Torabi1, A. Clark1, N. Freemantle2, K. Swedberg3, M. Komajda4, F. Follath5, J. Cleland1. 1University of Hull, Hull, UK; 2University of Birmingham, Birmingham, UK; 3Department of Medicine Sahlgrenska University Hospital, Göteborg, Sweden; 4CHU Pitié-Salpetrière, Paris, France; 5Department of Internal Medicine University Hospital, Zurich, Switzerland
Background: Heart failure (HF) is a complex clinical syndrome with high morbidity and mortality. Diagnosis of HF depends on clinical judgement and diagnostic tests. As the diagnosis of HF has important implications in terms of management and prognosis it is essential to make a correct diagnosis.
Aim: To build a multimodal diagnostic criteria using ECG and chest x ray (CXR) to predict echocardiographic findings in patients with suspected HF and to find out whether they could reliably differentiate between patients with and without major structural heart disease (MSHD) or major left ventricular systolic dysfunction (MLVSD).
Method: We used the data from The EuroHeart Failure survey that enrolled patients with a known or suspected diagnosis of HF at discharge from hospital in 2000/1. Detailed clinical information and a 12-lead ECG were available in 9315 patients (87%) of whom 5934 (64%) also had an assessment of cardiac function mainly by echocardiography. Our principal data set comprised 5476 patients who have complete record of clinical characteristics, LV function assessment, ECG and CXR.
Results: Median age was 69 (61–77) years. 3196 (58%) were women. 46% women and 27% men were aged >75 years. Median NT-proBNP was 968 pg/ml Of the 5934 patients, MLVSD was present in 2951 (54%) and MSHD in 3832 (70%) of patients. 457 (8%) of patients had normal echocardiogram. Median (IQR) LVEF was 40 (30–55) %. Both ECG and CXR were normal in only 33 (<1%) and both abnormal in 4006 (73%) of patients. ECG, echo and CXR all were normal in 14 (0.3%) of patients. 4687 (86%) ECGs showed major and 721 showed minor abnormalities. Only 68 ECGs (<2%) were normal, 65 (96%) of these patients had no major LVSD. 14 of 3832 (0.4%) patients with MSHD had no major ECG abnormality compared to 54 of 1644 (3%) patients without MSHD. On logistic regression analysis, after adjusting for age and sex, ECG variables independently associated with MLVSD were QRS duration >120 msec, pathological Q-waves, the overall severity of ECG abnormalities, severity of T-wave abnormalities, S in V1 and R in V5-6 >35 mm and LBBB. Patients with QRS width ⩾120 msec or anterior pathological Q-waves had a probability >80% of MSHD and >70% of MLVSD. Patients with AF had a probability >70% of MSHD but <50% of MLVSD. CXR reports showed either cardiomegaly or pulmonary congestion or both in 4041 (74%) patients. 819 of 3832 (21%) patients with MSHD had neither cardiomegaly nor pulmonary congestion compared to 616 of 1644 (37%) patients without MSHD. The negative predictive value of ECG for excluding MLVSD was 96% compared to only 54% for CXR. The positive predictive value of either ECG or CXR was 58% and both ECG and CXR was 75%.
Conclusions: A normal ECG is uncommon in patients with MSHD but few patients with suspected HF have a normal ECG. The CXR appears to have little value for the diagnosis or exclusion of MSHD but may be of value to exclude pulmonary pathology.
diagnosis; ECG, CXR; heart failure
072 INCIDENT ATRIAL FIBRILLATION AND NEW HEART FAILURE: THE CHICKEN OR THE EGG? INSIGHTS FROM THE IMPERIAL COLLEGE NEW AF STUDY
J. Martins1, K. Fox1, D. Wood1, D. Lefroy1, T. Collier2, N. Peters1. 1Imperial College, London, UK; 2London School of Hygiene & Tropical Medicine, London, UK
Background and Aim: Atrial fibrillation (AF) and heart failure (HF) are intricately related. AF can result in decompensated HF through a number of mechanisms including loss of atrial transport and a rapid ventricular rate. Conversely, HF may predispose to AF due to increased atrial filling pressures, atrial fibrosis and regional conduction abnormalities. Thus, for patients with a first presentation of both these pathologies, it is a case of “the chicken or the egg?” We studied patients with first-detected AF who also presented with a first diagnosis of HF in the Imperial College New AF Study to try and answer this question.
Methods: All patients with a first diagnosis of AF presenting to a Rapid Access Arrhythmia Clinic at Charing Cross Hospital were recruited prospectively into this study. Each patient underwent a full clinical assessment and had a CXR, serum analysis and echocardiography on the day of assessment. These data were reviewed by a panel of three cardiologists who confirmed the diagnosis of AF, attributed aetiological associations and determined whether there were functional and structural cardiac abnormalities on echocardiography.
Results: Over a 26-month period, 203 new cases of AF were detected. The median (IQR) age was 74 years (63,80) and 54% were male. A past history of hypertension was present in 74 (36%) and CHD in 20 (10%). Only 1 patient (0.5%) had a past history of HF. Despite this, 33 patients (16%) had a new clinical diagnosis of concomitant HF at first presentation. These patients were significantly older than the remaining 170 without HF (mean (SD) age 76 years (10) vs 68 years (15), p = 0.002), and a greater proportion were women, 64% (21) vs 42% (72), p = 0.025. There were no significant differences in their aetiologies or presenting blood pressure, but patients with HF had a higher heart rate (HR) (mean (SD) = 111 (24) bpm vs 94 (26) bpm, p = 0.001), and 55% of patients with HF presented with a rate >120 bpm compared with 23% without HF, p<0.001. Almost All patients with HF (31/33, 94%) had sustained AF compared with 90 (53%) without HF, p<0.001. On echocardiography, there was a higher prevalence of left ventricular hypertrophy, 36% (12) vs 14% (23), p = 0.002, and patients with HF had larger mean (SD) left atrial diameters, 44.7 mm (6.6) vs 41.2 mm (9.2), p = 0.046. However the mean (SD) ejection fraction was similar and mostly preserved, 52% (15) vs 57% (14), p = 0.08.
Conclusion: Altogether, these data suggest that in this community setting AF precedes and is the cause of HF. The principal mechanisms for the development of HF in these patients with a first presentation of AF are prolonged, sustained rapid and irregular ventricular activity in patients with older and stiffer ventricles. These findings emphasise the importance of early diagnosis and adequate ventricular rate control in patients with new AF, to potentially reduce the incidence of tachycardia-mediated cardiomyopathy.
atrial fibrillation; heart failure; epidemiology
073 VERY HIGH PREVALENCE OF SLEEP APNOEA SYMPTOMS IN PATIENTS WHO HAVE UNDERGONE ELECTIVE ELECTRICAL CARDIOVERSION FOR ATRIAL FIBRILLATION
F. Haddadin1, D. Swamydass1, S. Thomas1, G. Rees1, P. Avery1, K. Lewis2. 1Carmarthenshire NHS Trust, Swansea, UK; 2Swansea School of Medicine and Carmarthenshire NHS Trust, Swansea, UK
Introduction: Obstructive sleep apnoea (OSA) affects up to 4% of middle-aged adults1 and is associated with cardiovascular disease. In a large group of American patients, the prevalence of OSA (on formal sleep study) was much higher in those with atrial fibrillation (AF) than in other patients attending a cardiology clinic, matched for age, gender and weight.2 OSA is increasingly associated with arrhythmias independently of obesity and other comorbidity but its prevalence in UK populations with arrhythmias has not been reported. Recurrent nocturnal hypoxia from undiagnosed OSA may be an independent risk factor for AF and even a modifiable risk factor for relapsed AF following successful cardioversion (DC). We used a validated tool—the Berlin Sleep Questionnaire.3 to estimate the prevalence of OSA in UK patients who had undergone DC cardioversion for AF. In a subgroup analysis, we also compared the prevalence of OSA symptoms in those who had relapsed back into AF following successful DC, versus those who remained in sinus rhythm.
Abstract 073
Methods: Cross-sectional, observational study with LREC approval. The Berlin Qnr was mailed to all 180, still living, patients who had undergone elective DC in a UK District General Hospital, between the years 2000 and 2005. None had known OSA. Possible confounders on AF were noted. Failed DC was defined as being back in AF at 3 months on cardiology review, the need for repeat DC up to the end of 2005 (ie at least 6 months after last DC included) or any documentation of being in AF in the hospital notes, post DC.
Results: 52% (n = 94) responded. Non-responders were similar (p = NS) in age, gender, comorbidity and duration of AF, but were less heavy at baseline (p = 0.06). 51% (48/94) of responders had a Berlin Score of “medium to high risk” with 18% scoring as “high risk” of having OSA. The table compares Berlin scores in the responders according to whether their DC was successful. They were otherwise matched for confounders for AF (age, gender, smoking status, weight, blood pressure, duration of AF, presence of valvular heart disease, left atrial size, DC energy required).
Conclusions: Many people receiving elective DC for AF have symptoms of OSA. At least 27% (48/180)—and probably more if you consider the non-responders—scored “medium to high risk” and so fulfilled the Berlin Sleep Qnr criteria for sleep studies. This compares with a background population estimate of only 4–6%. However, the risk of OSA was not greater in those with AF who have failed DC, compared with those who remain in sinus rhythm. A prospective study, objectively screening people for OSA before managing AF, then an intervention trial looking at the effect of OSA treatment on success rates in cardioverting AF would help establish causal links.
sleep; apnoea; atrial fibrillation
1
2
3
074 PREVALENCE OF DEPRESSION AND ANXIETY AMONG PATIENTS WITH ATRIAL FIBRILLATION: EFFECTS ON 6-MONTH QUALITY OF LIFE
G. Thrall1, D. Lane1, D. Carroll2, G. Lip1. 1University Department of Medicine, City Hospital, Birmingham, UK; 2University of Birmingham, Birmingham, UK
Introduction: Psychological variables, such as depression and anxiety, have been implicated in the aetiology and progression of coronary heart disease. However, there is a paucity of data on the prevalence and persistence of symptoms of depression and anxiety, and their impact on quality of life in patients with atrial fibrillation (AF).
Abstract 074
Objective: To examine the prevalence and persistence of depression and anxiety in patients with AF and the effect of such symptoms on future quality of life.
Methods: The Beck Depression Inventory (BDI) and the State-Trait-Anxiety Inventory (STAI) were completed by 101 patients with AF (62 males; mean (SD) age 66.3 (11.0) years), compared to 97 hypertensive patients in sinus rhythm (64 males; mean (SD) age 68.0 (7.2) years; as “disease controls”) at baseline and 6 months. Quality of life was ascertained at both time points using the Dartmouth Cooperative Information Project (COOP) charts.
Results: Among AF patients at baseline, symptoms of depression, and state and trait anxiety prevailed in 38%, 28% and 38%, respectively. The analogous figures for hypertensive patients were 30%, 23% and 22%, respectively. AF patients displayed significantly higher levels of trait anxiety (p<0.05), with no significant differences in baseline depression or state anxiety between AF patients and “disease controls”. Symptoms of depression and state anxiety persisted at 6 months in 36.8% and 33.3%, respectively. Multiple regression analysis revealed that baseline depression score provideed the best independent prediction of quality of life at 6 months (see table).
Conclusions: Approximately one third of AF patients experience elevated levels of depression and anxiety, which persist at 6 months. Baseline symptoms of depression were the strongest independent predictor of future quality of life in AF patients.
atrial fibrillation; depression; quality of life
075 THE ROLE OF MODERATE ALCOHOL INTAKE IN FIRST DETECTED ATRIAL FIBRILLATION: THE IMPERIAL COLLEGE NEW AF STUDY
J. Martins1, K. Fox1, D. Wood1, D. Lefroy1, T. Collier2, N. Peters1. 1Imperial College, London, UK; 2London School of Hygiene & Tropical Medicine, London, UK
Background and Aim: Although a strong causal relation with paroxysmal atrial fibrillation (AF) and binge drinking has been reported, the evidence for an association between long-term alcohol consumption and risk of AF is inconsistent. Two studies of incident AF have observed an inverse relation with alcohol intake, while three others, including the Framingham study, have reported a significant correlation but only at higher levels of consumption (>32 units/week). The relation of alcohol use and incident AF was explored in the prospective Imperial College study of first-detected AF.
Methods: All patients presenting to a Rapid Access Arrhythmia Clinic at Charing Cross Hospital, London with symptoms of a new cardiac arrhythmia were asked about their weekly alcohol consumption. This was further categorised into teetotal, moderate consumption (1–14 units/week (u/wk) for females, 1–21 u/wk for males) and excessive consumption (anything greater than moderate). Patients with electrocardiographically confirmed AF were compared to all other patients presenting to the RAAC without AF.
Results: During a 26-month period 203 patients with first-detected AF and 781 patients without AF were assessed in the RAAC. Data on alcohol consumption were recorded in 983/984 patients (99.9%). Moderate consumption was equal in both groups (48%). However, the prevalence of excessive drinking was considerably higher in the AF cohort, 27% (55/203) vs 17% (131/781), p<0.001. The mean (SD) and median (IQR) alcohol consumption was also greater in the AF cohort: 16 (21) u/wk and 6 (0–22) u/wk vs 10 (16) u/wk and 4 (0–14) u/wk, p<0.001. On univariable logistic regression analysis, as the level of consumption increased beyond the recommended limits, so did the probability of AF, OR 2.4, 95% CI 1.3–4.4, p = 0.004 for consumption >30 u/wk rising to OR 3.5, 95% CI 1.5–8.5, p = 0.004 for consumption >60 u/wk. On multivariable analysis, with each increasing unit of alcohol the probability of AF rose by 2%, 95% CI 0.7–3%, p = 0.002. This small incremental risk did not lead to an overall increased likelihood of developing AF in patients with moderate consumption compared to teetotallers. However, in contrast to other reports, this study found that any alcohol consumption in excess of the recommended weekly allowance of 14 units for women and 21 units for men was an important independent predictor of new AF, OR 2.8, 95% CI 1.4–5.6, p = 0.003.
Conclusion: The implication of these results for the population burden of AF may be substantial, because alcohol excess was prevalent in 19% of the population assessed in the RAAC. This behaviour is potentially modifiable and thus even a small decrease in the prevalence of excess alcohol consumption could lead to a large reduction in the incidence of this arrhythmia.
atrial fibrillation; alcohol; epidemiology
076 THE EFFECT OF OBSTRUCTIVE SLEEP APNOEA ON LEFT ATRIAL AND LEFT VENTRICULAR STRUCTURE
S. Kesavan, R. Green, R. Mansfield. Royal United Hospital Bath NHS Trust, Bath, UK
Introduction: Obstructive sleep apnoea is associated with an increased cardiovascular morbidity and mortality due to the occurrence of heart failure and cardiac arrhythmias. But there is a paucity of literature concerning the effect of OSA on left atrial and left ventricular structure before the occurrence of heart failure and arrhythmias. Identification of the OSA-dependent and OSA-independent factors in the cardiovascular pathophysiology of obesity may hold clinical and therapeutic promise.
Methods: Ninety patients were recruited for the study. All patients were in sinus rhythm and underwent transthoracic echocardiography. Patients with heart failure, atrial fibrillation, cerebrovascular accident, valvular heart disease, ischaemic heart disease and hyperthyroidism were excluded from the study. The control group included 45 obese patients with no evidence of OSA. The study group involved 45 patients with obesity and OSA. Both groups were age, gender, blood pressure and body mass index matched. The diagnosis of OSA was established by polysomnography. The study group included 32 male and 13 female patients with a mean age of 54 years. Body mass index ranged from 30–50 (mean = 35).
Results: Subjects with obesity and OSA demonstrated an increase in the left atrial size (>4.2 cms, p<0.001) and increased left ventricular end systolic (>3.75 cm, p<0.001) and end diastolic dimensions (5.4 cm, p = 0.005). Hypertrophy of the interventricular septum (>1.1 cm, p = 0.004) and posterior wall (>1.1 cm, p<0.001) of the left ventricle were also noted.
Conclusion: OSA causes an increase in the left atrial and left ventricular dimensions and is a significant independent predictor of left atrial dilatation and left ventricular hypertrophy. This is due to an increased afterload and transmyocardial wall stress associated with the direct effect of recurrent apnoeic episodes during a prolonged period of time. The adrenergic system is activated in OSA which may contribute to myocardial hypertrophy, ventricular dysfunction and the genesis of atrial/ventricular arrhythmias. The degree of severity of sleep disturbance has been shown to be directly related to the severity of the arrhythmias. The coinciding epidemics of obesity and atrial fibrillation underscore the clinical importance of these results.
obstructive sleep apnoea; obesity; arrhythmias
077 PREVALENCE OF HYPERTROPHIC CARDIOMYOPATHY IN ELITE ATHLETES
S. Basavarajaiah1, M. Wilson2, L. Carby2, A. Shah1, S. Sharma1. 1King’s College Hospital, London, UK; 2University Hospital Lewisham, London, UK
Background: Hypertrophic cardiomyopathy is associated with exercise related sudden death in young athletes. The prevalence of hypertrophic cardiomyopathy (HCM) in the general population, as determined by echocardiographic studies in the US, Japan, and China ranges from 0.16 to 0.29%. The prevalence of HCM in individuals participating in regular sport, based upon the Italian screening programme is approximately 1 in 1600. The exact prevalence of HCM in highly trained British athletes is unknown and has important implications with regards to a potential future national screening programme.
Abstract 077
Methods: Between 1996 and 2006, 3200 asymptomatic and normotensive elite athletes (75% males) aged between 14–35 years (mean 20.5 (5.80)) and a mean body surface area of 1.86 (0.16) m2 (range 1.36–2.29) participating in 14 sporting disciplines underwent 12-lead ECG and 2D-echocardiography. No athlete had a family history of HCM or SCD. Left ventricular (LV) dimensions, left atrial diameter and indices of diastolic functions were measured using conventional methods.
Results: Of the 3200 athletes, 33 (1.0%) had maximal left ventricular wall thickness (LVWTd) >12 mm (mean 13.60 (0.89), range:13–16). All 33 athletes were males. The mean left ventricular internal cavity dimension and left atrial diameter in the 33 athletes were 58.5 (5.14) mm and 32 (4.8) mm respectively. Indices of diastolic function were normal. Only 3 athletes (0.09%) had a non-dilated LV cavity and bizarre ECG changes that could have been consistent with the diagnosis of HCM. Their echocardiographic measurements are shown in the table. Only 1 of the 3 athletes could be persuaded to detrain for 3 months, which resulted in regression of left ventricular hypertrophy and normalisation of 12-lead ECG changes that were seen before. The other 2 athletes did not have any other phenotypic features of HCM on exercise stress testing with gas exchange or 48-h Holter monitoring.
Conclusion: Although 1% of elite male athletes develop left ventricular hypertrophy >12 mm and in the range compatible with the diagnosis of morphologically mild HCM, most (91%) have a dilated LV cavity indicating physiological LVH. In this study only 3 athletes had echocardiographic findings consistent with HCM but further investigations in all 3 failed to support the diagnosis. These results indicate that the prevalence of HCM in highly trained athletes is extremely rare. The augmentation of stroke volume required to generate large cardiac output during exercise probably selects out most individuals with HCM. Our findings question the validity of previous data which propose that HCM is the commonest cause of exercise-related death in young athletes.
hypertrophic cardiomyopathy; elite athletes; British
078 PREVALENCE OF CARCINOID HEART DISEASE IN THE MODERN ERA
S. Bhattacharyya1, C. Toumpanakis2, M. Caplin2, J. Davar1. 1Department of Cardiology, Royal Free Hospital, London, UK; 2Neuroendocrine Tumour Unit, Royal Free Hospital, London, UK
Background: Carcinoid heart disease (CHD), classically characterised by thickened, fixed, retracted and non-coapting valve leaflets associated with severe valvular regurgitation or stenosis, has been reported in up to 70% of all patients with carcinoid tumours. Development and progression is thought to be related to production of serotonin and tachykinins by the tumour. The last decade has resulted in the development of new therapeutic agents and treatment modalities for carcinoid syndrome including somatostatin analogues, interferon, radionuclide therapy and chemoembolisation designed to attenuate and cause tumour regression. Reduction of tumour load reduces the production of tumour metabolites and may thereby alter the development of CHD. We aimed to establish the prevalence of carcinoid heart disease in the setting of modern treatment regimens.
Methods: 100 patients with mid gut carcinoid tumours were screened for CHD by transthoracic echocardiography. CHD was defined as was defined as thickened valve leaflets coupled with reduced excursion/fixation and retraction or non-coaptation of valve leaflets associated with valvular regurgitation or stenosis. Contrast echocardiography using agitated saline was used to assess the presence of patent foramen ovale. New York Heart Association Class (NHYA) at diagnosis was noted.
Results: Tweny one patients (21%) of patients were found to have CHD. Of those with CHD, 6 (28%) had both left and right sided valvular lesions. Patent foramen ovale was present in all patients with left sided CHD. Valvular involvement: the tricuspid valve was affected in 90% of patients with CHD, pulmonary valve in 76%, the aortic valve in 24% and mitral valve in 19%. Functional class at diagnosis: 24% of patients were in NYHA class 1, 33% in class 2, 33% in class 3 and 10% in class 4 (fig).
Conclusion: The prevalence of carcinoid heart disease has declined from that reported in previous decades. This is likely to be due to increased use of somatostatin analogues to reduce circulating serotonin levels and other anti-tumour therapies. Up to a quarter of patients with CHD were in NYHA Class 1 (functionally asymptomatic) at diagnosis. This study supports the need for a screening programme in all patients with carcinoid tumours.
valvular; carcinoid; prevalence
079 RISK STRATIFICATION IN REAL-WORLD ACUTE CORONARY SYNDROMES: DO CONVENTIONAL METHODS PREDICT EXTENT OF CORONARY ARTERY DISEASE AND NEED FOR REVASCULARISATION?
T. Johnson, S. Dorman, N. West. Gloucestershire Hospitals Foundation NHS Trust, Gloucester, UK
Background: Despite conflicting randomised trial data, many UK centres have adopted early coronary angiography and revascularisation strategies for patients presenting with acute coronary syndromes (ACS); the most contemporary study (ICTUS) favours a selective strategy, with angiography reserved for patients with evidence of refractory/recurrent ischaemia, although trial inclusion mandated high-risk features, including troponin (Tn) elevation, significant ECG change or history of ischaemic heart disease. How these data relate to an unselected “real world” population remains unclear. We aimed to examine the predictive value of markers of risk (Tn levels, ECG change, TIMI risk score) in prediction of extent of coronary artery disease and subsequent need for revascularisation in a cohort of unselected ACS patients undergoing early coronary angiography.
Methods: From April 2004, we adopted a strategy of universal early coronary angiography for all patients <80 years of age presenting with either a positive cardiac Tn or acute/dynamic ECG changes suggestive of ischaemia. Details of all such ACS patients were entered into a dedicated database. Data in this abstract relate to all patients presenting between June and December 2004 and includes follow-up to 12 months.
Results: Cardiac Tn (positive or negative), significant ECG change and TIMI risk score were correlated with need for revascularisation (by PCI or CABG) in all patients undergoing angiography for ACS in the study period (n = 158). A positive Tn was recorded in 75% (118/158) patients. Overall revascularisation rate within 12 months of admission was 56% (88/158). Admission TIMI score correlated with angiographic extent of coronary artery disease in the NSTEMI (r = 0.18; p = 0.04), but not overall population. Need for revascularisation was predicted by Tn positivity (positive vs negative, 0.61 vs 0.39; p = 0.03), but not by presence of significant ECG change (presence vs absence, 0.63 vs 0.48; p = 0.8), TIMI risk score (TIMI 0–3 vs 4–7, 0.52 vs 0.63; p = 0.8) or past history of ischaemic heart disease (history vs no history, 0.6 vs 0.48; p = 0.8). High TIMI score did, however, predict presence of 3 vessel/left mainstem disease at angiography (TIMI 0–3 vs 4–7, 0.17 vs 0.36; p = 0.01). Even 37% of the conventionally lowest-risk individuals, (negative Tn and TIMI score<3) required revascularisation, and 86% of TIMI 0 patients had at least single vessel coronary disease.
Conclusions: Our data suggest that in “real-world” populations, a selectively-invasive strategy in ACS may disadvantage those patients perceived to be at low risk, who require similar rates of revascularisation to those patients notionally at high risk. Conventional risk stratification measures applicable at the bedside may thus be mistaken as diagnostic tools for ACS and can lead to false reassurance regarding the absence of significant obstructive coronary artery disease warranting revascularisation in lower-risk individuals.
acute coronary syndrome; percutaneous coronary intervention; risk stratification
080 CONTEMPORARY ST ELEVATION MYOCARDIAL INFARCTION MANAGEMENT: RESULTS OF A HYBRID LYTIC PROGRAMME ARE EQUIVALENT TO PRIMARY PERCUTANEOUS CORONARY INTERVENTION
B. Freestone, A. Shufflebotham, E. Fountzopoulos, T. Lo, R. Butler, M. Gunning, J. Nolan. University Hospital of North Staffordshire, Stoke-on-Trent, UK
Introduction: Primary percutaneous coronary intervention (PCI) for acute ST elevation myocardial infarction (STEMI) has been reported to confer superior outcomes to thrombolysis, with reductions in short-term reinfarction, stroke and death. However, previous comparison trials did not routinely investigate or revascularise patients treated with thrombolysis. Based on an established prehospital thrombolysis service and an aggressive revascularisation approach (with primary angioplasty where thrombolysis is contraindicated, rescue angioplasty for failed reperfusion, and an early inpatient coronary angiogram for those thrombolysed), the aim of this study was to report practice and outcomes of our centre for patients presenting with acute STEMI.
Methods: We audited retrospective data for all patients admitted directly to University Hospital of North Staffordshire (UHNS) with a final diagnosis of STEMI included in the MINAP dataset (2005/6 financial year, completeness of dataset 99.4%). Patients transferred in to UHNS or without valid entries for method of admission or final diagnosis were not included for analysis.
Results: During 2005/6 there were 308 patients diagnosed with acute STEMI (195 (63.3%) male, mean age 66.3 (13.4), range 31–94 years) including 7 inpatients. Of these, 118 patients (38.3%) received prehospital thrombolysis, 121 (39.2%) received in-hospital thrombolysis and 13 (4.2%) underwent primary angioplasty. Median call to treatment time for those undergoing thrombolysis was 52 (IQR 37–77) minutes. Rescue angioplasty was undertaken in 34 (11.0%) patients for failed reperfusion. 180 (58.4%) underwent inpatient coronary angiography, and the overall inpatient percutaneous revascularisation rate was 40.9% (126 patients). Median time to revascularisation was 2 (IQR 0–4) days. Median length of stay for STEMI patients was 5 (IQR 4–9) days. In-hospital mortality was 6.1% for this period.
Conclusion: This study demonstrates that our hybrid lytic programme has similar in-hospital mortality to trials of primary PCI (estimated at 7% on previously reported metanalysis) and better outcomes than traditional STEMI management. Data from our own hospital also indicate that in-hospital mortality from STEMI has decreased since MINAP data collection began in 2001/2 (from 15% to 6.1%). Improved outcomes over this period may be mediated by an early revascularisation approach for thrombolysed patients as well as increased rates of pre-hospital thombolysis. These findings should be taken into account when considering implementation of a primary PCI strategy for acute STEMI management in the UK.
myocardial infarction; audit; outcomes
081 MANAGEMENT OF REPAIRED AND NATIVE MATERNAL AORTIC COARCTATION DURING PREGNANCY
S. Bowater1, L. Hudsmith1, E. Knox2, P. Clift1, P. Thompson2, S. Thorne1. 1University Hospital Birmingham, Birmingham, UK; 2Birmingham Women’s Hospital, Birmingham, UK
Background: Coarctation of the aorta (CoA) is generally well tolerated in pregnancy. The majority of mothers with CoA will have had previous intervention. The presence of a significant CoA or its sequelae (hypertension, recoarctation or aneurysm of the repair site) is potentially difficult to manage during pregnancy and both fetal and maternal life may be at risk.
Methods: Patients’ notes from the Adult Congenital Heart Disease database with third trimester pregnancies between 2001–6 and a diagnosis of CoA were retrospectively reviewed. In the absence of complication, our practice is to recommend normal vaginal delivery at a local hospital. Patients with native CoA, an aneurysm, significant hypertension or a tight recoarctation require tertiary centre management with regular review in a joint Obstetric and Cardiac clinic with an elective caesarean section (LSCS) advised. In the presence of hypertension or modest recoarctation, mode of delivery is individualised to LSCS or vaginal delivery with short second stage. All women are offered pre-conception counselling and assessment including aortic imaging with MRI.
Results: Twenty four pregnancies in 19 women (mean age at pregnancy 25 (6) years, range of 1–3 pregnancies per patient) resulted in 24 live births. 23/24 patients had previous repair of their CoA: 83% surgical and 17% primary balloon dilatation ± stent. The median age at repair was 9 months (range 9 days–23 years). 10 patients had at least one pre-pregnancy complication of their CoA repair: 42% patients had systemic hypertension, 32% had recoarctation (peak velocity range 1.8 m/s to 3.1 m/s on MRI) and 16% had mild aneurysm formation at the repair site. Nine patients had associated cardiovascular comorbidities including significant aortic valve disease (26%). Five patients had required a reoperation (all before pregnancy). All deliveries were between 35–41 weeks’ gestation. 16/24 (67%) were performed at our tertiary centre. Of these 50% (8/16) were by LSCS, 7 planned (2 for obstetric reasons and 5 for cardiac) and 1 obstetric emergency (for fetal distress). 3/8 vaginal deliveries required instrumentation. The second stage ranged from 22 to 155 min (median 67 min). No peripartum maternal complications or fatalities were recorded.
Conclusion: With good antenatal care, major complications of pregnancies in repaired or native aortic coarctation patients are rare but must remain a source of concern for patients with CoA who become pregnant. Women with a history of CoA contemplating pregnancy should have formal haemodynamic and aortic imaging assessment of the CoA site and associated lesions, preferably before conception. Appropriate risk stratification including joint consultation with obstetric and anaesthetic colleagues for careful management plans and serial monitoring of these patients, with careful attention to systemic blood pressure is essential to minimise risk.
coarctation; pregnancy; risk
082 TRAINING BASIC LIFE SUPPORT TO SCHOOL CHILDREN USING MEDICAL STUDENTS AND TEACHERS IN A “PEER-TRAINING” MODEL: RESULTS OF THE “ABC FOR LIFE” PROGRAMME
P. Toner1, M. Connolly2, L. Laverty3, P. McGrath3, D. Connolly3, D. McCluskey4. 1Craigavon Area Hospital, Craigavon, UK; 2Antrim Area Hospital, Antrim, UK; 3Queen’s University Belfast, Belfast, UK; 4Royal Victoria Hospital, Belfast, UK
Introduction: The “ABC for life” programme was designed to facilitate the wider dissemination of basic life support (BLS) skills and knowledge in the population. There are approximately 25 000 year 7 school children in 900 primary schools in Northern Ireland. By using a pyramidal teaching approach involving medical students and teachers, there is the potential to train BLS to all of these children each year. This study aimed to assess the effectiveness of a three tier “peer training” model of teaching CPR, designed specifically for school children, using medical students and primary school teachers.
Methods: The “ABC for life” programme is a course of instruction in cardiopulmonary resuscitation (CPR) specifically designed to teach 10–12 year old children BLS skills. Medical students were taught to train lay people in BLS. Each medical student subsequently instructs small groups of teachers in BLS, who then teach pupils in their schools. Training consists of a 2-hour teaching session based on video, small group teaching and manikin practice. Medical students instructed teachers from the Western Education and Library Board area of Northern Ireland how to teach BLS skills to year 7 pupils. The first five pupils to be trained in each school were selected from the year 7 class register using random numbers. Pupils were given a 22-point questionnaire to assess knowledge of BLS immediately before and after a teacher-led training session.
Results: Thirty eight teachers were trained (190 pupils included). Questionnaires were returned for 85 (44.7%) pupils at baseline and 80 (42.1%) pupils after training. Mean age was 10.7 years and 35.4% were male. Baseline CPR knowledge or change following training were not affected by sex, positive family history of heart disease or previous BLS training. The score distribution at baseline and following training were notably different (fig). Scores improved markedly following training with a mean increase from 57.2% to 77.7% (t test, p<0.001).
Conclusion: Primary school teachers, previously trained by medical students, can effectively teach BLS to 10–12 year old children using the “ABC for life” programme. There appears to be good transfer of knowledge down the teaching chain from medical student to pupil. By using this method, large numbers of children may be taught BLS successfully in an efficient and cost-effective manner.
basic life support; schools; peer-training
083 DOES A STRATEGY OF SELECTIVE BIOMARKER TESTING FOLLOWING PERCUTANEOUS CORONARY INTERVENTION MISS PROGNOSTICALLY IMPORTANT PROCEDURE-RELATED MYOCARDIAL INFARCTIONS?
C. Berry, P. L. L’Allier, R. Ibrahim, L. Bilodeau, E. Kedhi, R. Mikhail, J. Lavoie, J. Dupuis, J. Lambert. Montreal Heart Institute, Montreal, Canada
Introduction: Current guidelines indicate that cardiac biomarkers should be measured in patients with symptoms or signs of myocardial infarction (MI) after percutaneous coronary intervention (PCI) or in whom PCI was complicated. We questioned whether clinicians can accurately determine which patients will or will not have biomarker elevation post-PCI.
Methods: Data from consecutive non-primary non-rescue PCI cases performed in an acute tertiary care cardiac centre were prospectively recorded. Blood samples were obtained on admission and at 12–24 h post-PCI (normal ranges: troponin T 0–0.03 µg/l; creatinine kinase MB 0–5 mg/l). After the PCI, the operator indicated whether he believed a biomarker rise would occur. An elevated baseline troponin/CKMB concentration was not an exclusion criterion.
Results: 454 patients (mean (SD) age 63 (11) years; 74% men; 25% diabetes; 59% unstable angina/MI) were included. Previous PCI or CABG had been performed in 130 (29%) and 81 (18%) patients, respectively. 228 (50%) patients were pretreated with clopidogrel and 142 (31%) patients received glycoprotein IIbIIIa therapy. Troponin T elevations post-PCI versus baseline >x1ULN, >1ULN–⩾x3 ULN, >x3ULN–⩾x5 ULN, or >x5ULN occurred in 65.4%, 10.1%, 6.6% and 17.8% of patients, respectively. The corresponding values for CKMB were 79.5%, 12.8%, 4.0% and 3.7%, respectively. Interventional cardiologists (n = 13) predicted a biomarker elevation in 98 (21.6%) patients, and their responses were homogeneous (Breslow-Day Homogeneity Tests, p>0.1). The Mantel-Haenszel odds ratios (95% CI) for prediction of actual post-PCI elevations >x5ULN for CKMB and troponin T were 11.70 (3.62 to 37.84) and 3.82 (2.23 to 6.53), respectively. Prediction of these events was influenced by procedural complications. The sensitivity, specificity, and positive and negative predictive values of the clinicians’ responses for CKMB elevation post-PCI >x5ULN were 76%, 80%, 13%, and 99%. The corresponding values for troponin T elevation post-PCI >x5ULN were 43%, 83%, 36% and 87%, respectively.
Conclusions: Interventionalists can predict most, but not all cases, of prognostically important elevation in cardiac biomarkers post-PCI. A small but important number of post-PCI MI events are missed by a strategy of selective biomarker testing, and the positive predictive values for >x5ULN elevations in CKMB and troponin were relatively low. These results cast doubt on contemporary guideline recommendations which state that biomarker testing may be performed in selected patients in whom MI is suspected. Biomarker testing in all PCI patients may be required to prevent patients with undisclosed MI being discharged without appropriate risk stratification measures.
biomarker; myocardial infarction; angioplasty
084 FEASIBILITY OF DIAGNOSING AND QUANTIFYING METABOLIC SYNDROME IN CONSECUTIVE ACUTE MEDICAL ADMISSIONS
G. Balakrishnan1, A. Weerasinghe1, K. Zacharias1, J. Mathers1, N. Joseph1, R. Sudhir1, C. Andrews1, J. Katz1, A. Bakhai2. 1Barnet General Hospital, Barnet, UK; 2Barnet General Hospital/AMORE study group, London, UK
Introduction: Patients with metabolic syndrome (MetS) are at increased subsequent risk of cardiovascular disease and diabetes. Risk factors such as smoking and hypertension are routinely addressed in acute medical admissions even if coincidental. Data on identifying MetS in a secondary care setting are unavailable. Therefore we sought to quantify the potential number of patients with this novel risk factor and to evaluate the feasibility of diagnosing MetS among medical admissions with a view to early intervention.
Abstract 084 Table 1 Common exclusion reasons
Abstract 084 Table 2 Characteristics of patients with MetS
Methods: All consecutive medical admissions to our district hospital were screened for 2 months using the International Diabetes Federation (IDF) criteria to diagnose MetS. We reviewed all patients to remove those with pre-existing diabetes and cardiovascular disease and those with severe acute illness or cognitive impairment precluding consent. Consenting patients had mid-abdominal circumference (MAC) and fasting glucose and lipid profile measured pre-discharge.
Results: Of the 825 patients reviewed, 642 had to be excluded (see fig) for reasons presented in table 1. The prevalence of MetS in patients with complete data available was 29% (22/75, 95% CI 19–41%).
Conclusions/Implications: This study demonstrates the difficulties of identifying the novel risk factor of metabolic syndrome in secondary care with large numbers of patients being excluded and many patients not interested. Of those consenting, the prevalence was higher than smoking (29 vs 24%). We recommend modifications to the application of the IDF criteria in the acute settings to assist those screening patients for MetS in secondary care.
metabolic syndrome; diabetes; cardiovascular risk
085 USING CASE-MIX ADJUSTED FUNNEL PLOTS OF 30-DAY MORTALITY FOR ACUTE CORONARY SYNDROMES TO EXPLORE HOSPITAL PERFORMANCE
C. Gale1, R. Ramachandra2, V. Baliga2, F. Dudley2, R. Gale1, A. Roberts3, P. Batin2, J. Wilson2, A. Hall1. 1Leeds General Infirmary, Leeds, UK; 2Pinderfields Hospital, Wakefield, UK; 3University of Durham, Durham, UK
Introduction: Quality assurance and audit are central to good medical practice. Variation in hospital mortality for acute coronary syndromes (ACS) is in part attributable to case-mix and differences in mortality after case-mix adjustment reflect performance. The Evaluation of the Methods and Management of Acute Coronary Syndrome (EMMACE) risk score may be used for case-mix adjustment (EMMACE is a community-derived risk model that uses patient age, admission heart rate and admission systolic blood pressure to adjust 30-day mortality rates in patients with ACS) and temporal hospital performance may be explored with case-mix adjusted funnel plots. We aim to audit our hospitals 30 day mortality for ACS and investigate any inter- and intra-subgroup variation.
Methods: We identified 1279 consecutive patients admitted to Pinderfields General Hospital with an admission diagnosis of ACS during 2004 and 2005 and followed them up for 14 months. Data from patient records were encrypted into a cardiology-specific database (HD Clinical, UK). Cumulative funnel plots of observed and predicted mean performance on a case-series basis were generated. Upper and lower control limits calculated at 3 sigma around the mean predicted mortality were derived using the method described by Spiegelhalter. Groups were compared using the χ2 test for categorical data and analysis of variance for continuous variables. EMMACE had previously been validated in a wider population of ACS patients (C index 0.78 (95% CI 0.77 to 0.78)).
Results: Mean age was 65.5 (SD 13.9) years. 19.4% were diabetic. The mean (SD) systolic blood pressure and heart rates were 142 (28) and 80 (22) respectively. 55 patients (4.3%) died in hospital. The 30-day all-cause mortality was 6.17%. The 30-day/total mortality rates were significantly higher in patients with diabetes (p⩽0.001) and troponin-positive acute coronary syndromes (p⩽0.01). The mortality rates were not significantly different in patients with STEMI or NSTEMI. The observed and predicted mortality were easily visualised in the funnel plot and allowed comparison of the observed and expected quality of care. The control limits described expected variation around the predicted mortality rate, for a given volume of cases. The more cases studied, the more precisely the predicted mortality confined the observed mortality. If the observed mortality rate transgressed the control limit, special cause variation was implied. We identified areas of special cause variation in troponin-positive ACS but not in STEMI, NSTEMI, ACS troponin-negative and diabetes subgroups. The figure depicts cumulative mortality in the entire ACS cohort.
Conclusions: Using a combination of the EMMACE risk model and funnel plots, it is possible to assess case-mix adjusted hospital performance which can be easily visualised. Real-time monitoring of performance is possible allowing early assessment and intervention to variations.
acute coronary syndromes; case-mix adjusted funnel plots; hospital performance
086 SEX DIFFERENCE IN THE RELATION BETWEEN SOCIOECONOMIC DEPRIVATION AND FATAL VERSUS NON-FATAL MYOCARDIAL INFARCTION
P. Jhund, K. MacIntyre, J. McMurray. University of Glasgow, Glasgow, UK
Introduction: Socioeconomic deprivation (SED) has been identified as an important risk factor for myocardial infarction (MI). However, it is not clear whether it predicts outcome after adjustment for traditional risk factors. The relative importance of SED as a predictor of fatal versus non-fatal outcomes and in men versus women is also uncertain. We hypothesised that SED is an independent predictor of both first hospitalisation for MI and MI death (and equally so in men and women) even after adjustment for traditional risk factors.
Methods: We examined outcomes in 15 378 men and women initially surveyed between 1972–6 in Renfrew and Paisley, Scotland, and followed until 31/3/2004. Hazards ratios (HR) for a first admission with a MI (as principal diagnosis) and death from MI were calculated using Cox regression. All analyses were adjusted for age, body mass index, systolic and diastolic blood pressure, cholesterol, smoking, ECG ischaemia, and a history of diabetes, angina or stroke. Deprivation was defined using the seven category Carstairs-Morris deprivation index. Deprivation categories (depcat) 6 and 7 (the most deprived depcats) were combined to increase power due to small numbers of individuals in group 7. Log rank tests were used to compare the overall trend across depcats.
Results: During ⩾28 years follow-up, 1873 men and women had a first MI hospitalisation and 2370 a MI death. Compared to the most affluent (depcat 1), the risk of MI death in men and women combined in depcat 6/7 was 37% higher (hazard ratio (HR) 1.37 (p = 0.001)), trend p<0.0001. The HR for men alone in depcat 6/7 versus depcat 1 was 1.35 (p = 0.018) and similarly 1.38 for women alone (p = 0.027) after adjustment for risk factors. For men and women combined in depcat 6/7 (compared to depcat 1), the HR for a first MI hospitalisation was 1.34 (p = 0.007), p<0.0001. The HR was 1.1 for men (p = 0.5) and 1.74 for women (p = 0.002) after adjustment for risk factors.
Conclusion: Even after accounting for “traditional” risk factors, SED is associated with an increased risk of MI death which is of similar magnitude in men and women. By contrast, SED is associated with a smaller risk of first hospitalisation for MI in men than women after accounting for risk factors. The explanation for this sex difference is uncertain but may represent a differential effect of SED on survival to hospital admission in men and women with a MI.
sex; myocardial infarction; deprivation
087 USING THE MYOCARDIAL INFARCTION NATIONAL AUDIT PROJECT DATABASE TO VALIDATE ACUTE CORONARY SYNDROME RISK SCORES BY SUBGROUP RISK
C. Gale1, S. Manda2, C. Weston3, J. Birkhead4, P. Batin5, A. Hall1. 1Yorkshire Heart Centre, Leeds General Infirmary, Leeds, UK; 2Centre for Biostatistics, University of Leeds, Leeds, UK; 3Department of Cardiology, Singleton Hospital, Swansea, UK; 4Department of Cardiology, Northampton General Hospital, Northampton, UK; 5Department of Cardiology, Pinderfields General Hospital, Wakefield, UK
Introduction: Risk models help medical decision-making for patients with acute coronary syndromes (ACS) but many are developed from randomised controlled trials and are only validated in the derivation cohort. In addition, the use of ACS risk scores is often extrapolated to subgroups of differing mortality risk. We used the Myocardial Infarction National Audit Project (MINAP) database, a UK registry of ACS, to externally validate popular ACS risk models and to determine whether their performances were maintained across a range of subgroups.
Abstract 087
Methods: The performance of the risk models were evaluated using the area under the receiver operating curve (c-index) in those with and without diabetes, with and without chronic renal failure and with and without a history of angina. We had data for 187 069 patients and validated the following risk scores: Simple Risk Index; PURSUIT, GUSTO-1, EMMACE, and GRACE.
Results: We found that all risk scores performed well in their target populations (C index, (95% CI); Simple Risk Index = 0.790 (0.783 to 0.798); PURSUIT = 0.788 (0.779 to 0.797); GUSTO-1 = 0.804 (0.789 to 0.818); EMMACE = 0.797 (0.790 to 0.804); GRACE (in hospital mortality) = 0.804 (0.798 to 0.810); GRACE (6 month mortality) = 0.799 (0.794 to 0.804)). The risk scores’ ability to discriminate death was reduced when applied to higher risk subgroups (table).
Conclusion: Overall the risk scores demonstrated good discrimination of mortality across a spectrum of subgroups in our population. However, there was a trend towards reduced discriminative performance in higher risk subgroups.
MINAP; acute coronary syndrome; risk score
088 INFANT ASSESSMENT FOR CARDIAC TRANSPLANTATION
C. Kirk, A. Hasan, G. Parry, J. Cassidy, N. Wrightson. Freeman Hospital, Newcastle upon Tyne, UK
Aim: A retrospective review of infants (children less than 1 year old) with end-stage cardiac failure referred for assessment for cardiac transplantation was undertaken to determine their outcome in a centre offering all modalities of treatment for severe heart failure (inotropic, mechanical support and transplantation).
Methods: A total of 26 referrals (15 females and 11 males) for cardiac transplantation were made to this unit between April 1996 and March 2006. The mean (range) age at assessment was 156 days (16–362 days). 19 had dilated cardiomyopathy (14 idiopathic, 3 non-compaction, 1 associated with Barth syndrome, 1 associated with complete heart block), 2 hypertrophic cardiomyopathy, 4 congenital heart disease and 1 secondary to neonatal myocardial infarction. Mean time from symptom onset to assessment was 65 days (0–207 days). At the time of assessment 13 were ventilated with inotropic support with 2 also on ECMO, 4 were on inotropic support alone and the remaining 9 patients were on oral therapy. The mean (range) follow-up time was 2.35 (1 day–11.1) years.
Results: Figure 1 shows the outcome of the infant assessments. Of those listed for transplant the mean (range) waiting time to transplant, death or delisting was 69 (1–390) days. The Kaplan Meier survival curve (fig 2) shows an early rapid attrition with a subsequent long-term survival of 55%. The patient support at time of assessment, age, length of history, renal function and blood group had no influence on outcome. In general those with congenital heart disease had poorer outcomes. Dividing the study period into two eras (financial years 1996–2000 and financial years 2001–5) demonstrated an increased waiting time from a mean of 44 days to 99 days. This coincided with a dramatic fall in donor offers suitable for infants from a mean (range) of 21 (13–31) offers per year to 7 (7–8) offers per year. There was however no increase in deaths while waiting for transplant between the two eras, which may have been due to the introduction of ABO mismatched transplants in 2000.
Conclusion: This information allows better counselling of families undergoing assessment for infant transplantation. The increased waiting time for infant cardiac transplantation and reduction of donor organ offers is of major concern and has implications for the use of mechanical support as a bridge to transplant in this group.
infant; transplant; assessment
089 PLANAR CELL POLARITY SIGNALLING PLAYS CRUCIAL ROLES IN OUTFLOW TRACT DEVELOPMENT
D. Henderson, H. Phillips. Institute of Human Genetics, Newcastle University, Newcastle upon Tyne, UK
Background: The non-canonical Wnt, planar cell polarity, regulates the movement of polarised cells within the developing embryo. Our studies have shown that this pathway plays crucial roles in cardiac development. Mice that carry mutations in the Vangl2 gene, a crucial member of the pathway, develop double outlet right ventricle and ventricular septal defects (
) . Moreover, polarised migration of myocardial cells is disrupted in the mutant embryos. We also see similar defects in mutants for several other members of the “core” pathway, and in embryos that are doubly heterozygous for mutations in two different genes acting in the pathway. Together, these data suggest that planar cell polarity signalling is crucial for normal outflow tract development.
Methods and Results: In order to begin to analyse the pathway downstream of PCP signalling, we have examined the expression patterns of a number of factors implicated in the pathway. Strikingly, the PCP downstream effector Rho kinase 1 (ROCK1) is highly expressed in the polarised myocardial cells that migrate into the outflow tract cushions and that are disrupted in Lp mutant hearts. Moreover, the expression of ROCK1 is altered in the myocardialising cells of Lp mutants. In order to determine whether PCP signalling via ROCK is essential for development of the outflow tract, we have begun to use transgenic mouse lines that allow tissue-specific expression of dominant-negative forms of ROCK in order to inhibit ROCK expression in specific cell types within the developing heart. Surprisingly, ROCK expression in the myocardium was not essential for normal outflow tract development. However, knockout of ROCK in neural crest cells resulted in double outlet right ventricle, and knockout in secondary heart field cells resulted in common arterial trunk.
Conclusions: Together these data show that PCP signalling via ROCK is essential within multiple cell types during outflow tract development and supports a crucial role for this pathway during outflow tract development. We propose that this pathway may be of importance for human congenital heart defects and that mutations should be sought in patients with congenital defects affecting the outflow of the heart.
congenital heart defects; mouse model; outflow tract
090 PREDICTION OF FETAL COARCTATION OF THE AORTA FROM THE THREE VESSEL AND TRACHEAL VIEW
H. Matsui1, L. Pasquini1, A. Seale2, M. Mellander2, M. Roughton2, S. Ho2, H. Gardiner1. 1Faculty of Medicine, Imperial College at Queen Charlotte’s & Chelsea Hospital, London, UK; 2Royal Brompton Hospital, London, UK
Background: Prenatal diagnosis of isolated coarctation of the aorta (CoA) suffers from high false positive and false negative rates. Suspicion is raised by disproportion at four chamber and/or great arterial views. The aim of our study was to develop Z scores for the aortic isthmus and measure the isthmal:duct ratio (I:D) in normal fetuses as a reference for fetuses with suspected coarctation and test these scores in fetuses referred with suspected CoA based on sonographic appearances of disproportion at four chamber and/or great arterial levels.
Methods: The aortic isthmal diameter, immediately proximal to the insertion of the arterial duct, was measured prospectively in the transverse plane (three vessel and tracheal view) in 221 normal fetuses at 18 to 37 weeks’ gestation. The ductal diameter (D) was measured immediately before it entered the descending aorta (DAo) in the same view. All measurements were repeated three times by a single investigator and averaged. Z scores were created relating isthmal and ductal diameters to femoral length and gestational age and the I:D ratio recorded. Isolated CoA was defined as hearts with normal situs and connections, with or without a VSD and a narrow transverse aortic arch or isthmus. Cases with bicuspid aortic valve were included. Archived digital data of 31 fetuses with suspected CoA were examined by a single observer, blinded to outcome. Isthmal Z scores were plotted on the normal charts and I:D ratio calculated.
Results: Inter-observer mean difference of isthmal Z scores was −0.04 mm (95% CI −0.8 to 0.71). Serial isthmal Z scores improved to >−2 during pregnancy in most normal neonates; those requiring surveillance or surgery remained <−2. The normal I:D ratio = mean 0.99 (SD 0.13) (95% CI 0.97 to 1.01) and did not change through pregnancy so 95% of all normal values lay between (0.74 to 1.23). The I:D ratio was helpful in distinguishing (a) normal from abnormal arches at first scan; (b) the need for neonatal surgery at serial assessment (table).
Conclusions: Serial isthmal Z scores distinguish between normal arches and those with coarctation of the aorta or hypoplasia, but they appear unable to identify those requiring early surgery. The I:D ratio measured at first scan helped distinguish those with coarctation from fetuses with a normal aortic arch and was a better indicator of need for surgery than isthmal Z scores of those with arch hypoplasia.
fetus; coarctation of the aorta; isthmal Z-Scores
091 RENAL FUNCTION AND OUTCOME FROM VALVE SURGERY
P. Gibson, M. Chiwara, B. Croal, B. Cuthbertson, G. Small, G. Gibson, R. Jeffrey, K. Buchan, H. El-Shafei, G. Hillis. Aberdeen Royal Infirmary, Aberdeen, UK
Background: Renal dysfunction is an important risk factor in patients undergoing coronary artery bypass grafting (CABG). The prognostic importance of renal function in patients with valvular heart disease is poorly defined. We hypothesised that, although the mechanisms may differ, renal function would be an important determinant of outcome after surgery for valvular heart disease.
Methods: We studied 514 consecutive patients undergoing heart valve surgery between April 2000 and March 2004. Patients with active infective endocarditis and/or requiring emergency surgery were excluded. The glomerular filtration rate was estimated (eGFR) using the Modification of Diet in Renal Disease equation. Baseline demographic and clinical variables were recorded prospectively, including the European System for Cardiac Operative Risk Evaluation (EuroSCORE). The primary outcome variable was all-cause mortality.
Results: During a median follow-up of 2.0 (interquartile range 1.2–4.5) years, 87 patients died (74 primarily or partly from cardiovascular disease). In univariable analysis both eGFR (hazard ratio (HR) 0.68 per 10 ml/min per 1.73 m2, 95% CI 0.60 to 0.78, p<0.001) and creatinine (HR 1.04 per 10 µmol/l, 95% CI 1.02 to 1.06, p<0.001) were predictive of mortality. Estimated GFR was, however, the stronger predictor (χ2 30.1 vs 15.3, p<0.001) and was used in subsequent multivariable models. Estimated GFR remained a powerful independent predictor of death in a backward selection multivariable model including all study variables (HR 0.75 per 10 ml/min per 1.73 m2, 95% CI 0.64 to 0.88, p<0.001) and in a model with EuroSCORE (HR 0.74 per 10 ml/min per 1.73 m2, 95% CI 0.64 to 0.87, p<0.001). An eGFR of <60 ml/min per 1.73 m2 was associated with greatly increased short and long-term mortality (fig) and after correction for preoperative EuroSCORE conferred an excess hazard of death of 2.31 (95% CI 1.41 to 3.80, p = 0.001). In the subgroup of 321 patients (62%) who underwent only valve surgery (without concomitant CABG), eGFR remained a strong univariable (HR 0.68 per 10 ml/min per 1.73 m2, 95% CI 0.58 to 0.80, p<0.001) and multivariable predictor (HR 0.74 per 10 ml/min per 1.73 m2, 95% CI 0.62 to 0.88, p<0.001). The excess hazard associated with an eGFR of <60 ml/min per 1.73 m2 in this subgroup was 2.73 (95% CI 1.41 to 5.28, p = 0.003).
Conclusion: Renal function, in particular the eGFR, is a powerful predictor of outcome in patients undergoing surgery for valvular heart disease. This prognostic utility is independent of other recognised risk factors and the EuroSCORE.
valve surgery; renal function; survival
092 THE IMPACT OF PERCUTANEOUS ATRIAL SEPTAL DEFECT CLOSURE IN THE OLDER POPULATION
A. Khan, J. Tan, W. Li, M. Spence, M. Mullen. Royal Brompton Hospital, London, UK
Background: Atrial septal defect (ASD) closure before the age of 25 years has been demonstrated to improve cardiac status and functional class in young adults. The benefit of ASD closure in elderly subjects is less clear. We therefore, prospectively, assessed the impact of percutaneous ASD closure on cardiovascular form and function in patients >50 years of age.
Abstract 092 Table 1
Abstract 092 Table 2
Methods: Patients (n = 23, age median 68 years, mean 67 years, range 50–91 years) referred for percutaneous ASD closure were assessed with a six minute walk test (6MWT), electrocardiogram (ECG), chest x ray (CXR) and transthoracic echocardiogram at baseline (pre closure) and at 6 weeks following device closure. Blood sample were also taken for ANP and BNP analysis.
Results: See tables 1 and 2. All patients had successful closure of their ASD (mean defect size 20 mm, mean device size 26 mm, mean Qp/Qs >2, mean PA pressure 21 mmHg, atrial fibrillation 21%). One patient died suddenly 24 weeks after device closure. At follow-up, NYHA class improved (p = 0.004) in 14 patients with a trend towards increased 6MWT (p = 0.001). Right ventricular volume was significantly reduced (p = 0.05) while left ventricular size increased with a significant improvement in EF (p = 0.05) after the device closure compared to baseline. However there was no change observed in heart rate and oxygen saturations in these patients with 6MWT. ANP and BNP levels remain unchanged 6 weeks after device closure (p = NS).
Conclusion: These results demonstrate significant improvement in symptoms and cardiac function following ASD closure despite the patients’ advanced years.
atrial septal defect; device closure; elderly
093 ARRHYTHMIA BURDEN IN ADULTS WITH CONGENITAL HEART DISEASE IN A LEVEL 2 GUCH CENTRE
P. Felix, S. Howard, L. Freeman. Norfolk and Norwich University Hospital NHS Trust, Norwich, UK
Introduction: The number of patients born with congenital heart disease (CHD) surviving to adult life is increasing exponentially. Our institution is an intermediate (level 2) grown-up congenital heart disease (GUCH) centre with a dedicated clinic for adults with congenital heart disease started in 1993. The patient population has increased from 330 in 1998 to 632 in 2004 (820 in 2006). Arrhythmia is an increasingly important cause of morbidity and mortality in GUCH patients. We have sought to determine the arrhythmia burden in a secondary care hospital which is likely to be reflected through many other institutions. This has not previously been established.
Method and Results: The GUCH clinic database was used for the patient demographics and to analyse the frequency and types of arrhythmias in the different groups. The records of patients who have died during this time were also assessed to determine the frequency of sudden cardiac death (SCD). Certain patient groups have annual ambulatory 24-h Holter monitoring (eg TGA, Fallot) while in others this is triggered by symptoms. Routine exercise testing may occur in certain groups (eg TGA, Fallot with pulmonary regurgitation) or for pre-pregnancy assessment which may highlight arrhythmias.
Patient Population: There are 632 patients seen in the clinic with an average age of 36 years (range 10–80 years). Operative intervention has been performed in 468 (74%) with 96 (15.2%) requiring a second operation and 39 (6.2%) a third operation. An additional 20 patients have died. Our clinic serves a catchment population of around 700 000.
Results: Of the 632 patients, 16.1% (102) had a documented arrhythmia. Conditions with the highest arrhythmia load were secundum ASD 39% (27/69), TGA 50% (10/20), Ebstein 57% (4/7), complex CHD 32% (8/25). Fallot’s tetralogy surprisingly had infrequent arrhythmias (10/56). All other groups have incidence less than 18%. 22.3% of these underwent EPS and ablation, while 16.5% had permanent pacemaker(PPM) insertion. Routine screening only detected 16% of the total arrhythmias in simple CHD compared with 38% in complex CHD. The number of congenital heart disease patients admitted with an arrhythmia over the last 4 years is 33 (5.2%). An additional 20 patients have died since inception of the clinic; of these 8 patients had SCD at home.
Conclusion: 16.1% of this heterogeneous group of adults with congenital heart disease have arrhythmias; this is the first report documenting the arrhythmia burden in a secondary care setting. Screening as a tool for identifying these arrhythmias is more useful in complex congenital heart disease—where resources for screening should be directed. Supra regional EPS centres for this group with complex anatomy need to be increased to deal with this increasing demand. This is an important area that needs specialist recognition and funding.
arrhythmias; adult congenital heart disease; GUCH
094 ROLE OF MODIFIED VALSALVA MANOEUVRE IN THE DIAGNOSIS OF PATENT FORAMEN OVALE BY TRANSOESOPHAGEAL ECHOCARDIOGRAPHY
U. Velupandian1, R. Khiani1, S. Ray2, J. Morris2, A. Heagerty1, C. McCollum1. 1University of Manchester, Manchester, UK; 2South Manchester University Hospital, Manchester, UK
Purpose: Paradoxical embolism through a patent foramen ovale (PFO), may cause ischaemic stroke in young adults and decompression sickness. PFO is a flap valve and shunting is dynamic and dependant on the pressure gradient between the right and left atrium. Valsalva manoeuvre (mVM) can increase the right atrial pressure; however it cannot be performed effectively with transoesophageal echocardiogram (TOE) owing to sedation and oesophageal intubation. We assessed the effect of abdominal compression as mVM with TOE using antecubital (AV) and femoral vein (FV) for contrast administration.
Methods: Young adults (n = 62) with possible paradoxical embolism underwent TOE A standard injection protocol was used with ultrasound contrast (agitated saline-air-blood) administered via both AV and FV (1) at rest and (2) with an mVM in the form of external abdominal compression applied to coincide with appearance of microbubbles in the right atrium and causing visible displacement of the interatrial septum. All studies were analysed post-test by two observers blind to clinical details and the shunt with each injection were graded as negative, small, moderate or large shunts based on passage of 0, <10, 10–50 and >50 microbubbles respectively.
Results: Twenty four out of 62 patients (38.7%) were detected to have a PFO. With AV injections, 6 out of 24 (25%) PFOs were detected only with the use of mVM, of which 5 were classified as moderate shunts. In addition mVM increased the shunt grade from small to moderate in one patient. However, 3 out of 24 (12.5%) PFOs failed detection even with the use of mVM with AV injections (fig 1). With FV injections, in 1 out of 24 (4%) patients, a small PFO was detected only with use of mVM and the shunt grade was increased in 3 out of 24 (12.5%) patients to a large shunt with the use of mVM (fig 2).
Conclusion: For TOE with AV injections, use of mVM improves PFO detection and should be included in the diagnostic protocol as a routine. For TOE with FV injections the use of mVM may help in better estimation of the shunt size.
patent foramen ovale; Valsalva manoeuvre; echocardiogram (transoesophageal)
095 THE TIME COURSE OF IMPROVEMENT IN ECG STRAIN PATTERN AFTER AVR FOR AORTIC STENOSIS AND ITS UNDERLYING MECHANISMS
X. Du, X. Jin. John Radcliffe Hospital, Oxford, UK
Background: ECG lateral leads S-T depression and T wave inversion (ECG strain pattern) is commonly present in patients with left ventricular hypertrophy (LVH) caused by aortic stenosis (AS). The quantitative correlation between the strain pattern and the degree of AS and LVH has not been fully elucidated. The aim of the present study was to assess the time course of changes in lateral leads S-T segment level and T wave amplitude after AVR for AS, and to determine whether aortic valve pressure gradient and left ventricular mass index can predict the ST-T changes.
Methods: Eighty three patients (mean age 72.0 (5.0), 55 male) with AS who underwent AVR were prospectively studied by digital 12-lead ECG and echocardiography before AVR and at 1 week, 6, 12 and 24 months after the operation. Aortic valve mean systolic pressure gradient (AVMG) and left ventricular mass index (LVMI), S-T segment level and T wave amplitude with respect to ECG isoelectric line were measured by built-in software of lead I, aVL, V5 and V6. The mean S-T segment level and T wave amplitude of 4 leads was calculated.
Results: After correcting AS, AVMG fell from 44.7 (15.5) to 9.7 (6.5), mmHg (p<0.001); the preoperative ST depression was improved immediately from −34 (38) to 0.3 (36) uV, p<0.001) at one week after AVR and remained unchanged up to 24 months afterwards. Despite LVMI has regressed significantly at 6 months after AVR (131.4 (33.0) vs 174.9 (37.8), g/m2, p<0.01), the improvement of T wave amplitude from pre-AVR occurred at 12 months after AVR (54 (118) vs −6 (192) uV, p<0.001). Stepwise regression analysis of whole dataset identified that AVMG or LVMI was the most significant echo predicator of S-T segment level or T wave amplitude, respectively (r = −0.46 and −0.358; p<0.001).
Conclusion: In patients with AS, the two elements of ECG strain pattern are determined by different physiological mechanisms and improves with different time course after AVR. S-T segment depression is mainly caused by aortic valve pressure gradient, it therefore improves immediately after AVR; T wave amplitude reduction is, however, resulted from LVH, and it improves only after LVH has regressed towards normal level. S-T segment and T wave amplitude should therefore be regarded as different physiological entities when their clinical implications in AS patients are considered.
ECG strain pattern; aortic stenosis; left ventricular hypertrophy
096 LEFT DOMINANT CORONARY ARTERIAL SYSTEM IN AORTIC STENOSIS: AN ASSOCIATION, CAUSE OR EFFECT
A. Innasimuthu1, G. Morris2, G. Rao1, J. Fox3, R. Perry4. 1University Hospital Aintree, Liverpool, UK; 2Division of Cardiovascular and Endocrine Sciences, University of Manchester, Manchester, UK; 3Southport and Ormskirk NHS Trust, Southport, UK; 4The Cardiothoracic Centre, Liverpool, UK
Background: Traditionally, aortic stenosis (AS) was thought to be caused by passive calcium deposition in the valve. The advancement of molecular medicine introduces the concept of inherited susceptibility to vascular inflammation and calcification. Furthermore, clinical observations have suggested an association between left dominant coronary artery circulation and significant AS which has been previously investigated using small samples of patients.
Method: A retrospective study was designed looking at coronary angiograms from 2000 to 2006 at the Cardiothoracic Centre. Using the angiogram database we studied dominance of coronary arteries (determined by supply of posterior descending artery), ejection fraction and aortic gradient. 2027 patients underwent angiography, of these 1891 were included in the study. 136 were excluded from the study due to insufficient data (dominance was not mentioned in 37 patients, the remaining 99 had insufficient aortic gradient data or EF <30% and therefore possibility of false low aortic valve gradient). We classified the severity of AS by measured pressure gradient—none (0), mild (<30), moderate (30–49), severe (>49). Statistical analysis was performed with χ2 test using Statsdirect.
Results: There were 627 patients with AS and 1264 with no AS. In the non-AS group there were 201, 960 and 103 patients with left, right and co-dominance respectively. In the AS group, there was a significant association with a left dominant circulation: 145, 415 and 67 patients respectively (p<0.001). We further analysed the AS group on the severity to determine the trend. In the mild AS group, there were 39, 160 and 20 patients with left, right and co-dominant respectively. Similarly in the moderate AS group, 34, 129 and 15 respectively and severe AS group 72, 126 and 24 respectively (p<0.001). The linear trend analysis shows sample correlation (r) of −0.124837.
Conclusion: There is association of AS and left dominance of coronary arterial system and there is increased association with the severity of AS showing a linear trend. The reasons and implications of this finding are unclear. The left dominance may be a causative factor altering the blood flow near the aortic valve causing degeneration and stenosis or the genetics of left dominance may be associated with other risk factors for AS by genetic linkage. Lastly the result may represent bias, in that a left dominant circulation may cause increased symptoms of AS and thus more patients to present.
aortic stenosis; left dominance of coronary arteries; severity of aortic stenosis
097 IS HEART FAILURE A PROCESS OF RELENTLESS PROGRESSIVE VENTRICULAR REMODELLING AND FUNCTIONAL DETERIORATION?
N. Lewis, D. Barker, D. Schlosshan, L. Tan. Leeds General Infirmary, Leeds, UK
Background: The course of dilated cardiomyopathy is usually one of progressive deterioration. However improvements in cardiac performance are also known to occur frequently with optimal medical management. The ongoing assessment in this group that improve has not been well described. We report a series of 13 patients with idiopathic dilated cardiomyopathy, referred for evaluation for heart transplantation, who showed evidence of improvement without any interventions except optimal medical therapy.
Abstract 097
Methods: All 13 subjects underwent baseline assessment with echocardiography and maximal symptom limited cardiopulmonary exercise testing with non-invasive estimation of cardiac output by the CO2 re-breathing method. Repeat echocardiography and cardiopulmonary exercise testing were performed after a mean follow-up of 21 (13) months.
Results: At baseline, all 13 patients were treated with ACE inhibitors, 10 patients with betablockers, 13 patients with loop diuretics, 5 patients with digoxin and 5 patients with spironolactone. Baseline ejection fraction (EF) was 26% and left ventricular end diastolic diameter (LVEDD) 76 mm. The patients showed a highly significant improvement in peak oxygen consumption (VO2), peak cardiac output (CO), peak systolic blood pressure (SBP) and peak cardiac power output (CPO). There was also a significant improvement in EF and LVEDD, however both these measurements did not return to normal. At follow-up assessment, 12 patients were treated with ACE inhibitors, 12 patients with beta blockers, 6 patients with digoxin, 5 patients with spironolactone. Only 8 patients still needed loop diuretics.
Conclusion: Recovery from acute dilated cardiomyopathy is better assessed by measuring improvement in peak cardiac power output and maximal oxygen consumption, than ejection fraction or left ventricular dimensions. This in turn helps guide ongoing management, especially in the use of loop diuretics.
idiopathic dilated cardiomyopathy; cardiac power output; cardiac function
098 LEFT VENTRICULAR REVERSE REMODELLING AFTER CARDIAC RESYNCHRONISATION THERAPY IN HEART FAILURE PATIENTS WITH A NARROW QRS DURATION
L. Williams1, S. Ellery2, B. Stegemann3, K. Patel1, F. Leyva4, V. Paul2, M. Frenneaux1. 1University of Birmingham, Birmingham, Uk; 2St Peter’s Hospital, Chertsey, UK; 3Medtronic Bakken Research Centre, Maastricht, the Netherlands; 4Good Hope Hospital, Birmingham, UK
Aims: Cardiac resynchronisation therapy (CRT) is currently restricted to those patients with a QRS duration >120 ms. We hypothesised that CRT would result in left ventricular reverse remodelling in patients with left ventricular systolic dysfunction, a normal QRS duration, and no evidence of significant inter- or intraventricular dysynchrony according to current echocardiographic criteria.
Patients and Methods: Eighteen patients with a left ventricular ejection fraction (LVEF) ⩽35% (6 with non-ischaemic dilated cardiomyopathy (DCM) and 12 with ischaemic cardiomyopathy), in sinus rhythm, and with no evidence of inter- or intraventricular conduction delay on both ECG (QRS duration <120 ms) and echocardiography (12-segment standard deviation dysynchrony index <32 and Qp-Qa duration <40 ms) were randomised to active biventricular pacing (n = 10) versus inactive pacing (VVI at 40 beats/min) (n = 8). Echocardiographic measures were compared before implantation and after 3 months of active biventricular pacing.
Results: At baseline there were no significant differences between the active and inactive pacing groups with regard to LVEF (26.5±5.52 vs 26.5±4.75%; p = 1.00), left ventricular end-diastolic diameter (3.47±0.36 vs 3.14±0.48 cm; p = 0.11), or MR jet area (5.72±7.04 vs 2.90±4.87; p = 0.33). LVEF was significantly increased in the active pacing group compared with a decrease in the inactive pacing group after three months (+4.6±7.08 vs −4.38±6.82; p = 0.002). A decrease in LVEDd was seen in the active group compared with the inactive group (−0.29 ±0.25 vs +0.121 ±0.26; p = 0.004), associated with a decrease in the MR jet area (−2.45 ±3.14 vs +0.56 ±1.36; p = 0.02).
Conclusion: Cardiac resynchronisation therapy in patients without significant dysynchrony results in left ventricular reverse remodelling after 3 months of active pacing. It appears that resynchronisation is not the only mechanism by which remodelling may occur with CRT. ECG and echocardiographic indices of dysynchrony are therefore potentially inaccurate tools upon which to select patients for CRT.
heart failure; cardiac resynchronisation therapy; ventricular reverse remodelling
099 MEDIUM-TERM ECHOCARDIOGRAPHIC ASSESSMENT OF HEART FAILURE PATIENTS IMPLANTED WITH AN AXIAL FLOW LVAD
X. Jin1, S. Westaby1, J. Pepper2, P. Poole-Wilson2, A. Banning1. 1John Radcliffe Hospital, Oxford, UK; 2Royal Brompton Hospital, London, UK
Background: Using axial flow LVADs in treating heart failure patients has achieved promising early clinical results. The aim of this study was to assess medium-term performance of the Jarvik Flowmaker LVAD in heart failure patients with respect to cardiac and valvular remodelling, systemic vascular hemodynamics and LVAD response to pump speed changes.
Methods: Five patients (all males, mean age 61 (6) years) with end-stage non-ischaemic DCM received a Jarvik Flowmaker LVAD, and were prospectively studied by Doppler echocardiography before, then 4, 16 and 45 months after the operation. Systemic BP, HR, LV cavity size, geometry (T/R ratio), LV EF and filling time, and MR and AR degree were all measured. LIMA flow velocity time integral (LIMA-VTI) and LVAD outlet graft flow VTI (LVAD-VTI) were also quantified at different pump speed settings.
Results: The mean echo follow-up was 30 (16) months, and LVAD’s speed setting was on 10K rpm at rest and during baseline echo study. Clinically, all patients had improvement in NYHA class (from IV to I-II). Throughout the post-op follow-up, HR, BP, LV ESD, T/R, LVEF, LA diameter and MR degree did not differ from pre-LVAD implant (all p>0.05). LV EDD, LV SVI and AR degree however increased after LVAD implant and was correlated to follow up time (r = 0.65, 0.52, 0.45; p = 0.0001, 0.006, 0.028). LIMA-VTI increased significantly after LVAD implant, while LVAD-VTI remained unchanged postoperatively. By verifying pump speed from 8K to 12K rpm, we found that the setting of 10K rpm produced most physiological systemic BP and LIMA flow profiles. LVAD regurgitation during its power being switched off accounted for 10–15% of its normal forward flow.
Conclusion: In this medium-term study, the axial flow LVAD consistently improves cardiac output, systemic circulation perfusion and relieves clinical symptoms in heart failure patients. Pulsatile systemic blood flow and pressure can be achieved with an axial flow LVAD when LV contraction results in partial aortic valve opening. Assessing LIMA and LVAD flow velocity profiles at different pump speeds helps defining LVAD performance and appropriate setting. The adverse cardiac remodelling due to DCM appears to be halted by axial flow LVAD. One year after LVAD support, however, there is a gradual increase in AR and LV cavity size. Their clinical implications for patients’ long-term outcome remain to be determined.
cardiac assist device; heart failure; echocardiography
100 COMMON ABNORMALITIES OF INSULIN ACTION IN PATIENTS WITH DIABETES AND HEART FAILURE
S. Cook1, T. Khan1, M. Mongillo1, L. Leccisotti1, N. Strickland1, A. Rosenzweig2, P. Punjabi1, P. Camici1. 1Imperial College, London, UK; 2Harvard University, Boston, USA
Background: Whole body and myocardial insulin resistance occur in both heart failure and type 2 diabetes mellitus (T2DM), which are diseases of interrelated pathophysiology that are of pandemic proportions. Decreased skeletal muscle insulin receptor substrate-1 (IRS-1) tyrosine phosphorylation and associated signalling contributes to insulin resistance in T2DM. The molecular basis of myocardial or whole body insulin resistance in heart failure is unknown.
Methods: We measured whole body and myocardial insulin resistance in vivo in patients with normal ventricular function with or without T2DM and in patients with heart failure using a hyperinsulinaemic-euglycaemic clamp combined with positron emission tomography approach. We determined IRS-1 expression, IRS-1 phosphotyrosine content and IRS-1-associated phosphatidylinositol 3-kinase (PI3K) activity in MRI-guided, full thickness myocardial biopsies and in skeletal muscle samples.
Results: Glucose use was reduced in patients with heart failure or T2DM at the whole body level (32%, p = 0.002 and 50%, p = 0.001 respectively) and in the myocardium (27%, p = 0.006; 28%, p = 0.02 respectively) as compared to the control group who had normal ventricular function in the absence of T2DM. At the molecular level, IRS-1-associated PI3K activity was higher in myocardial biopsies from patients with heart failure (80%, p = 0.02) or T2DM (170%, p<0.001) as compared to controls. This activity negatively correlated (r = −0.81, p<0.001) with whole body glucose uptake across the study population. Furthermore, insulin receptor phosphorylation and physical association of the insulin receptor with IRS1 (markers of activated insulin signalling) were both elevated in patients with heart failure or T2DM as compared to controls. We expanded on these observations in a comparative study in a mouse model of obesity and diabetes and observed similar activation of myocardial IRS1-PI3K activity in insulin resistant mice as compared to littermate controls (p = 0.009). In human skeletal muscle biopsies, IRS-1 phosphotyrosine content was reduced in patients with heart failure (48%, p = 0.001) or T2DM (53%, p<0.001) as compared to controls.
Conclusions: Heart failure and T2DM have common abnormalities of insulin signalling. This may form the molecular basis of the pathophysiological interrelationship between these conditions. Treating whole body insulin resistance may be beneficial in heart failure.
insulin resistance; diabetes; insulin receptor substrate-1
101 THE RISK ASSOCIATED WITH DIABETES MELLITUS IN PATIENTS WITH PRESERVED AND LOW EJECTION FRACTION HEART FAILURE. AN ANALYSIS OF THE CANDESARTAN IN HEART FAILURE: ASSESSMENT OF REDUCTION IN MORTALITY AND MORBIDITY PROGRAMME
M. MacDonald1, F. Varyani2, J. Carlsson3, M. Petrie1, J. Ostergren4, E. Michelson5, S. Solomon6, C. Granger7, K. Swedberg8, M. Pfeffer6, S. Yusuf9, J. McMurray2. 1Glasgow Royal Infirmary, Glasgow, UK; 2Western Infirmary, Glasgow, UK; 3AstraZeneca, Molndal, Sweden; 4Karolinska Hospital, Stockholm, Sweden; 5AstraZeneca, Wilmington, USA; 6Brigham & Women’s Hospital, Boston, USA; 7Duke University Medical Center, Durham, USA; 8Sahlgrenska University Hospital, Goteborg, Sweden; 9HGM-McMaster Clinic, Hamilton, Canada
Introduction: Diabetic patients with low ejection fraction (EF) heart failure (HF) have an increased risk of death compared to non-diabetic patients. The risk associated with diabetes in patients with HF and a preserved EF (PEF), compared to low EF, HF is unknown and has now been examined in the Candesartan in Heart failure: Assessment of Reduction in Mortality and morbidity (CHARM) programme.
Methods: The programme had three component trials: CHARM-Alternative (EF <40%, ACE-I intolerant, n = 2028), -Added (EF <40%, ACE-I treated, n = 2548) and -Preserved (EF >40%, n = 3023). The primary outcomes of the component trials (cardiovascular (CV) death or HF hospitalisation) and overall programme (all-cause mortality), were evaluated in diabetic and non-diabetic patients. Comparison of the outcomes in these two groups is expressed as a hazard ratio (HR) adjusted for the 33 most important prognostic covariates.
Results: At baseline 29% (n = 1306) of low EF and 28% (n = 857) of PEF patients had diabetes. Diabetes was an important independent predictor of outcome in both types of HF. In low EF patients, CV death or HF hospitalisation occurred in 50% of diabetics and 34% of non-diabetics—adjusted HR 1.6 (1.44 to 1.77). In PEF patients, these proportions were 36% and 18%, respectively—adjusted HR 2.0 (1.70 to 2.36). For death, the proportions in low EF patients were 38% and 26%, respectively, adjusted HR 1.55 (1.38 to 1.74) and in PEF patients they were 22% and 14% HR 1.84 (1.51 to 2.26). For the outcome of CV death or HF hospitalization, the patient group-diabetes interaction p value was 0.0009 (ie diabetes was associated with a significantly greater risk in PEF patients than in low EF patients). The interaction p value for death alone was 0.51.
Conclusions: Diabetes is associated with a higher risk of adverse outcomes in patients with both low and preserved EF HF. The magnitude of the increase in risk associated with diabetes is at least as great in patients with PEF.
heart failure; diabetes; risk
102 IRON METABOLISM IS IMPAIRED IN HEART FAILURE IRRESPECTIVE OF HAEMOGLOBIN CONCENTRATION AND LEFT VENTRICULAR EJECTION FRACTION
C. Murphy1, E. Lundmark2, E. Fitzsimons3, A. Jardine3, N. Sattar3, J. McMurray1. 1Glasgow Cardiovascular Research Centre, Glasgow, UK; 2Western Infirmary, Glasgow, UK; 3University of Glasgow, Glasgow, UK
Introduction: Anaemia is associated with increased morbidity and mortality in heart failure (HF) and is often due to abnormal iron metabolism. Iron status has been described in anaemic patients with HF, but not in non-anaemic patients with HF. Assessment of iron status in all patients with HF may identify those patients at risk of developing anaemia.
Abstract 102
Methods: We measured left ventricular ejection fraction (LVEF performed using Simpson’s biplane technique), serum iron (μmol/l), transferrin saturation (Tsat%), ferritin (ng/ml) and haemoglobin (Hb g/dl) concentration in 110 consecutive consenting patients hospitalised with HF. Anaemia was defined as Hb <13 in men and <12 in women (World Health Organization (WHO) criteria). A low Tsat was defined as <16%, that is, below the population reference range.
Results: The mean age of the cohort was 72 years, 50% were male, 54% were anaemic by WHO criteria, 76% had reduced LVEF (EF <50%) and 24% had preserved LVEF. Almost three quarters of anaemic and two thirds of non-anaemic patients had a low Tsat. In all patient categories, Tsat and mean iron levels were low despite ferritin levels being normal or elevated, that is, reduced iron supply to the bone marrow and tissues (see table).
Conclusions/implications: Iron metabolism appears to be impaired in HF, irrespective of Hb concentration and LVEF. Assessment of iron status in all HF patients may identify, earlier, those at risk of developing anaemia and the risk of developing anaemia might be reduced by iron supplementation. These findings have potentially important clinical implications and this hypothesis requires prospective testing.
heart failure; anaemia; iron metabolism
103 EFFECT OF INTRAVENOUS IRON SUCROSE ON EXERCISE TOLERANCE IN ANAEMIC AND NON-ANAEMIC PATIENTS WITH SYMPTOMATIC CHRONIC HEART FAILURE AND IRON DEFICIENCY (FERRIC-HF): A RANDOMISED, CONTROLLED, OBSERVER-BLINDED TRIAL
D. Okonko1, A. Greszlo2, T. Witkowski2, A. Mandal3, R. Slater3, M. Roughton1, G. Foldes1, W. Banasiak2, C. Missouris3, P. Poole-Wilson1, S. Anker4, P. Ponikowski2. 1Clinical Cardiology, NHLI, Imperial College London, London, UK; 2Cardiac Department, Military Hospital, Wroclaw, Poland; 3Department of Cardiology, Wexham Park Hospital, Slough, UK; 4Department of Cardiology, Charité Campus Virchow-Klinikum, Berlin, Germany
Background: Iron deficiency anaemia is common in patients with chronic heart failure (CHF) and associated with exercise intolerance. Iron deficiency may diminish exercise performance even in the absence of anaemia. We tested the hypothesis that intravenous (iv) iron supplementation would safely improve exercise tolerance in anaemic and non-anaemic iron deficient CHF patients.
Methods: We randomly assigned 35 patients with CHF (age 64 (13) years, 25 male, peak oxygen consumption (pVO2)/kg 14.0 (2.7) ml/min/kg, NYHA class II (n = 18)/III (n = 17), LVEF 30 (7)% (all <45%)) and iron deficiency (ferritin <100 ng/ml or ferritin 100–300 ng/ml with transferrin saturations (TSAT) <20%) to 16 weeks of iv iron or no treatment in a 2:1 ratio. Randomisation was stratified according to haemoglobin (Hb) levels (<12.5 g/dl vs 12.5–14.5 g/dl) and centre. Treatment comprised of 200 mg iv iron sucrose weekly until iron repletion (repletion dose = weight (kg) × 2.4 × (15 - Hb (g/dl)) + 500 mg) and 200 mg monthly thereafter. The observer-blinded primary endpoint was the change in absolute pVO2 from baseline to end of study.
Results: The difference (95% CI) in the mean changes from baseline to end of study between iv iron and control groups was 273 ng/ml (151 to 396) for ferritin (p<0.001), 11% (5 to 17) for TSAT (p = 0.001), 0.1 g/dl (−0.8 to 0.9) for Hb (p = 0.9), 96 ml/min (−12 to 205) for absolute pVO2 (p = 0.08), 2.2 ml/kg/min (0.5 to 4.0) for pVO2/kg (p = 0.01), 60 sec (−6 to 126) for treadmill exercise duration (p = 0.08), −0.6 (−0.9 to −0.2) for NYHA class (p = 0.007), and 1.7 (0.7,2.6) for patient global assessment (p = 0.002). In the anaemic subgroup, the difference in the mean changes between iv iron (n = 12) and control (n = 6) groups was 204 ml/min (31 to 378) for absolute pVO2 (p = 0.02), 3.9 ml/kg/min (1.1 to 6.8) for pVO2/kg (p = 0.01) and 42 sec (−66 to 153) for exercise duration (p = 0.4). Increments in peak VO2 were related to increases in TSAT (r = 0.75, p = 0.002), a marker of iron supply to aerobic enzymes, but not to Hb levels (r = 0.23, p = 0.34). In the non-anaemic subgroup, iv iron improved exercise duration (83 sec (−3 to 169), p = 0.06) and NYHA class (p = 0.06). The incidence of adverse events did not differ between the treatment arms (p = 0.6).
Conclusions: Iron repletion with intravenous iron sucrose was safe and associated with improvements in exercise capacity and symptoms in CHF patients with iron deficiency. Benefits were more evident in anaemic patients. Functional benefits appear to have been derived from an increase in oxygen utilisation and not oxygen delivery.
heart failure; iron deficiency; exercise
104 HEART TRANSPLANTATION IN THE CURRENT ERA: A 10-YEAR PERSPECTIVE
I. Hamour, F. Omar, M. Panicker, R. Banerjee, A. Mitchell, A. Khaghani, G. Dreyfus, N. Banner. The Royal Brompton and Harefield NHS Trust, Harefield Hospital, Harefield, UK
Introduction: Heart transplantation has become accepted as the standard treatment for advanced heart failure; however outcomes with medical therapy have improved and alternative surgical treatments for heart failure are becoming available. We examined the outcome of heart transplantation with current immunosuppressive therapy to determine its role in the current management of advanced heart failure.
Methods: We analysed the outcome of 355 patients who underwent a first orthotopic heart transplantation (HTx) at our centre between January 1995 and January 2005. There were 284 males (80%); the mean age was 48 (range 18–71). Ischaemic heart disease was the indication for HTx in 167 (47%) and dilated cardiomyopathy in 147 (41%). 21% (n = 76) required inotropic support prior to HTx, 9.6% (34) had an intra-aortic balloon pump (IABP) and 8.2% (29) had a ventricular assist device (VAD).All patients received ciclosporin and corticosteroids, with or without rabbit anti-thymocye globulin induction therapy and with either azathioprine or mycophenolate mofetil.
Results: Actuarial patient survival was 87% at 30 days, 79% at 1 year, 77% at 3 years, 74% at 5 years and 64% at 10 years. Conditional survival beyond 30 days was 91% at 1 year, 86% at 5 years and 74% at 10 years. A Cox analysis indicated that survival has improved during the 10 year period, p = 0.01. Actuarial survival was similar regardless of the severity of heart failure (NYHA class 3 and 4, pre-transplant inotropic support, IABP or VAD, p = NS). The cumulative incidence of cardiac allograft vasculopathy (Costanzo grades moderate and severe) was 3% at 3 years, 7% at 5 years and 20% at 10 years with a 12% cumulative probability of requiring a percutaneous coronary intervention by 10 years. Graft function was preserved with a mean left ventricular ejection fraction of 74 (SD 6)% at 1-year, 75 (7)% at 5 years and 75 (4)% at 10 years. The cumulative incidence of all malignancies by 10 years was 22%, of non-skin malignancies 15% and post-transplant lymphoproliferative diseases 3%. The cumulative probability of developing chronic kidney disease with an (MDRD) eGFR <45 ml/min per 1.73 m2 was 45.5% at 1 year, 71% at 5 years, 75% at 7 years and 83.3% at 10 years with a 12% cumulative incidence of the need for renal replacement therapy.
Conclusions: Heart transplantation provided excellent long-term survival for patients with advance heart failure and the outcome was independent of the severity of heart failure. Long-term survival has continued to improve and exceeded that reported by the International Society of Heart and Lung Transplantation Registry at 10 years. The incidence of cardiac allograft vasculopathy was lower than previously reported and left ventricular function was well preserved; however the incidence of chronic kidney disease and of malignancy remains a cause for concern. These results provide a yardstick to judge newer therapies for advanced heart failure.
heart transplantation; survival; cardiac allograft vasculopathy
105 THE CHANGING RISK:BENEFIT RATIO OF ENDOMYOCARDIAL BIOPSIES WITH IMPROVED IMMUNOSUPPRESSION AFTER HEART TRANSPLANTATION
I. Hamour, M. Panicker, R. Banerjee, A. Bell, M. Burke, N. Banner. The Royal Brompton and Harefield NHS Trust, Harefield Hospital, Harefield, Middlesex, UK
Introduction: Acute cardiac allograft rejection, detected mainly by endomyocardial biopsy, is an important cause for allograft dysfunction. Routine surveillance endomyocardial biopsy (EMBx) protocols are used by most centres and became standardised in an earlier era of immunosuppression. We analysed the yield of such a protocol with azathioprine (AZA) or mycophenolate mofetil (MMF) immunosuppression (MMF has been shown to provide more effective immunosuppression).
Methods: We studied 258 heart transplantation recipients (207 (80%) male; mean age 50 years (range 18–68)) comparing 135 patients immunosuppressed by MMF (August 2000–August 2005) with 123 patients treated by AZA (August 1997–July 2000). Both were given in combination with ciclosporin (Neoral) and corticosteroids after induction therapy with rabbit antithymocyte globulin. Fifteen routine EMBx were scheduled per patient in the first year after transplantation. Additional EMBx were performed for suspected rejection, following treatment of rejection or inadequate samples. The MMF group had 1875 EMBx performed within the first year of transplantation vs 1854 in the AZA group. Actuarial survival was 81.5% MMF vs 80.5% AZA at 1 year.
Results: The yield of ISHLT grade >3a (2R) biopsy-proven acute rejection (BPAR) within the first year of transplantation was 37 (1.9% of biopsies) MMF vs 56 (3%) AZA. In the MMF group 26.8% (n = 11) of BPAR were symptomatic vs 33.3% (23) in the AZA group. The proportion of biopsies leading to treatment for rejection was less in the MMF group 3.6% (65) vs 4.4% (82) by 1 year. Patients who experiencing BPAR episodes within the first 90 days post-transplantation were at a significantly increased risk of further rejection during the first year, p = 0.002, although the incidence was lower for the MMF group 31% (5), p = 0.11 vs AZA 36% (9), p = 0.008. The number of asymptomatic BPAR that lead to change in treatment (the true yield of routine surveillance) were 30 (1.6% of biopsies) MMF vs 46 (2.5%) AZA, p = 0.48. Symptomatic low-grade rejection episodes (ISHLT grade <3a) were similar in the two groups 21 (1.1% of biopsies) MMF vs 22 (1.2%) AZA, p = 0.8. The incidence of any complication per biopsy was 1.1% (42). However, the total number of patients experiencing a complication within 1 year was 16.2%. The number of serious complications requiring intervention or with long-term sequelae was only 0.13% (5) per patient. There was no biopsy-related mortality.
Conclusions: The yield of BPAR per biopsy was low in the AZA group (3%) and even lower in the MMF group (1.9%). The overall incidence of complications and serious complications per EMBx was low, however repeated biopsies led to a higher rate of (usually minor) complication per patient. The role of protocol driven routine surveillance EMBx should be re-evaluated in the light of their low yield under current immunosuppressive therapy.
heart transplantation; endomyocardial biopsies; immunosuppression
106 THE ROLE OF SECONDARY PREVENTION STRATEGIES IN PATIENTS WITH DIABETES MELLITUS SUSTAINING AN ACUTE CORONARY SYNDROME: TIME FOR A CRITICAL REAPPRAISAL?
R. Cubbon1, A. Rajwani1, P. Grant1, S. Wheatcroft1, J. Barth2, M. Kearney1, A. Hall1. 1The University of Leeds, Leeds, UK; 2Leeds General Infirmary, Leeds, UK
Background: Much of the well-documented improvements in outcome after acute coronary syndrome (ACS) relate to the increased use of evidence based therapies such as; HMGCoA reductase inhibitors (statins), beta-adrenoceptor antagonists, angiotensin converting enzyme inhibitors (ACEI) and aspirin. The pharmacologic effects of aspirin however, may be impaired in patients with diabetes mellitus, moreover some studies have linked in vitro aspirin resistance to poor outcome after ACS. We aimed to assess the prognostic importance of aspirin, and other commonly prescribed secondary prevention agents, in patients with and without diabetes mellitus who have suffered from an ACS.
Methods: Retrospective analysis of data from the EMMACE-II (Evaluation of Methods and Management of Acute Coronary Events) prospective cohort study. Analysis included 1851 patients (1530 no DM; 321 DM) with confirmed ACS admitted to 11 UK hospitals. Cox proportional hazards multivariable analysis was performed to assess the impact of aspirin, statins, ACEI and beta-adrenoceptor antagonists on two year all cause mortality. Other variables entered into the analysis to account for baseline health included age, gender, background heart failure, renal impairment and cardiovascular disease. The risk of the index event was reflected by variables denoting ST elevation ACS and troponin I elevation (>0.05 ng/ml); treatment factors including reperfusion and early revascularisation were also included.
Results: The provision of statins, ACEI and beta-adrenoceptor antagonists resulted in similar hazard reductions in groups with and without DM (fig); interaction terms between these agents and diabetes status did not reach statistical significance. Conversely, aspirin use in patients with DM was not associated with a significant improvement in outcome (Hazard ratio 0.83 (95% CI 0.54 to 1.27) p = 0.385), contrasting with the non-diabetic group (Hazard ratio 0.48 (95% CI 0.39 to 0.60) p<0.001). Diabetes status and aspirin use interacted strongly (p<0.001) indicating patients with diabetes derived less hazard reduction from aspirin than patients without diabetes.
Conclusions: In patients with DM aspirin use does not appear to afford a beneficial effect on survival, contrasting with the favourable effects of other secondary prevention agents in this group. Further observational and pharmacological studies in patients with diabetes suffering an ACS are required.
Acknowledgements: Dr Cubbon is supported by a British Heart Foundation Clinical PhD Studentship.
acute coronary syndrome; diabetes; secondary prevention
107 IMPAIRED GLUCOSE TOLERANCE IS ASSOCIATED WITH ENDOTHELIAL DAMAGE FOLLOWING ACUTE MYOCARDIAL INFARCTION
S. Jessani, T. Millane, G. Lip. City Hospital, Birmingham, UK
Introduction: Impaired glucose tolerance (IGT) is commonly associated with cardiovascular disease. Whereas diabetes mellitus (DM) is sought and treated, IGT is largely ignored despite evidence of poorer clinical outcome in such patients. We hypothesised that endothelial damage following acute myocardial infarction (AMI), as measured by a rise in circulating endothelial cells (CECs), would be more pronounced in patients with IGT compared to those with normal glucose tolerance (NGT).
Abstract 107 CECs by glycaemic status
Method: Consecutive non-diabetic patients presenting with AMI underwent standard oral glucose tolerance testing (OGTT) 3–5 days after admission. We established existing endothelial cell damage as assessed by CECs count in the fasting state, and investigated the effect on the endothelium of a 75 g glucose load. CEC counts were quantified using CD146/immunobead capture methodology.
Results: Seventy nine patients (mean (SD) age 60 (12.8) years; 67 (85%) male) were studied. Baseline median CEC count was higher in patients with impaired glucose tolerance versus those with normal glucose tolerance (p<0.001) (table). The increase (Δ) in CECs in response to the glucose load correlated with the increase (Δ) in plasma glucose levels (Spearman, r = 0.37, p<0.001). At baseline, median (IQR) CEC count was significantly higher in patients with HbA1c >6.5% versus normal [(11 (9–15) vs 7 (5–9)); p<0.05).
Conclusion: We have demonstrated, using circulating endothelial cell counts, that impaired glucose tolerance after acute myocardial infarction is associated with significant endothelial damage when compared with normal glucose tolerance. Further endothelial cell damage appeared to occur in response to a rise in plasma glucose levels. Interestingly, the degree of endothelial damage in subjects with impaired glucose tolerance appears comparable to that observed in frank diabetes. IGT is not currently actively sought in this population, let alone treated. Is a change in practice due?
impaired glucose tolerance; acute myocardial infarction; endothelial damage
108 THROMBOGENICITY IN TYPE 2 DIABETES AND CORONARY ARTERY DISEASE
A. Natarajan1, S. Marshall2, J. Badimon3, A. Zaman4. 1Newcastle University and Freeman Hospital, Newcastle upon Tyne, UK; 2Newcastle University, Newcastle upon Tyne, UK; 3Mount Sinai School of Medicine, New York, USA; 4Freeman Hospital, Newcastle upon Tyne, UK
Background: Patients with type 2 diabetes mellitus (T2DM) and coronary artery disease (CAD) die predominantly of thrombotic events. The procoagulant nature associated with these conditions may be contributory. Ex vivo thrombogenicity in patients with T2DM, with and without CAD, treated with aspirin, has not been compared previously.
Abstract 108 All results presented as mean (SD) or median (range)
Methods: Eighty one patients in four groups were studied: (1) T2DM and established CAD (n = 23), (2) T2DM without clinically evident macrovascular disease (n = 20), (3) established CAD without diabetes (n = 21) and (4) control subjects with neither diabetes nor clinical macrovascular disease (n = 17). All patients were on 75 mg daily aspirin and were nonsmokers. All apart from control subjects were on statins. Non-anticoagulated venous blood flowed through an ex vivo arterial injury model (Badimon chamber) at high shear rates (1690/s). Porcine aortic media was the thrombogenic substrate used in the chamber. After blood perfusion, thrombus laden media were fixed, mounted and stained. Thrombus images were digitised and thrombus areas calculated by computerised planimetry using Image-Pro Plus software.
Results: One-way analysis of variance (ANOVA) demonstrated a significant difference between the thrombus areas in the four groups (p = 0.012). In post hoc analysis with Bonferroni adjustment, the greatest difference was found between patients with T2DM plus CAD and control subjects (p = 0.007).
Conclusions: Blood thrombogenicity is increased in patients with T2DM who have clinically established CAD despite therapeutic doses of aspirin and statin use. This may contribute to the increased incidence of atherothrombotic events in them. Further research into potent yet safe antithrombotic agents is needed in this high-risk group of patients.
thrombogenicity; type 2 diabetes; coronary artery disease
109 ELEVATED NEOPTERIN AFTER ACUTE CORONARY SYNDROME PREDICTS LONG-TERM RISK OF DEATH OR NON-FATAL CORONARY EVENTS: ANALYSIS FROM PROVE IT-TIMI 22
K. Ray1, D. Morrow1, C. Cannon1, M. Sabatine1, A. Shui2, E. Braunwald1. 1Harvard Medical School, Boston, USA; 2Brigham and Women’s Hospital, Boston, US
Background: We assessed the long-term prognostic value of neopterin (a marker of monocyte activation) in acute coronary syndrome (ACS) patients in the PROVE IT-TIMI 22 trial, which randomised patients to intensive vs standard statin therapy.
Methods: Plasma neopterin levels were measured at 7 days (n = 3946) and at 4 months (n = 3369) after ACS. The relation between neopterin and risk of death or acute coronary events (non-fatal myocardial infarction or unstable angina) over 2 years was assessed using a Cox proportional hazards model.
Results: Within individuals neopterin levels were remarkably stable over 2 years (intraclass correlation 0.6). At 7 days after ACS, neopterin levels ⩾75th percentile (⩾12.11 nmol/l) were associated with an increased risk of death or acute coronary events (p = 0.006) independent of traditional risk factors, LDL-C, hsCRP and statin regimen. Similarly, at 4 months a neopterin level ⩾12.11 nmol/l independently predicted the risk of death or an acute coronary event (HR 1.60, 95% CI 1.21 to 2.11, p = 0.001) (fig 1) Both among subjects who either achieved or failed to achieve the dual goal of LDL <1.8 mmol/l and CRP<2 mg/l, neopterin levels ⩾12.11 nmol/l identified individuals at increased risk of adverse events (fig 2).
Conclusions: We provide evidence that increased levels of neopterin independently predict long-term risk in ACS patients, supporting a potentially important biological role of monocyte activation in the pathogenesis of ACS.
acute coronary syndrome; monocyte activation; prognosis
110 COST EFFECTIVENESS OF EZETIMIBE CO-ADMINISTRATION VS DOUBLING STATIN DOSE IN PATIENTS NOT AT CHOLESTEROL TARGETS ON STATIN MONOTHERAPY IN THE UK
A. Brady1, G. Davies2, H. Urdahl3, D. Yin4, E. Alemao4, J. Cook2. 1Department of Medical Cardiology, Glasgow Royal Infirmary, Glasgow, UK; 2Health Economics Statistics, Merck and Co, Upper Gwynedd, PA, USA; 3Outcomes Research, MSD, Hoddesdon, Hertfordshire, UK; 4Outcomes Research, Merck and Co, Whitehouse Station, USA
Background: Recent guidance on the use of statins published by the National Institute for Health and Clinical Excellence (NICE) recommends use of statins in adults with cardiovascular disease (CVD) and in adults without existing CHD who have a 20% or greater 10-year risk of developing CVD. Guidelines from professional organisations in recent years have recommended increasingly lower cholesterol targets for treatment. Statins are the foundation of pharmacological therapy for hypercholesterolaemia. However, many patients who do not reach target on their initial statin dose still do not reach targets after doubling the statin dose, because of the poor dose response curve to statins. Doubling the dose of statin lowers total cholesterol (TC) by about 5%–6%. Clinical studies have demonstrated that co-administration of ezetimibe to statins in patients not at target provides substantially greater reduction in cholesterol compared to doubling of the statin dose. Addition of ezetimibe to a statin lowers TC by approximately an additional 18% (LDL-C 22%).
Objective: To assess the cost effectiveness of co-administering ezetimibe 10 mg to statins in patients not at target (TC <4.0 mmol/l) while on statin monotherapy compared to doubling the statin dose.
Method: A validated and peer-reviewed decision-analytic model was used to estimate the cost effectiveness of ezetimibe co-administration with statin. The risk of CVD events was estimated using the UK Prospective Diabetes Study (UKPDS) for patients with diabetes and the Framingham Heart Study for patients with CVD. Non-CHD mortality was based on UK survival rates by age and gender. Health-related quality of life weight estimates and cost of treating CV events were taken from the NICE statin guidance. Statin cost was weighted based on current usage in the UK. The impact of ezetimibe and statin titration on change in cholesterol profile were based on a systematic literature review and meta-analysis of published randomised controlled trials (RCTs). The cost per quality adjusted life years gained (QALY) were estimated for ezetimibe 10 mg co-administration versus statin titration in patients with existing CVD (with or without diabetes) and for patients with diabetes but without CVD.
Results: The table shows the range of incremental cost effectiveness ratios (ICERs) for both men and women from the two subpopulations which were studied. The ICERs from the NICE statin review are also listed.
Conclusion: Co-administration of ezetimibe with a statin in patients not at target is a cost effective alternative to statin titration regimen for most of the subgroups studied in this analysis. In particular, secondary prevention in men, and primary prevention among people with diabetes, show QALY costs well within the accepted UK limits of cost efficacy.
cost effectiveness; modelling; ezetimibe
111 MINOR TROPONIN T RISE IN NEW ONSET ATRIAL FIBRILLATION SIGNIFICANTLY INCREASES FUTURE CARDIOVASCULAR RISK
A. Dhawan, L. Ganaraj, S. Khan, I. Ahmad, J. Singh, N. Malik, P. Lewis. Stepping Hill Hospital, Stockport, UK
Introduction: The association of cardiac arrhythmias (including atrial fibrillation) with minor troponin T (TnT) rise (>0.01<0.1 ng/ml) is well recognised. This has been generally attributed to enzyme leak associated with myocardial stress induced by the arrhythmias. Quite often this minor TnT rise, in the absence of any other symptoms and signs of IHD is overlooked. We were keen to examine the clinical significance of minor TnT rise (>0.01<0.1) following admission with new onset atrial fibrillation.
Methods: We studied patients with new onset atrial fibrillation with no previous history of ischaemic heart disease, congestive cardiac failure or any structural/valvular heart disease. All patients had baseline blood tests including renal and thyroid function, an ECG on admission and TnT at 12 h after admission. All patients were followed up after discharge for major adverse cardiac events (MACE) (ischaemic death, myocardial infarction, ischaemic left ventricular failure, readmission with acute coronary syndrome, positive exercise tolerance test/Myoview scan and need for revascularisation).
Results: We studied 257 patients (141 male). 118 patients had a minor TnT rise (mean 0.0453 (SD 0.0898)) while 139 were TnT negative. Patients with TnT rise were significantly older than the TnT negative group (69.4 (SD 12.7) vs 78.2 (10.7), p<0.001). Over the median follow-up period of 894 days (range 444–1301) there were 47 MACE. Incidence of MACE was significantly higher in the TnT positive group (31/118 vs 16/139, p<0.001). Furthermore among the TnT positive group of patients who had MACE TnT rise was significantly higher as compared to those who did not have MACE (0.0842 (SD 0.168) vs 0.043 (SD 0.0255), p = 0.028). Using a multivariate binary logistic model (including age, sex of patient, renal function, log TnT and hypertension), TnT (OR 5.76, 95% CI 1.14 to 29.15, p = 0.034) was the only significant independent predictor of future MACE.
Conclusion: This study suggests that patients admitted with new onset atrial fibrillation and a minor TnT rise have an adverse cardiovascular prognosis and merit further investigation.
troponin T; atrial fibrillation; cardiovascular risk
112 TROPONIN ELEVATION IN NON-ACUTE CORONARY SYNDROMES: OXVASC DATA
A. Ryding1, L. Silver2, A. Banning1 on behalf the OXVASC study31John Radcliffe Hospital, Oxford, UK; 2OXVASC study, Radcliffe Infirmary, Oxford, UK; 3Radcliffe Infirmary, Oxford, UK
Introduction: The significance of troponin elevation in the absence of other diagnostic criteria for acute coronary syndrome (ACS) is largely unknown. This is a common problem, as troponin is increasingly used to screen patients in whom a clinical diagnosis is not initially clear. For this reason we analysed the Oxford Vascular Study (OXVASC) database to identify the frequency of non-ACS troponin elevation, and the characteristics of this population.
Methods: The OXVASC Study is a prospective epidemiological study of all acute vascular events in any arterial territory in a population of 91 106 people in Oxfordshire. Patients admitted to hospital with a possible diagnosis of ACS were identified and screened to confirm the diagnosis. Among this cohort patients with troponin I elevation (1.0 ng/ml or more (upper limit of normal 0.20 ng/ml)) were identified who did not meet the diagnostic criteria for ACS. The hospital notes of each patient were reviewed to establish an alternative diagnosis.
Results: 144 cases of non-ACS troponin elevation were identified, compared to 856 cases of ACS between 2002–5. The median age was 79 (interquartile range 72–84) and the median troponin I was 1.75 ng/ml (IQR 1.3–3.2). The underlying diagnoses were sepsis (38%), atrial arrhythmia (23%) heart failure (7%), renal failure (4%) and the remainder were accounted for by 14 other diagnostic categories. Median survival of all patients was 33 months. Survival stratified by troponin quartile did not demonstrate any significant differences, independent of age, blood pressure, heart rate, CRP or risk factors for ischaemic heart disease.
Conclusions: Non-ACS related troponin elevation is common, and associated with a wide range of conditions. In this elderly cohort overall survival is poor, irrespective of the troponin level.
troponin; epidemiology; acute coronary syndrome
113 HEART RATE LOWERING ACTION OF IVABRADINE DEPENDS ON BASELINE HEART RATE: MECHANISM OF LOW INCIDENCE OF EXCESSIVE BRADYCARDIA DURING THERAPY WITH IVABRADINE
I. Savelieva1, J. Borer2, A. Camm1. 1St George’s University of London, London, UK; 2Weill Medical College, Cornell University, New York, USA
Background: The use of heart rate (HR)-lowering drugs in patients with heart disease may be associated with the risk of excessive bradycardia leading to hypotension, exacerbation of angina and arrhythmias. Ivabradine is a novel pure HR-lowering agent developed for treatment of stable coronary artery disease (CAD). The mechanism of action is selective inhibition of the pacemaker If current in the sinoatrial cells which is associated with prolongation of the slow diastolic depolarisation phase of the action potetntial and the subsequent decrease in heart rate. Binding of ivabradine to f-channels is restricted to open channel state, which is characterised by the profound autonomic responsiveness. In vitro, 100% block of the If current resulted in a reduction of the sinus node rate by 25–30%. In experiments, ivabradine produced a plateau dose-response, use-dependent effect on HR reduction implying the greater effect at faster HR.
Objectives: To investigate (1) whether HR reduction by ivabradine correlates with baseline HR in the clinical setting; and (2) whether this property of ivabradine translates into fewer adverse event reports of bradycardia compared with conventional HR-lowering drugs.
Methods: A total of 1328 patients with documented CAD and stable angina had their resting ECGs recorded at baseline and after 3–4 months of treatment with ivabradine 5, 7.5, or 10 mg bd. ECGs were read centrally by cardiologists blinded to treatment assignment.
Results: Inverse linear correlations between baseline HR and changes in HR on treatment were observed for all three doses of ivabradine (fig). Thus, the magnitude of the HR-lowering effect of ivabradine was the highest in patients with sinus tachycardia at baseline and the least in those with the lowest baseline HR, which is consistent with the known effect of HCN4 channel function modulation by the autonomic nervous system. The incidence of bradycardia <40 bpm was 0% and 0.5% in patients receiving two recommended treatment doses of 5 and 7.5 mg bd, respectively.
Conclusion: The HR-lowering effect of ivabradine is determined by HR at baseline. This property accounts for a low incidence of severe bradycardia during therapy with ivabradine.
stable coronary artery disease; antianginal drugs; heart rate lowering drugs
114 EVIDENCE FOR A STRONG ANTIARRHYTHMIC EFFECT OF SPIRONOLACTONE IN PATIENTS WITH CORONARY ARTERY DISEASE BUT WITHOUT HEART FAILURE
N. Shah1, P. Donnan2, S. Pringle3, A. Struthers1. 1University of Dundee/ Ninewells Hospital, Dundee, UK; 2University of Dundee, Dundee, UK; 3Ninewells Hospital, Dundee, UK
Background: Aldosterone blockade has been shown to reduce mortality and in particular sudden death in patients with heart failure. The reduction in sudden death in heart failure could be due to a reduction in arrhythmias and/or in coronary events. Whether either effect also occurs in other cardiac patients without heart failure is currently unknown. We have therefore examined whether aldosterone blockade shows favourable effects on arrhythmias or on endothelial function in patients with CAD (coronary artery disease) but without heart failure.
Method: We performed a randomised, placebo-controlled, double-blind crossover study on 98 patients with CAD but without heart failure on standard therapy, comparing 12.5–50 mg/d spironolactone (3 month) versus placebo. Endothelial function was assessed by bilateral forearm venous occlusion plethysmography using acetylcholine and sodium nitroprusside. Ventricular extrasystoles (VEs), PIIINP (procollagen III N-terminal peptide) and QT interval length were used to represent arrhythmias and their determinants. We also examined BNP and vascular ACE.
Results: Our main finding was that spironolactone produce a highly significantly 75% reduction in VEs, (median = 192, range (48–744)) on placebo compared to (median = 48, range (19.2–288)) on spironolactone, p<0.003. Spironolactone also decreased the QT interval (from mean 440 (28) to mean 425 (25), p<0.001) and a collagen marker (PIIINP) (from mean 3.6 (0.9) to mean 3.0 (0.8), p<0.001); however spironolactone did not significantly change endothelial dysfunction, vascular ACE or heart rate variability.
Conclusions: These results suggest that spironolactone may be a highly effective antiarrhythmic agent in patients with coronary artery disease, but without heart failure. The underlying mechanism for its antiarrhythmic effect in these patients could be that it also reduces myocardial fibrosis and shortens the QT interval as well as increasing potassium.
spironolactone; arrhythmias; coronary artery disease
115 AN AUDIT OF PACING PRACTICE IN THE 33 CARDIAC NETWORKS SERVING ENGLAND AND WALES
C. Plummer1, A. Cunningham2, M. Cunningham2, R. Charles2, J. McComb1. 1Freeman Hospital, Newcastle upon Tyne, UK 2National Pacemaker and ICD Database, Central Cardiac Audit Database, London, UK
Introduction: Pacemaker implantation rates and pacing mode selection are known to vary widely between Western countries despite similar guidelines on the indications for implantation. The National Institute for Health and Clinical Excellence (NICE) published guidance on pacing mode for symptomatic bradycardia due to sick sinus syndrome (SSS) and/or atrioventricular block (AVB) in February 2005. This recommends dual chamber (DDD±R) pacing unless patients are in continuous atrial fibrillation (AF), when a ventricular (VVI±R) system is indicated, or have SSS without AVB when an atrial (AAI±R) system may be appropriate. The guidance recognises patient-specific factors which may favour VVI±R. We have audited UK pacing practice against these standards at the level of cardiac networks.
Methods: The National Pacemaker Database is part of the Central Cardiac Audit Database in the NHS Information Centre in London. It registers all pacemakers and implantable cardioverter defibrillators implanted in the UK. Data for 2003 and 2004 were cross-checked with individual pacing centres and are ⩾98% complete. The data were then analysed by individual pacing centre and the cardiac networks they serve to produce a database including all 33 networks covering all 52.9 million people in England and Wales.
Results: Age and sex corrected annual pacing rates varied between networks from 258.3 to 513.1/million and pacing for complete heart block (CHB), from 68.4 to 126.5/million. The proportion of devices implanted for CHB was negatively correlated with total pacing rate (r2 = 0.284). The mean proportion of patients receiving AAI±R devices was 1.1%, far below the proportion paced for SSS of 26.9%. A mean of 42.2% of patients received VVI±R devices while only 23.8% were in AF. A local audit demonstrated that all 35 patients in sinus rhythm (SR) receiving a VVI±R device out of a total of 134 VVI±R (26.1%) devices implanted in the year, had documented comorbidity favouring single chamber pacing. The number receiving VVI±R devices in SR in excess of this varied between 18 to 136 devices/million/year, 4.7 to 35.7% of all devices implanted in a network.
Conclusions: There are large variations in pacing practice in England and Wales which cannot be explained on clinical criteria. Some pacing centres in the UK will need to change practice significantly if they are to follow National guidance on pacing mode: A large number of patients with SSS are receiving DDD±R pacing systems when AAI±R is recommended. An even larger number in SR appear to be receiving VVI±R devices when DDD±R is recommended. This database provides a powerful audit tool to address these inconsistencies in practice.
audit; pacemakers; cardiac networks
116 LACK OF KNOWLEDGE OF PACEMAKER INDICATIONS AT THE FRONT LINE
J. McComb, C. Plummer. Freeman Hospital, Newcastle upon Tyne, UK
Introduction: The permanent pacemaker implantation rate in the UK is much lower than in comparable Western European countries. Investigation of the reasons for this suggested that failure to recognise pacemaker indications in symptomatic patients might contribute. We therefore studied physicians’ knowledge of pacemaker indications.
Method: Ten cases, with a brief clinical history and an ECG, were shown to physicians, who were asked to answer “is there a class I or IIa pacing indication?” Pacing indications were defined using the 2002 ACC/AHA pacemaker guidelines, and the answer in each case was agreed by two cardiologists. Phase 1 included validation of the cases, with 42 internal medicine physicians and 11 cardiologists. Minor adjustments were made to two of the cases as a result of this validation, and the cases were then presented to 103 internal medicine physicians and 11 other cardiologists in phase 2.
Results: In phase 1 consultant cardiologists scored a mean of 8/10 and consultant physicians (various specialties) 5.4/10. After the changes made in response to this validation, consultant cardiologists scored 8.25/10. Overall, in both phases, excluding cardiologists, there was a learning curve, foundation doctors scoring a mean of 3.5/10, senior house officers 4.5, specialist registrars 5.9 and consultants 5.9. Junior doctors (foundation and senior house officers) were therefore excluded from further comparisons, which are based on the responses of consultants and specialist registrars. In both phases, cardiologists (n = 21) scored significantly higher (8 and 8.25/10) than internal medicine physicians (5.5, n = 39) and care of the elderly physicians (5.5, n = 10). Participating in acute unselected take did not affect the results.
Conclusion: There is a learning curve, specialist registrars and consultants being more likely to recognise class I/IIa pacing indications than more junior doctors. However, despite this, internal medicine and care of the elderly physicians still frequently fail to recognise pacing indications. As the majority of our pacemaker recipients present initially to general internal medicine or to care of the elderly, this lack of knowledge among the doctors responsible for their care may contribute to patients with pacing indications not being referred to cardiology, and so to the low pacemaker implantation rate in the UK.
pacemaker; indication; guideline
117 INEQUITY OF ACCESS TO CARDIAC PACING: RESULTS OF A NATIONAL SURVEY
J. McComb1, C. Plummer1, R. Charles2, M. Cunningham2, A. Cunningham2. 1Freeman Hospital, Newcastle upon Tyne, UK; 2Central Cardiac Audit Database, London, UK
Introduction: In the years 2003 and 2004, >40 000 new pacemakers were implanted in England (population 50 million), equating to a new implantation rate of 411/million, much less than the rates in economically comparable countries in Europe, with similar population demographics. Although variation in implantation rates has been observed within the UK, and other European countries, the explanation for it is not known.
Methods: All pacemaker implantations in England are reported to the National Pacemaker Database (NPD). Registration deficits for 2003 and 2004 were checked with 120 individual pacing centres; attempts were made to recover all data from 40 284 patients, including postcodes. Data are 98% complete. Data regarding pacemaker centres were obtained from NPD; other data, including demographics, information relating to socioeconomic deprivation, mortality and provision of cardiac services were obtained from government sources. The collection of postcodes allowed attribution of each patient and pacemaker to an individual primary care trust (PCT). As the need for pacing is critically age- and sex-dependent, regional pacing rates were corrected to allow for this according to analysis of NPD and detailed demographic data for each region. Analysis of pacing rates, and factors affecting them, has been made at cardiac network and PCT level.
Results: Marked variation in pacemaker implantation rates was observed, both between and within networks. At network level, age and sex corrected implantation rates ranged from 258 to 513/million, varying by 100%. Variation was much greater at PCT level, ranging from 166 to 745/million (350%). There was no correlation with measures of socioeconomic deprivation, health, standardised mortality for coronary artery disease, provision of other cardiac procedures or number of cardiologists. There was no relation with distance from pacing centre, although larger volume pacing centres (implanting >500 new pacemakers per year) tended to provide pacing for the PCTs with higher implantation rates, and PCTs with pacing provided by low volume centres (<50 per year) tended to have low implantation rates. Single large centres providing pacing for several PCTs however did not provide uniform pacing rates, suggesting local, rather than central factors, may influence pacing rates.
Conclusion: There is marked variation in provision of pacing in England, with regional implantation rates varying by up to 350%. There is no obvious reason for this, and in contrast with other cardiac procedures, it is not related to socioeconomic deprivation. The only factor which may have an impact is the size of the centre providing pacing.
pacemaker; inequity; epidemiology
118 SAFETY OF SPIRONOLACTONE WITH ACE INHIBITORS/ANGIOTENSIN RECEPTOR BLOCKADE IN PATIENTS WITH CHRONIC KIDNEY DISEASE
N. Edwards1, R. Steeds2, C. Ferro2, J. Townend2. 1University of Birmingham, Birmingham, UK; 2University Hospital Birmingham, Birmingham, UK
Introduction: Over two thirds of patients with end stage chronic kidney disease (CKD) have “uraemic cardiomyopathy” and most will die from heart failure and sudden cardiac death. We are examining the use of aldosterone inhibition in combination with established ACE inhibitor and/or angiotensin receptor blocker (ARBs) therapy in patients with early CKD (GFR 40–80 ml/min) to prevent this cardiomyopathy. This strategy has not previously been employed in CKD due to concerns about hyperkalaemia and adverse impacts upon renal function. Before randomisation to long-term spironolactone or placebo, safety and tolerability is assessed by open-label treatment with spironolactone 25 mg once daily for 4 weeks in addition to continued ACE inhibitor or ARB. We present the results from the first 100 patients.
Methods: Potassium levels were monitored at baseline and after 1, 2 and 4 weeks of treatment. Patients were withdrawn if serious hyperkalaemia, defined as a serum concentration >6.5 mmol/l developed or if potassium was persistently >6.0 mmol/l. Patients with potassium levels between 5.5–6.0 mmol/l received spironolactone 25 mg on alternate days. Estimated GFR (eGFR ml/min, Cockroft-Gault), urinary albumin-creatinine ratio (ACR, mg/mmol) and 24-h ambulatory blood pressure (ABP) were assessed at baseline and after 4 weeks of treatment.
Results: Spironolactone treatment had no clinically significant effects on eGFR (60 (1) vs 57 (2) ml/min) or serum creatinine (133 (4) vs 138 (5) mmol/l) after 4 weeks (mean (SEM)). Serum potassium levels were increased from 4.4 (0.1) to 4.7 (0.1) (p<0.01). One patient experienced serious hyperkalaemia (6.8 mmol/l) and was uneventfully withdrawn from the study. Six patients had potassium levels between 5.5–6.0 mmol/l, returning to ⩽5.5 mmol/l on alternate day dosing. Treatment with spironolactone decreased mean ACR by 51% from 59 (16) mg/mmol to 29 (10) mg/mmol (p<0.01). Mean 24-h ABP was significantly reduced with spironolactone from a baseline 125 (1)/77 (2) mmHg to 117 (2)/71 (1) mm Hg (p<0.01) after treatment.
Conclusion: Aldosterone blockade with spironolactone, in combination with ACE inhibitor or ARBs appears to be safe in patients with mild-moderate CKD providing potassium concentration is monitored. In combination with conventional therapy, it produced a further reduction in blood pressure and a significant reduction in albuminuria.
aldosterone; chronic kidney disease; potassium
119 A 15-YEAR AUDIT OF ACUTE TYPE A AORTIC DISSECTION: HAVE THE OUTCOMES CHANGED WITH TIME?
P. Narayan, C. Rogers, M. Caputo, G. Angelini, A. Bryan. Bristol Heart Institute, Bristol, UK
Objective: To observe the change in incidence of type A aortic dissections and determine whether improvements in surgical, anaesthetic and perfusion techniques in the treatment of type A aortic dissection have resulted in improved clinical outcome.
Methods: A consecutive series of 165 repairs for type A aortic dissections carried out between April 1992 and March 2006 in a single centre were analysed. Operations were grouped according to era of surgery (before April 1999 vs from April 1999).
Abstract 119
Results: Patients operated in the later era were older (59 years (45–68) vs 62 years. (51–68), p = 0.18), with a significantly higher incidence of concomitant coronary artery disease (5 (7%) vs 13 (18%), p = 0.03)) and significantly worse (moderate to poor) left ventricular function (13 (18%) vs 33 (40%), p = 0.002). The duration of circulatory arrest was lower in the later era (37.5 min (31–45) vs 31 min (26.5–39), p = 0.009) with a higher incidence of concomitant procedures (10 (14%) vs 19 (21%), p = 0.22). Except for total hospital stay, which increased over time, there were no significant differences in post operative outcomes (table).
Conclusions: Despite the adoption of techniques to improve outcome for patients with type A dissection operative mortality remains substantial. A deteriorating risk profile and factors relating to the disease process may explain this observation.
aorta; dissections; change in era
120 CARDIOVASCULAR MORTALITY IN DIALYSIS PATIENTS
F. Vrapi1, A. Bakhai2, P. Kabunga1, J. Buscombe1, A. Davenport1, J. Coghlan1. 1Royal Free Hospital, London, UK; 2Barnet & Chase Farm and Royal Free Hospital, London, UK
Introduction: Patients on dialysis are known to have a poor prognosis; half of all patients on dialysis die within 6 years, and over 50% of deaths are cardiovascular in all registry populations. We wished to determine whether aggressive management of cardiovascular risk factors and investigation and revascularisation of coronary disease would reduce avoidable cardiac deaths.
Abstract 120
Methods: We analysed a cohort of 502 patients starting dialysis between 1997 and 2002. The policy of the unit was to identify and manage optimally all cardiac risk factors and to investigate possible coronary disease in patients likely to benefit from intervention. Duration of follow-up was calculated from first dialysis, to death, transplantation or last review/dialysis session, patients have been followed for an average of 3.3 years. None was lost to follow-up, deaths were classified from death certification, and in addition deaths at home and deaths of unknown mode were treated as cardiac. Stepwise multivariable analysis was used to determine the impact of coronary risk factors on survival and likelihood of cardiovascular mortality.
Results: The median age of the population was 66 years (Q1 49: Q3 77), 327 were male. Mortality in this population remains high with an 83% one-year survival and a 55% five-year survival. The mean age at death was 72 years, while the average age of survivors was 55 years. During follow-up there were 210 deaths, the largest single cause was cardiovascular disease (93) with an annual cardiac mortality of 5% (graph 1), followed by sepsis (49) and “other” mainly withdrawal of treatment (45). The annual non-cardiac mortality was 6%. Younger age, transplantation and male sex were independent predictors of survival. Dyslipidemia (cholesterol >5), diabetes, hypertension and the presence of proven coronary disease did not independently predict total or cardiovascular mortality. The impact of age on survival is evident from graph 2, showing the Kaplein–Meier survival curves for the age categories <55, 56–65, 66–80 and 80+ years.
Conclusion: In a well-managed dialysis population, cardiovascular mortality falls below 50%, and is now in line with the general increase in mortality seen in this population. Traditional risk factors no longer predict cardiovascular mortality, suggesting that with management their impact has been neutralised. Sepsis remains the dominant contributor to avoidable mortality in the dialysis population in 2006.
dialysis; mortality; risk
121 DOES THE LEVINE SIGN AID DIAGNOSIS OF ANGINA IN A RAPID-ACCESS CHEST PAIN CLINIC?
S. Wheeler, A. Halliday, N. West. Gloucestershire Hospitals NHS Foundation Trust, Gloucester, UK
Introduction: Levine’s sign (a clenched fist held to the chest) has historically been used to aid differentiation of anginal from non-cardiac chest pain. A previous study examined the utility of this sign to discriminate between cardiac and non-cardiac pain in a population of patients admitted to a coronary care setting; the authors found Levine sign-type hand gestures had a positive predictive value of 77% for an exit diagnosis of ischaemic heart disease, with sensitivity 49% and specificity 80%. Rapid access chest pain clinics (RACPC) triage large numbers of patients with relatively-undifferentiated chest discomfort and utility of the Levine sign as discriminator in this setting has not been tested.
Methods: Consecutive patients presenting to a specialist nurse-led RACPC between June and November 2006 (n = 480) were screened; demographic data, description of chest pain quality/location, exercise test data and exit diagnosis/management plan were recorded on a dedicated database.
Results: Of the study population, 119/480 (25%) described their chest pain with the aid of a hand gesture (L+). Comparisons of demographic data between L+ and non-gesturing (L-) patients, including age, sex, ethnicity and both individual and total number of conventional risk factors revealed no significant differences. 131/480 (27%) patients were given a clinical diagnosis of angina before exercise stress testing (EST), and 91 (20%) had a positive EST. 176/480 (37%) patients were given an exit diagnosis of angina, of whom 84 (48%) were referred directly for coronary angiography. L+ patients were more likely to be initially classified as suffering from angina (36% vs 24%; p = 0.02) but no more likely to have a positive EST (24% vs 19%; p = 0.3); exit diagnosis of angina and likelihood of being referred for angiography were also more likely in L+ patients (50 vs 32%; p = 0.001 and 24 vs 15%; p = 0.03). Overall sensitivity of the Levine sign for a final diagnosis of angina was 33%, with specificity 80%. Positive predictive value of the sign alone was 50% for a final diagnosis of angina, but only 24% for indicating EST positivity.
Conclusions: In the RACPC setting, the Levine sign appears to indicate a population of patients who are more likely to be diagnosed with and investigated for ischaemic heart disease, but are not necessarily more likely to have a positive EST. Caution should be exercised in populations of patients with relatively-undifferentiated chest pain when assuming that the Levine sign is a useful discriminator between anginal and non-anginal chest pain.
chest pain; rapid access; angina
122 A REPORT ON THE REFERRAL RATE OF PATIENTS SEEN IN A RAPID ACCESS CHEST PAIN CLINIC FOR ENDOSCOPY: ARE WE CREATING WORK FOR OUR COLLEAGUES?
J. Tenkorang1, D. Tataree2, D. Wood1, D. Bansi1, A. Thillainayagam1, K. Fox1. 1Imperial College, London, UK; 2Charing Cross Hospital, London, UK
Introduction: Rapid access chest pain clinics (RACPCs) were established as part of the National Service Framework for Coronary Heart Disease to reduce morbidity and mortality from coronary artery disease. Thus their primary aim is to promptly diagnose and effectively initiate management of these patients, in as cost effective a way as possible. It is recognised however that 50–70% of patients seen in RACPCs will not have cardiac chest pain. Moreover, 30–60% of these patients will have a gastrointestinal cause for their chest pain. We investigated the impact of a RACPC on gastrointestinal services.
Abstract 122
Methods: We matched records of all patients attending our RACPC in West London (a same or next day service) with records from the oesophagogastroduodenoscopy (OGD) service (waiting list 21 weeks) to track patients who had attended both services. We reviewed records to investigate indications and outcomes of both services.
Results: 1062 patients were seen in the RACPC between 1 October 2001 and 28 February 2003, 779 (73%) of whom lived within the catchment area of the host NHS Trust and were therefore likely to be referred to the same hospital for OGD. Of these 779 patients, 17 (2%) including 5 patients who were subsequently referred for coronary angiography, were referred for OGD in this time frame, with 15/17 attending for their OGD. Three of the 5 patients had been diagnosed “definite angina” and 2 had the diagnosis of “possible angina”. All 5 underwent coronary revascularisation. Abnormal findings were present in 11/15 (73%) including 4 of the 5 revascularised patients. In other words, 4/15 (27%) had dual pathology. Diagnoses on OGD included oesophagitis, gastritis, duodenitis, hiatus hernia, Barrett’s oesophagus and gastroesophageal reflux disease (GORD). There were no cases of malignancy, nor were there any reported delayed diagnoses of upper gastrointestinal malignancy in patients seen in the RACPC.
Conclusion: These data imply that RACPCs do not generate an increased workload for gastrointestinal services and the high yield of positive results suggests appropriate referral. An expected role of RACPCs is to adequately reassure those diagnosed with non-cardiac chest pain. One way of doing this is simply to exclude significant coronary disease but published reports show that this does not appear to eliminate symptoms or further health-seeking behaviour. Combining the above reports with our data would suggest that far from creating excessive workload, patients diagnosed with non-cardiac pain after assessment in a RACPC may be under-referred for further assessment for a gastroenterology cause to their symptoms. In addition, these data also highlight the important message that over a quarter of RACPC patients with an abnormal OGD may have dual pathology as a cause of their chest pain.
rapid access chest pain clinic; oesophagogastroduodenoscopy; non-cardiac chest pain
123 PROFILING ENGLISH HOSPITAL MORTALITY RATES FOR ACUTE CORONARY SYNDROMES USING THE MYOCARDIAL INFARCTION NATIONAL AUDIT PROJECT DATABASE
C. Gale1, S. Manda2, D. Greenwood2, M. Gilthorpe2, C. Weston3, J. Birkhead4, P. Batin5, A. Hall1. 1Yorkshire Heart Centre, Leeds General Infirmary, Leeds, UK; 2Biostatistics Unit, University of Leeds, Leeds, UK; 3Department of Cardiology, Singleton Hospital, Swansea, UK; 4Department of Cardiology, Northampton General Hospital, Northampton, UK; 5Department of Cardiology, Pinderfields General Hospital, Wakefield, UK
Introduction: Quality assurance and audit are central to good medical practice. The Myocardial Infarction National Audit Project (MINAP) audits standards set by the NSF for coronary heart disease. This allows clinicians to examine the management of acute coronary syndromes (ACS) in their hospital. Variation in hospital mortality is, in part, attributable to case-mix and differences in mortality after case-mix adjustment reflect performance. The EMMACE risk score may be used for case-mix adjustment.
Abstract 123
Methods: We aim to quantify hospital-specific expected 30-day mortality for ACS adjusted for case-mix for 141 acute hospitals in England. We excluded 10 hospitals with limited data. Bayesian models were used to fit a hierarchical model, thus incorporating a random hospital effect (reflecting the similarity amongst hospitals in the way they are supposed to operate). The model comprised 100 686 patients between 1 January 2003 and 31 March 2005.
Results: EMMACE was a good discriminator of 30-day death C index = 0.78 (95% CI = 0.77 to 0.78, p<0.001). The hospital average 30-day mortality rate was 10.2%. The 30-day EMMACE risk adjusted mortality rate (RAMR) ie had the hospitals admitted patients identical to the overall case-mix was 10.6% (median = 10.0.%). The table summarises the top 9 hospital rankings (and 95% credible intervals) for the model.
Conclusion: A profile of estimated hospital-specific RAMR shows case-mix adjusted variation in excess of 30-day mortality. Although data completeness remains an issue, we demonstrate that risk-adjusted hospital performance for the management of ACS may be easily compared, displayed, and quantified. The EMMACE risk model allows case-mix adjustment without restricting the number of cases due to incomplete data fields. Hospitals may be profiled according to quality of care, which may help identify best practice.
MINAP; acute coronary syndrome; mortality
124 NO DIFFERENCE IN 2-YEAR MORTALITY BETWEEN DRUG-ELUTING STENT AND BARE-METAL STENT IMPLANTATION IN “REAL WORLD”
A. Alahmar, A. Grayson, M. Andron, A. Naji, M. Jackson, N. Palmer, R. Perry. Cardiothoracic Centre Liverpool, Liverpool, UK
Background: The impact of drug-eluting stent implantation on long-term mortality is uncertain.
Aim: To assess the long-term impact of drug eluting stent (DES) implantation in percutaneous coronary intervention (PCI) on mortality in routine clinical practice.
Design: We carried out retrospective analysis of prospectively collected data on all patients undergoing PCI with stent implantation at our institution between January 2003 and December 2004. To account for differences in patient characteristics, logistic regression was used to produce a propensity score for DES group membership using age, smoking status, New York Heart Association class, diabetes, priority, left anterior descending artery, left main stem lesion, restenotic lesion, vessel diameter, and length of lesion. Patients receiving DES were then matched to patients receiving bare metal stents (BMS) with identical propensity scores using the greedy match technique. These two groups were then compared with respect to the incidence of death, which was obtained from a national death registry. Kaplan–Meier curves were used to assess differences between DES and BMS.
Results: During the study period 995 patients received DES. Of these, 82 patients had combined DES and BMS use and were therefore excluded, leaving 913 DES patients compared to 2105 BMS patients. Patients who received DES were more likely to be diabetic (p<0.001), hypertensive (p = 0.004), had more lesions treated (p<0.001), restenotic lesions treated (p<0.001), LAD interventions (p = 0.005), LMS interventions (p<0.001), long lesions treated (p<0.001), small diameter lesions treated (p<0.001), and AHA C-type lesions treated p<0.001). After performing propensity-matching, we were able to successfully match 777 DES patients to 777 BMS patients. The mortality difference over 2 years between DES and BMS was not statistically significant (fig, p = 0.081). Although the mortality rate was higher in BMS (4.2%) compared to DES (2.8%).
Conclusion: In our series, there was no significant difference in 2-year mortality between DES and BMS implantation. However, there was trend towards lower mortality in DES group.
drug-eluting stent; mortality; percutaneous coronary intervention
125 A RANDOMISED TRIAL OF DRUG ELUTING VERSUS BARE METAL STENTS IN ACUTE ST ELEVATION MYOCARDIAL INFARCTION
J. Pitt, M. Reeve, H. Whitlam, G. Pulikal, J. Ment, N. El Gaylani, J. Beattie, G. Murray, M. Pitt. Heart of England NHS Foundation Trust (Heartlands), Birmingham, UK
Introduction: Percutaneous coronary intervention (PCI) using stents is the optimal reperfusion strategy for acute ST elevation myocardial infarction (STEMI). Drug-eluting stents (DES) are now used extensively in patients with both stable and unstable coronary syndromes giving excellent early and longterm clinical results. Whether DES can be safely used to treat acute thrombotic coronary occlusions is unclear, although recent studies suggest that DES may be beneficial in STEMI. We present initial data from a randomised study of drug eluting versus bare metal stents in STEMI.
Abstract 125
Methods: From April 2005, in a unit with a 4-year experience of “round the clock” primary PCI for STEMI, consecutive patients adjudged to have sustained a STEMI were randomised, on an intention-to-treat basis, to receive either paclitaxel eluting stents (PES) or bare metal stents (BMS). Randomisation was performed in the cardiac catheter laboratory before diagnostic angiography was undertaken. All other aspects of the PCI procedure were standard and as per unit protocol. The default intervention strategy was to limit revascularisation to the infarct related artery (IRA) unless there was a compelling clinical reason to perform multivessel PCI. Abciximab was used unless contraindicated. Study end points were target lesion revascularisation (TLR) <30 days (examining early subacute thrombosis) and >30 days (examining restenosis and late thrombosis). Clinical follow-up was scheduled for 30 days, 6 months and 1 year. Surveillance angiography was not included as part of the study protocol. The study recruitment target is 250 patients.
Results: We present data for the first 163 patients. Patient and procedural characteristics were not significantly different between the BMS (n = 82) and PES (n = 81) patients with comparable age (mean 57 vs 58 years), incidence of diabetes mellitus, smoking, hypertension and abciximab use. The table shows comparisons between the two groups with respect to TLR and mortality. Of the 8 BMS patients undergoing TLR at >30 days, 4 were treated by CABG and 4 by DES implantation. The single DES patient requiring TLR presented with stent thrombosis at 6 months after index procedure, 7 days after discontinuation of all antiplatelet medication pending non-cardiac surgery. The majority of deaths by 30 days were due to cardiogenic shock (3 in each BMS and DES group). There was one fatal subacute stent thrombosis in a DES patient at 8 days after initial PCI.
Conclusion: In line with recent published data this study suggests that PES use in STEMI appears safe with the promise of reduced requirement for subsequent target lesion revascularisation. Extension of the follow-up period will allow examination of possible late complications of PES use in this clinical setting.
randomised trial; drug-eluting stents; myocardial infarction
126 COMPARISON OF CLINICAL OUTCOMES IN SMALL VESSEL PERCUTANEOUS CORONARY INTERVENTION BEFORE AND AFTER THE INTRODUCTION OF DRUG-ELUTING STENTS
R. Antony1, S. Aziz2, R. Kia3, R. Grainger1, R. Stables1. 1The Cardiothoracic Centre, Liverpool, UK; 2Royal Blackburn Hospital, Blackburn, UK; 3Aintree University Hospital, Liverpool, UK
Introduction: We investigated the impact of drug-eluting stents (DES) on improving the clinical outcomes of small vessel (SV) percutaneous coronary intervention (PCI).
Methods: We performed a retrospective observational study including patients who had undergone a PCI procedure involving the treatment of at least one SV lesion (reference vessel diameter ⩽2.5 mm). The results of 299 patients (633 lesions) treated with DES were compared with 215 patients (272 lesions) who had undergone SV PCI pre-DES. Kaplan-Meier method was used to estimate adverse events at follow-up.
Results: Stents were used as the primary treatment modality in 79% of lesions in the pre-DES group and in 85% of lesions in the DES group (Cypher 58% and Taxus 27%). Diabetes mellitus, multilesion treatment and complex lesion morphology (AHA class C) were more common in the DES group. At 1 year the cumulative rate of major adverse cardiac events (death, myocardial infarction and target vessel revascularisations) was 18% in the pre-DES group and 4% in the DES group (hazard ratio 0.18, 95% CI 0.11 to 0.31, p<0.0001) (fig 1). This was largely due to a reduction in the target vessel revascularisation rate (TVR) in the DES vs pre-DES groups, 14% vs 3% respectively (hazard ratio 0.16, 95% CI 0.08 to 0.32, p<0.001).The frequency of angina reported at follow-up was reduced from 46% in the pre-DES to 27% in DES patients, p<0.001.
Conclusion: The introduction of DES into routine clinical practice has resulted in a significant reduction in major adverse cardiac events and angina symptoms for patients undergoing SV PCI.
percutaneous coronary intervention; small vessels; drug-eluting stents
127 LATE STENT THROMBOSIS: LONG-TERM CLINICAL RESULTS OF THE ELUTES POLYMER-FREE DRUG-ELUTING STENT TRIAL
N. Swanson, A. Carver, D. Kelly, A. Gershlick. Glenfield Hospital, Leicester, UK
Introduction: The ELUTES Study was a dose-finding trial to determine clinical safety and angiographic efficacy of a polymer-free, paclitaxel-eluting stent (PES). This study presents the longer-term follow-up to 24 months, including incidence of late stent thrombosis (LaST). The ISAR-TEST trial,1 comparing polymer-free to polymer-coated stents, has reported a lower LaST rate in the polymer-free group.
Abstract 127
Methods: 192 patients with de novo lesions were randomised to either control or one of four doses of paclitaxel directly applied to a Cook Incorporated V-Flex PlusTM stent without polymer. Clopidogrel was given for 3 months. Clinical follow-up by telephone interview or review in outpatient clinic was completed at 6, 12 and 24 months.
Results: The 6-month data have been published2 showing a dose-response effect on binary stenosis. Binary restenosis was 3% in the highest dose density group versus 21% in controls. Clinical follow-up data were obtained in 152 patients (79%) to 24 months (see table). Event free survival in the PES arms was 85% (102/120). Two late (12–24 months) events occurred, a TLR and CABG in the PES groups. One case of subacute stent thrombosis occurred in the control (day of implant) and the highest paclitaxel dose (after 8 days) arms. One death occurred early (without postmortem) in the PES highest dose group. This patient had had a PES used during primary angioplasty, a protocol violation. No suspected LaST events were reported from 6 to 24 months in any arm of the study—that is, no documented stent thrombosis, MI or cardiac deaths. Follow-up data are incomplete so some of the patients not followed may have had adverse events that are not recorded.
Conclusions: Non-polymer, paclitaxel-coated stents effectively inhibited angiographic parameters of restenosis. The stent system appeared safe, with a high event-free survival. The lack of late stent thrombosis may support the use of polymer-free stents to avoid any potential prothrombotic long-term effects of polymer-coated stents.
stent thrombosis; polymer-free; ELUTES
1
2
128 SERUM CREATININE CONCENTRATION IS AN INDEPENDENT PREDICTOR OF LONG-TERM MORTALITY FOLLOWING PERCUTANEOUS CORONARY INTERVENTION; DRUG-ELUTING STENT IMPLANTATION REDUCES THIS RISK
A. Alahmar, M. Shaw, M. Egred, E. Roberts, M. Andron, A. Grayson, R. Antony, K. Albouaini, M. Jackson, R. Stables, R. Perry. Cardiothoracic Centre Liverpool, Liverpool, UK
Background: Patients with renal insufficiency (RI) who undergo percutaneous coronary intervention (PCI) experience increased long-term mortality. Creatinine clearance is an accurate marker of the degree of RI; however it is not practical for use in routine daily practice.
Abstract 128
Aim: We examined the effect of pre-PCI serum creatinine levels on long-term mortality.
Methods: We carried out retrospective analysis of prospectively collected data on 6160 consecutive patients who underwent PCI between January 2000 and December 2004. Baseline serum creatinine levels were available in 5656. Patients were followed up to 31 March 2005 with a mean follow-up duration of 3 years. Cox proportional hazard analysis was used to examine the association between serum creatinine levels and long-term mortality, while accounting for other patient characteristics.
Results: 392 deaths occurred during the follow-up period. Increasing levels of serum creatinine were shown to be a significant risk factor for follow-up mortality (hazard ratio (for each additional 10 μmol/l): 1.05, 95% CI 1.04 to 1.07, p<0.001; table). Figure 1 shows the risk of mortality by increasing serum creatinine levels, adjusted for other risk factors for mortality. The risk of mortality at 1-year depending on increased levels of serum creatinine was significantly reduced when using drug-eluting stents (DES) compared to conventional bare metal stents (fig 2).
Conclusions: In this large PCI series, increasing pre-PCI serum creatinine levels were an independent predictor of long-term mortality. Use of DES may alleviate this risk.
percutaneous coronary intervention; serum creatinine; drug-eluting stent
129 INDIVIDUAL RESPONSES TO ASPIRIN USING A NOVEL METHOD OF THROMBELASTOGRAM ANALYSIS: HYPORESPONSIVENESS OR POOR COMPLIANCE?
A. Hobson, K. Dawkins, N. Curzen. Wessex Cardiac Unit, Southampton University Hospitals Trust, Southampton, UK
Introduction: Individual responses to aspirin are known to vary with adverse events more common in those with relative hyporesponsiveness. However, responses are difficult to assess clinically and reports of “aspirin resistance” yield estimates of prevalence ranging from <1% to 40%. A rapid and reliable point of care test of the effects of aspirin would therefore be of clinical value. Gold standard tests such as optical aggregation are time consuming and measure the effects of aspirin on isolated platelets rather than on whole blood coagulation. We have previously shown that modified thrombelastography (TEG) has the ability to detect responses to aspirin. However, results have taken 60 min to obtain and analysis required a baseline sample for comparison. We report a novel method of TEG analysis which (a) allows assessment of the effects of aspirin in only 15 min and (b) does not require a baseline sample for comparison.
Methods: Ten healthy volunteers and 10 patients attending for elective PCI were recruited. In the healthy volunteers blood tests were taken immediately before and 2, 6 and 24 h after a witnessed 300 mg dose of aspirin. In patients, all of whom reported compliance with aspirin 75 mg daily for >28 days, blood tests were taken on admission and 24 h later, between which timepoints a 150 mg dose of aspirin was administered. Blood samples were analysed using TEG PlateletMapping according to manufacturer’s instructions. Analysis was performed using a novel parameter (the area under the response curve at 15 min (AUC15)), from which we derived the percentage clotting inhibition (%CIn) for each sample, calculated using a thrombin stimulated clot as a patient specific reference.
Results: All volunteers responded well to aspirin (fig 1). There was little variation in the response observed. Mean %CIn was 86.1 (4.6)% at 2 h, 86.7 (4.8)% at 6 h and 84.7 (4.3)% at 24 h, thus demonstrating that this test can rapidly and reproducibly detect time-dependent responses to aspirin. By contast, in PCI patients on maintenance aspirin therapy mean %CIn was 53 (26)% with 4 patients (highlighted in fig 2) demonstrating little evidence of aspirin response (%CIn<50%). Following a witnessed dose of aspirin 150 mg all patients exhibited significant response to aspirin (fig 2) with a mean %CIn of 80.0 (7.1)% (similar to the response observed in volunteers).
Conclusions/Implications: This novel TEG technique using the AUC15 and %CIn can assess individual responses to aspirin in only 15 min. We have detected evidence of lack of apparent response to aspirin in 4 of 10 patients which could represent either true hyporesponsiveness or poor compliance. The subsequent response to 150 mg aspirin implies that poor compliance was the responsible mechanism. This technique shows promise in differentiating true aspirin resistance from poor compliance.
aspirin; platelet; thrombelastography
130 MARKED HETEROGENEITY OF INDIVIDUAL RESPONSES TO LOADING DOSE CLOPIDOGREL EMPLOYING A NOVEL POINT OF CARE TEST
A. Hobson, K. Dawkins, N. Curzen. Wessex Cardiac Unit, Southampton University Hospitals Trust, Southampton, UK
Background: Despite the routine use of clopidogrel in percutaneous intervention (PCI) adverse events such as Stent thrombosis, although rare, continue to occur, and have been linked to relative hyporesponsiveness to standard doses. An assay that could rapidly assess individual responses to clopidogrel would be clinically useful in the detection of this risk and possibly in its therapeutic manipulation. We have previously shown that the Thrombelastogram PlateletMapping (TEG) system can detect responses to antiplatelet agents but conventional analysis is relatively slow and inflexible.
Methods: Fifteen patients attending for routine PCI received 600 mg loading doses of clopidogrel. Blood tests were taken immediately before and 2, 6 and 24 h after the loading dose. TEG analysis was undertaken using a novel parameter, the area under the response curve at 15 min (AUC15), which was calculated with a purpose-specific software programme “Areafinder 2.1” developed by this group. A percentage clotting inhibition (%CIn) due to clopidogrel was calculated at each timepoint using thrombin stimulated clot formation as a patient specific reference.
Results: There were significant changes in mean %CIn at all timepoints compared with baseline (all p<0.001) and a significant increase in inhibition from the 2- to 6-h timepoints (p<0.05). However, this masks marked heterogeneity in both the timescale and extent of response of individual patients to clopidogrel (fig 1). At the 2-h timepoint individual inhibition varied from 0 to 72% and 7 of 15 patients (highlighted in fig 1) had %CIn of <10%.
Conclusions/Implications: Using the AUC15 and %CIn TEG analysis can rapidly detect changes in blood clotting due to clopidogrel at any timepoint without the need for a baseline reference sample. There is marked heterogeneity in the timescale and extent of individual response to clopidogrel. Further studies are required to determine whether the level of response is predictive of adverse events and whether treatment modification, using higher than standard doses, to optimise the level of response, improves subsequent outcome.
clopidogrel; platelet; thrombelastography
131 RESTING MYOCARDIAL BLOOD FLOW NOT MYOCARDIAL FLOW RESERVE PREDICTS HIBERNATING MYOCARDIUM: A QUANTITATIVE MYOCARDIAL CONTRAST ECHOCARDIOGRAPHY STUDY
M. Hickman, L. Burden, R. Senior. Northwick Park Hospital, Harrow, UK
Background: Both resting myocardial blood flow (MBF) and myocardial flow reserve (MFR) may be affected in hibernating myocardium (HM). We assessed the relative value of resting MBF parameters and MFR for the prediction of HM, using quantitative myocardial contrast echocardiography (MCE).
Abstract 131 Quantitative MCE in segments with normal and abnormal function
Methods: Accordingly, 27 patients (LVEF: 30±10%) scheduled for revascularisation underwent resting low power MCE and vasodilator stress followed by echocardiography (23 patients) 3–6 months after revascularisation. Resting peak contrast integrity A and microbubble velocity B (MBF) parameters and β reserve (MFR) were assessed. Improvement in wall thickening of dysfunctional segments or improvement after low dose dobutamine in a persistently dysfunctional segment after revascularisation was defined as HM.
Results: Of the 310 dysfunctional segments before revascularisation 228 (74%) demonstrated HM. All resting MCE parameters were significantly reduced in HM compared to segments with normal baseline function but were significantly higher compared to necrotic myocardium (table). However, β reserve was similarly (p = 0.15) reduced in hibernating and necrotic myocardium. A cut-off of 5 dβ of A provided the best sensitivity (87%) an specificity (67%) for the detection of HM.
Conclusion: Both resting MBF parameters and MFR are reduced in HM, but only the former predicted HM. Thus, MCE provides both pathophysiological and diagnostic information in patients with HM.
contrast echocardiography; artery disease; hibernating myocardium
132 IDENTIFYING RESPONDERS TO CRT: ARE WE USING THE RIGHT METHOD?
C. Parsai1, B. Bijnens2, G. Sutherland1, A. Baltabaeva1, M. Marciniak1, A. Marciniak1, L. Anderson1. 1St George’s Hospital, London, UK; 2University of Leuven, Leuven, Belgium
Introduction: Cardiac resynchronisation therapy (CRT) is established treatment for refractory heart failure, broad QRS, and severely impaired ejection fraction (EF<35%). However, up to 30% of patients fail to respond. Currently, the timing of long axis systolic events (regional velocity or strain) is used to better predict response to CRT. However, cardiac rotation or LV displacement induced by preserved right ventricular (RV) long axis shortening may affect LV peak systolic velocities and thus not detect dyssynchrony in “rocking hearts”, negating long axis systolic velocity indices as dyssynchrony markers. Moreover, this approach assumes a single mechanism of effect (dyssynchrony) in CRT.
Methods: To determine if there are other mechanisms involved in response to CRT, the following study was performed. Data from 21 patients (pre- CRT, 61 (12) years, EF 28 (6)%, QRS>130 msec) were obtained at baseline (pre-CRT) and 6 months after CRT. Clinical data (NYHA class, quality of life and 6 min walk) and echocardiographic remodeling (reduction of LVESV >10%) were defined as markers of response. Dyssynchrony was measured using radial velocity parameters (theoretically not influenced by cardiac rotation) and compared with the dyssynchrony index (Yu method). Radial Tissue Doppler velocity profiles were obtained from the septum and inferolateral walls at mid-ventricular level using short axis views.
Results: Four different subgroups were identified. Group 1: 11 patients (52%), had radial velocity dyssynchrony and an early peak septal radial velocity occurring during the isovolumic contraction period (septal flash). Ten responded and showed resolution of the septal flash and 1 patient failed to respond due to lead displacement. Group 2: 5 patients (24%), had no dyssynchrony but an abnormal diastolic filling pattern (Atrio-ventricular (AV) dyssynchrony). They all responded after AV optimisation. Group 3: 3 patients (14%), had none of the previous parameters, but a direct RV-LV interaction causing a passive septal motion. A marked clinical improvement was obtained in all after RV-LV optimisation, despite the lack of remodelling. Group 4, 2 patients had none of the previous features and did not respond. The published dyssynchrony index failed to identify 33% (n = 7) of our responders. Four CRT patients (19%) with preserved RV long axis function, and rocking heart appearance on echo, had no measurable long axis dyssynchrony (Yu method) due to the pulling effect of radial RV fibres inserted on the LV free wall. However, dyssynchrony was identified in all of them using radial velocities, thus predicting response.
Conclusions: In heart failure patients fulfilling the current clinical criteria for CRT, potential response can be assessed individually by identifying the underlying mechanisms amenable to CRT. Radial velocity parameters (combined with conventional 2-D data) could provide an easy way to classify patients according to 4 different pathological subgroups and thus help predict response.
cardiac resynchronisation therapy; radial velocity dyssynchrony; responders
133 2D-STRAIN DERIVED ANTEROSEPTUM TO POSTERIOR WALL DELAY PREDICTS REVERSE REMODELLING AFTER CARDIAC RESYNCHRONISATION THERAPY
N. Artis1, D. Oxborough1, L. Tan1, G. Williams2, C. Pepper2. 1University of Leeds, Leeds, UK; 2Leeds General Infirmary, Leeds, UK
Introduction: 2D-Strain imaging using speckle-tracking is a Doppler independent method enabling simultaneous analysis of myocardial strain in both the radial and circumferential dimensions. Using commercially available software it is possible to measure the time-to-peak strain of left ventricular segments. The changes that occur following CRT and the usefulness of this technique to predict response to CRT are unknown and may assist in our understanding of dyssynchrony.
Methods: Thirty one subjects who successfully underwent cardiac resynchronisation therapy (CRT) implantation were recruited with the approval of the local ethics committee. The primary outcome was evidence of reverse remodelling at 6 months (a reduction in left ventricular end systolic volume (LVESV) of >15%.) NYHA class, 6 Minute Walk Test (6MWT) and the Minnesota living with heart failure questionnaire (MLWHF) were used as secondary markers of response. Images were acquired the day prior to implantation using a Vivid 7 (GE Vingmed) ultrasound system and analysed offline using dedicated 2D-Strain software. A parasternal short-axis view at papillary muscle level was used to assess circumferential and radial strain. The time differences from Q wave of the ECG to peak strain was measured in the anteroseptum and posterior regions (SPW).
Results: Of the 31 subjects, 2 died before 6 months and 4 others withdrew their consent from the study. SPW circumferential strain difference was superior to SPW radial strain difference as a predictor of reverse remodelling. Using ROC curve analysis the area under the curve (AUC) was 0.756. A time to peak circumferential strain difference of >130 ms between the anteroseptum and posterior wall predicted reverse remodelling with a specificity of 85% and a sensitivity of 67%. This marker also performed well in the prediction of a clinical response (AUC for 6MWT 0.79, MLWHF 0.83).
Conclusion: This technique is advantageous in allowing assessment of short axis function. The time difference to peak circumferential strain between the anteroseptum and posterior wall is a good predictor of reverse remodelling. This new technique illustrates that short axis function is important in the assessment of dyssynchrony prior to CRT and further work is required to evaluate its clinical application and utility.
cardiac resynchronisation therapy; 2D-Strain; reverse remodelling
134 QUANTIFICATION OF CARDIAC DYSSYNCHRONY AT REST AND AFTER PEAK EXERCISE IN HEART FAILURE PATIENTS
J. Silberbauer1, L. Beale2, G. Brickley2, W. Taggu1, R. Veasey1, N. Patel1, A. Sulke1, G. Lloyd1. 1East Sussex Hospitals NHS Trust, Eastbourne, UK; 2University of Brighton, Eastbourne, UK
Introduction: Cardiac dyssynchrony at rest is associated with impaired exercise capacity and suggests likely response to biventricular pacing in severe heart failure. Further work is needed to understand alterations in ventricular synchrony and the implications of such changes during exercise.
Methods: Fourteen patients (mean age 72 (9) years, 10 male), NYHA III/IV, left ventricular ejection fraction <40% underwent maximal bicycle exercise stress echocardiography. Cardiopulmonary data were also obtained. Pulsed-wave tissue Doppler was taken in six left ventricular walls at the level of the mitral annulus and the RV free wall at rest and immediately after exercise. Q wave to onset and peak systolic velocities were analysed offline. Onset timings were adjusted on a beat-to-beat basis by dividing by the R-R interval for the heart rate-adjusted dyssynchrony indices. Combined left ventricular (LV) and right ventricular dyssynchrony was analysed using the method described by Penicka et al and termed the sum dyssynchrony. The maximal dispersion in time to onset of systolic motion between the six left ventricular walls was termed the intra-LV dyssynchrony. Both measures were adjusted for heart rate to allow comparison of rest and exercise dyssynchrony.
Results: Q wave to onset and peak of systolic contraction increased in all segments with exercise. However, when adjusted for heart rate increase, the anterior and lateral walls were slower than baseline and the posterior wall was faster. The resting sum asynchrony index significantly worsened with exercise (absolute – 100 (52) ms vs 114 (68) ms, p = 0.04 and adjusted − 8.4 (5.7)% vs 12.3 (8.2)%, p = 0.007). Recent work has been completed which will allow determination of these dephasing effects on cardiopulmonary exercise performance in heart failure. Using the combined and intra-LV dyssynchrony indices respectively, 9 and 10 patients worsened and 5 and 4 patients improved during exercise. One patient using the combined index and 2 patients using the LV-only index, not fulfilling resting CRT echo criteria, developed significant “responder” dyssynchrony during exercise.
Conclusions: This study suggests that increasing dyssynchrony through alterations in LV activation patterns with exercise in heart failure may be responsible for worsening cardiopulmonary exercise performance in a subgroup of patients. This hypothesis has been formally investigated. Furthermore, a subgroup of patients without resting dyssynchrony develop dyssynchrony during exercise. This may therefore have implications for programming of biventricular devices and patient selection.
heart failure; exercise; dyssynchrony
135 EXTENT OF MYOCARDIAL VIABILITY DETECTED BY MYOCARDIAL CONTRAST ECHOCARDIOGRAPHY EARLY AFTER ACUTE MYOCARDIAL INFARCTION IS AN INDEPENDENT PREDICTOR OF MORTALITY AND RE-INFARCTION
G. Dwivedi, S. Hayat, R. Janardhanan, N. Ruperalia, T. Lim, R. Senior. Northwick Park Hospital, Harrow, UK
Background: Myocardial viability (MV) detected by myocardial contrast echocardiography (MCE) has been shown to predict recovery of left ventricular (LV) function in patients with acute myocardial infarction (AMI). However, to date no study has shown its value in predicting major adverse outcomes in patients after AMI in whom thrombolysis is the major mode of reperfusion therapy.
Objective: To determine whether residual MV determined by MCE after AMI can predict hard cardiac events.
Methods: Accordingly, 99 stable patients underwent low power MCE at 7 days after AMI. Contrast defect index (CDI), a measure of residual myocardial viability, was obtained by adding contrast scores (1 = homogenous; 2 = reduced; 3 = minimal/absent opacification) in all 16 LV segments divided by 16. At discharge 65 (68%) patients, had either undergone or were scheduled for revascularisation independent of the MCE result. The patients were subsequently followed up for cardiac death and non-fatal AMI.
Results: Of the 99 patients, 95 were available for follow-up. Of these, 86 (87%) underwent thrombolysis. During the follow-up time of 46 (16) months, there were 15 (16%) events (8 cardiac deaths and 7 non-fatal AMIs). Among the clinical, biochemical, electrocardiographic and echocardiographic markers of prognosis, the extent of residual MV was an independent predictor of cardiac death (p = 0.01); cardiac death or AMI (p = 0.008). Age (p = 0.02) and mean stenosis on coronary arteriography (p = 0.03) were other significant multivariate predictors of cardiac death but not cardiac death or AMI. A CDI of ⩽1.86 (fig) and ⩽1.67 ruled out death and death or MI in 99% and 95% of the patients respectively.
Conclusions: The extent of residual MV predicted by MCE is a powerful independent predictor of hard cardiac events in patients following AMI and may be used to risk stratify such patients.
contrast echocardiography; myocardial viability; acute myocardial infarction
136 CONTRAST ULTRASONOGRAPHY: A NOVEL APPLICATION FOR THE ASSESSMENT OF GRAFT PERFUSION
K. Greaves1, S. Sharma1, R. Anand1, J. Bowden1, V. Ilankovan1, M. Hickman1, S. Walji1, R. Senior2. 1Poole Hospital, Poole, UK; 2Northwick Park, Harrow, UK
Introduction: Reconstructive surgery for maxillofacial cancer uses free flap grafts with their vascular pedicles. Methods to detect graft viablity are crude. Contrast ultrasonogrpahy is a novel technique that can assesses graft perfusion at the bedside. We hypothesised that contrast ultrasonography (CU) detects graft perfusion and accurately predicts graft outcome.
Abstract 136
Methods: Twenty seven patients (17 male) mean age 56 (range 29–82) years undergoing free flap surgery for maxillofacial cancer were recruited. Standard assessment of grafts with direct inspection (DI) and non-imaging spectral Doppler (NISD) were performed three times daily and CU performed 12, 24 and 48 h after surgery. Tissue perfusion was assessed qualitatively by the presence or absence of microbubbles, and quantitatively by peak contrast intensity (α) and blood velocity (β).
Results: Out of 27 grafts implanted 3 (11%) failed (confirmed at rescue surgery). Qualitative CU predicted failure in all 3 grafts (100%) and success in the remaining (100%). All graft failures had complete contrast absence at 12, 24 and 48 h. Mean quantitative α values in the healthy and failed grafts were 4.9 (2.2) (range 1.7–11.6) and 0.22 (0.14) (range 0.09–0.9) respectively. All failed graft α values were <1.0. β values in healthy grafts were 0.69 (0.68). The agreement values of DI, NISD, and qualitative CU are shown in the table. Although CU visualised all grafts, standard techniques could not assess 3 buried grafts. Of the 3 graft failures, DI did not detect impaired graft function until day 2 (1 graft) and day 5 (2 grafts). NISD did not detect any of the graft failures.
Conclusion: CU is a simple bedside technique that accurately and rapidly assesses tissue perfusion following graft surgery and is superior to standard techniques.
contrast; perfusion; ischaemia
137 STRESS ECHOCARDIOGRAPHY IN THE DISTRICT HOSPITAL SETTING: A COST-EFFECTIVENESS ANALYSIS
N. Wennicke1, R. Senior2, K. Greaves1. 1Poole Hospital, Poole, UK; 2Northwick Park Hospital, Harrow, UK
Introduction: Stress echocardiography (SE) has been shown to be cost effective in the evaluation of chest pain suspected to be due to coronary artery disease. Despite this, SE is severely underused in the UK (only 17% of UK hospitals perform >100 SE per year). We sought to assess the cost savings produced by the introduction de novo of a SE service for the investigation of chest pain in a district general hospital (DGH).
Abstract 137
Methods: Consecutive patients with chest pain referred for SE either directly, or following an exercise treadmill ECG test, in an outpatient setting, were recruited. The referring physician was asked to choose an alternative investigation if SE had not been available: myocardial perfusion scintigraphy (MPS), coronary angiogrpahy (CA), exercise treadmill ECG (ETT) or none. Cost effectiveness was calculated as the difference in the cost if a SE service had not been available minus the cost if SE had been available.
Results: Of the 200 patients referred (age 61, range 36–86 years) 46% were male. 141 (70%) patients had a normal SE and 59 (30%) an abnormal SE. In the abnormal SE group 15 (8%) patients had conservative therapy and 44 (22%) underwent CA. In the normal SE group at 6 months follow-up there was one adverse event (0.7%). If SE was unavailable 61% would have had MPS, 39% CA, 0% ETT and 0% no test at all. The 2006 UK reference cost for CA is £724 and our calculated true costs for MPS and SE are £345 and £133 respectively. The table below shows SE provides a significant cost-saving over other imaging techniques.
Conclusion: This study shows that SE used for the investigation of chest pain in a DGH setting provides significant cost-savings.
stress echocardiography; cost; chest pain
138 PARTIAL VOLUME EFFECT, NOT HYPOPERFUSION, IS THE CAUSE OF PERFUSION DEFECTS ON SINGLE PHOTON EMISSION COMPUTED TOMOGRAPHY IN LEFT BUNDLE BRANCH BLOCK PATIENTS WITHOUT CORONARY ARTERY DISEASE: A QUANTITATIVE MYOCARDIAL CONTRAST ECHOCARDIOGRAPHY STUDY
S. Hayat, G. Dwivedi, T. Lim, A. Jacobsen, R. Senior. Northwick Park Hospital, Harrow, UK
Background: Complete left bundle branch block (LBBB) is a common electrocardiographic disorder and is often associated with coronary artery disease (CAD). Perfusion abnormalities have been noted to occur both at rest and during vasodilator stress on single photon emission computed tomography (SPECT) even in the absence of flow limiting CAD. However, the underlying mechanism remains unclear. We hypothesised that partial-volume effect may be the underlying mechanism.
Abstract 138
Methods: Accordingly 37 patients, mean age 66 (8) years, mean LVEF 37 (14)%, with LBBB and no evidence of ⩾50% stenosis on angiography underwent 2D echocardiography, and simultaneous vasodilator 99mTc-sestamibi SPECT and myocardial contrast echocardiography (MCE). Patients were assessed for left ventricular (LV) volumes, LV ejection fraction (LVEF), and LV wall thickness on 2D echocardiography. Perfusion defects, both at rest and stress, were scored by independent blinded observers on a matching 16 segment LV model for both imaging modalities. Quantitative MCE was also performed to assess myocardial blood volume (MBV) and myocardial blood flow (MBF) reserve (MBFR).
Results: Of the 37 patients 19 (51%) demonstrated perfusion abnormalities on SPECT of which 17 (89%) demonstrated perfusion abnormalities involving the septum. The only univariable predictors of SPECT perfusion defect were LVEF (p = 0.04) and mean SWT (p = 0.0017; table). Mean SWT was the only multivariable predictor of SPECT perfusion defects. Mean SWT was found to be significantly lower than mean PWT (1.25 (0.20) cm vs 1.32 (0.18) cm, p = 0.003). Mean SWT was significantly lower than mean PWT (1.15 (0.12) cm vs 1.28 (0.14) cm, p<0.0001) in patients with SPECT perfusion defect. However, there was no significant difference between the two walls in patients with normal SPECT perfusion (p = 0.92). MBV and MBF were similar in patients with and without SPECT perfusion defects (fig).
Conclusion: We have shown with quantitative MCE that both resting MBF and MBFR are homogenous in patients with non-ischaemic dilated cardiomyopathy and LBBB. 99mTc-MIBI SPECT in these patients is significantly affected by heterogeneity in regional myocardial wall thickness and commonly (51%) results in false perfusion defects.
contrast echocardiography; perfusion imaging; radionuclide imaging
139 ASSESSMENT OF VENTRICULAR FUNCTION IN ATRIAL FIBRILLATION: SINGLE BEATS WITH EQUAL PRECEDING AND PRE-PRECEDING R-R INTERVALS ALLOW ACCURATE ESTIMATION OF LEFT VENTRICULAR SYSTOLIC FUNCTION
A. Bajpai, A. Kiotsekoglou, I. Savelieva, C. Dougal, E. Rowland, G. Sutherland, A. Camm. St George’s, University of London, London, UK
Background: During atrial fibrillation (AF), the irregularly irregular rhythm has historically presented a major challenge to estimate the left ventricular (LV) systolic function. In clinical practice echocardiographic parameters are averaged over several cardiac cycles (commonly 3–5 beats which is unreliable and is dependent on the selected window of cycles). Studies have shown that during AF, it requires measured parameters to be averaged over 13–17 consecutive cardiac cycles in order to have less than 2% variability as compared to sinus rhythm. Although the LV systolic function in AF shows wide beat-to-beat variability, it appears to have a positive linear relationship to the ratio of preceding (RR1) and pre-preceding (RR2) cycle lengths.
Methods: We performed a pilot study on 11 patients with persistent AF to comprehensively compare parameters of LV systolic function measured over 17 consecutive cardiac cycles, with those from beats with equal RR1 and RR2 intervals. Beats with equal preceding and pre-preceding RR intervals (RR1 = RR2) were labelled as index beats (IB). Two kinds of IB were identified—those with longest equal RR intervals (IB1) and those with shortest equal RR intervals (IB 2). 2D echocardiographic images were acquired for each LV parameter over 20 consecutive cardiac cycles. LV stroke output was assessed by measuring aortic time velocity integral (TVI). LV ejection fraction (EF) was assessed by Simpson’s biplane method in apical four and two chamber views. LV longitudinal function was assessed by 2D-guided M-Mode and anatomical M-Mode with cursor placed at the lateral, septal, anterior and inferior aspects of mitral valve annular margins in apical four and two chamber views respectively. Measurements were performed offline using the Echopac software.
Results: We found a strong correlation between all LV systolic parameters measured over the index beats and from average values obtained over 17 consecutive cardiac cycles (coefficient of correlation in the range of 95–99%; p<0.001) (fig). The mean relative error for EF calculated from index and averaged beats was <1% and in the range of <1% to 3% for LV volumes. Moreover, measurements were not significantly affected by short or long sets of cardiac cycles and provided values with the same level of accuracy between IB 1 and IB 2.
Conclusion: Echocardiographic measurements obtained from single beats with equal preceding and pre-preceding cardiac cycles provide accurate assessment of LV systolic function in AF and obviate the need to average multiple cardiac cycles. We are continuing our work to include more patients and also to assess whether LV diastolic parameters can be measured with the same accuracy.
atrial fibrillation; RR intervals; ventricular function
140 PHYSIOLOGICAL EVIDENCE OF THE “SECOND FACTOR” IN ATRIAL REMODELLING IS ACCOMPANIED BY LOCALISED CONDUCTION ABNORMALITIES IN THE CHRONIC GOAT MODEL OF ATRIAL FIBRILLATION
S. Kirubakaran1, M. Hall1, N. Peters2, C. Garratt1. 1Manchester Heart Centre, Manchester, UK; 2Imperial College, London, UK
Background: Atrial fibrillation (AF) is known to be self-perpetuating due to short-term changes in atrial refractoriness and poorly characterised “second factors” acting over a longer period. We examined the role of AF-induced localised conduction abnormalities in a goat model of AF in which the physiological effects of “second factors” are well characterised.
Method: Twelve goats each had pacing systems implanted designed to induce and maintain AF. Three goats were kept in sinus rhythm (controls) and 9 goats underwent a sequence of three 1-month periods of pacemaker-maintained AF, separated by one week periods of sinus rhythm. After each one-month period 3 goats underwent epicardial mapping of the right atrial free wall during atrial pacing. Epicardial mapping was performed using a multipolar rectangular array of 112 unipolar electrodes (Prucka Inc) with a 3.57 mm interelectrode separation. Electrograms were acquired using a Cardiomapp system at a sampling rate of 1 kHz. The morphology of the atrial unipolar electrograms were divided into 3 categories: single, double (two negative deflections) and fractionated electrograms (exhibiting more than two negative deflections). Local atrial conduction velocity was calculated by the method of triangulation.
Results: There was a cumulative increase in AF stability over successive 1-month periods of AF (time to persistent AF: 1st AF month 252 (3) h, 2nd AF month 120 (8) h and 3rd AF month 38 (8) h, ANOVA p<0.05), with no difference in the rate of fall of the AERP. After successive one month periods of AF there was no change in the mean atrial conduction velocity (control 77.3 (9.6), 1st AF month 88.7 (5.5), 2nd AF month 78.5 (23), 3rd AF month 78.2 (14) cm/s, ANOVA p = NS).There was however a progressive increase in the proportion of fractionated atrial electrograms (control 0.3%, 1st AF month 1.3 (1.5)%, 2nd AF month 10.6 (2)%, 3rd AF month 17.0 (5)%, ANOVA p<0.05) (fig 1) and the proportion of areas of slow atrial conduction defined as a local conduction velocity of <10 cm/s (control 0.1 (0.1)%, 1st AF month 0.3 (0.6)%, 2nd AF month 6.5 (3)%, 3rd AF month 6.9 (4)%, ANOVA p<0.05).
Conclusion: The progressive development of localised conduction abnormalities in this model have a time course similar to that of AF-induced changes in arrhythmia stability. These localised conduction changes may underlie the “2nd factor” involved in the self-perpetuation of AF.
atrial fibrillation; conduction; remodeling
141 RELATIVE CONTRIBUTION OF ELECTRICAL AND NON-ELECTRICAL (STRUCTURAL) REMODELLING ON THE ATRIAL FIBRILLATION CIRCUIT SIZE IN THE CHRONIC GOAT MODEL OF ATRIAL FIBRILLATION
S. Kirubakaran1, M. Hall1, N. Peters2, C. Garratt1. 1Manchester Heart Centre, Manchester, UK; 2Imperial College, London, UK
Background: It has been postulated that the stability of atrial fibrillation (AF) is determined by the size of reentrant wavelets circulating within the atria (atrial circuit size). Previous work in the goat model has demonstrated a large difference between calculated atrial circuit size in acute AF compared to that measured up to 6 months of AF (chronic AF).1 The relative contribution of electrical and non-electrical or structural remodeling to this process are not clear however. We examined this question using a protocol of successive one month periods of maintained AF in the goat model.
Methods: Twelve goats each had pacing systems implanted designed to induce and maintain AF. Three goats were kept in sinus rhythm (controls) and nine goats underwent a sequence of three 1-month periods of pacemaker-maintained AF, separated by 1-week periods of sinus rhythm. After each 1-month period three goats underwent epicardial mapping of the right atrial free wall during AF. Epicardial mapping was performed using a multipolar rectangular array of 112 unipolar electrodes (Prucka Inc) with a 3.57 mm interelectrode separation. Electrograms were acquired using a Cardiomapp system at a sampling rate of 1 kHz. Isochronal maps were constructed from local activation times at each electrode, from which the complexity of AF was divided into type 1 (single broad wavefront propagating across the right atrium), type 2 (two separate wavefronts) and type 3 (three or more wavefronts present). Measurements were made of AF cycle length (AFCL) and average atrial conduction velocity during AF (AFCV) by the method of triangulation. We defined reentry pathlength (as a surrogate of atrial circuit size) as the product of AFCL and AFCV. Comparison was made between reentry pathlength of acute AF, AF of 1 month duration and previous measurements of chronic AF in this model.
Results: The calculated reentry pathlength progressively decreased after successive one month periods of AF (control 11.9 (0.4) cm, 1st AF month 7.1 (0.4) cm, 2nd AF month 6.2 (0.4) cm and 3rd AF month 6.2 (0.4) cm) (fig 1). There was a significant difference between acute AF and the 1st AF month (−4.8 cm, p<0.05) due to electrical remodeling and a significant difference between the 1st AF month and chronic AF (−3.0 cm, p<0.05) due to non-electrical (structural) remodelling. These changes were accompanied by an increase in complexity of AF (type 3 AF control 0%, AF period 1, 3 (3)%, AF period 2, 33 (15)%, AF period 3, 83 (21)%, ANOVA p<0.05).
Conclusion: Electrical and non-electrical (structural) remodelling result in approximately equivalent changes in atrial circuit size. This finding highlights the importance of developing effective treatments for both types of remodelling in order to combat the self-perpetuation of AF.
atrial fibrillation; circuit size; complexity
142 DOES CONDUCTION DELAY IN THE RIGHT VENTRICULAR OUTFLOW TRACT UNDERLIE ARRHYTHMOGENESIS IN BRUGADA SYNDROME? A NON-CONTACT ENDOCARDIAL MAPPING STUDY
A. Ahmed1, D. Rogers1, M. Uddin2, M. Lowe1, M. Dhinoja1, A. Chow1, P. Lambiase1. 1Heart Hospital, UCL, London, UK; 2Kettering General Hospital, Kettering, UK
Background: The pathophysiological basis of Brugada syndrome (BS) remains contentious. Characterised by a triad of right bundle branch block (RBBB) pattern, ST elevation in V1-V3 and ventricular fibrillation, it remains one of the leading causes of sudden cardiac death in the young. Hypotheses explaining the propensity to developing fatal arrhythmias in this condition have so far focussed on right ventricular epicardial conduction delay and repolarisation abnormalities leading to subepicardial attenuation of the action potential (AP) dome in the right ventricular outflow tract (RVOT) and phase 2 re-entry. A single Langendorff perfused explanted human heart study suggested endocardial conduction delay accounts for the typical ECG features but there was no evidence of mid-myocardial action potential differences. To date there has been no report of in vivo high density mapping of the Brugada heart in man. We investigated the hypothesis that significant endocardial conduction delays exist in the RVOT of BS patients.
Methods: Seventeen patients (Brugada n = 9, normal n = 8) were studied using non-contact mapping. Conduction curves were generated from electrograms recorded in the RVOT, RV body and apex using a standard S1-S2 decremental pacing protocol down to ERP with pacing from RV apex following a 9 beat 600 msec and 400 msec baseline drivetrain respectively. Activation times (AT) were measured for baseline stimulation at 400 and 600 msec and each premature impulse (S2) in these three sites. The area under the AT curve and mean increase in delay (MID) were calculated.
Results: Significant differences in conduction delay was found between the RVOT and RV body and apex in BS patients (p = 0.001) (fig 1). There was no significant delay in AT between these two regions in the normal group (p = 0.17). There was a trend to prolonged delay in the RVOT of Brugada patients (p = 0.056) compared to normal RVOT. Conduction times in the LVOT were not significantly prolonged compared to the apex and body in BS. Isochronal maps were constructed for these endocardial sites which confirmed isochrone crowding and conduction delay in the RVOT of patients with BS (fig 2).
Conclusion: Significant conduction delays exist in the RVOT of BS patients compared to RV body and apex versus normal RV where no significant differences exist. The extent of conduction delay may be a determinant of risk from lethal arrhythmia in these patients.
Brugada syndrome; conduction delay; non-contact mapping
143 COMPUTER-ASSISTED ELECTRICAL MAPPING OF ATRIAL TACHYARRHYTHMIAS IN PATIENTS WITH SURGICALLY CORRECTED TETRALOGY OF FALLOT
D. Raine1, J. O’Sullivan1, M. Chaudhari1, L. Hamilton2, A. Hasan2, J. Bourke1. 1Department of Paediatric Cardiology, Freeman Hospital, Newcastle upon Tyne, UK; 2Department of Paediatric Cardiothoracic Surgery, Freeman Hospital, Newcastle upon Tyne, UK
Introduction: The excellent long-term outcome following surgical correction of tetralogy of Fallot is hampered by the significant incidence of postoperative arrhythmias. Traditionally, the majority of research has been focused on ventricular arrhythmias due to the risk of sudden cardiac death. However, the prevalence of atrial tachyarrhythmias in these patients has recently been reported to be as high as 34% which, combined with the higher frequency of associated symptoms and morbidity, has resulted in a significant shift in the focus of research within this subject. The aim of this analysis was to characterise the mechanisms and circuit locations of atrial tachyarrhythmias in this patient group using computer assisted electrophysiology mapping techniques.
Abstract 143
Methods: Consecutive patients with surgically corrected tetralogy of Fallot and atrial tachyarrhythmias, who underwent computer assisted mapping and radiofrequency ablation procedures in the period from January 2001 to October 2006 at the Freeman Hospital, UK were identified retrospectively from case notes and electrophysiological case records. Computer assisted mapping of atrial tachyarrhythmias was performed in all using either EnSite (St Jude Medical Inc) arrhythmia mapping and intracardiac catheter guidance system or CARTO (Biosense Webster Inc) electroanatomical system.
Results: Ten patients (4 male; mean age at first ablation procedure 38 (8) years) were included. Mean age at surgical correction was 9 (7) years and the mean interval between corrective surgery and onset of atrial tachyarrhythmia was 24 (9) years. Mean number of ablation procedures was 2 (1) per patient with EnSite being used on 7 and CARTO on 5 patients. One patient had undergone a conventional right atrial flutter ablation procedure prior to their first computer assisted mapping procedure. Total number of separate atrial tachyarrhythmia loci/circuits identified was 27 (10 macro-reentrant, 3 micro-reentrant, 14 focal). Mean duration of follow-up was 21 (14) months. Five patients required pacing for sinus and/or AV node disease, 4 required additional surgery post ablation and 8 still require antiarrhythmic drug therapy. Key patient characteristics are summarised in the table.
Conclusions: Patients with surgically corrected tetralogy of Fallot continue to present a significant challenge to the electrophysiologist. Typically, they have multiple tachyarrhythmia circuits with differing mechanisms of initiation and propagation arising from highly scarred right atria, which can be difficult to induce. It is unwise to guarantee total abolition of arrhythmia and thus management still needs to be hybrid, comprising pharmacology, pacing, ablation and surgery, tailored to the individual patient’s needs.
tetralogy of Fallot; atrial arrhythmia; electroanatomical mapping
144 CAN UNSTABLE ARRHYTHMIAS BE DETECTED BY CHANGES IN INTRACARDIAC IMPEDANCE?
T. Mudawi1, G. Kaye2, T. Houghton3, M. Lippert4, G. Czygan4, D. Edgar5. 1Cardio-Thoracic Centre, Liverpool, UK; 2Princess Alexandra Hospital, Woolloongabba, Australia; 3Hull Royal Infirmary, Hull, UK; 4Biotronik GmbH & Co KG, Erlangen, Germany; 5Biotronik UK, Bicester, UK
Introduction: Implantable defibrillators (ICDs) are currently unable to assess the haemodynamic stability of arrhythmias and can occasionally deliver intracardiac shocks when patients are conscious. We investigated the use of left ventricular (LV) impedance as a haemodynamic sensor during arrhythmias in man.
Methodology: LV impedance and systemic blood pressure were continuously monitored during clinical VT stimulation studies. LV impedance was measured by injecting a biphasic rectangular current pulse of 600 µA amplitude at a sampling rate of 128 Hz between the proximal poles of a standard quadrapolar pacing/recording electrode at the right ventricular apex, and the proximal poles of a decapolar catheter positioned within the coronary sinus. Current was injected using an external pacemaker (INOS, Biotronik) connected to the poles of the RV and CS catheters (see fig).
Results: Thirty patients were studied. Unstable VT: 3 (10%), stable VT: 2 (7%), SVT: 3 (10%). Haemodynamically unstable arrhythmias were defined as those causing systemic hypotension (BP<90 mmHg), and those needing urgent cardioversion for loss of consciousness. The stroke impedance (the difference between the end systolic and end diastolic impedance) over 8 sinus/paced/arrhythmia cycles, correlates significantly with the arterial pulse pressure amplitude with a coefficient of r = 0.78 (0.22). Prolonged averaging (for an episode of >1 min duration of sinus rhythm, pacing or arrhythmia) resulted in a mean correlation coefficient of r = 0.86 (0.27).
Conclusion: LV impedance can assess the pumping efficacy of the heart during sinus rhythm, ventricular pacing and ventricular arrhythmias, and correlates well with changes in pulse pressure. Further studies are needed to determine the long-term stability of LV-impedance measurement.
arrhythmias; intracardiac impedance; haemodynamics
145 WHY DO SOME PATIENTS WITH WOLFF–PARKINSON–WHITE SYNDROME PRESENT LATER IN LIFE?
L. Boodhoo, D. Pradhan, M. Hall, R. Snowdon, J. Waktare, D. Todd. The Cardiothoracic Centre, Liverpool, UK
Background: Atrioventricular reentrant tachycardia (AVRT) commonly presents during childhood or adolescence, but a significant proportion of patients present in later years. We hypothesised that electrophysiological mechanisms that prolong tachycardia cycle length (TCL), thereby stabilising tachycardia, may explain why some patients present in later life.
Abstract 145
Methods: The electrophysiology studies of 100 consecutive patients with AVRT performed at a single centre between 2004 and 2006 were retrospectively examined for tachycardia cycle length prolonging features. We defined TCL prolonging features as: (a) dual AV nodal physiology, defined as an increase in AH interval by 50 ms with a decrease in atrial extrastimulus coupling interval of 10 ms, and (b) the presence of bundle branch block (BBB) ipsilateral to the side of the accessory pathway during tachycardia.
Results: Dual AV physiology was found in 20 (20%), and ipsilateral BBB during tachycardia in 3 (3%) of patients undergoing ablation. AVRT patients with dual AV nodal physiology were significantly older at the onset of symptoms than patients without dual AV nodal physiology. (28.7 vs 21.1 years, p = 0.04). These patients were also significantly older at ablation (41.2 vs 29.7 years, p<0.01). The TCL was significantly longer in the group with dual AV nodal physiology (362 ms vs 314 ms, p = 0.001). No differences in these parameters were found between AVRT patients with ipsilateral BBB and AVRT-only patients.
Conclusion: The presence of dual AV nodal physiology in patients with AVRT is associated with longer tachycardia cycle length, and presentation at a later age. The development of dual AV physiology later in life may provide a mechanism by which AVRT is stabilised thereby promoting symptoms.
atrioventricular re-entrant tachycardia; dual AV nodal physiology; bundle branch block
146 CT GUIDED TRANSSEPTAL LEFT HEART CATHETERISATION FOR LEFT ATRIAL ABLATION: A NOVEL TECHNIQUE
L. Graham1, I. Melton2, S. MacDonald3, I. Crozier2. 1Yorkshire Heart Centre, Leeds General Infirmary, Leeds, UK; 2Department of Cardiac Electrophysiology, Christchurch Hospital, Christchurch, New Zealand; 3Department of Radiology, Christchurch Hospital, Christchurch, New Zealand
Introduction: Transseptal left heart catheterisation can be a difficult procedure and is not without risk of serious complications. The purpose of this study was to prospectively evaluate the role of three-dimensional (3D) multidetector row computed tomography (MDCT) to localise the fossa ovalis (FO) and facilitate transseptal puncture in patients undergoing left atrial catheter ablation.
Methods: Fourteen consecutive patients undergoing left atrial ablation were studied. 13 patients underwent pulmonary vein isolation (PVI) and 1 patient had ablation for left atrial flutter. All patients routinely underwent 3D MDCT imaging of the heart and pulmonary veins pre-ablation for use in conjunction with electroanatomic mapping. The FO was identified on transverse images and marked using a 10 mm marker sphere, which was then converted to a 3D volume rendering. Prior to puncture of the interatrial septum, standard fluoroscopic views of the transseptal sheath were compared to the corresponding 3D MDCT images localising the FO. Data are expressed as mean (standard deviation).
Results: Successful, uncomplicated transseptal puncture was achieved in all 14 patients. The mean duration of transseptal puncture was 15.6 (10.0) min and the average fluoroscopy time was 8.5 (7.4) min. The MDCT images were deemed helpful in assisting the transseptal puncture in 13 patients (93%).
Conclusion: This study demonstrates the feasibility of using 3D multidetector row MDCT to localise the FO and aid transseptal puncture. For patients undergoing left atrial catheter ablation in whom MDCT imaging is routinely performed pre-ablation, additional tagging of the FO can be easily performed and is a novel tool for guiding transseptal catheterisation without additional risk.
transseptal catheterisation; computerised tomography; left atrial catheter ablation
147 VIDEO-ASSISTED THORACOSCOPIC ABLATION FOR TREATMENT OF ATRIAL FIBRILLATION
V. Avlonitis, S. Murray, S. Hunter. James Cook University Hospital, Middlesbrough, UK
Introduction: The video-assisted thoracoscopic (VAT) ablation is a new technique for treatment of atrial fibrillation (AF). We reviewed our experience.
Methods: From 09/2003–08/2006, 40 symptomatic lone AF patients were scheduled for VAT microwave ablation. Data were collected prospectively.
Results: One patient was cancelled for anaesthetic problems, 31 had VAT (26 complete ablations, 5 abandoned), 8 converted to sternotomy intraoperatively (75% of conversions occurred during first half of cohort). Of 26 complete VAT procedures, 14 had paroxysmal AF, 8 persistent, 4 permanent. Of the paroxysmals, 10 (71.4%) were cured; 4 after subsequent additional catheter ablation for postoperative cavotricuspid-isthmus-dependent right atrial flutter (CTIRAF). In 3, AF recurred: 2 had additional catheter pulmonary vein isolation (CPVI), successful in 1; the third opted for atrioventricular node ablation. One was lost to follow-up. Of the persistents, 6 (75%) were cured; 1 after additional CTIRAF ablation. In 1, AF recurred and 1 was lost to follow-up. Of the permanents, 1 was cured after additional CTIRAF ablation and 1 after CPVI. One had postoperative flutter and is awaiting cardioversion. One remains in AF. All AF recurrences had 60 seconds ablation during VAT ablation. Ablation was recently increased to 120 seconds and results are awaited. Median hospital stay was 4 days. In-hospital mortality was 0%.
Conclusions: VAT ablation is a promising minimally invasive procedure for treatment of AF. None of the patients had postoperative left atrial flutter. Postoperative CTIRAF is common but can be easily treated with catheter ablation. Close collaboration between surgeons and electrophysiologists is necessary. With this approach, 71–75% of patients with paroxysmal/persistent AF can be cured. Our understanding of the technique is improving and with longer ablation time we expect even better cure rates.
atrial fibrillation; video-assisted thoracoscopy; catheter ablation
148 INITIAL EXPERIENCE OF CATHETER ABLATION USING A NOVEL REMOTELY STEERABLE CATHETER SHEATH SYSTEM
M. Koa-Wing1, P. Kanagaratnam1, D. Wallace2, P. Lim1, B. Willis3, L. Alton3, K. Aston3, P. Sciberras3, P. Kojodjojo1, M. Wright3, R. Kaba3, N. Peters1, D. Davies3. 1St Mary’s Hospital and Imperial College, London, UK; 2Hansen Medical, Inc, Mountain View, United States; 3St Mary’s Hospital, London, UK
Background: A novel remotely controlled steerable catheter sheath system (Hansen Medical, Inc, California, USA) enables precise positioning and manipulation of any 7F electrophysiological catheter within any cardiac chamber for the purposes of mapping and ablation. The system uses a “master-slave” electromechanical system (Sensei Robotic Catheter System) that controls a steerable guide catheter (Artisan Control Catheter) within the heart (fig 1). We report our initial experience of the safety and feasibility of this system for remotely performing catheter ablation.
Abstract 148 Table 1
Abstract 148 Table 2
Methods: Ten consecutive patients undergoing elective catheter ablation procedures were recruited (table). Routine multipolar catheters were used to map a left sided accessory pathway, typical atrial flutter and atrial fibrillation. Additional 3D mapping techniques were used in seven patients. The Artisan Control Catheter was inserted into the right femoral vein through a 14F sheath. Irrigated-tip Navistar Thermocool and non-irrigated-tip EPT Blazer II™ catheters were used through the lumen of the Artisan catheter for ablation. Conventional endpoints of loss of accessory pathway conduction, bidirectional cavo-tricuspid isthmus conduction block and electrical isolation of all pulmonary veins were used to determine procedural success.
Results: All procedural endpoints (table 2 and fig 2) were achieved using the Sensei Robotic Control System without manual manipulation of the ablation catheter and without complication. A radiation dosimeter (Mydose Mini X, Aloka Co Ltd, Japan) positioned at the Sensei master console approximately 2.7 metres away from the x ray source showed negligible exposure despite a mean cumulative dose of 7281.4 cGycm2 to the patient.
Conclusions: The Sensei Robotic Control System in combination with the Artisan Control Catheter enables safe and clinically effective remote navigation of conventional 7F mapping and ablation catheters and reduces operator radiation exposure.
catheter ablation; remote; robot
149 DEMONSTRATION OF CORONARY VENOUS ANATOMY USING CARDIAC MRI
J. Younger, A. Crean, S. Plein, S. Ball, J. Greenwood. Leeds University, Leeds, UK
Objectives: We sought to evaluate the ability of cardiac MRI to demonstrate the anatomy of the coronary venous system.
Background: Cardiac MRI is useful in the diagnosis and management of patients with impaired left ventricular (LV) function, providing information about anatomy, function, perfusion, and viability. Cardiac resynchronisation therapy (CRT), an established treatment of LV dysfunction, requires the deployment of a left ventricular pacing lead via the coronary sinus to a branch of the cardiac venous system. Knowledge of coronary venous anatomy, and the presence or absence of suitable veins for CRT, may be useful in the management of patients referred for cardiac MRI to investigate heart failure. Although coronary veins can be seen by cardiac CT, they are not routinely demonstrated with conventional cardiac MRI protocols.
Methods: The cardiac MRI scans of 30 patients (21 men; mean age 58.2 (11.1) years) were studied. All scans had been performed on a 1.5 T MR scanner (Gyroscan Intera CV, Philips Medical Systems, Best, the Netherlands), and were requested for assessment of known or suspected ischemic heart disease. All scans were judged suitable for coronary imaging, and performed as part of a comprehensive protocol involving LV function, perfusion and delayed enhancement imaging. A 3D volume stack was acquired, using a single diaphragmatic navigator, using an SSFP sequence with a fat suppression and T2 preparation prepulses (TR/TE/flip angle 4.6/2.3/100; spatial resolution 1.18×1.18×1.80 mm). The scans were commenced after first pass perfusion imaging with intravenous administration of 0.05 mmol/kg of a gadolinium based contrast agent. The sequences were reviewed on a ViewForum Workstation (Philip’s Medical Systems) equipped with a dedicated cardiac analysis package and volume rendering tools. The ability to visualise the coronary sinus (CS), anatomical variants and the presence of an LV branch after volume rendering were recorded. The diameter of the CS ostium on the axial images, and the uninterrupted distance from this point to the most distal demonstrable end of a cardiac vein on the volume rendered image was measured.
Results: Continuous data are presented as mean (standard deviation). The coronary sinus was demonstrated in all patients. The average diameter of the CS ostium was 11.5 (4.2) mm. The mean distance for which continuous vein could be visualised from the ostium of the CS was 81.5 (43.6) mm. An LV branch was demonstrated in 22 (71%) patients and an anterior interventricular branch was seen in 14 (45%) patients.
Conclusions: The anatomy of coronary veins can be reliably imaged by cardiac MRI in a manner similar to CT. This technique may prove a useful addition to the already impressive armamentarium of cardiac MRI for the assessment of patients with left ventricular dysfunction.
cardiac MRI; cardiac veins; heart failure
150 THE FEASIBILITY OF WHOLE HEART MAGNETIC RESONANCE CORONARY ANGIOGRAPHY TO DETERMINE THE COURSE OF ANOMALOUS CORONARY ARTERIES
J. Younger, A. Crean, S. Ball, S. Plein, J. Greenwood. Leeds University, Leeds, UK
Background: Anomalous coronaries are present in 1% of the population and may be associated with sudden death, particularly if the aberrant vessel courses between the aorta and right ventricular outflow tract (RVOT) to supply the left coronary distribution. Although the course of these vessels can be demonstrated both by CT and by cardiac magnetic resonance imaging, traditional magnetic resonance coronary angiography (MRCA) is a time consuming examination that requires multiple, double oblique, three-dimensional (3D) acquisitions that are targeted to the likely course of the coronary. A recently introduced technique allows visualisation of all three coronary arteries with a single 3D volume acquisition. This “whole heart coronary imaging” (WHCA) uses a navigator-gated sequence to generate a 3D volume stack, which can subsequently be analysed as axial slices or reformatted to produce multi-planer, or volume rendered images.
Abstract 150 Number and type of sequences performed on each patient
Aims: To evaluate the utility of WHCA to define the proximal course of anomalous coronary arteries.
Methods: Between April 2006 and November 2006 seven patients who were referred for cardiac MRI because of known or suspected anomalous coronaries were evaluated by both traditional targeted acquisitions which were either navigated free breathing or breath hold, and with WHCA. WHCA was performed with a sufficient number of transverse slices to cover the proximal course of the anomalous coronary using an SSFP sequence with a fat suppression and T2 preparation prepulses TR/TE/flip angle 4.6/2.3/100 and spatial resolution was 1.18×1.18×1.80 mm. Both sets of images were then assessed independently for visual quality of the coronary images and diagnostic ability. The sequence which most clearly and unequivocally defined the course of the vessel was judged superior.
Results: Thirty four sequences were used in the 7 patients, of which 24 were targeted. Ten of these targeted acquisitions provided unambiguous diagnostic images, but in 3 patients the multiple targeted sequences were unable to adequately demonstrate the course of the anomalous vessel. Nine WHCA sequences were performed, of which only one did not provide diagnostic images. Image quality was assessed as superior for the targeted sequences in 2 patients, for the WHCA in 3 patients and equivalent in 2 patients.
Conclusions: Magnetic resonance WHCA is feasible in patients with anomalous coronary arteries. It provides diagnostic quality images in the majority of cases. As it does not require complex planning, WHCA may be preferable as the initial sequence to demonstrate anomalous vessels.
cardiac MRI; coronary imaging; anomalous coronary
151 DETERMINANTS OF PROGRESSION OF CORONARY ARTERY CALCIFICATION IN TYPE 2 DIABETES
D. Anand1, E. Lim1, D. Hopkins2, D. Darko3, D. Lipkin1, R. Corder4, A. Lahiri1. 1Cardiac Imaging and Research centre, Wellington Hospital, London, UK; 2King’s College Hospital, London, UK; 3Central Middlesex Hospital, London, UK; 4William Harvey Research Institute, London, UK
Background: Type 2 diabetes is associated with accelerated atherosclerosis and considered a coronary heart disease (CHD) equivalent. Coronary artery calcification (CAC) measured by cardiac CT has evolved into a useful tool for risk prediction in patients with and without diabetes. Initial studies suggest that progression of CAC is associated with an unfavourable prognosis especially in patients with diabetes. We prospectively evaluated the clinical determinants of CAC progression in type 2 diabetic subjects without previous CHD.
Methods: 398 asymptomatic type 2 diabetic subjects (mean age 52 (8) years, 61% male, mean HbA1c 8 (1.5)) were evaluated serially by coronary calcium imaging (mean follow-up 2.5 (0.4) years) using an electron beam CT scanner. Progression/regression of CAC score was defined as a change in square root transformed volumetric CAC score ⩾2.5 cubic mm, based on previously published data. Demographic data, cardiovascular risk factors, glycaemic control, medication use, biomarkers of inflammation (high sensitivity-C reactive protein (hs-CRP) and interleukin-6 (IL-6)) and vascular calcification (osteoprotegerin (OPG) and osteopontin (OPN)) were measured at baseline and during follow-up.
Results: At baseline CAC was present in 211 patients (53%). Progression of CAC was found in 119 patients (29.9%). The likelihood and magnitude of progression increased with increasing baseline CAC severity. Regression of CAC was seen in 3 patients (0.8%). Hs-CRP and IL-6 levels did not correlate with the extent of baseline CAC (r = 0.02 and 0.09 respectively). Plasma OPG levels were positively correlated with age, duration of diabetes and the severity of CAC at baseline (0.42, p<0.0001). Age, male gender, presence of hypertension, baseline HbA1c, CAC score, serum IL-6 and plasma OPG were univariate predictors of CAC progression. In a multivariate logistic regression model adjusted for baseline CAC (p<0.0001), serum HbA1c (odds ratio (OR) = 10.5 (95% CI 2.04 to 53.9), p = 0.02), plasma OPG (OR = 2.50 (1.19 to 5.22), p = 0.02) and IL-6 (OR = 2.06 (1.13 to 3.75), p = 0.05) were independent predictors of CAC progression. Patients in the highest tertile of plasma OPG (>9 pmol/l) had a 2.5-fold increased risk of CAC progression in comparison to those in the lowest tertile of OPG (0–5.2 pmol/l).
Conclusion: Progression of CAC was frequent in those subjects with pre-existing CAC and unlikely in patients without significant baseline CAC at an average follow-up of 2.5 years. Suboptimal glycaemic control was a strong risk factor for progression of CAC in asymptomatic type 2 diabetic subjects. Of the biomarkers studied, only plasma OPG levels predicted the extent of coronary atherosclerotic plaque burden and its progression.
coronary calcium; type 2 diabetes; osteoprotegerin
152 CORONARY CALCIFICATION IN TYPE 2 DIABETES PATIENTS IS ASSOCIATED WITH AN INCREASED RISK OF MYOCARDIAL ISCHAEMIA COMPARED TO NON-DIABETIC PATIENTS
E. Lim1, F. Ghani1, P. Jain1, D. Anand1, J. Kooner2, A. Lahiri1. 1Cardiac Imaging Department, Wellington Hospital, London, UK; 2Ealing Hospital, London, UK
Background: In retrospective studies involved mixed populations of diabetic and non-diabetic subjects, coronary calcification has been shown to be closely associated with myocardial ischaemia. In our previous work involving exclusively diabetic subjects, we have observed significantly more ischaemia at similar levels of coronary calcification than has been reported in the literature in mixed populations. Since diabetes is known to affect the atherogenesis process at multiple levels, we hypothesised that diabetes may be an independent risk factor which increases the likelihood of myocardial ischaemia for any given level of coronary artery calcification.
Methods: Subjects were recruited from two ongoing prospective studies of coronary artery calcification (one representing a population cohort study of asymptomatic subjects drawn from the local community, one representing a type 2 diabetic clinic population). Subjects had no evidence of clinical cardiovascular disease at baseline (no prior history of acute coronary syndrome, myocardial infarction, cerebrovascular disease or peripheral artery disease, normal electrocardiogram). Subjects with at least 100 Agatston units of coronary artery calcification were invited for a 2-day symptom-limited dipyrimadole/treadmill stress-rest gated Tc-99m sestamibi SPECT myocardial perfusion scan.
Results: 209 diabetic, 101 non-diabetic subjects were recruited (mean age 58, 75% male). Mean coronary artery calcium score was 613, 20% of myocardial perfusion scans were abnormal. In a multivariable logistic regression model included the established cardiovascular risk factors and coronary artery calcium score, only the coronary artery calcium score and diabetes were independent predictors of abnormal myocardial perfusion (p = 0.03, OR = 3.1, 95% CI 1.1 to 8.3).
Conclusion: This study suggests that subjects with type 2 diabetes appear to have a significantly elevated risk of myocardial ischaemia compared to non-diabetic subjects with similar levels of coronary artery calcification. This difference was not explained by the other established cardiovascular risk factors.
diabetes; myocardial perfusion scintigraphy; coronary calcification
153 PREDICTORS OF PROGRESSION OF CORONARY ARTERY CALCIUM IN TYPE 2 DIABETES: THE PREDICT STUDY
M. Flather1, M. Rubens1, I. Godsland2, M. Feher3, F. Nugara1, W. Richmond2, R. Elkeles2. 1Royal Brompton Hospital, London, UK; 2Imperial College London and St Mary’s Hospital, London, UK; 3Chelsea and Westminster Hospital, London, UK
Background: The PREDICT Study aims to determine whether coronary artery calcium score (CACS) measured by electron beam tomography can enhance the prediction of cardiovascular events in type 2 diabetic subjects beyond that of other risk factors.
Methods: Baseline measurements of CACS were made in 589 patients in the cohort. In 202 patients a further measurement of CACS was made 2.1 to 5.0 years after baseline (mean 3.9), enabling analysis of predictors of progression of calcification in patients with diabetes.
Results: The CACS follow-up group was highly comparable with the cohort as a whole. Median baseline CACS in the follow-up group was 78 (range 0–3402). CACS regressed or did not change in 32 patients (mean change −8, range −103 to 0) and progressed in 165 patients (mean change +216, range 1 to 1440). Follow-up CACS correlated with baseline CACS (r = 0.94, p<0.0001). Logistic regression predictors of progression were male gender (p = 0.02), ex-smoking (p = 0.02), age (p = 0.04), waist circumference (p = 0.04), waist:hip ratio (p = 0.003), systolic blood pressure (p = 0.002), low HDL cholesterol (p = 0.01), low apolipoprotein AI (p = 0.003), use of antihypertensive agents (p = 0.03) and baseline CACS (p<0.001). Predictors independent of baseline CACS, age and duration of follow-up were waist:hip ratio, systolic blood pressure, low apolipoprotein AI and use of antihypertensive agents. In continuous regression analysis baseline CACS (p<0.001) and weight (p = 0.03) were the only independent predictors of change in CACS.
Conclusions: Central body fat, blood pressure and low apolipoprotein AI contribute to coronary artery calcium progression. Baseline coronary calcium score is, however, the major determinant.
1Royal Brompton Hospital, London, UK; 2Imperial College London and St Mary’s Hospital, London, UK; 3Chelsea and Westminster Hospital, London, UK
coronary artery calcification; diabetes; electron beam computed tomography
154 EFFECTS OF OFF-PUMP VERSUS ON-PUMP CORONARY ARTERY BYPASS SURGERY ON EARLY AND LATE RIGHT VENTRICULAR FUNCTION AS ASSESSED BY CARDIAC MRI
T. Pegg, J. Selvanayagam, T. Karamitsos, J. Arnold, S. Neubauer, D. Taggart. University of Oxford, Oxford, UK
Abstract 154
Background: Right ventricular (RV) function is a major determinant of outcome following cardiac surgery. There is uncertainty as to the effect of coronary artery bypass grafting (CABG) on recovery of RV function, whether done as an off-pump (OPCABG) or on-pump (ONCABG), procedure because studies of the right ventricle are inherently limited by its complexity and the poor reproducibility of conventional assessments. Using the gold standard of cardiac magnetic resonance imaging (CMR) we investigated the effects of OPCABG and ONCABG on RV function.
Methods: In a single-centre randomised trial, 60 patients with normal ventricular function undergoing multivessel total arterial revascularisation were randomly assigned to OPCABG or ONCABG. Patients underwent 1.5 Tesla MRI for assessment of RV function preoperatively, prior to discharge and at 6 months. After piloting, steady-state free precession cine images (TE/TR 1.5/3.0 ms, flip angle 60°) were acquired in the short axis plane, slice thickness 7 mm, inter-slice gap 3 mm. The short axis stack was analysed using Argus (Version 2002B, Siemens Medical Solutions) by a single experienced cardiologist blinded to the surgical randomisation and scan order. All volumes were corrected for body surface area. Data were analysed using SPSS and based on intention to treat from the point of randomisation.
Results: Preoperative characteristics did not differ significantly between the two groups, table 1 (right ventricular stroke volume index ml (RVSVI): OPCABG 49 (9), ONCABG 50 (15), p = 0.7). There were no differences between the mean number of distal anastomoses (2.8 (0.9) OPCABG, and 2.8 (0.9) ONCABG, p = NS). All grafts in the OPCABG group were arterial as were 97% in the ONCABG, p = NS. In the ONCABG group the mean aortic cross clamp time was 41 (13) min, and cardiopulmonary bypass time was 57 (18) min. Of the 60 patients recruited into the trial, 51 patients were included in the final analysis (26 OPCABG, 25 ONCABG). Two were unable to undergo the postoperative scan because of serious postoperative morbidity. Three patients declined follow-up imaging, and four patients could not be included as the postoperative scan was affected by significant artefact. The median interval between surgery and the second CMR scan was 6 days (4–16) in the ONCABG group, and also 6 days (5–10) in the OPCABG group. The main finding of this study is that RV function is impaired shortly after coronary artery bypass surgery. The fall in RVSVI was significant, 10 (10) ml in the ONCABG group and 13 (9) ml in the OPCABG group (p<0.01), but the difference between the surgical techniques was not significant (p = 0.2). This effect is completely reversed at 6 months, figure 1.
Conclusions: This is the first study assessing RV function with CMR. We found that RV function is impaired early following CABG and recovers by 6 months, and that the changes were similar in both the OPCABG and ONCABG groups.
cardiac magnetic resonance imaging; right ventricular function; coronary artery bypass surgery
155 EFFECTIVE RADIATION DOSE IN ANGIOGRAPHY OF CORONARY ARTERY BYPASS GRAFTS USING MULTISLICE COMPUTED TOMOGRAPHY
D. Smith1, I. Negus2, M. Hamilton2, A. Baumbach3. 1Gloucestershire Royal Hospital NHS Trust, Gloucester, UK; 2Bristol Royal Infirmary, Bristol, UK; 3Bristol Heart Institute, Bristol, UK
Objectives: We aim to evaluate effective radiation dose in a series of 113 coronary artery bypass graft patients undergoing coronary angiography using 16-slice computerised tomography (MSCT).
Methods: We used a Siemens Sensation 16 (Siemens, Forchheim, Germany) software version 70A with retrospective electrocardiogram-gated reconstruction. Parameters are shown in table 1. Scan sequence was as follows: Topogram, Calcium Scoring Scan, Test Bolus at level of the pulmonary trunk, 20 ml of Iomeron at 4 ml/sec until peak opacification, Angiogram caudocranial to level of sternoclavicular joint to include any internal mammary artery origins, timing of 105 ml Iomeron 4 ml/sec determined by test bolus scan. The radiation dose calculation used the Computed Tomography Dose Index (CTDI) which is the radiation dose within a single slice. We measured CTDI free in air for our scanner using a calibrated ionisation chamber. The effective dose accounts for the radiation type and the organs irradiated and is proportional to the risk of inducing a fatal cancer. We applied published conversion factors specific to the scanner from NRPB to measured CTDI to give effective dose. These factors use Monte Carlo modelling (Cristy). All methods of calculating effective dose are estimates.
Abstract 155 Table 1
Abstract 155 Table 2
Results: Of 113 patients, 97 were male with an overall mean age of 68 (8.6) years. Mean basal metabolic index was 28.1 (4.5) kg/m2 and mean heart rate 64.8 (8.7) bpm. Effective radiation doses are presented in table 2.
Conclusions: The International Commission on Radiological Protection suggests an additional lifetime risk of fatal cancer of 1 in 20 000 per millisievert for the population. Hence, a CT head represents an additional risk of 1 in 10 000, native invasive coronary angiography (ICA) 1 in 3600, native MSCT 1 in 1400 and graft MSCT 1 in 950. Compared to an individual’s risk this is small. Our mean age was 68 and hence this is likely to be an overestimate. There are methods to minimise this effective dose: ECG-dependent dose modulation can reduce MSCT dose by 40%; New dual-source scanners have been reported to achieve up to 50% dose reductions. Hence in suitable patients, the resultant effective dose may only be a few millisieverts greater than invasive coronary angiography on the same patient. Furthermore, one should offset this against the well-documented risks inherent in ICA. A recent report calculated the overall risk of radiogenic and non-radiogenic mortality of ICA was double that for MSCT. Angiography of coronary artery bypass grafts using MSCT delivers a relatively high radiation dose and this should be carefully considered in its justification. In practice operators should make every effort to keep exposure to a minimum, though advancing CT technology may be able to bring effective doses down to levels comparable with ICA.
effective radiation dose; coronary artery bypass graft; multislice computed tomography
156 REVASCULARISATION FOR ISCHAEMIC MYOCARDIAL DYSFUNCTION LEADING TO AN IMPROVEMENT IN EJECTION FRACTION IS NOT ASSOCIATED WITH AN INCREASE IN LONG AXIS TISSUE DOPPLER VELOCITY
S. Khan, P. Heck, S. Hoole, D. Dutka. Addenbrooke’s Hospital, Cambridge, UK
Introduction: There is an increasing group of patients with ischaemic left ventricular dysfunction who do not have limiting angina. Revascularisation, in addition to optimum medical therapy, ameliorates symptoms and improves prognosis and left ventricular performance as measured by resting ejection fraction. Myocardial colour tissue Doppler velocities may also be used to assess left ventricular performance. We postulated that revascularisation for ischaemic left ventricular dysfunction would be associated with an improvement in long axis tissue Doppler systolic velocities at rest and during peak dobutamine stress.
Abstract 156
Methods: Seventeen patients with ischaemic left ventricular dysfunction who underwent revascularisarion according to our standard clinical protocol, participated in this study. Dobutamine stress echocardiography (GE Medical systems, Vivid 7) was performed at baseline and 6 months post revascularisation. Digital ultrasound images of the left ventricle were acquired with tissue Doppler at each stage and analysed off-line. Peak systolic velocity (Vs) at the mitral annulus was recorded for the septum, lateral, anterior and inferior walls from the apical 2 and 4 chamber views. The ejection fraction was calculated using Simpson’s modified biplane method.
Results: During dobutamine stress at baseline and follow-up there were increments in peak systolic velocity, confirming contractile reserve. The ejection fraction improved from 28.9 (6.8)% at baseline to 37.9 (9.8)% at 6 months (p<0.05), however there was no change in peak systolic velocities either at rest or during stress (p = NS for all myocardial regions) (table). This study suggests that long axis tissue Doppler velocity should not be used as a measure of improvement in contractile function following revascularisation in ischaemic cardiomyopathy.
cardiomyopathy; tissue Doppler; stress echocardiography
157 MYOFIBRILLAR OEDEMA CAUSES POST-ISCHAEMIC MYOCARDIAL DYSFUNCTION
T. Bragadeesh1, R. Jayaweera2, E. Le2, C. Kramer3, F. Epstein2, S. Kaul2. 1Castle Hill Hospital, Kingston-Upon-Hull, UK; 2Oregon Health Sciences University, Portland, USA; 3University of Virginia, Charlottesville, USA
Background: We hypothesised that post-ischemic myocardial dysfunction (“stunning”) is due to myofibrillar oedema.
Methods and Results: In Group 1 pigs (n = 15), we produced myocardial stunning by repetitive ischemia and reperfusion and studied 5 pigs each 2 h, 2 days, and 5 days later. Circumferential left ventricular (LV) mid-wall myocardial strain (Ecc) was estimated in vivo using tagged magnetic resonance imaging. Myocardial water content (MWC) was measured postmortem from which interfilament lattice distance (d) was calculated. In Group 2 pigs (n = 6), we produced myocardial dysfunction by intracoronary administration of a mast cell degranulator. Animals were euthanised immediately upon induction of regional LV dysfunction, so as not to allow inflammation to develop. In Group 3 pigs (n = 4) we performed transmission electron microscopy (EM) to quantify d in stunned versus normal myocardium. MWC was elevated in the stunned compared to normal myocardium (p<0.02) and decreased over time. There was an inverse relation between Ecc and MWC in the stunned myocardium (r = −0.76) in the Group 1 pigs. Excellent inverse relations were noted between Ecc and d in Group 1 (r = −0.90) pigs and between wall thickening and increase in MWC in Group 2 (r = −0.84) pigs. In the Group 3 pigs, d on EM was 40 (3) nM in the normal myocardium, which was significantly (p<0.001) lower than that in the stunned myocardium (46.4 (4) nM).
Conclusions: Ischaemia reperfusion results in myocardial oedema, with consequent myocyte swelling and myofibrillar oedema. The latter leads to an increase in d causing myosin heads to either fail to latch on or to latch improperly on the actin filament with poor force generation, leading to myocardial dysfunction. As the myocardial oedema abates, myocyte function improves.
myocardial stunning; myocardial oedema; reperfusion
158 WHAT RISK OF DEATH WOULD YOU ACCEPT BEFORE HAVING AN IMPLANTABLE CARDIAC DEFIBRILLATOR?
C. Garratt. Manchester Heart Centre, Manchester, UK
Background: The clinical decision to implant an implantable cardioverter defibrillator (ICD) in a patient with one of the inherited sudden cardiac death syndromes is based on a balance between the perceived risks of sudden death in that patient and morbidity/possible mortality associated with the device. Although there are data available to assist in estimating sudden death risk (usually expressed as percentage risk of death/year) in these patients, the important question of the threshold that might trigger an ICD is a matter of debate. It could be argued that consultant electrophysiologists with a large experience of ICD implantations and follow-up would be best placed to make this judgement.
Methods: The following question was emailed to 71 consultant electrophysiologists/ICD implanters in the UK. “If you personally had a cardiac condition with a quantifiable risk of sudden death, and the only treatment was an ICD, what level of risk (in terms of percentage risk of death/year) would prompt you to have an ICD implanted? The question refers to your current age and it is assumed that this level of risk remains constant with time ie a 5%/year risk would mean that you would have a 50% chance of dying suddenly from the condition in the next 10 years.”
Results: Fifty electrophysiologists (49 male) responded to the email. The most commonly selected level of risk was 1%/year (44% of respondents), with a mean value of 2.47 (1.43) %/year. Older electrophysiologists (above 45 years old) selected a higher threshold of risk (mean 3.06 (1.38)%/year compared with 1.64 (1.08)%/year for those less than 45 years old, p<0.05), although 1% was the commonest level of risk selected in both the younger and older groups (52% and 32% respectively).
Conclusions: The majority of electrophysiologists/ICD implanters would wish to have an ICD if their risk of sudden death was estimated to be in the range of 1–3%/year or above. Older electrophysiologists would have a higher threshold for device implantation than their younger counterparts. These findings have relevance to the clinical threshold for ICD implantation in patients with inherited sudden cardiac death syndromes.
sudden death; defibrillator; risk assessment
159 INFLUENCE OF GENETIC TESTING ON IMPLANTATION OF IMPLANTABLE CARDIOVERTER DEFIBRILLATORS IN PATIENTS WITH SUSPECTED ION CHANNELOPATHIES
S. Collitt1, L. Kerzin-Starr1, N. Moreton1, K. Metcalfe1, W. Newman1, C. Garratt2. 1Regional Genetic Service, Manchester, UK; 2Manchester Heart Centre, Manchester, UK
Introduction: Genetic testing for ion channelopathies has been recommended as a strategy for screening family members of patients with these conditions. Concerns have been raised, however, that this is likely to result in a dramatic increase in costly implantable cardioverter defibrillator (ICD) implants.
Abstract 159
Methods: We reviewed the records of all patients with suspected ion channelopathies referred for genetic testing at a regional genetic unit over a 3 year period (August 2003–August 2006). We recorded details of clinical diagnosis, results of genetic testing, indications for ICD implantation (in those in whom it was undertaken) and clinical outcome.
Results: A total of 136 individuals from 47 families were screened (see table), of whom 34 had ICDs implanted. Ninety two patients actually underwent genetic testing, of which 38/92 were positive. Of those with a positive test, 9 had ICDs inserted. Indications for ICD implantation were a clinical history of cardiac arrest or ventricular fibrillation (24 patients), recurrent syncope despite beta-blockade (6 patients) or recurrent syncope and a contraindication to beta-blockade (2 patients). Two asymptomatic patients with LQTS had devices implanted prior to genetic testing because of an extremely strong family history of sudden death. In 8 of the 9 patients with both positive genetic tests and ICDs, the device was implanted before the result of genetic testing was known.
Conclusion: In patients with ion channelopathies, ICD implantation is nearly always based on the presenting or ongoing clinical picture rather than the results of genetic testing. Concerns about downstream ICD costs of genetic screening strategies in this patient population are unwarranted.
implantable cardioverter defibrillator; genetic; channelopathy
160 THE USE OF AMIODARONE IN IMPLANTABLE CARDIOVERTER DEFIBRILLATOR PATIENTS
A. Sandilands, T. Cripps. Bristol Royal Infirmary, Bristol, UK
Background: Implantable cardioverter defibrillators (ICDs) are most effective at improving mortality in patients with life threatening ventricular arrhythmias. Despite their use, the recurrence of ventricular arrhythmias and the development of atrial arrhythmias cannot be prevented. The use of adjunctive antiarrhythmic therapy can reduce the incidence of both appropriate and inappropriate defibrillator shocks. Despite the evidence on the effectiveness of amiodarone to reduce arrhythmias, there are no data to suggest its safety and efficacy in patients with ICDs.
Methods: We retrospectively analysed the pacing, medical and GP notes of patients currently under follow up in our ICD pacing clinic. The data retrieved included tolerability of amiodarone, number of appropriate or inappropriate shocks, ejection fraction at implant, the incidence of atrial arrhythmias together with the use of other anti-arrhythmic drugs.
Results: 209 patients (37 females, mean age at implant 61.9 (12.3) years) were followed up for a mean of 44.7 (27.4) months (range 9–132). 88 patients were treated with amiodarone (14 females, 71 ischaemic aetiology, mean age at implant 64.8 (12.2) years, ejection fraction 32.5 (0.8)% with 55 of these patients on β-blockers) compared to 121 patients not on amiodarone (23 females, 89 ischaemic aetiology, mean age at implant 59.8 (12.1) years, ejection fraction 34.1 (0.9)% with 100 of these patients on β-blockers). 25 patients (12%) had adverse effects from amiodarone including intolerability (3), lung fibrosis (3), skin sensitivity (2), thyroid disease (13) and reduction in cycle length of VT under device programmed detection zone (4). 15 (7.2%) of these patients had to discontinue the drug. Eight (3.8%) patients were using Class 1 anti-arrhythmics. During the follow-up period there were 31 patients with appropriate shocks and 17 patients had inappropriate shocks with 29 patients experiencing documented paroxysmal atrial arrythmias. Given these data, there was no significant difference in the number of patients with appropriate shocks in the amiodarone treated group vs non-amiodarone treated group (18.2% vs 12.4%, p = 0.313) which was maintained when comparing patients without atrial arrhythmias (15.9% vs 10.0%, p = 0.458) and in patients treated with β-blockers with no atrial arrhythmias (8% vs 8.3%, p = 0.637). There was a small but significant increase in the number of inappropriate shocks in the amiodarone group (13.6% vs 4.1%, p<0.05).
Conclusion: There would appear to be no extra benefit of amiodarone treatment in ICD patients in the long term identified in this cohort. We propose cessation of amiodarone treatment with substitution or increase with β-blockade if possible, in those patients with no recent shocks and with no evidence of atrial arrhythmias.
amiodarone; implantable cardioverter defibrillator; defibrillator shocks
161 A STUDY OF THE EFFECTIVENESS OF PUBLIC ACCESS DEFIBRILLATION IN URBAN AND RURAL POPULATIONS IN NORTHERN IRELAND: THE NORTHERN IRELAND PUBLIC ACCESS DEFIBRILLATION STUDY
M. Moore1, A. Hamilton1, K. Cairns2, B. Glover1, P. Ferguson1, D. Gray3, A. Marshall2, A. Adgey1, F. Kee3. 1Regional Medical Cardiology Centre, Royal Victoria Hospital, Belfast, UK; 2Department of Applied Mathematics, Queen’s University, Belfast, UK; 3Department of Epidemiology and Public Health, Queen’s University, Belfast, UK
Background: In Belfast City, 78% of out-of-hospital cardiac arrests (OHCAs) occur in the home and are not amenable to public access defibrillation (PAD) with automated external defibrillators (AEDs) in public places. The Northern Ireland Public Access Defribrillation (NIPAD) study examined mobile AEDs in urban and rural populations.
Methods: The urban (NWB) and rural (NN) areas each had populations of approximately 140 000. In year 1 (2004) we prospectively assessed the demographics of OHCA, including call to response interval (CRI) for the emergency medical services (EMS). In year 2 (2005) we deployed mobile AEDs, 29 in NWB and 42 in NN. In NWB 327 first responders (FRs), (267 lay, 60 police) and in NN 417 FRs, (347 lay, 70 police) were trained in AED use. Over 60% of FRs had CPR training. In year 2 FRs were dispatched to OHCAs via automated internet paging (AIP) in conjunction with the EMS.
Results: In NWB, year 1 there were 159 OHCAs, mean EMS CRI 6 min 58 sec (SD 3 min), initial rhythm ventricular fibrillation (VF) 28/159 (18%) and 22% were witnessed. In year 2 there were 154 OHCAs, VF 19/154 (12%). In year 2 FRs were paged to 162 events coded as OHCA and attended 113/162 (69.8%), 20/113 (17.7%) were reached before the EMS. The combined mean EMS/FR CRI for year 2 was 5 min 49 sec (SD 3 min) (p<0.001). In NWB survival rate was 5.2% in Year 1 and 3.2% in Year 2 (p = 1.0). In NN, year 1 there were 131 OHCAs, mean EMS CRI 10 min 54 sec (SD 6), VF 19/131 (14.5%) and 34% witnessed. In year 2 there were 93 OHCAs, VF 14/93 (15%), FRs were paged to 75 events coded as OHCA and attended 59/75 (78.7%). They attended 28/59 (47.5%) before the EMS. The combined mean EMS/FR CRI for year 2 was 7 min 40 sec (SD 4 min) (p<0.001). In NN survival rate was 2.5% in year 1 and 5.9% in year 2 (p = 0.11). In both areas FRs attended 172 events, reaching 48 (29.7%) before the EMS. Only 2/48 (4.2%) had VF as the initial rhythm on FR arrival.
Conclusion: Preliminary results have shown that mobile FRs had a significant impact on reducing the CRI in urban and rural areas, with a greater impact in the rural area. There was no impact on survival despite a high percentage of events being reached first by the FRs due to a low incidence of VF. Dispatch by AIP represents a novel method of AED delivery.
defibrillator; public access; cardiac arrest
162 PREVALENCE AND SIGNIFICANCE OF AN ISOLATED LONG QTC INTERVAL ON 12-LEAD ECG IN ELITE ATHLETES
S. Basavarajaiah1, M. Wilson2, A. Chlebinska2, A. Shah1, S. Sharma1. 1King’s College Hospital, London, UK; 2University Hospital Lewisham, London, UK
Background: Congenital long QT syndromes (LQTS) are relatively rare but a recognised cause of sudden cardiac death (SCD) in young athletes. Many individuals with congenital LQTS are asymptomatic and SCD may be the first presentation. The prevalence and significance of an isolated Long QTc (LQTc) interval on the 12-lead ECG in asymptomatic athletes has never been reported. Its identification represents a dilemma, since the diagnosis of congenital LQTS calls for permanent disqualification from competitive sports.
Methods: Between 2002 and 2006, 1400 elite asymptomatic athletes aged between 14–35 years (mean 20.26 (5.40) years) underwent 12-lead ECG as a part of pre-participation screening programme. 975 (69.64%) were male and 425 (30.35%) were female athletes. The QT interval was measured using callipers and corrected for the heart rate using Bazett’s formula (QTc). Athletes with LQTc (>440 ms in males and >460 ms in females) were investigated further with 24-holter monitor and an exercise stress test. All athletes with a LQTc were offered genetic testing and their first-degree relatives were offered a 12-lead ECG.
Results: Out of 1400 athletes, 6 (0.42%) (5 males and 1 female) athletes had LQTc interval. The QTc interval ranged from 460–580 msec. Two males and one female athlete had QTc interval >500 ms. None had a family history of syncope or SCD. Subsequent Holter monitoring did not reveal polymorphic ventricular tachycardia, but exercise stress testing demonstrated paradoxical prolongation of the QTc during the recovery phase in 2 (33%) of these athletes. Both had a QTc >500 msec and 1 had first degrees relatives with a LQTc on ECG and was gene positive for LQT1. None of the other athletes had family members with ECG abnormalities and the genetic results on these athletes for known LQT mutations have proved negative so far.
Conclusion: The prevalence of an isolated LQT on the ECG in asymptomatic athletes is 0.42%. One third of our athletes with a LQT had other phenotypic manifestations of the disorder and their QTc interval >500 msec was highly suggestive of LQTS. Our results indicate that the finding of an isolated LQTc is rare in athletes and warrants detailed investigations for congenital LQTS.
congenital long QT syndrome; elite athletes; sudden cardiac death
163 IMPLANTABLE CARDIOVERTER DEFIBRILLATOR SHOCKS: APPROPRIATE VERSUS INAPPROPRIATE IN MADIT II PATIENTS
G. Lin, P. Brady. Mayo Clinic, Rochester, Minnesota, USA
Background: The Multicenter Automatic Defibrillator Implantation Trial II (MADIT-II) established a mortality benefit with prophylactic implantable cardioverter defibrillator (ICD) implantation in patients with ischemic cardiomyopathy and ejection fraction <30%. However, the rate of appropriate ICD therapies in this group is not known. To determine this, we reviewed our single centre experience of patients meeting MADIT-II criteria for prophylactic ICD.
Methods: All consecutive patients meeting MADIT-II implant criteria at the Mayo Clinic in Rochester, MN from 2000–5 were included. Patients with non-ischaemic cardiomyopathy and those receiving cardiac resynchronisation therapy devices were excluded. Appropriate ICD therapies were defined as those triggered by a sustained ventricular arrhythmia, and inappropriate ICD therapies were defined as those triggered by sinus tachycardia, atrial fibrillation, or device malfunction. Rate of appropriate ICD therapies was determined with a Kaplan–Meier survival curve.
Results: Of 331 patients who met inclusion criteria, 281 had ⩾1 month of follow-up with a mean follow up time of 20±16 months. Mean age was 70±10 years, with 252 (90%) males. Ejection fraction, creatinine, and defibrillation threshold were 23%±5%, 1.52±0.05 g/dl, and 14±3, respectively. Of 134 (48%) patients who received a dual chamber ICD, 23 had complete heart block, 14 had high grade AV block, 8 had sinus node dysfunction, and 7 had AV node ablations. Over the follow-up period, 35 (12%) and 21 (7%) patients were appropriately treated with shocks and anti-tachycardia pacing, respectively, while 20 (7%) patients received inappropriate ICD therapies. The rate of appropriate ICD shock was 7% per year versus 4% inappropriate shocks per year (p = 0.04).
Conclusions: Rate of inappropriate ICD shocks in patients undergoing ICD implantation for MADIT II criteria is not low and is >50% of the rate of appropriate shocks. This rate of appropriate and inappropriate shocks needs to be considered when discussing primary prevention for sudden cardiac death in this population.
implantable cardioverter defibrillator; MADIT II; implantable cardioverter defibrillator therapies
164 IMPROVED SAFETY OF COMPLEX DEVICE IMPLANTATION CAN BE ACHIEVED USING SIMPLE RADIATION DOSE REDUCTION MANOEUVRES
D. Rogers, F. England, M. Dhinoja, R. Simon, M. Lowe, P. Lambiase, A. Chow. The Heart Hospital, London, UK
Introduction: Increasing numbers of implantable cardioverter defibrillators (ICDs) and biventricular (BiV) devices are being implanted worldwide. Implantation of these devices can involve long fluoroscopy screening times and consequently high radiation doses. Exposure to radiation carries potential risks to both patients and operators, including an increased risk of malignancy.
Methods: To assess the efficacy of simple dose reduction manoeuvres, the following changes were instigated for complex device implantations: (1) minimising fluoroscopy dose by reducing pulse rate and dose; (2) removal of secondary radiation grids; (3) optimising use of collimation; (4) maximising field of view; (5) halving frame rate for acquisitions from 12.5 to 6.25 frames per second. Radiation dose and screening time for device implantation procedures were compared for the periods 15 months before and 17 months after these changes. Procedures were classified as BiV (biventricular pacemakers or defibrillators) or ICD (dual or single chamber implantable defibrillators). Device replacement and revision procedures were excluded from analysis.
Results: A total of 624 procedures (484 ICD insertions, 140 biventricular device insertions) were analysed. Screening times were unchanged before and after dose reduction manoeuvres for both groups (ICD 7.1 (0.6) min vs 7.7 (0.9) min, p = NS; BiV 29.0 (2.0) min vs 30.9 (3.1) min, p = NS). Radiation exposure was reduced by 51% for ICD insertion and by 45% for BiV device insertion after dose reduction interventions (see graphs).
Conclusion: The radiation safety of device implantation procedures can be significantly improved by simple radiation reduction manoeuvres. These measures can halve the radiation doses without increasing screening time.
biventricular devices; defibrillator; radiation dose
165 AN AUDIT OF HIGH DOSE VS STANDARD DOSE LIPID-LOWERING THERAPY FOLLOWING ACUTE MYOCARDIAL INFARCTION: THE PATIENT COSTS RESULTING FROM A FINANCIALLY-MOTIVATED DRUG CHANGE IN NORTH STAFFORDSHIRE
R. Butler1, J. Wainwright2. 1University Hospital of North Staffordshire, Stoke on Trent, UK; 2Keele University Medical School, Stoke on Trent, UK
Introduction: There are robust data supporting high dose statins after acute coronary syndromes (ACS) (PROVE IT and MIRACL), in patients with established coronary heart disease (TNT IDEAL) and mechanistic studies (REVERSAL and ASTEROID) looking at plaque regression with IVUS.
Methods: Our department took a corporate decision to administer high dose statin therapy to high risk patients; post-MI and post-revascularisation (atorvastatin 80 mg or 40 mg). Due to mounting cost pressures within the local health economy, a decision was taken jointly between the local Primary Care Trusts (funders of health care) and the local NHS Trust (provider of secondary and tertiary health care) to suspend the prescription of atorvastatin and institute a switch to generic simvastatin 20–40 mg depending on the clinical scenario driven by the need to achieve cost savings. Despite clinical objections to this decision the change over occurred in September/October 2005.
Results: This presented an opportunity to audit the impact of this therapeutic change. Patients were identified who presented to our institution with a discharge diagnosis of myocardial infarction or unstable angina in two time periods December 2004–February 2005 (atorvastatin period) and the same months one year later (simvastatin period). Both groups were observed from December to May. Data were then collected in the index ACS event, cardiac readmissions, non-cardiac readmissions and death. The high dose (n = 100) and low dose (121) groups were then compared. The mortality rate post was 5% vs 14%: high dose vs low dose statin (p<0.01). The cardiac readmission rate was 31% vs 53%: high dose vs low dose statin (p = 0.02). The high dose statin therapy had larger infarcts (p = 0.058). There were no statistically significant differences in non-cardiac readmission, age, gender, type of MI.
Conclusions: Such an audit may be of limited utility when compared to the randomised control trials such as Treating to New Targets and PROVE-IT. It undoubtedly will suffer from all the faults of small scale audits when compared to large scale RCTs such as power to detect change, balance of groups, confounding variables, etc. However, this information highlights a more pertinent point; that the wholesale change of an effective therapeutic modality to one less efficacious may adversely affect patient morbidity and mortality, as seen in Stoke. The cost of the additional cardiac readmissions will almost certainly offset the additional cost of the high dose statin therapy. The effect seen locally in Stoke is certainly predictable with the published numbers need to treat for benefit seen in TNT and PROVE IT. Perhaps it is time to reconsider high dose statin therapy in post-MI patients, who do not have time to up-titrate lipid lowering therapy. As a result of this audit along with the large volume of RCT evidence, PCTs with the North Staffordshire area have started to re-review the role of high dose statin therapy post-MI.
myocardial infarction; mortality; statin
166 A ONE YEAR EXPERIENCE OF PRIMARY PERCUTANEOUS CORONARY INTERVENTION IN LEEDS: AN AUDIT OF PATIENTS EXCLUDED FROM INTERVENTIONAL THERAPY
M. Jani1, M. Lister1, C. Priestly1, D. Blackman2, J. Greenwood2, J. McLenchan2, J. Blaxill1. 1St James University Hospital, Leeds, UK; 2The General Infirmary at Leeds, Leeds, UK
Background: A 24/7 PPCI service has been in place in Leeds to treat all patients with acute STEMI/LBBB from 7 March 2005. We have audited the period 7 March 2005–31 March 2006 to understand the reasons why some patients received thrombolysis or no reperfusion treatment at all.
Methods: Prospective data collection of acute STEMI/LBBB cases, corroborated by Myocardial Infarction National Audit Project (MINAP) database were categorised according to method of reperfusion with PPCI the default therapy. Patient records for those not undergoing PPCI were reviewed by two auditors.
Results: 233 patients received PPCI, 42 thrombolysis, and 20 neither. Figure 1 shows the age distribution of lysed patients: mean age 68 years (range 33–93 years, SD 15.2) compared with 63 PPCI and 77 no reperfusion. The reasons for thrombolysis (fig 2) included cath lab non-availability (24%), patients unstable for transfer (10%), not referred for PPCI by A/E (7%), declined by interventional team but no clear documentation (7%) and staff fatigue (7%). Medical reasons included known triple vessel disease not suitable for PCI, poor arterial access, severe pulmonary oedema (26%) and dementia/inability to cooperate (5%). ECG diagnostic difficulty occurred in 12%. The interventional team were non-contactable in 2%. Six lysed patients died within 30 days—4 patients as a consequence of thrombolysis (large intracerebral haemorrhage and retroperitoneal haemorrhage) and 2 patients of cardiogenic shock. Patients were found to be more likely to receive thrombolysis at the beginning of the observed period. Of the non reperfused, the reasons were: 40% late presentation, adverse comorbidities 30%, normal coronaries 15%, no targetable lesion 10%, revised diagnosis 5%. The mortality rates were: 5.9% PPCI, 14.3% thrombolysis, 15% non-reperfused. Mortality for the thrombolysed group rose to 25% in the 70–80 age group and 43% for the over 80s.
Conclusions: There was a trend for lysed patients to be older, reflecting more comorbidities, particularly PVD. More died as a consequence of haemorrhage. Reasons for thrombolysing patients varied considerably. These included non medical reasons such as lack of availability of a cath lab (more common during working hours) or on occasions staff fatigue, particularly nocturnal. Technical reasons included issues of arterial access and florid pulmonary oedema. The high mortality (9.5%) directly attributable to the bleeding complications of thrombolysis only further highlight the advantages of PPCI. The mortality increased sharply in patients over 70 when thrombolysed. The non-perfused were older still but on clinical review all were treated appropriately. The commonest reason was late presentation. The mortality rates, although not directly comparable, do nonetheless favour PPCI. The total mortality rates compare favourably with our institution’s historical records: 9.9% 2003, 9.1% 2005 and 6.4% for this period.
primary PCI; thrombolysis; myocardial infarction
167 DRUG-ELUTING STENTS ARE NOT ASSOCIATED WITH AN INCREASE IN ALL-CAUSE MORTALITY: RESULTS FROM A SINGLE TERTIARY CENTRE FOLLOWING NICE GUIDELINES
K. Balachandran, B. Singh, J. Edmond, D. Finch, A. Baumbach. Bristol Royal Infirmary, Bristol, UK
Background: Recent presentations have raised concerns about the medium- to long-term outcomes following implantation of drug-eluting stents (DES) in various coronary syndromes. The impact of its use within NICE guidelines is uncertain.
Methods: All patients who underwent percutaneous coronary intervention (PCI) at our centre between January 2003 and December 2005 were identified from our dataset. Those patients who died up to a follow-up period extending to October 2006 were detected from the NHS mortality database. Wilcoxon (Gehan) test was used to compare mortality between bare metal stents (BMS) and DES. Appropriate Kaplan–Meier curves were constructed.
Results: We strictly followed NICE guidelines on stent implantation. 2961 PCIs were performed in 2771 patients during the study period. Median follow-up was 28 months (range 10–46 months). The pattern of stent use changed dramatically with 56.4% of patients having a DES implanted in 2005 compared to 6.5% in 2003. There was a trend towards a better all-cause mortality among patients who had DES implanted (DES, 22 deaths in 1186 patients; BMS, 49 in 1417: p = 0.045; fig). There was no difference in mortality when various subgroups were analysed according to presentations (acute (primary or rescue) PCI: DES, 5 deaths in 136 patients vs BMS, 20 in 289, p = 0.24; urgent in-hospital PCI: DES, 12 deaths in 549 vs 26 in 699, p = 0.29 and elective PCI: DES, 5 deaths in 501 vs 3 in 429, p = 0.5).
Conclusion: The use of DES as per NICE guidelines is not associated with an increase in all cause mortality.
all-cause mortality; drug-eluting stents; NICE guidelines
168 SAFETY AND UTILITY OF 0 AND 6-HOUR POINT OF CARE TROPONIN TESTING IN LOW-RISK POSSIBLE ACUTE CORONARY SYNDROMES: A DISTRICT GENERAL HOSPITAL EXPERIENCE
G. Ray1, T. Gaffney2, S. Hood2, P. Macintrye2, M. Morgan2, S. Russell2, I. Findlay2. 1Royal Alexandra Hospital, Paisley, UK; 2
Introduction: Cardiac troponins are an established tool for early triage and management of patients presenting with cardiac sounding chest pain. We assessed the utility of a bedside troponin T measured on admission and at 6 h after admission in patients with possible acute coronary syndrome.
Methods: We studied all patients (1622 in total, 923 males and 699 females) admitted between October 2002 and April 2004 with acute onset chest pain which could not readily be explained by any other non-cardiac cause. They had either normal ECG or unchanged ECG from previous documented ECG. Patients with ST elevation myocardial infarction, fresh ST -T wave abnormalities, new onset arrhythmias and heart failure were excluded from the study. After admission ECG, a 0-h and subsequent 6-h troponin T estimation was done by a trained chest pain nurse using a bedside quantitative point of care (POC) troponin T test (Roche Cardiac Reader). Troponin T was considered negative if the reading was ⩽0.04 ng/ml and positive if ⩾0.05 ng/ml.
Results: The mean time between onset of qualifying chest pain and admission was 5.3 h. Thus most of the patients had at least one troponin T tested within 12 h of onset of chest pain. 144 patients (8.9%) had a positive bedside troponin T at 0 h. Troponin T was positive at 6 h after admission in 246 patients (15.16%). Therefore of all Troponin positive patients 59% (144/246) had positive POC troponin T at 0 h. A total of 910 patients (56.10%) were discharged from hospital within 24 h of whom 761 patients (83.62%) had a pre-discharge exercise tolerance test (ETT). 53 (7%) of the patients who had pre-discharge ETT had a positive result. Adherence to discharge protocol was reduced at weekends when no dedicated chest pain nurse was available. 283 patients (17.44%) were readmitted again within one year with chest pain. Of these 43 (2.65% of total 1622 patients) had a discharge diagnosis of unstable angina, 10 patients (0.62% of total 1622 patients) had non-ST elevation myocardial infarction and none had ST elevation myocardial infarction. Only 6 (0.37% of total) patients died within the next year following discharge and all were troponin T positive on the initial admission.
Conclusion: POC testing is safe and allows rapid decision making for most patients with acute chest pain. Positive zero-hour troponin identified on admission in over half of those patients destined to be troponin positive allowed immediate management decision to be made in A&E reducing waiting time there. In suspected acute coronary syndrome complications are extremely uncommon in this low risk population with a negative 0 and 6 h bedside troponin T test result. When combined with a pre-discharge exercise test, selected patients can be safely discharged within 24 h. In our population of 200 000 we estimate that this early discharge possibly saves around 600–800 bed days per annum.
troponin T; acute coronary syndrome; point of care
169 ASSESSMENT OF STANDARDS OF PERCUTANOUS INTERVENTIONAL PRACTICE: DEVELOPMENT OF A NETWORK-WIDE PEER REVIEW AUDIT PROCESS
L. Blows, G. Dixon, A. de Belder. Sussex Cardiac Centre, Brighton, UK
Background: Audit for PCI procedures identifies operator and institutional volumes with a focus on in-hospital MACE. This is a relatively crude tool for defining a successful PCI procedure. A successful percutaneous intervention requires appropriate clinical judgement about whether the patient should be having the procedure, an appropriate strategy and the technical skills to achieve an optimal result. These are complex matters as decisions are based on numerous factors. We report a mechanism to evaluate PCI performance on a network-wide basis.
Abstract 169
Methods and Results: The network consists of a tertiary centre and three district general hospitals performing PCI with 10 interventionalists. A total of 1750 cases are performed annually. On a monthly basis a review meeting is held whereby, 10% of cases, randomly selected by an audit manager (at least 1 case per operator), are examined by 3 reviewers (1 tertiary and 1 DGH interventionalist and 1 cardiac surgeon) on a rotational basis. Appropriateness of intervention, strategy and outcome are recorded with confidential feedback to the primary operator. Additional procedural details such as lesion assessment with IVUS or pressure wire, use of drug-eluting stents and glycoprotein IIbIIIa inhibitors are collected (measuring concordance with NICE guidelines). To date 182 cases have been evaluated (table). Individual operator performance is presented in the figure.
Conclusion and Discussion: This model identifies patterns of interventional practice, which will become more robust as the database is expanded. For example operator 1 (fig) was more likely to receive comments regarding strategy which appeared to lead to less satisfactory outcomes. Unsurprisingly it was the surgeon on the committee who has been most likely to report “inappropriate for PCI”. However, overall this tool has demonstrated that appropriate standards of care are maintained. The particular value of involving a surgeon in a PCI audit is an improved understanding of what can be done percutaneously with an objective view of outcomes. Moreover, it consolidates relationships with surgical colleagues, which is central to a cohesive revascularisation service. In this model feedback to individual operators, allows debate and provokes thought about PCI decisions. There are no penalties in this model, but trends can be identified which might help improve practice. This audit tool allows development of practice across the network, protecting patients and operators alike.
percutaneous intervention; audit; performance
170 INDISCRIMINATE USE OF TROPONIN I IN UNSELECTED MEDICAL EMERGENCIES
A. Nisbet1, F. Dunn2. 1BHF Glasgow Cardiovascular Research Centre, Glasgow, UK; 2Stobhill Hospital, Glasgow, UK
Introduction: Following introduction of troponin I (TnI) measurements strict criteria for its use were adopted. However with its increasing availability, there has been an exponential rise in requests from acute medical receiving units. This raises issues in regard to interpretation of elevated TnI in view of its limited specificity. Positive results must be interpreted with caution in the absence of additional criteria suggestive of myocardial infarction. This audit aimed to survey the number of TnI requests from the acute medical receiving ward of Stobhill Hospital, Glasgow and identify those considered to be inappropriate in the context of the patient’s presenting complaint.
Methods: Over a 6-week period from June to July 2004 data were collected, by either medical or nursing staff, on all admissions to the acute medical receiving unit in whom a TnI was requested. Completed forms were collected and analysed with the assistance of the local Clinical Audit team.
Results: There were 141 TnI requests during the 6-week period. The mean age of the patients was 65 (range 26–92) years. 74 (54%) were male. The mean TIMI risk score was 1.88 (range 0–5). 56 (39.7%) had TnI requested for symptoms consistent with myocardial ischaemia (7 (12.5%) of these had a positive TnI). In the remainder (10 (58.8%) of whom had a positive TnI) the most common indications were atypical chest pain (18 (21%)), dyspnoea (15 (17.6%)) and collapse (15 (17.6%)). Of the patients with a positive TnI in the absence of ischaemic sounding chest pain, the majority presented with dyspnoea (30%), followed by collapse (20%), followed by pleuritic (10%) or “atypical” (10%) chest pain. In 13 (15.2%) no specific reason for checking TnI was given. In 76 of 124 (60%) patients with a negative TnI, there was no suggestion of myocardial ischaemia from the patient’s presenting complaint or ECG. Renal impairment (defined as a creatinine of greater than 120) was present in 32 (22%) of cases. Of this group, 6 (18.75%) had a positive TnI, and 1 case had a positive TnI in the context of a normal ECG. Linear regression analysis revealed a positive correlation between creatinine and TnI in those with an elevated TnI (p = 0.036).
Conclusions: This audit suggests that there are a significant number of inappropriate requests for TnI in the setting of an acute medical ward, with the majority of negative results having no ischaemic indication in the first instance. Renal impairment did not account for a significant number of positive results in the absence of symptoms or signs of myocardial ischaemia. This study emphasises the need for ongoing education of nursing and medical staff in the acute medical receiving ward setting to ensure that requests for TnI are appropriate. Guidelines for measurement of TnI should not be relaxed because of its increased availability. Otherwise additional unnecessary investigations and erroneous diagnoses result with additional costs to the health service and concern for the patients and their families.
troponin I; myocardial ischaemia; audit
171 NEED FOR CORONARY ARTERY BYPASS GRAFTING FOLLOWING PERCUTANEOUS CORONARY INTERVENTION: A SINGLE CENTRE UK AUDIT OF 2395 REVASCULARISATION PROCEDURES
G. Milborrow, N. Child, I. Purcell. Freeman Hospital, Newcastle upon Tyne, UK
Introduction: Advances in percutaneous coronary intervention (PCI) have permitted percutaneous revascularisation in patients historically referred for coronary artery bypass grafting (CABG). Recently surgeons have expressed concern regarding an apparent high incidence of CABG following PCI. We audited the relationship between PCI and CABG as performed in the Freeman Hospital, Newcastle, UK.
Method: An audit of the hospital’s electronic records for patients treated in 2004. Cohort 1: Retrospective audit of CABG procedures, recording incidence of patients with previous PCI and time interval between PCI and CABG. Cohort 2: Prospective audit of PCI procedures with minimum 1 year follow-up. Incidence, indication and waiting time for CABG following PCI was investigated.
Results: Cohort 1 (CABG): 731 patients received first time CABG only in 2004. 65 (8.9%) had previous PCI. 92% of CABGs were performed within 1 year of PCI. Cohort 2 (PCI): 1664 PCIs were performed in 2004. 52 cases (3.1%) underwent subsequent CABG. 4 referral groups were identified: (1) surgical bail out: 4 patients (0.24%); (2) failed chronic total occlusion (CTO): PCI was performed in 210 subjects with CTO consisting of 45 failures with 15 patients (7.14% of CTO/0.9% of total) receiving CABG; (3) failed PCI: 19 patients (1.14%); (4) successful PCI: 18 patients (1.08%) consisting of 9 patients (0.53%) planned for subsequent CABG and 9 patients (0.53%) who received subsequent unplanned CABG. Surgical classification (Cohort 2): (1) emergency: 10 patients (19.2%); (2) urgent: 11 patients (21.2%); (3) elective: 31 patients (59.6%). Time to CABG (Cohort 2): 50% within 4 months; 75% within 6 months.
Conclusion: Bail out following PCI was an infrequent complication and within national expectations. Failed PCIs to both complex lesions and CTOs constituted the majority of cases referred for CABG and can be expected. Only 0.5% of all PCI patients required unplanned bypass following successful PCI. Our data suggest that surgical concern regarding possible high rates of unplanned CABG procedures following PCI are unfounded.
percutaneous coronary intervention; coronary artery bypass grafting; audit
172 INTRODUCTION OF INTEGRATED NURSE SPECIALIST LED MANAGEMENT OF ACUTE CORONARY SYNDROME PATIENTS: AN AUDIT
K. Alfakih, M. Melville, J. Nainby, J. Waterall, J. Walsh, A. Harcombe. Queen’s Medical Centre, Nottingham, UK
Introduction: The management of acute coronary syndromes (ACS) has changed greatly over recent years. Trials evidence encouraged clinicians to consider early invasive management in high-risk patients and this has created a large clinical burden. We instituted a comprehensive system of nurse specialist led diagnosis and management of ACS. In-patients are seen by a Cardiac Outreach nursing team who coordinate a management plan according to the patient’s risk profile. This may include admission to a designated “Acute Cardiac Unit”. Following in-patient management we have set up a pilot “ACS clinic” where patients at high or moderate risk by TIMI score are seen only two weeks after discharge. All patients are discussed with a consultant cardiologist. As a result of restructuring our services we have carried out audits to measure the impact on appropriate use of invasive strategy, revascularisation rates, 6-month re-admission rates and uptake of cardiac rehabilitation.
Methods and Results: We identified 158 patients in the ACU admissions book as having had unstable angina or NSTEMI in the first 6 months of 2005. This followed the introduction of the outreach team but pre-dated the introduction of the ACS clinic. Mean age was 64 (13) years, 37% were 70 years old and 72% male. ST segment depression was present in 23% and T wave inversion in 42%. Troponin I was raised in 59%. The in-patient coronary angiography rate was 48%, PCI rate 15% and CABG rate 4%. At 6 months total PCI rate was 27% and total CABG was 14% giving a total revascularisation rate of 41%. The total mortality rate was 5.1%, with 7.6% non-fatal re-infarctions, giving a composite endpoint of death and MI of 12.7%. The 6-month readmission rate with further anginal symptoms was 28.5% with 44.4% of these patients readmitted within a month of discharge. In-patient coronary angiography halved the rate of readmission 20.0% vs 38.5%. The ACS clinic opened in November 2005 and in the first 6 months 143 patients were seen. Of these 26 were readmitted within 6 months (18.2%). If patients were both nursed on ACU and followed up in the ACS clinic the rate of readmission was only 11.2%, comparing very favourably with the previous audit figure of 28.5% and with the GRACE registry figure of 31 and 32% for low- and high-risk patients respectively. By the end of 12 months 309 patients had been seen, 166 had ongoing symptoms and medications were titrated. 258 patients were suitable for rehabilitation and 92% accepted. As a result of ACS clinic review a further 25 were referred for angiography, 9 for PCI and 2 for CABG, with 4 direct admissions being made.
Conclusions: A nurse-led programme of identification of ACS patients, management in a designated area, invasive investigations and follow-up in a nurse-led specialist clinic all promote effective use of resources, increase uptake of cardiac rehabilitation and reduce 6-month re-admission rates.
audit; acute coronary syndromes; nurse
173 CLINICAL PRE-TEST PROBABILITY IS SUPERIOR TO EXERCISE-TESTING AS A TOOL FOR IDENTIFYING THE HIGHEST RISK PATIENTS: DATA FROM A RAPID ACCESS CHEST PAIN CLINIC
G. Thakaran, J. Deane, J. Tenkorang, R. Rakhit. Royal Free Hospital, London, UK
Introduction: The aim of rapid access chest pain clinics (RACPCs) is to identify and promptly and effectively manage patients at high risk of coronary artery disease. Predicting significant coronary artery disease is achieved with both clinical and non-invasive data. The higher the sensitivity and positive predictive value (PPV) of the risk stratification method used, the higher the likelihood of the patient undergoing coronary angiography as the gold standard for diagnosis of coronary disease. There are different methods of each risk stratification be it based on clinical information or non-invasive tests. Here we compare the effectiveness of two of the commonest used methods of risk assessment.
Abstract 173
Methods: 155 patients (62% male) seen between September 2002 and April 2004 at the Royal Free Hospital RACPC were risk-stratified according to the Diamond–Forrester criteria (based on age, sex and chest pain characteristics) as well as exercise testing (ETT) using the Full Bruce Protocol into high, intermediate or low risk respectively. 119 of them underwent coronary angiography to determine the sensitivity and positive predictive value of each risk stratification method used.
Results: Sensitivity and PPV of the highest risk group using the Diamond–Forrester criteria were 81% and 82% respectively compared to that of ETT of 32% and 95% respectively. Combining both risk stratification tools increased the sensitivity and PPV of the highest risk group to 80% and 76% respectively.
Conclusions: The use of clinical risk stratification is not to be underestimated. A high pre-test probability based on clinical information in isolation is more effective than non-invasive risk assessment also used in isolation. Combining the two achieves a predictability of a positive coronary angiogram similar to that achieved by clinical information alone. In addition, non-invasive tests other than exercise testing should be considered to facilitate the clinical risk stratification of patients presenting to RACPCs.
Diamond–Forrester pre-test probability; rapid access chest pain clinic; exercise testing
174 OUTCOME OF PRIMARY PERCUTANEOUS CORONARY INTERVENTION IN THE VERY ELDERLY
A. Crean, M. Dorsch, K. Somers, C. Hague, J. McLenachan, J. Blaxill, S. Wheatcroft, A. Mackintosh, J. Greenwood, D. Blackman. Leeds General Infirmary, Leeds, UK
Introduction: Primary percutaneous coronary intervention (PPCI) is superior to thrombolysis for the treatment of acute ST-elevation myocardial infarction (STEMI). However, it is unclear whether this advantage extends to the very elderly. Subgroup analysis of octogenarians in the only randomised controlled trial data available indicated equally poor outcomes with primary PCI (mortality 19%) and thrombolysis (mortality 16%). The aim of this study was to determine the outcome of PPCI in the over 80s in a real-world UK setting.
Methods: Retrospective review of case records of all patients age ⩾80 undergoing PPCI within a 24/7 service at the Yorkshire Heart Centre (YHC) from April 2005 to October 2006. Comparison with outcome of PPCI in the under 80s, and with a historical cohort of 55 patients age >80 years receiving thrombolysis.
Results: Forty five patients aged ⩾80 years (mean 85, range 80–96) were treated with PPCI, 11% of the total population of 399. Very elderly patients presented late (median pain to balloon time 338 min), but door to balloon times were short (median 73 min). Patients were high risk: 73% (33/45) had renal impairment (Cr >100 μmol/l) and 62% (28/45) had multivessel disease. All patients were treated with aspirin and clopidogrel (300–600 mg) pre-procedure. 91% (41/45) received abciximab. PCI was successful in 100% (45/45) with final TIMI 3 flow in 82% (37/45) and TIMI 2 flow in the remaining 18%. In-hospital and 30-day mortality was 13% (6/45). Death/re-infarction/stroke occurred in 16% (7/45). Major bleeding was common, occurring in 11% (5/45) with 2 fatal bleeds (intracranial haemorrhage, massive haematoma). In-hospital mortality was much higher than for PPCI in the under 80s over the same period (13% vs 5.4%) but considerably lower than with thrombolysis in the historical control group of over 80s (13% vs 33%).
Conclusions: Primary PCI in the over 80s is high risk. Mortality is much higher than in younger patients. Nevertheless it is lower than that seen with thrombolysis in age-matched historical controls suggesting that the benefits of primary PCI extend at least in part to the very elderly.
primary percutaneous coronary intervention; elderly; outcomes
175 SHOULD PATIENTS IN CARDIOGENIC SHOCK UNDERGO RESCUE ANGIOPLASTY AFTER FAILED FIBRINOLYSIS? COMPARISON OF PRIMARY VS RESCUE ANGIOPLASTY IN CARDIOGENIC SHOCK PATIENTS
B. Kunadian, A. Thornley, K. Vijayalakshmi, A. Sutton, D. Muir, R. Wright, J. Hall, M. de Belder. The James Cook University Hospital, Middlesbrough, UK
Background: Trials of rescue angioplasty (rPCI) following failed fibrinolysis have excluded patients with cardiogenic shock and the benefit of rPCI in this setting is unknown. We compared the clinical, angiographic characteristics, 30 day and one year outcomes of cardiogenic shock patients undergoing rPCI with those undergoing primary percutaneous coronary intervention (PPCI).
Methods: Of the 171 patients undergoing PCI for cardiogenic shock between 1994 and 2005 in our institution, the indication was for PPCI in 65 and rPCI in 59 patients. Clinical, procedural, 30-day and 1-year mortality data were compared.
Results: There were no differences between the cohorts with regards to clinical and pre-PCI angiographic variables except patients who underwent rPCI were more likely to be interhospital transfers (64% vs 43%, p = 0.02) and had a longer chest pain onset to PCI time (median 411 (IQR 567–310) min in the rPCI group vs 275 (IQR 450–189) min in the PPCI group, p<0.01). Glycoprotein IIb/IIIa inhibitors were used less often (20% vs 42%, p = 0.01) but use of stents was similar in both groups. Patients undergoing rPCI had a lower rate of final TIMI 3 flow grade (56% vs 74%, p = 0.04) and a higher 1-year mortality (71% vs 49% p = 0.01). In the patients with final TIMI flow 3, 1-year mortality was higher in the rPCI group (61% vs 37% p = 0.04). In patients with successful procedures (survived procedure, no emergency CABG, TIMI 3 flow), 1-year mortality was higher in the rPCI group (59% vs 33%, p = 0.02). One-year mortality was 85% in both groups if the procedure was unsuccessful. One-year mortality in patients >70 years old with cardiogenic shock undergoing rPCI was 100% (n = 15) and with PPCI was 70% (n = 14). Rescue angioplasty, anterior myocardial infarction, multivessel disease, and post-procedure TIMI flow grade <3 were found to be independent predictors of mortality at 30 days.
Conclusions: In the setting of cardiogenic shock, rPCI patients were treated later than those undergoing PPCI. They had a lower final TIMI 3 flow and higher 1-year mortality. Even patients with a successful rPCI procedure had a higher 1-year mortality than those with a successful PPCI. Rescue angioplasty in the setting of cardiogenic shock was found be an independent predictor of mortality. Rescue angioplasty in elderly patients (>75 years) in cardiogenic shock may be a futile treatment. Efforts should be made to improve reperfusion and survival in these patients, possibly by either adopting PPCI for all patients presenting with ST elevation AMI or, if this is not logistically possible, adopting PPCI for selected high-risk patients or early referral for rPCI in high-risk groups receiving fibrinolysis.
cardiogenic shock; rescue angioplasty; failed fibrinolysis
176 RESCUE ANGIOPLASTY AFTER FAILED FIBRINOLYSIS FOR ACUTE MYOCARDIAL INFARCTION: PREDICTORS OF A FAILED PROCEDURE AND 1-YEAR MORTALITY
B. Kunadian, R. Thornley, K. Vijayalakshmi, J. Dunning, A. Sutton, D. Muir, R. Wright, J. Hall, M. de Belder. The James Cook University Hospital, Middlesbrough, UK
Background: Rescue angioplasty for failed fibrinolysis is associated with a low mortality if successful, but a high mortality with a failed procedure. Whether the latter reflects identification of a high-risk group or harm in some patients is unclear. Predictors of likely success or failure of a rescue procedure may enhance the selection of patients to be treated.
Methods: Unselected patients referred for rescue angioplasty after failed fibrinolysis from March 1994 to March 2005 were studied to determine the characteristics, predictors and one year mortality of patients with a failed rescue procedure. We also determined independent predictors of 1-year mortality.
Results: 440 patients underwent emergency coronary angiography for failed fibrinolysis. One-year mortality was 18%. 101 patients had TIMI 3 flow in the infarct related vessel (IRV) on initial angiography. Rescue angioplasty was attempted in 318 of the 339 patients with <TIMI 3 flow but not in 21 patients (angiography produced TIMI 3 flow (n = 7) or unsuitable anatomy (n = 14)). Of the rescue angioplasty cohort, 77% had a successful procedure (no in-lab death or emergency CABG and TIMI 3 flow in the IRV) and 23% had a failed procedure. One-year mortality rates for successful and failed rescue angioplasty were 14% and 43% respectively. Patients who had failed rescue angioplasty were older and more likely to be diabetic, have anterior myocardial infarction, be interhospital transfers, be in cardiogenic shock and less likely to be a current smoker. Cardiogenic shock was the only independent predictor of failed rescue angioplasty. In multivariate analysis, age group >75 years, cardiogenic shock and final post-procedure TIMI flow grade less than 3 were independent predictors of 1-year mortality.
Conclusions: Cardiogenic shock in patients referred for rescue angioplasty is an independent predictor of failed rescue angioplasty. Age group >75 years and cardiogenic shock were the only independent clinical predictors of mortality at 1 year. These clinical variables may help in selecting patients for a strategy of rescue angioplasty after failed fibrinolysis.
rescue PTCA; angioplasty; thrombolysis
177 REDUCED VASCULAR COMPLICATIONS AND LENGTH OF STAY WITH TRANSRADIAL RESCUE ANGIOPLASTY FOR ACUTE MYOCARDIAL INFARCTION
N. Cruden1, C. Huat2, I. Starkey1, D. Newby2. 1Western General Hospital, Edinburgh, UK; 2University of Edinburgh, Edinburgh, UK
Introduction: Patients with acute ST elevation myocardial infarction (STEMI) undergoing rescue percutaneous coronary intervention (PCI) following failed thrombolysis are at significant risk of vascular complications. The transradial approach may reduce vascular complications, improve mobilisation and facilitate earlier discharge. We examined outcomes for the transradial and transfemoral approaches in patients with STEMI undergoing rescue PCI.
Abstract 177
Methods: Clinical outcomes from 287 consecutive patients undergoing rescue PCI for STEMI over a 3-year period were determined retrospectively. Data were collected via a standardised proforma and analysed using SPSS. Data are presented as n (%) or mean (SD).
Results: Procedural success was similar for the transradial and transfemoral routes (43 (98%) vs 225 (93%); p = 0.3). There were reductions in vascular complications (0 (0%) vs 32 (13%); p<0.01) and post-procedural stay (7.0 (7.9) vs 7.9 (5.6) days; p<0.005) in the radial group compared with the femoral group respectively. There were no differences in procedural or in-hospital mortality, study duration or radiation dose between the two groups.
Conclusions: Rescue PCI performed via the radial artery is safe, effective and associated with a reduction in vascular complications and length of hospital stay compared to the femoral approach. Our findings suggest that where facilities and experience allow, rescue PCI in patients with STEMI should be performed via the radial artery.
myocardial infarction; angioplasty; thrombolysis
178 EVALUATION OF SAFETY AND EFFICACY OF ANGIOJET USAGE IN A UK HEART ATTACK CENTRE
J. Strange, Z. Cheng, C. Critoph, S. Archbold, M. Rothman. The London Chest Hospital, London, UK
Introduction: Rheolytic thrombectomy device such as AngioJet (Possis Medical) facilitates the removal of thrombus and has been used in conjunction with stenting in the treatment of acute myocardial infarction (AMI). It aims to improve myocardial reperfusion. This study evaluates the effects of such device on the final angiographic results and its safety profile.
Methods: Retrospective cohort study over a period of 12 months identified 33 patients presenting with AMI and receiving thrombectomy with AngioJet prior to stent deployment. Age- and sex-matched control group who received primary angioplasty without thrombectomy were also identified. Clinical and angiographic outcomes were compared between the two groups.
Results: The mean age of all patients was 59 (7) years, 67% were male. All patients were given upfront glycoprotein (GP) IIb/IIIa receptor inhibitor. The AngioJet group had significant greater angiographic evidence of thrombus compared with control group, (thrombus score of 3.7 (0.1) vs 2.54 (0.2), p<0.001, thrombus length of 23 (3) mm vs 12.5 (1.5) mm, p<0.001). 26/33 patients were noted to have an improvement in TIMI flow (+1.7, p<0.01) and thrombus score (−1.8, p<0.01) after AngioJet. There was a trend towards improvement of TIMI flow and cTIMI frame count comparing angiographic films after AngioJet and after subsequent stenting. The difference was not statistically siginificant. The final angiographic results, assessed by TIMI flow and cTIMI frame count, were not significantly different between the AngioJet group and the control group (TIMI flow 2.81 (0.5) vs 2.96 (0.5), p = 0.13, cTIMI frame count 11.7 (2.1) vs 9.5 (1.7), p = 0.51). There were 3 cases of cardiac tamponade and 3 deaths in the AngioJet group. No deaths were seen in the control group at time of hospital discharge. Two of the deaths were in patients with right coronary artery occlusion and subsequent cardiac tamponade.
Conclusion: Despite AngioJet’s apparent efficacy at removing thrombus, it does not appear to improve final angiographic results in patients presenting with AMI associated with high thrombus burden. There is a concern regarding the potential complication of cardiac tamponade, likely to be associated with temporary wire insertion, especially in the setting of acute right ventricular infarct. Local practice has changed and now when AngioJet thrombectomy is attempted a temporary pacing wire is not inserted into the right ventricle, but left in the right atrium ready if so required.
179 EFFECT OF DISTAL EMBOLISATION ON MYOCARDIAL PERFUSION RESERVE FOLLOWING PERCUTANEOUS CORONARY INTERVENTION: AN QUANTITATIVE MR PERFUSION STUDY
J. Selvanayagam1, A. Cheng1, K. Rahimi1, I. Porto2, W. Van Gaal2, K. Channon1, S. Neubauer1, A. Banning2. 1University of Oxford, Oxford, UK; 2John Radcliffe Hospital, Oxford, UK
Introduction: Studies have shown that a subset of patients demonstrate persistent impairment in microcirculatory function after percutaneous coronary intervention (PCI). Distal embolisation of plaque contents has been postulated as the main mechanism for this. We sought to investigate this further by evaluating PCI induced changes in myocardial perfusion reserve index (MPRI) over time in segments with “distal type” procedure related myonecrosis using high resolution quantitative CMR.
Methods and Results: Forty patients undergoing PCI were studied with pre-PCI and 24-h post PCI DE-MRI and first pass perfusion MR imaging at rest and stress. 20 patients underwent a third MRI scan at 6 months. For perfusion imaging, 3 short axis images were acquired during every heartbeat using a T1-weighted turboFLASH sequence. MPRI was calculated as the ratio of hyperaemic to resting myocardial blood flow and subdivided according to presence and location of new delayed hyperenhancement (HE). 21 patients demonstrated new distal HE post PCI. Mean MPRI in revascularised myocardial segments not demonstrating new HE was significantly increased post-procedure (2.06 (0.65) pre-PCI and 2.50 (0.90) post-PCI; p<0.001, fig 1). In contrast, MPRI in segments with distal HE did not improve post PCI (2.16 (0.95) pre-PCI; 2.00 (0.85) post-PCI; mixed model z = −1.88, p>0.05, fig 1). Changes in mean MPRI 24-h post-PCI in segments upstream to new injury was not significantly different when compared with perfusion changes in remote myocardium (z = −1.14; p = 0.25, fig 2). At 6 months following the procedure, mean MPRI in segments with new injury improved significantly compared with MPRI measured in these segments at 24 h post-PCI.
Conclusion: MPRI is reduced in myocardial segments demonstrating new “distal” irreversible injury at 24 h post-PCI. These reductions are transitory and seem to be confined to the segments with injury. They do not affect the entire supply territory of the culprit vessel.
percutaneous coronary intervention; myocardial perfusion; magnetic resonance imaging
180 IMPACT OF PERIPROCEDURAL CREATINE KINASE-MB ISOENZYME ELEVATION ON LONG-TERM MORTALITY AFTER PERCUTANEOUS CORONARY INTERVENTION
M. Andron, M. Egred, A. Alahmar, M. Shaw, T. Grayson, E. Roberts, R. Perry, N. Palmer. Cardiothoracic Centre, Liverpool, UK
Background: Creatine kinase MB elevation following percutaneous coronary intervention (PCI) is common and it has been suggested that large elevations in periprocedural CKMB is independent predictor of long-term mortality. Aim, to study the impact of CKMB isoenzyme elevation on long-term mortality in the contemporary era of PCI.
Abstract 180
Methods: We carried out retrospective analysis of prospectively collected data on 4341 consecutive patients who underwent PCI with stent deployment between January 2003 and December 2005. Patients with ST segment elevation myocardial infarction and patients with cardiogenic shock were excluded. Post-procedure CKMB enzyme levels were available in 3864 patients. Patients were followed up to 30 June 2006, all-cause mortality was taken from a national death registry. The association between creatine kinase MB (CKMB) enzyme levels and follow-up mortality were examined using Cox proportional hazard analyses. We performed repeated dichotomous analyses entering CKMB >2, >3, >4, >5, >6, >7, >8, >9, >10 times the upper limit of normal (× ULN), to the Cox proportional hazard model. Stratums of CKMB (1–3 ×, 3–5 × and >5 ×) were also offered to the model.
Results: The univariate analysis for follow-up mortality showed 127 deaths and a mean follow up duration of 22.1 months. Five hundreds and fifty patients (14.2%) had CKMB enzyme release >2 × ULN, 365 (9.5%) >3 × ULN, 270 (7.0%) >4 × ULN, 198 (5.1%) >5 × ULN, 158 (4.1%) >6 × ULN, 127 (3.3%) >7 × ULN, 106 (2.7%) >8 × ULN, 96 (2.5%) >9 × ULN, 90 (2.3%) >10 × ULN. Logistic regression analysis revealed that post-procedure CKMB enzyme level of >4 × ULN was associated with a significant increase in follow-up mortality (HR: 2.10, 95% CI 1.31 to 3.38, p = 0.002; table). The figure illustrates the adjusted hazard ratio for mortality for each stratum of CKMB. Other independent risk factors for follow-up mortality are shown in the table.
Conclusion: : In our series, CKMB elevation greater than four times ULN was found to be an independent predictor of long-term mortality following PCI.
creatine kinase; PCI; mortality
181 DO PATIENTS UNDERGOING PERCUTANEOUS CORONARY INTERVENTION STILL REQUIRE CONSENTING FOR EMERGENCY CORONARY BYPASS SURGERY?
J. Arnold, C. Shirodaria, T. Karamitsos, W. van Gaal, J. Forfar, O. Ormerod, K. Channon, S. Westaby, A. Banning. John Radcliffe Hospital, Oxford, UK
Background: Patients undergoing percutaneous coronary intervention (PCI) are routinely consented for emergency coronary artery bypass grafting (CABG), with a quoted incidence of 0.5–1%. In the era of contemporary PCI, with advances in stent technology and pharmacotherapy, and changing patient demographics, we sought to re-evaluate this risk.
Methods: We examined our local cardiac database to determine the rates of emergency CABG following PCI, and emergency PCI following CABG, between January 2001 and March 2006. Emergency CABG was defined as occurring within 6 h of PCI, and emergency PCI within 24 h of CABG. All CABG patients undergoing simultaneous valve surgery were excluded from the analysis.
Results: In our institution, a total of 7855 PCIs were performed during this period (55% elective, 37% urgent, 8% emergency). The inpatient mortality rate was 0.6% (0.2% elective PCI, 0.5% urgent PCI, 5.2% emergency PCI). Nine patients (0.11%; 7 males, 2 females, mean age 65.3 (10.5) years, 1 emergency and 8 elective procedures) required emergency CABG for procedural complications (5 perforations, 3 dissections, 1 guidewire fracture). There were two deaths, both occurring within 48 h of emergency CABG (one after emergency PCI and one following elective PCI). Of a total of 3216 CABGs carried out during the same period, 3 patients (0.09%; 2 males, 1 female, mean age 67.7 (8.1) years) required emergency cardiac catheterisation. There was no significant difference between the crossover rates in the two groups (0.11% for the PCI group vs 0.09% for the CABG group, p = 0.9).
Conclusions: In a surgical centre undertaking unselected PCI in a high-risk population, the risk of emergency CABG is lower than previously reported in the literature, suggesting that routine consent for emergency CABG is no longer appropriate. Indeed, we observed similar rates of emergency CABG following PCI and emergency PCI following CABG. Patients undergoing PCI continue to be routinely consented for emergency CABG, whereas the converse does not occur in patients undergoing CABG. We conclude that the same standard should apply to both procedures.
percutaneous coronary intervention; coronary artery bypass grafting; emergency
182 THE EFFECT OF REGIONAL WALL MOTION ABNORMALITIES ON CORONARY HAEMODYNAMICS
N. Hadjiloizou, J. Davies, D. Francis, I. Malik, C. Manisty, R. Foale, K. Parker, A. Hughes, J. Mayet. International Centre for Circulatory Health, St Mary’s Hospital, London, UK
Background: In normal coronary arteries, the large increase in flow velocity in diastole has been attributed to a distally-originating “suction” wave. If this is true, and if this wave arises from relief of the systolic myocardial compression of the microcirculation, then this “suction” wave should be smaller when myocardium is akinetic. We tested this hypothesis in patients undergoing coronary stenting, some of whom had akinetic walls. Using wave intensity analysis, we identified and separated the proximal (aortic) and distal (microcirculatory) contribution to flow distal to a stenosis and hypothesised that, following stenting, the distal contribution would be less in nonviable, infarcted myocardium than in viable, normally contracting myocardium.
Methods: In 11 subjects sensor-tipped intra-arterial wires were used to measure simultaneous pressure and Doppler velocity before and after percutaneous coronary revascularisation. The subjects were grouped into those with no previous history of myocardial infarction and no regional wall motion abnormalities on tissue Doppler echocardiography and those with previous acute myocardial infarction and had regional wall motion abnormalities on tissue Doppler. Wave intensity analysis was applied to derive the proximal- and distal-originating waves that are responsible for augmenting flow velocity.
Results: Distal to the stenosis, the distal-originating waves contributed more than four times as much for the increase in flow velocity than the proximal-originating waves (0.36 (0.17) m/s vs 0.08 (0.04) m/s, p<0.001). These distal-originating waves were greater than the proximal-originating waves (19.9 (12.5)×105 Wm−2s−1 vs 7.5 (4.5)×105 Wm−2s−1, p<0.02). In infarcted, non-viable myocardium the distal-originating waves were much smaller than in viable, non-infarcted myocardium (6.1 (2.6)×105 vs 21.0 (7.3)×105, p<0.03).
Conclusion: Distal to a stenosis, flow is augmented by a distal-originating suction wave that contributes more than four times as much to flow velocity as does the proximal-originating wave. The distal “suction” depends critically on the integrity of the microcirculatory bed.
ventricular dysfunction; coronary haemodynamics; coronary artery disease
183 IMPAIRED LEFT VENTRICULAR LONG AXIS FUNCTION IN MARFAN SYNDROME DEMONSTRATED BY ABNORMAL MITRAL ANNULAR DISPLACEMENT
A. Kiotsekoglou1, A. Bajpai1, K. Karastergiou1, G. Athanasopoulos2, J. Moggridge1, B. Bijnens1, D. Nassiri1, A. Camm1, G. Sutherland1, A. Child1. 1St George’s University of London, London, UK; 2Onassis Cardiac Surgery Centre, Athens, Greece
Background: While cardiac function is considered to be preserved in Marfan syndrome (MFS), in a recent report the sensitive techniques of MRI and pulsed wave Tissue Doppler Imaging (TDI) demonstrated a primary impairment of left ventricular (LV) function. Fibrillin-1 deficiency resulting from fibrillin-1 mutation in MFS may lead to impaired myocardial contractility. We aim to study LV long axis function using M-mode imaging, which is widely available in all echocardiographic units and systolic annular velocities from colour Doppler tissue images.
Abstract 183 Table 1
Abstract 183 Table 2
Methods: We assessed the LV long axis function in 63 un-operated patients—34 men and 29 women (mean age 31.4 (12.6) years) with established diagnosis of MFS. All fulfilled Gent criteria and 24 (38%) had causative fibrillin-1 mutations. We also examined 55 sex-, age- and body surface area-matched normal controls. All subjects underwent echocardiographic examination at rest, using a VIVID 7 Vingmed-General Electric ultrasound scanner equipped with a 4S-MHz probe. Atrioventricular plane displacement (AVPD) measurements were obtained from the lateral, septal, inferior and anterior mitral annular borders. Systolic mitral annular velocities were calculated by tracking colour tissue Doppler images. Digital images were analysed offline using the Echopac (version 6.0.0) software.
Results: LV internal dimensions and wall thicknesses did not differ between MFS patients and controls. Aortic root (AR) diameter was significantly higher in MFS (3.98 (0.56) vs 3.07 (0.33) cm, p<0.001). Ejection fraction evaluated by modified Simpson’s rule was significantly lower in MFS patients (66.6 (6.2)%) in comparison to normal volunteers (71.75 (4.4)%, p<0.001) although still within normal limits. Dilated AR (>3.9 cm) was present in 39 (61.9%) of MFS patients. This subgroup also showed increased interventricular septum (IVS) thickness (1.075 (0.18) vs 0.925 (0.09) cm in MFS patients with normal AR, p<0.001). Normalised (mitral annular displacement/longitudinal LV inner distance) AVPD was globally reduced in MFS (table 1). Patients with dilated AR showed further decrease in septal long axis function (0.14 (0.03) vs 0.17 (0.03), p<0.001) compared with patients with normal AR size. Normalised septal AVPD inversely correlated with AR diameter (r = −0.508, p<0.001). There was also significant inverse correlation between systolic blood pressure (BP) and normalised lateral AVPD (r = −0.353, p<0.01). Mitral annular (MA) velocities obtained from the septal and lateral portions were reduced in MFS (table 2). Those from lateral and anterior portions inversely correlated with age, systolic and diastolic BP (p<0.001).
Conclusions: Conventional LV ejection fraction and long axis function indices are reduced in MFS. This may be due to fibrillin-1 deficiency in LV myocardium. Our data suggest that AVPD assessment by 2D-targeted M-mode imaging alone may be useful in monitoring MFS patients.
Marfan syndrome; systolic function; atrioventricular plane displacement
184 DIFFERENTIATION BETWEEN HYPERTROPHIC CARDIOMYOPATHY AND HYPERTENSIVE LEFT VENTRICULAR HYPERTROPHY: THE ROLE OF STRAIN RATE IMAGING STUDY AND INTEGRATED BACKSCATTER ANALYSIS
S. Orlando, V. Puntmann, A. Baltabaeva, M. Marciniak, A. Marciniak, T. Karu, B. Bijnens, G. Sutherland. St George’s Hospital, London, UK
Background: Differentiation of hypertrophic cardiomyopathy (HCM) from hypertensive left ventricular hypertrophy (H-LVH) is prognostically important and may be difficult in the absence of family history and histological confirmation, due to the widespread muscle fibre disarray in the former and to the often intense septal involvement in the latter condition.
Abstract 184 Table 1
Abstract 184 Table 2
Methods and Results: We investigated the role of strain rate myocardial imaging (SRI) and integrated backscatter (IB) tissue characterisation in 45 age- and gender-matched subjects, in 16 LV segments from parasternal long-axis and three apical views (table 1). In comparison to hypertensive and normal subjects, global peak systolic strain rate (SR sys), early diastolic strain rate (SR E dia), peak systolic strain (S sys) and cyclic variation of IB (CVIB), were significantly reduced in HCM (p<0.01) (table 2). Multivariate analysis revealed that combination of the four above indices enables to differentiate between the two hypertrophic conditions (p<0.0001). Longitudinal systolic strain was found to be the most sensitive index of differentiation with a cut-off value of 14.5% (sensitivity 89%, specificity 94%, likelihood ratio 16, AUC of 0.97, p<0.001). Regional examination revealed that in HCM, SR and CVIB indices were the most reduced in basal and mid septal segments, affecting both radial and longitudinal function. On the contrary, in H-LVH deformation and reflectivity indices did not significantly differ from normal subjects.
Conclusions: Using SRI and IB analysis greatly improves the power of differentiation between the two hypertrophic conditions, with S and SR reflecting reduced global and regional deformation, and CVIB reduced contractility.
hypertrophic cardiomyopathy; strain rate imaging; integrated backscatter
185 MYOCARDIAL DEFORMATION IMAGING FOR THE PREDICTION OF SUBCLINICAL LEFT VENTRICULAR DYSFUNCTION AND MORTALITY IN ASYMPTOMATIC PATIENTS WITH END STAGE RENAL DISEASE AND NORMAL LEFT VENTRICULAR EJECTION FRACTION
R. Sharma1, D. Pellerin2, H. Gregson3, C. Streather3, D. Gaze3, P. Collinson3, S. Brecker3. 1Ealing Hospital, London, UK; 2The Heart Hospital, London, UK; 3St George’s Hospital, London, UK
Background: Cardiac failure is a major cause of morbidity and mortality in patients on dialysis. However, left ventricular (LV) ejection fraction (LVEF) is often preserved in patients with end stage renal disease (ESRD) at the onset of renal replacement therapy. The aim of this study was to determine whether tissue Doppler velocities and strain/strain rate imaging detect LV dysfunction and predict mortality in asymptomatic patients with ESRD and normal LVEF.
Methods: 86 patients with ESRD (mean age 57 (16) years, 55 male, mean creatinine 689±208 μmol/l) were enrolled immediately prior to the initiation of dialysis therapy. All had LVEF >50% with no prior history of cardiac disease. 65 age- and sex-matched controls were also studied. All underwent a standard cross sectional transthoracic echocardiogram with tissue Doppler imaging (TDI). Peak long axis velocity (Sm) was determined by averaging the values from the septal and lateral sites of the mitral annulus. Peak systolic Strain and strain rate (SR) data were collected from the basal, mid and apical segments of the anterior and inferior walls and an averaged value calculated for each patient.
Results: Mean LVEF and LV end systolic diameter (LVESD) were similar in the 2 groups. Mean Sm was significantly lower in patients with ESRD compared to controls (7.4 (1.8) cm/sec vs 9.8 (1.4) cm/sec, p = 0.02). Peak systolic strain (−13.9 (5.1)% vs – 18.9 (4.6)%, p = 0.004) and peak systolic SR (−0.72 (0.18)/sec vs −1.16 (0.21)/sec, p = 0.001) were significantly lower in patients with ESRD compared to controls. Peak systolic strain and SR were significantly lower in all LV segments of the inferior and anterior walls for patients with ESRD compared to controls. Systolic SR correlated with LV mass (r = 0.49, p = 0.03) but not LVESD in patients with ESRD. Over a mean follow-up time of 2.24 (0.64) years, there were 2 deaths in the control group and 14 in the ESRD group. From ROC analysis, a peak systolic SR ⩽ - 0.65/sec, found in 31% ESRD patients, predicted mortality in the ESRD group with a sensitivity of 83% and a specificity of 88% (AUC = 0.81, 95% CI 0.75 to 0.91, p = 0.002).
Conclusions: Subclinical changes in LV function can be detected in ESRD patients with normal LVEF at the onset of dialysis. Reduced myocardial peak systolic SR at the onset of dialysis was a marker of increased mortality in these patients. TDI may be useful in the future for predicting LV dysfunction in this patient group before the ventricle starts to fail irreversibly.
end stage renal disease; subclinical cardiomyopathy; strain rate imaging
186 THE EXTENT OF RESIDUAL CONTRAST PERFUSION AND NOT LEFT VENTRICULAR FUNCTION PREDICTS LATE RECOVERY OF GLOBAL CONTRACTILE FUNCTION AFTER ACUTE MYOCARDIAL INFARCTION AND REPERFUSION THERAPY
G. Dwivedi, R. Janardhanan, J. Swinburn, K. Greaves, R. Senior. Northwick Park Hospital, Harrow, UK
Background: Following acute myocardial infarction (AMI) and reperfusion therapy, there are often persistent wall thickening (WT) abnormalities and perfusion defects due to variable degrees of myocardial stunning and necrosis. We hypothesised that the extent of residual perfusion assessed by myocardial contrast echocardiography (MCE) and not the extent of WT predicts subsequent global recovery of left ventricular (LV) function, an important marker of prognosis.
Methods: Accordingly, 112 patients underwent simultaneous assessment of WT and perfusion using MCE 7 (2) days after AMI and reperfusion therapy. Both WT (1 = normal; 2 = reduced; 3 = absent; 4 = dyskinetic) and perfusion (2 = normal; 1 = reduced; 0 = absent) were scored on a 16 segment LV model. Contrast perfusion index (CPI), a measure of extent of myocardial perfusion and global LV function was calculated by adding the respective scores in the 16 LV segments divided by 16. Echocardiography was repeated 12 weeks after the reperfusion therapy to assess recovery of LV function.
Results: Follow-up echocardiography was available in 98 patients. Of these 66 (69%) demonstrated improvement in LV function. The area under the receiver operator characteristic curve for predicting recovery of LV function by MCE and by LV function at baseline were 0.79 and 0.59 respectively. Furthermore, CPI was significantly higher (p<0.0001) in the 66 patients, which showed late recovery of LV function (1.67 (0.27)) compared to those who did not (1.27 (0.04)). No significant difference was noted in the indices of baseline LV function in patients with (1.67 (0.32)) and without (1.80 (0.36)) recovery of LV function. The multivariable predictors of recovery of function were MCE (p = 0.02), diabetes (p = 0.02) and peak creatine kinase (p = 0.01). Of the 62 patients with minimal perfusion defect (CPI>1.5), 54 (87%) showed recovery of LV function, conversely, 22 (64%) of 32 patients with significant perfusion defect failed to recover function. Recovery of function was markedly reduced if the percentage of perfused myocardium (scores 1 and 2) was below 40%.
Conclusions: The extent of residual contrast perfusion and not LV function predicts late recovery of global LV function after AMI and reperfusion therapy.
myocardial infarction; contrast echocardiography; ventricular function
187 ABNORMAL LEFT VENTRICULAR TORSION IN CHRONIC MITRAL REGURGITATION: A SPECKLE TRACKING ECHOCARDIOGRAPHY STUDY
A. Borg, J. Harrison, C. Laws, D. Fox, W. Khan, S. Ray. Department of Cardiology, Wythenshawe Hospital, Manchester, UK
Introduction: Counter-rotation of the base and apex results in systolic torsion of the left ventricle (LV), followed by rapid untwisting in early diastole. Abnormal torsion is related to progressive LV dysfunction in models of mitral regurgitation (MR). We used speckle tracking echocardiography to measure LV torsion and untwist in patients with chronic organic MR.
Methods: We measured rotation and rotation rate from 2D greyscale LV base and apex short axis images by speckle tracking software (2D Strain, GE Vingmed). Using a custom written MATLAB 7 (MathWorks) algorithm, plots of torsion/torsional velocity against time were constructed by deducting base rotation/rotation rate from apex rotation/rotation rate at isophasic time points. Graphs of torsion against time-varying LV volume (derived from radial displacement at the mid-LV short axis, and longitudinal displacement of the mitral valve annulus from the apical 4-chamber view) were plotted automatically. From the plots, we measured peak systolic torsion (PST), peak systolic torsional velocity (PSTV) and peak untwisting velocity (PUV). Time to PST, PSTV, and PUV were also measured. To account for different cycle lengths, all time intervals were normalised to systolic duration. Aortic valve closure (AVC) defined end systole. Mitral valve opening (MVO) was also recorded.
Results: We recruited 36 patients with moderate-severe MR (age 65 (13) years) and 30 controls (C) (age 60 (12) years). PST, PSTV and PUV were similar in MR (11.8 (6.5)°, 69.0 (31.8)°/s, 86.1 (51.9)°/s) and C (11.5 (6.1)°, 65.7 (32.8)°/s, 82.3 (36.9)°/s), p>0.6. All time intervals were increased in MR compared to C: Time to PST, (105 (14) vs 93 (8)%, p<0.001), time to PSTV (62 (14) vs 54 (13)%, p = 0.03), and time to PUV (131 (15) vs 116 (9)%, p<0.001). Untwisting started, on average, 18 ms before AVC in C but, in MR, was delayed to 16 ms after AVC, p<0.001. In C, PUV occurred 9 ms before MVO, but was delayed to 38 ms after MVO in MR, p<0.001 (fig 1). Isovolumic untwist ratio (untwist during isovolumic relaxation period/twist at end-systole) was less in MR: 5.7 (30.7) vs 38.1 (25.8)%, p<0.001. During the isovolumic relaxation period, all C exhibited untwisting, while 16 MR subjects (44.4%) sustained continued twisting. Correlations between torsion parameters and LV properties showed the magnitude of PST and PUV decreases significantly with worsening LV remodelling and MR severity, while untwisting is progressively delayed. Averaged torsion-volume loops (fig 2) demonstrate less systolic torsion at a given volume, early peaking of torsion before AVC in C with later peaking in MR, and less untwisting between AVC and MVO in MR compared to C.
Conclusion: LV torsional dynamics are altered in patients with chronic MR in relation to the severity of regurgitation and the extent of ventricular remodelling. Analysis of torsion may provide insight into the mechanism of early ventricular dysfunction in this population.
torsion; mitral regurgitation; speckle tracking
188 INDEPENDENT VALUE OF LEFT ATRIAL VOLUME INDEX FOR THE PREDICTION OF ALL CAUSE MORTALITY IN PATIENTS WITH SUSPECTED HEART FAILURE REFERRED FROM THE COMMUNITY
T. Lim, G. Dwivedi, S. Hayat, R. Senior. Northwick Park Hospital, Cardiovascular Medicine, Harrow, UK
Background: Left ventricular (LV) ejection fraction (LVEF) and LV end systolic size are recognised markers of mortality but it is now increasingly apparent that a significant proportion of patients with heart failure (HF) have normal LVEF. Left atrial volume index (LAVI) reflects LV filling pressure and has been shown to predict outcome independent of Doppler parameters. However, the ability of LAVI to predict mortality independently of LV systolic function in patients with suspected HF referred from the community is unknown.
Methods: Accordingly, 356 suspected HF patients referred from the community were followed up for mortality after undergoing clinical assessment, electrocardiography (ECG) and echocardiography including Doppler to assess LV filling. Cox regression analysis was used for the evaluation of the independent predictors of mortality.
Results: Data were obtained in 335 (mean age 72 (13) years, 162 male and 173 female) (94%) patients over a mean follow-up period of 30 (10) months during which 38 (11.3%) died. The univariate predictors for all cause mortality were age (p<0.001), symptom of leg swelling (p = 0.001), clinical sign of HF (p = 0.01), abnormal ECG (p = 0.008), LVEF (p = 0.001), LAVI (p<0.001), septal wall thickness (p = 0.007), LV end systolic and diastolic dimension (p<0.01). However, the only independent predictors of mortality were age (hazard ratio (HR) = 2.12, 95% CI 1.42 to 3.25, p<0.001), symptom of leg swelling (HR = 2.83, 95% CI 1.43 to 5.59, p = 0.005), LAVI (HR = 1.25, 95% CI 1.01 to 1.54, p = 0.04) and LV end systolic size (HR = 1.32, 95% CI 1.02 to 1.70, p = 0.04).
Conclusion: LAVI was superior to LVEF for the prediction of mortality and provided independent information over clinical variables for predicting mortality in patients with suspected HF referred from the community. Hence LAVI should be routinely assessed for evaluating such patients.
heart failure; mortality; left atrial volume index
189 TRANSTHORACIC ECHOCARDIOGRAPHY PRACTICE IN THE UK
M. MacDonald1, N. Hawkins1, S. Balmain2, J. McMurray3, M. Petrie1. 1Glasgow Royal Infirmary, Glasgow, UK; 2Western Infirmary of Edinburgh, Edinburgh, UK; 3Western Infirmary, Glasgow, UK
Introduction: High quality echocardiography is essential in the diagnosis and management of cardiovascular conditions. We aimed to assess the quality of echocardiographic services provided in the UK in 2005.
Methods: A questionnaire was sent to the chief cardiac physiologist in every hospital in the UK.
Results: 125 hospitals responded. The median number of echocardiograms (echos) performed per year was 3500. The mean age of the primary echo machine was 3.3 years.
Staff and Accreditation: Cardiac physiologists perform echocardiograms in 98% of hospitals, and report in 88%. In terms of workload, cardiac physiologists perform and report over 80% of all echocardiograms in most hospitals (87%). In one quarter of hospitals (26%) all echocardiograms are performed and reported by cardiac physiologists. Only 57% of cardiac physiologists have a formal echocardiographic accreditation. Of those doctors reporting echos, only 22% are accredited.
Waiting Lists: The median in-patient and outpatient waiting times were 2 (range 1–20) days and 8 (range 0–40) weeks, respectively. Over 20% of hospitals have an in-patient waiting list of greater than 5 days and an outpatient waiting time of greater than 4 months.
Quality Control: Only 60% of hospitals had criteria that had to be met prior to an operator being allowed to report echos unsupervised. Only 48% of the hospitals perform regular audit of echocardiography scans and reports.
Diastolic Function: 92% of hospitals included assessment of diastolic function in routine examinations. 22% of these hospitals used E:A ratio alone.
Dysynchrony: Cardiac dysynchrony was assessed in 71% of hospitals. Of these, 29% performed “eye-ball” dyssynchrony assessment alone. Tissue Doppler techniques were employed in 39% of centres.
Mitral Regurgitation: Only 39% and 6% of hospitals calculated proximal isovelocity surface area and regurgitant volume, respectively.
Conclusion: The UK has an echo service lead by cardiac physiologists, half of whom do not hold an echocardiographic accreditation. Over half of hospitals do not have quality control systems. Approximately one third use modern echocardiographic techniques.
echocardiography; survey; practice
190 PATENT FORAMEN OVALE: AN EVALUATION OF DIFFERENT DIAGNOSTIC TECHNIQUES AND ROUTES OF CONTRAST ADMINISTRATION
U. Velupandian1, R. Khiani1, S. Ray2, R. Calderwood1, E. Herring1, Z. Bonner1, A. Heagerty1, J. Morris2, C. McCollum1. 1University of Manchester, Manchester, UK; 2South Manchester University Hospital, Manchester, UK
Introduction: Paradoxical embolism usually through a patent foramen ovale (PFO) may cause ischaemic stroke in young adults and decompression sickness. Detection and quantification of a shunt through a PFO, is therefore important. Transoesophageal echocardiogram (TOE) was compared with transthoracic echocardiogram (TTE) and transcranial Doppler (TCD) using an arm vein (AV) and femoral vein (FV) for contrast administration.
Methods: Fifty five young adults with possible paradoxical embolism referred for diagnosis of PFO, underwent TCD insonation of the middle cerebral artery, TTE with second harmonic imaging and TOE with contrast (agitated saline-air-blood) administered via AV and FV using a standardised protocol (1) at rest (2) with coughing and (3) a Valsalva manoeuvre (VM) or modified VM on TOE.
Results: When compared with TOE with FV as the gold standard, the sensitivity and specificity for TCD was 100% and 91.2% with AV and 100% and 94.4% with FV injection. The sensitivity and specificity for TTE was 84.2% and 75% with AV and 100% and 75% with FV injection. The sensitivity and specificity of conventional TOE with arm vein injection was 89.5% and 97.2% (figs 1 and 2). One of the three studies positive on TCD with arm vein injection but negative on TOE, was a significant shunt only with VM and also confirmed on TTE with VM and must have been a false negative on TOE. The sensitivity of TTE with arm vein injection was mainly limited by image quality and the three patients who missed detection had poor image quality. Image quality did not limit detection by TTE when FV was used.
Conclusion: TCD with AV contrast administration is a reliable alternative to TOE for detection of PFO. TTE would be equally effective only with FV contrast administration. Conventional TOE with AV injections may not be the “gold standard” for PFO detection. Sensitivity of TOE, TCD and TTE with arm vein and femoral vein contrast injections when compared with TOE with femoral vein injection as the gold standard. Specificity of TOE, TCD and TTE with arm vein and femoral vein contrast injections when compared with TOE with femoral vein injection as the gold standard.
patent foramen ovale; transcranial Doppler; echocardiogram (transoesophageal, transthoracic)
191 ASSESSMENT OF MYOCARDIAL PERFUSION: CAN IT BE DONE USING REAL-TIME 3D ECHO?
A. Bhan, S. Kapetanakis, B. Rana, E. Ho, K. Wilson, M. Monaghan. King’s College Hospital, London, UK
Background: 2D low mechanical index (LMI), contrast specific myocardial perfusion imaging is now an accepted and widespread technique. We evaluated the first implementation of LMI imaging with real time 3D echo (RT3DE), to establish its feasibility in unselected patients.
Methods: Twenty two consecutive patients (10 male) referred for contrast enhanced echo were imaged using a Philips IE33 3D scanner, with novel 3D LMI power modulation software. All patients underwent 2D contrast echo and RT3DE apical full volume acquisition, during contrast infusion (Sonovue 0.7 ml/min). Datasets were taken in left ventricular opacification (LVO), and LMI perfusion modes. The datasets were then evaluated segmentally for wall motion and myocardial contrast enhancement, relative to the LVO mode.
Results: A total of 352 left ventricular segments were evaluated. Wall motion and perfusion could be assessed in 98.8% and 98% respectively of the 2D segments, and in 97.4% and 96% of the 3D segments. 318 segments had normal wall motion and thickening. In these, normal 3D myocardial opacification was seen in 97.5% of apical, 96.5% of mid and 94.3% of basal segments (p = NS for all comparisons). Twenty one segments were akinetic with no 2D evidence of perfusion and of these, RT3DE successfully demonstrated a perfusion defect in 19 (90.5%) (p = NS).
Conclusion: Evaluation of myocardial perfusion using LMI RT3DE appears to be feasible in most left ventricular segments. In the future it should be useful, not only for specifying accurate location, but also quantifying volume of perfusion defects.
real-time 3D echo; contrast echo; myocardial perfusion
192 HERITABILITY OF THE QTC INTERVAL: ANALYSIS IN A POPULATION-BASED FAMILY STUDY
C. Hajat1, J. Gracey2, T. Smith2, P. MacFarlane3, A. Ng2, P. Burton1, M. Tobin1, N. Samani2. 1Department of Health Sciences and Department of Genetics, University of Leicester, Leicester, UK; 2Department of Cardiovascular Sciences, University of Leicester, Leicester, UK; 3Medical Sciences, University of Glasgow, Glasgow, UK
Introduction: Inherited long (and short) QT syndromes are associated with a significant risk of malignant arrhythmias and sudden cardiac death. They are caused by mutations in genes for cardiac ion channels. Within the general population, the heart-rate corrected QT interval (QTc), also shows considerable variation. The extent to which this variation within the putative normal range is also genetically determined remains to be fully clarified. Our aim was to investigate the relative influence of genetic and environmental determinants on QTc interval in a UK population based-sample of 1491 subjects from 386 representative white European families.
Methods: The mean QTc interval was determined from a resting 12-lead electrocardiogram using an automated technique. Gibbs sampling-based variance component modelling was implemented in WinBUGS 1.4 to estimate the proportion of the variance in the QTc interval attributable to additive polygenic effects (narrow sense heritability or h2N), shared family environment and shared sibling environment. Age and sex were included as covariates. As the slope of relationship between age and QTc interval differed between males and females, a sensitivity analysis was undertaken with their ages modelled separately and to allow for non-linear correlation of QTc with age.
Results: The age range of subjects was 18–60 years. Mean ages were for parents 52.7 (SD 4.4) and for offspring 25.4 (SD 5.2). Of 1491 subjects, 745 (50.0%) were female and 746 (50.0%) were male. The mean QTc interval was 404.7 ms (95% CI 402.8–406.7 ms) and was higher in females (410.1 ms) compared with males (399.3 ms) and in parents (409.7 ms) compared with their offspring (399.6 ms) (p<0.001). Shared family and sibling environment were much less important than genetic influence on QTc variance. The proportion of the variance in the QTc interval attributable to additive polygenic effects (h2N) was 42.5% (95% CI 24.4%–61.2%) and did not differ significantly with the sensitivity analyses.
Conclusions: Our findings suggest that a significant proportion of the inter-individual variability in QTc interval is due to additive polygenic effects. Identifying the genetic variants that affect QTc could have important clinical utility, for example in identifying otherwise healthy subjects who may be more prone to iatrogenic prolongation of their QTc interval and the associated risk of severe arrhythmias with various therapeutic agents.
QTc interval; genetics; sudden cardiac death
193 ASSOCIATION BETWEEN POLYMORPHIC VARIATION IN THE ENDOTHELIN-1 TYPE A RECEPTOR GENE AND AMBULATORY BLOOD PRESSURE
T. Rahman, D. Hall, P. Avery, B. Keavney. Newcastle University, Newcastle upon Tyne, UK
Aims: The endothelins are among the most potent vasoconstrictors known. Pharmacological blockade of endothelin receptors lowers blood pressure. It is unknown whether naturally occurring genetic variation in the endothelin receptors influences blood pressure. We have evaluated the type A endothelin receptor (EDNRA) as a candidate gene for hypertension in a large family study.
Methods and Results: 1428 members of 248 families selected via a proband with hypertension were studied. Ambulatory blood pressure monitoring was conducted using the A&D TM2421 device. Four single nucleotide polymorphisms (SNPs) spanning the EDNRA gene were typed. There was strong evidence of association between genotype at the C+70G (rs5335) SNP and daytime systolic blood pressure (+2.26 (SE 0.87) mmHg per G allele; p = 0.009); daytime diastolic blood pressure (+1.49 (0.56) mmHg per G allele; p = 0.007); and daytime mean blood pressure (+1.74 (0.62) mmHg per G allele; p = 0.006). There was also strong evidence of association between rs5335 genotype and night systolic blood pressure (+2.74 (0.89) mmHg per G allele; p = 0.002); night diastolic blood pressure (+1.82 (0.56) mmHg per G allele; p = 0.001); and night mean blood pressure (+1.48 (0.63) mmHg per G allele; p = 0.001).
Interpretation: The C+70G polymorphism of the EDNRA gene has small but consistent effects on the variability of blood pressure within the “normal range” both by day and by night. Natural variation in other genes in the endothelin signalling pathway should be explored to identify additional influences on blood pressure regulation.
hypertension; genetics; endothelin
194 LEUKOTRIENE B4 PRODUCTION IN SUBJECTS WITH VARIANTS OF THE 5-LIPOXYGENASE ACTIVATING PROTEIN GENE ASSOCIATED WITH RISK OF MYOCARDIAL INFARCTION
A. Maznyczka1, M. Mangino1, A. Whittaker1, P. Braund1, T. Palmer2, M. Tobin2, A. Goodall1, P. Bradding3, N. Samani1. 1Department of Cardiovascular Sciences, University of Leicester, Leicester, UK; 2Department of Health Sciences, University of Leicester, Leicester, UK; 3Department of Infection, Inflammation & Immunity, University of Leicester, Leicester, UK
Introduction: Leukotrienes are implicated in the pathogenesis of coronary artery disease. Recently two haplotypes (Hap A and Hap B) in the gene encoding arachidonate 5-lipoxygenase activating protein (ALOX5AP), the main regulator of 5-lipoxygenase, have been associated with a doubling of the risk of myocardial infarction. Studies have also shown that treatment with a leukotriene inhibitor reduces biomarkers for coronary risk in patients carrying HapA, raising the possibility of developing genotype-specific therapy.
Methods: In this study, we examined whether carriage of HapA or HapB is associated with increased leukotriene B4 (LTB4) production in healthy subjects. We screened DNA from 1268 subjects from a population based study to identify subjects carrying different haplotypes of ALOX5AP. Age and gender-matched healthy HapA carriers (n = 21), HapB carriers (n = 20) and non-A/non-B carriers (n = 18), with no reported history of cardiovascular disease, were recruited. Blood neutrophils were isolated and LTB4 production measured in response to stimulation with 1 µM of the calcium ionophore A23187.
Results: There was no difference in the mean level for LTB4 production in the three groups (non-A/non-B: 24.9 (8.3) ng/106 cells; HapA: 22.2 (11.9) ng/106 cells; HapB: 19.8 (4.8) ng/106, p = 0.14). The study had 90% power for an alpha of 0.05, to detect a 32% difference in LTB4 production between haplotype groups. The findings indicate that if either the HapA or the HapB haplotype of ALOX5AP indeed increases cardiovascular risk, then the mechanism is not simply due to a systematically observable effect of the haplotype on LTB4 production in response to stimulation. The results suggest that knowledge of a patient’s haplotype may not provide useful information on the likely clinical response to ALOX5AP inhibitors.
leukotrienes; genetics; myocardial infarction
195 CHARACTERISATION OF MICRORNAS IN THE HUMAN HEART
H. Lu1, P. Punjabi2, F. Rahman1, P. Camici1, T. Aitman1, S. Cook1. 1Clinical Sciences Centre, MRC, London, UK; 2Hammersmith Hospital, London, UK
Introduction: MicroRNAs are small, non-coding RNA species encoded within the human genome that regulate gene expression by inhibiting mRNA translation. Some microRNAs are important in developmental biology but the role(s) of microRNAs in the postnatal heart remain unclear.
Methods: To begin to investigate the role(s) of microRNAs in the postnatal human heart, we collected cardiac MRI and positron emission tomography guided left ventricular biopsies from three groups: patients with normal ventricular function with or without diabetes (n = 6 and n = 7 respectively) and from patients with heart failure (n = 6). Small RNA species were extracted from the biopsies and we determined the expression of 155 mature miRNAs using a TaqMan based real-time PCR method.
Results: The relative amounts of mature microRNA species ranged widely with the expression of most highly expressed microRNA being ∼15 000 times higher than that of the lowest detectable microRNA. We observed that some microRNAs that were previously un-described in the heart (eg, microRNA-30b) are expressed at levels comparable with that of microRNA-133, which has an important role in cardiac development. We compared relative microRNA expression levels between patient groups and identified differentially regulated species (fold change ⩾± twofold, nominal p value <0.05) in patients with diabetes (14 species) or heart failure (44 species) as compared to the group with normal ventricular function in the absence of diabetes. The majority of differentially regulated microRNA species were downregulated in heart failure whereas they were evenly distributed in the diabetic heart biopsies (9 upregulated, 5 downregulated). Some microRNA species were specifically upregulated (eg, microRNA-367, p<0.001, 4.4-fold and microRNA-342, p<0.001, 2.8-fold) in the diabetic heart as compared to the other two patient groups.
Conclusions: We observed a single microRNA, microRNA-223, that was upregulated in both diabetes and heart failure, which are diseases of interrelated pathophysiology. The strongest and most consistent predicted target for microRNA-223 is myocyte enhancer factor 2C that is know to be deleteriously downregulated in both the failing and the diabetic heart. Functional and coding mRNA microarray studies have been used to further investigate the role of microRNA-223 in the heart. These data describe the expression of microRNAs in the human heart in health and disease and indicate that microRNA-223 may have an important pathophysiological role in the development of heart failure. As microRNA function can be inhibited by systemically delivered microRNA inhibitors this may have therapeutic implications for the treatment of heart disease.
microRNA; heart failure; diabetes
196 PLASMA BRAIN NATRIURETIC PEPTIDE PREDICTS OUTCOME IN PATIENTS WITH FRACTURED NECK OF FEMUR
M. Descamps1, A. Ryding1, M. Jeilan1, J. Bankart2, E. Crawfurd1, D. Gidden1, D. Sprigings1. 1Northampton General Hospital, Northampton, UK; 2Department of Health Sciences, University of Leicester, Leicester, UK
Introduction: Patients with fractured neck of femur have a high risk of perioperative death due to cardiovascular complications. Current methods of preoperative assessment appear to be inadequate in this patient group.
Methods: We assessed the predictive value of preoperative bedside echocardiography, the Revised Cardiac Risk Index and plasma Brain Natriuretic Peptide (BNP, Bayer Centaur assay) in a prospective observational study of 101 patients with a fractured neck of femur under going emergency surgery. The primary outcome measure was postoperative all cause mortality at 30 days. The secondary outcome was a composite of 30 day mortality or perioperative troponin I elevation.
Results: The primary outcome occurred in 5 patients, and the secondary in 13 patients. Multivariable logistic regression demonstrated that BNP was the only significant predictor of both the primary (p = 0.0211, sensitivity of 1.00, specificity 0.736) and secondary outcomes (p = 0.0025, sensitivity 1.00, specificity 0.79). Using ROC analysis the area under the curve for BNP was 0.880 and 0.906 for the primary and secondary outcomes, with optimal cut points of 255 pg/ml and 210 pg/ml respectively.
Conclusion: Preoperative measurement of BNP is a practical and powerful predictor of outcome in patients presenting with fractured neck of femur. Our data suggest that it performs best as a negative predictor of adverse cardiac events in this setting.
brain natriuretic peptide; risk assessment; echocardiography
197 HEART-TYPE FATTY ACID BINDING PROTEIN PREDICTS MORTALITY IN PATIENTS WITH SINUS RHYTHM AND LEFT VENTRICULAR SYSTOLIC DYSFUNCTION
P. Loh1, L. Tin1, J. Windram1, P. Reddy1, O. Khaleva1, G. Mathur1, R. Nicholls1, K. Goode1, N. Nikitin1, E. Stanton2, A. Clark1, J. Cleland1. 1Academic Cardiology Department, University of Hull, Hull, UK; 2McMaster University, Ontario, Canada
Background: Patients with left ventricular systolic dysfunction may suffer from continuing myocardial damage without any obvious episode of myocardial ischaemia. Heart-type fatty acid binding protein (H-FABP) is a sensitive maker of myocardial injury. In patients who are hospitalised for worsening heart failure (HF) due to LVSD, elevated H-FABP predicts future cardiovascular events. We investigated the prognostic role of H-FABP in stable LVSD patients.
Methods: H-FABP (median (inter-quartile range)) was measured in 345 consecutive patients attending a local hospital HF service with at least mild-to-moderate LVSD, in sinus rhythm and on optimal HF treatment. The median follow-up was 31 (range 19–42) months. The primary outcome was all-cause mortality.
Results: The mean age was 69 (10) years and 79% were men. 83% had ischaemic heart disease (IHD) and 33% had severe LVSD. The NYHA breathlessness classes were I (15%), II (63%) and III/IV (22%). 26% reported at least an episode of angina/week. 91% were taking an angiotensin converting enzyme inhibitor or angiotensin receptor blocker (ACEI/ARB) and 86% were taking a beta-blocker (BB). Compared to 88 age- and sex-matched non-LVSD patients who had established or were at risk of developing cardiovascular disease, LVSD patients had higher H-FABP (2.3 (1.7–3.5) vs 1.6 (1.3–2.0) ng/ml, p<0.001). H-FABP correlated with age (r = 0.459, p<0.001) and calculated glomerular filtration rate (GFR) (r = −0.667, p<0.001) but not frequency of angina. It was higher in patients with NYHA III/IV compared to NYHA I/II (3.2 (2.0–4.9) vs 2.2 (1.7–3.6) ng/ml, p<0.001). Patients with more severe LVSD had higher H-FABP (2.5 (1.8–3.6) vs 2.1 (1.6–3.3) ng/ml, p = 0.039). Anaemic and diabetic patients had higher H-FABP (2.9 (2.1–4.3) vs 2.0 (1.6–2.8) ng/ml and 2.7 (2.0–4.4) vs 2.2 (1.7–3.3) ng/ml respectively, all p<0.001). The 18-month mortality was 13.3%. H-FABP was higher in those who died (3.3 (2.4–4.3) vs 2.2 (1.7–3.4) ng/ml, p<0.001). Using Cox regression analysis, H-FABP above median was associated with an increase in mortality (HR 2.06; 95% CI 1.02–4.17, p = 0.045) after adjustment for age, sex, severity of LVSD, NYHA, IHD, diabetes, GFR, albumin and medications (ACEI/ARB, BB, loop diuretic, statin and anti-thrombotic). Independent predictors for H-FABP level above median were age (OR 1.06; 95% CI 1.03–1.09, p<0.001), renal dysfunction (OR 4.81; 95% CI 2.68–8.63, p<0.001) and anaemia (OR 2.28; 95% CI 1.31–3.96, p = 0.004). Severity and aetiology of LVSD were not independent predictors.
Conclusion: Patients with sinus rhythm and LVSD on stable treatment have higher H-FABP. This is associated with age and the presence of renal dysfunction and anaemia. A higher H-FABP level in these patients is associated with a greater mortality.
heart-type fatty acid binding protein; heart failure; left ventricular systolic impairment
198 NT-PROBNP AS A BIOMARKER FOR THE DEVELOPMENT OF CARCINOID HEART DISEASE
S. Bhattacharyya1, C. Toumpanakis2, M. Caplin2, J. Davar1. 1Department of Cardiology, Royal Free Hospital, London, UK; 2Neuroendocrine Tumour Unit, Royal Free Hospital, London, UK
Introduction: Carcinoid heart disease (CHD) develops in a substantial proportion of patients with carcinoid tumours. The current gold standard for diagnosis of CHD is by echocardiography. Regular echocardiography is time consuming, expensive and in some areas local capacity limits availability. A biomarker which provides an sensitive, quick and easily reproducible method of screening for CHD is needed. N terminal fragment brain natiuretic peptide (NT-proBNP) is secreted by myocytes in response to increases in wall stress. NT-proBNP is elevated in patients with severe CHD. We aimed to assess whether NT-proBNP can be used as screening test for CHD.
Methods: Seventy patients with mid-gut carcinoid tumours were screened for CHD using two dimensional transthoracic echocardiography. CHD was defined as was defined as thickened valve leaflets coupled with reduced excursion/fixation and retraction or non-coaptation of valve leaflets associated with valvular regurgitation or stenosis. NT-proBNP was measured in all patients prior to echocardiography using an electrochemiluminescence immunoassay.
Results: CHD was present in 15 out of 70 patients (21%). NT-proBNP was significantly higher in those with CHD (median 1347 pg/ml (interquartile range 406–3389)) than in those without CHD (median 135 pg/ml (interquartile range 59–288)), p<0.0001. The sensitivity and specificity of BNP in this patient group for detection of CHD were 0.93 and 0.87 respectively. The area under reciever operator curve, for a cut-off value of 259 pg/ml, was 0.96 (fig).
Conclusion: NT-proBNP is a excellent marker of the development of CHD. At a cut-off level of 259 pg/ml, NT-proBNP virtually excludes a diagnosis of CHD. We propose the use of NT-proBNP as a screening investigation to exclude CHD.
carcinoid; valvular; brain natiuretic peptide
199 SERUM METABOLOMIC ANALYSIS SUCCESSFULLY DISCRIMINATES HEART FAILURE PATIENTS FROM CONTROLS
S. Deepak1, W. Dunn2, D. Broadhurst2, M. Buch3, G. McDowell4, D. Ellis2, N. Brooks1, D. Kell2, L. Neyses3. 1South Manchester University Hospitals NHS Foundation Trust, Wythenshawe Hospital, Manchester, UK; 2School of Chemistry and The Manchester Centre for Integrative Systems Biology, The University of Manchester, Manchester, UK; 3Division of Cardiovascular and Endocrine Sciences, The University of Manchester, Manchester, UK; 4Department of Clinical Biochemistry, Manchester Royal Infirmary, Manchester, UK
Introduction: Brain natriuretic peptide (BNP) and N-terminal - pro BNP (N-BNP) are the best currently available biomarkers for heart failure (HF) but limitations exist. The novel post genomic science of metabolomics is the study of the metabolic profile of a given cell, tissue, fluid, organ or organism at a given point in time. The metabolome represents the end products of gene expression. Metabolomic analysis reflects the functional activities of the cell. In contrast to malignancy, where tissue is available for transcriptomic and proteomic analysis, laboratory tests for heart failure are limited to serum samples. Furthermore, cardiac and systemic metabolic alterations have been well documented in heart failure. Thus serum metabolomic analysis may offer a new approach in identifying more accurate biomarkers for the diagnosis and risk stratification of patients with heart failure.
Methods: Peripheral venous blood samples from 52 patients with significant left ventricular dysfunction (ejection fraction ⩽35%) and symptomatic chronic heart failure (NYHA class II-IV) were collected. They were compared with 57 age-matched normal controls. Serum samples were simultaneously analysed by gas chromatography time-of-flight mass spectrometry (GC-TOF-MS). N-BNP was measured on the Roche E170 immunoassay analyser. Statistical analyses were performed using the Matlab scripting language.
Results: From the processed serum fingerprints (276 characteristic peaks) across 109 patients, two highly significant metabolite biomarkers for heart failure were evident (peak 495 and 816; p<10–12 for Mann–Whitney test). Their concentrations (GC-MS relative peak areas) were compared with N-BNP using receiver operating characteristic (ROC) curves (Image 1). Image 2: Comparison of Mass spectra of a peak identified as 816 obtained from clinical serum sample (top) and (bottom) an authentic standard. (Identified metabolites have not been named due to intellectual property issues and will be revealed at the time of presentation if successful).
Conclusion: Two serum metabolites (816 and 495) that characterise heart failure have been detected. In this initial study their sensitivity and specificity in the diagnosis of heart failure is at least equal to N-BNP; larger studies may go on to demonstrate their superiority.
metabolomics; heart failure; biomarker
200 A NOVEL SCORE BASED ON AGE AND CARDIAC BIOMARKERS PREDICTS OUTCOMES IN SEVERE SEPSIS AND SEPTIC SHOCK
A. Turley, A. Thornley, B. Kunadian, A. Roberts, M. Johnson, J. Gedney, M. de Belder. The James Cook University Hospital, Middlesbrough, UK
Background: Myocardial dysfunction is common amongst critically ill septic patients and prompt recognition is essential for the administration of the most appropriate therapy. Elevated levels of cardiac biomarkers are predictors of mortality in acute coronary syndrome patients and in unselected critically ill patients. Their diagnostic and prognostic utility in critically ill septic patients remains unclear.
Abstract 200
Aims: To evaluate the role of the cardiac markers NT-proBNP, Troponin T (TnT) and Myoglobin as predictors of in-hospital and 6-month all-cause mortality in patients admitted to a non-cardiothoracic tertiary intensive care unit (ICU) with severe sepsis/septic shock.
Methods: A prospective observational study was carried out on patients admitted to ICU within 24 h of the development of symptoms and signs of severe sepsis/septic shock. Plasma samples were taken on all patients on admission and for five sequential days. NT-proBNP, TnT and myoglobin were determined using commercially available assays. Acute Physiological and Chronic Health Evaluation (APACHE) II scores were calculated. Data were analysed for normality and analysed using Student’s t test or Mann–Whitney U test. Log-rank test was performed for Kaplan–Meier curves. Significance was assumed at the p<0.05 level.
Results: Forty nine patients were enrolled and had samples suitable for analysis. 45/49 (92%) required inotropic support on admission to ICU. No patient received recombinant human activated protein C (Xigris). Results are summarised in the table. Elevated Myoglobin was the only predictor of ITU mortality. Age, myoglobin and NT-proBNP levels predicted hospital mortality. Predictors of death by 6 months included age, peak troponin T, peak myoglobin and peak NT-proBNP levels. The APACHE II score did not predict mortality. A score was established dependent on troponin T (<0.1 = 1, ⩾0.1 = 2), age (<65 = 1, ⩽65 = 2), BNP (<10000 = 1, >10000 = 2), and myoglobin (<750 = 1, >750 = 2). Patients were subsequently placed in to tertiles (score = 4&5, 6, 7&8) to produce Kaplan–Meier curves (fig, p = 0.001).
Conclusion: In critically ill patients with severe sepsis or septic shock a score based on age and increased plasma levels of Troponin T, N terminal pro Brain Natriuretic Peptide and Myoglobin can accurately risk stratify patients and predict outcome in the short-term (<6 months). This has important clinical implications. A further study is required to confirm the potential use of cardiac biomarkers in combination with internationally recognised scoring systems such as the APACHE II score to see if this provides additional prognostic information.
troponin T; brain natiuretic peptide; sepsis
201 A UNIFYING EXPLANATION OF THE ARTERIAL PULSE WAVEFORM IN HUMANS AND THE IMPLICATIONS FOR CENTRAL BLOOD PRESSURE AUGMENTATION
J. Davies, N. Hadjiloizou, C. Manisty, Z. Whinnett, R. Foale, I. Malik, A. Hughes, K. Parker, D. Darrel, J. Mayet. International Centre for Circulatory Health, St Mary’s Hospital and Imperial College, London, UK
Background: Central pressure augmentation is becoming recognised as mechanistically important in arterial disease. It is usually explained by an indirect mechanism of earlier distal wave reflection. Yet, this mechanism ignores the direct effects the elastic properties of the aorta (reservoir or windkessel pressure) make to pressure augmentation. In this series of studies we describe a new technique to identify and separate the contributions the aortic windkessel and forward and backward travelling waves make to arterial pressure. We use this technique to assess the determinants of pressure augmentation, and go on to see how these contributions change with age and following administration of nitrate.
Method: In 20 subjects with a mean age of 53 (10) years, we measured simultaneous pressure and Doppler velocity using intra-arterial wires. We applied an established wave-only pressure separation technique and a new wave-reservoir technique, to separate and quantify the components of pressure waveform. In a subset of 6 patients intra-arterial isosorbide dinitrate was administered.
Results: The new wave-reservoir technique revealed that in all subjects reservoir pressure (17 (4.2) mmHg) exceeded waves pressure (11.1 (4.7) mmHg, p<0.001), accounting for 62% of total pressure. The backward-travelling calculated by the new technique was significantly smaller than by the wave-only technique (0.6 mmHg vs 7.2 mmHg, p<0.001). This backward-travelling wave was thus found to contribute only 3.5% to overall pressure, compared to 35.1% for forward-travelling waves and 61.4% for reservoir pressure. Reservoir pressure was found to increase with age (r = 0.67, p = 0.002), and arterial wave speed (r = 0.7, p<0.001). Following administration of nitrate, reservoir pressure fell (52 to 45.3 mmHg, p<0.04), but proximal originating pressure (34.9 vs 31.8 mmHg, p = 0.2) and distal originating pressure (2.6 vs 3.1 mmHg, p = 0.51) remained unchanged.
Conclusion: Almost all of what is generally considered “wave reflection” is in fact merely the contribution of the aortic reservoir. Thus “augmentation pressure” is principally determined by the aortic reservoir, which greatly exceeds the remnants of the forward-travelling wave from the heart and the reflected waves from the periphery. Recognition of the arterial reservoir reveals that the changes in the pressure wave which occur with age and following nitrate administration do not occur through changes in wave reflection.
physiology; ageing; nitrates
202 THE C-532T POLYMORPHISM OF THE ANGIOTENSINOGEN (AGT) GENE IS ASSOCIATED WITH ARTERIAL STIFFNESS: A POSSIBLE EXPLANATION FOR HETEROGENEITY IN GENETIC ASSOCIATION STUDIES OF AGT AND HYPERTENSION
T. Rahman1, M. Baker1, D. Hall1, P. Avery1, B. Mayosi2, J. Connell3, M. Farrall4, H. Watkins4, B. Keavney1. 1Newcastle University, Newcastle upon Tyne, UK; 2University of Cape Town, Cape Town, South Africa; 3University of Glasgow, Glasgow, UK; 4University of Oxford, Oxford, UK
Background: Many previous studies have investigated whether there is an association between genotypes at the angiotensinogen (AGT) gene and hypertensive status, but few have incorporated quantitative data. Although meta-analyses have suggested a possible effect of angiotensinogen variants on blood pressure, substantial unexplained between-study heterogeneity has been observed. We hypothesised that a primary effect of angiotensinogen variants on arterial stiffness (and thus pulse pressure) might explain such heterogeneity, and tested for such an effect in a family study.
Methods and Results: We studied 1425 individuals from 248 families ascertained via a hypertensive proband. Blood pressure was measured using 24-h ambulatory monitoring, and polymorphisms of the angiotensinogen gene that had been previously associated with hypertension and/or plasma angiotensinogen levels were typed. Pulse pressure was used as a measurement of arterial stiffness. We observed a highly significant association between genotypes at the AGT C-532T polymorphism and pulse pressure (p<0.0001). The -532T allele was associated with a 5% lower pulse pressure, in a co-dominant fashion. This resulted from genotypic effects in opposite directions both on systolic BP (slightly lower) and DBP (slightly higher) which individually were not significant even in this large study.
Interpretation: These results suggest that genetic variation at the angiotensinogen locus principally affects arterial stiffness and therefore pulse pressure. The heterogeneity observed in previous genetic studies of AGT and hypertension status could in part be explained by this finding, since case selection criteria based on systolic BP, diastolic BP, or both would result in different levels of selection for the -532T allele.
angiotensinogen; genetics; hypertension
203 DIFFERENCES IN THE MAGNITUDE RATHER THAN THE TIMING OF WAVE REFLECTION CAN EXPLAIN THE ASCOT RESULTS
C. Manisty1, J. Davies1, Z. Whinnett1, D. Francis1, A. Zambanini1, A. Zambanini1, S. Curtis1, S. Thom1, A. Hughes2, J. Mayet1. 1International Centre for Circulatory Health, Imperial College and St Mary’s Hospital, London, UK; 2International Centre for Circulatory Health and Imperial College, London, UK
Background: Treatment differences in central blood pressure have been demonstrated using pulse wave analysis in the CAFÉ trial, and this may provide an explanation for the benefits unrelated to brachial blood pressure seen in ASCOT. The greater reduction in central pressures in subjects taking amlodipine ± perindopril as compared to atenolol ± bendroflumethiazide has been attributed to different effects of the two treatments on wave reflection; however pulse wave analysis cannot discriminate whether this effect is on the magnitude or timing of the reflected wave. Wave intensity analysis enables us to isolate and measure reflection waves directly, without the need for transformation of a radial artery waveform. We are therefore able to investigate the effects of the two treatment combinations on the timing and magnitude of wave reflection separately.
Method and Results: We measured wave reflection using non-invasive wave intensity analysis in the carotid artery of 260 subjects (mean age 64 (7.7) years) in the Hypertension Associated Cardiovascular Disease (HACVD) substudy of the ASCOT trial. There were no differences either in wavespeed (p = 0.09) or the timing of wave reflection with respect to systole between subjects in the two treatment groups (p = 0.8), however the reflection coefficient was significantly lower in the amlodipine-perindopril arm than the atenolol-bendroflumethiazide arm −20% versus 23% (p = 0.02).
Conclusions: Wave intensity analysis, in contrast to pulse wave analysis, allows us to separately measure both the magnitude and timing of the reflection wave. This non-invasive method of wave separation has therefore enabled us to explain the mechanism behind the differences in central pressures seen in the two arms of the CAFÉ trial. We are able to conclude that the greater reductions in central blood pressure seen in the amlodipine ± perindopril arm of the CAFÉ trial as compared to the atenolol-bendroflumethiazide arm, were the result of greater reductions in impedance mismatch, rather than effects on heart rate, wavespeed or reflection site.
hypertension; wave reflection; wave intensity analysis
204 EFFECTS OF INHIBITION OF NITRIC OXIDE SYNTHASE ON SYSTOLIC PRESSURE AUGMENTATION AND CONDUIT ARTERY DIAMETER
S. Munir1, B. Jiang1, A. Guilcher1, S. Brett1, S. Redwood2, P. Chowienczyk1. Cardiovascular Division, King’s College London, London, UK; 2St Thomas’ Hospital, London, UK
Introduction: Exercise reduces systolic augmentation in the peripheral pulse wave, an effect similar to that produced by the nitric oxide (NO) donor nitroglycerin (NTG). Changes produced by exercise persist into the recovery period for >30 min. The aim of this study was to investigate if the exercise induced changes are dependent on endothelium-derived NO. We used the NO synthase inhibitor NG-monomethyl-L-arginine (L-NMMA) to test this.
Methods: Healthy volunteers (n = 10, 5 female, aged 19-33 years) participated in a two-phase randomised controlled crossover study. L-NMMA (6 mg/kg iv over 5 min) and saline placebo were given immediately before exercise on two occasions separated by at least 5 days. During exercise, workload increased from 25W to 150 W by increments of 25 watts at 2 min intervals. Mean arterial blood pressure (MAP, Finapress), radial augmentation index (RAIx, SphgymoCor) and cardiac output (Innocor) were measured at baseline, after infusion of L-NMMA/saline immediately before exercise, during exercise (except for radial artery measurements) and during recovery. Peripheral vascular resistance (PVR) was calculated from MAP and cardiac output. “M” mode ultrasound measurements of femoral artery diameter were made at baseline, after the infusion and during the recovery period.
Results: Before exercise, L-NMMA increased MAP (101.2 (4.3) vs 85.1 (3.8) mmHg, p<0.01), PVR (24.7 (1.7) vs. 16.4 (0.7) mmHg/ml/min, p<0.01) and RAIx (70.2 (6.5) vs 50.2 (4.5)%, p<0.01) and decreased heart rate (49.1 (2.8) vs 65.6 (5.7) bpm, p<0.01). During and after exercise, MAP and PVR were similar after L-NMMA and saline. However, L-NMMA attenuated the exercise induced fall in RAIx so that RAIx was higher after L-NMMA compared to saline at 15 min in recovery (49.5 (5.3) vs 36.0 (4.4)%, p<0.02). Exercise induced vasodilation of the femoral artery (measured in recovery) was similar after L-NMMA and placebo.
Conclusion: These results suggest that, although endothelium derived NO has little effect in regulating PVR or conduit artery diameter during/after exercise, it has a role in mediating exercise induced changes in the pulse waveform.
exercise; nitric oxide; artery
205 ASSOCIATION BETWEEN ALDOSTERONE PRODUCTION AND VARIATION IN THE GENE ENCODING 11-BETA HYDROXYLASE (CYP11B1)
H. Imrie1, M. Freel2, B. Mayosi3, E. Davies2, R. Fraser2, M. Ingram2, H. Cordell1, P. Avery1, M. Farrall4, H. Watkins4, J. Connell2, B. Keavney1. 1Newcastle University, Newcastle upon Tyne, UK; 2University of Glasgow, Glasgow, UK; 3University of Cape Town, Cape Town, South Africa; 4University of Oxford, Oxford, UK
Context: Variation in the region of chromosome 8 including the genes steroid 11-beta hydroxylase (CYP11B1) and aldosterone synthase (CYP11B2) influences mineralocorticoid and glucocorticoid metabolism. However, the relative importance of polymorphisms in CYP11B1 and CYP11B2 in determining these phenotypes is unknown.
Objective: To investigate genetic influences of the CYP11B1 and CYP11B2 genes on mineralocorticoid metabolism.
Design: We measured 24-h urinary excretion of the key metabolites of the principal mineralocortoids, glucocorticoids and androgens secreted by the adrenal cortex. We genotyped polymorphisms spanning the CYP11B1 and CYP11B2 genes which together capture all common variation at the locus.
Participants: 573 members of 105 British white families ascertained on a hypertensive proband.
Main Outcome Measures: Heritability of urinary tetrahydroaldosterone (THAldo) excretion; association of THAldo excretion with genotype.
Results: The heritability of THAldo excretion was 52% (p<10–6). There was significant association between THAldo and genotype at several of the CYP11B1/B2 polymorphisms. The strongest association was observed at the rs6387 (2803A/G) polymorphism in intron 3 of CYP11B1 (p = 0.0004). Association followed a codominant model with a 21% higher THAldo excretion per G allele. Genotype at rs6387 accounted for 2.1% of the total population variability of THAldo. We found significant association between THAldo excretion and urinary total androgen excretion, urinary tetrahydrodeoxycortisol level, and urinary cortisol metabolites (all p<0.001).
Conclusions: Aldosterone synthesis is highly heritable, and is affected by genotype at CYP11B1. Our findings support the hypothesis that genetically determined differences in 11-hydroxylation efficiency can have downstream effects on mineralocorticoid synthesis. Such effects may be of relevance to the development of low renin essential hypertension.
aldosterone; genetics; hypertension
206 CHARACTERISATION OF THE VASODILATORY ACTION OF 17β OESTRADIOL IN THE HUMAN PULMONARY CIRCULATION
A. Smith1, R. Sandher2, R. Bennett3, T. Jones4, R. Jones2, M. Cowen3, K. Channer1. 1Royal Hallamshire Hospital, Sheffield, UK; 2University of Sheffield, Sheffield, UK; 3Castle Hill Hospital, Cottingham, UK; 4Barnsley District General Hospital, Barnsley, UK
Abstract 206
Background: This study was carried out to assess for the first time, the vasodilatory effect of 17β oestradiol in the human pulmonary circulation. The influence of gender upon the response to 17β oestradiol was studied in isolated human pulmonary arteries and in isolated perfused whole lungs.
Methods: Isolated human pulmonary arteries were studied by wire myography. Vessels were obtained from male (n = 6, age 70 (4) years) and female (n = 5, age 61 (4) years) patients. Vessels were preconstricted with U46619 (1 μM) and endothelial integrity was tested with acetylcholine (1 µM). Vessels were then washed before the addition of U46619 (1 µM) prior to exposing them to either 17β oestradiol (1 nM–100 µm) or ethanol vehicle. Isolated lungs were studied in a ventilated and perfused model (methodology described in (Bennett et al, 2004)). Lung samples (n = 6) were obtained from male (n = 3, age 65 (7) years) and female patients (n = 3, age 68 (3) years). They were exposed to potassium chloride (KCl) (100 mM), prior to the addition of either 17β oestradiol (1 nM–100 µM) or ethanol vehicle.
Results: In the isolated human pulmonary arteries, 17β oestradiol caused significant vasodilatation (table). Results from the isolated perfused human lung model showed greater responses to 17β oestradiol than the pulmonary arteries (table). There was however no significant difference in the magnitude of the response to 17β oestradiol between the sexes.
Conclusion: This is the first study to show the vasodilatory properties of 17β oestradiol in the human pulmonary circulation, with no significant differences between male and female vessels. This finding may therefore have therapeutic implications for patients with pulmonary vascular disease, for example pulmonary hypertension.
human; pulmonary; oestrogen
207 VITAMIN D IMPROVES MARKERS OF VASCULAR HEALTH IN PATIENTS WITH TYPE 2 DIABETES
J. Sugden, J. Davies, M. Witham, A. Morris, A. Struthers. University of Dundee, Dundee, UK
Background: Vitamin D insufficiency is common in type 2 diabetes and is associated with an increased risk of cardiovascular events. We aimed to determine whether a single large dose of oral vitamin D could improve markers of vascular health in patients with type 2 diabetes and vitamin D insufficiency (vitamin D <50 nmol/l).
Methods: This was a double blind parallel group randomised controlled trial. Patients with type 2 diabetes were recruited from Tayside diabetes services between November 2005 and March 2006. Endothelial function measured by flow mediated vasodilation (FMD) of the brachial artery, office and 24-h blood pressure, and fasting bloods (calcium, phosphate, vitamin D, HbA1C, glucose, insulin, PTH) were assessed at baseline and 8 weeks after ingesting 100 000 U ergocalciferol or placebo.
Results: 43/87 (49%) of subjects screened had vitamin D <50 nmol/l and were included in the study. Mean age was 64.2 years, mean BMI 31.8 kg/m2 and mean baseline vitamin D 37.1 nmol/l. Patients receiving vitamin D increased their serum 25-hydroxyvitamin D by 22.9 nmol/l vs 7.6 nmol/l for the placebo group (p<0.001). Patients in the vitamin D group showed significant improvement in FMD compared to the placebo group (2.35% vs 0.06%, p = 0.048). No significant difference was seen in insulin sensitivity, HbA1c or PTH between groups.
Conclusions: Vitamin D insufficiency is common in patients with type 2 diabetes in Tayside over the winter. Supplementation with a single dose of oral vitamin D leads to significant improvements in endothelial function in patients with type 2 diabetes.
vitamin D; diabetes; endothelial function
208 C-TERMINAL PROVASOPRESSIN (COPEPTIN) PREDICTS RISK OF DEATH OR HEART FAILURE IN ACUTE MYOCARDIAL INFARCTION. THE LEICESTER ACUTE MYOCARDIAL INFARCTION PEPTIDE STUDY
S. Khan1, R. O’Brien1, J. Struck2, P. Quinn1, O. Dhillon1, N. Morgenthaler2, I. Squire1, J. Davies1, A. Bergmann2, L. Ng1. 1University of Leicester, Leicester, UK; 2BRAHMS AG, Hennigsdorf/Berlin, Germany
Introduction: The role of the vasopressin (AVP) system post-acute myocardial infarction (AMI) is unclear. Copeptin, the C-terminal part of the AVP prohormone is secreted stoichiometrically with AVP. We compared the prognostic value of copeptin and an established marker N-terminal pro-B-type natriuretic peptide (NTproBNP) post-AMI.
Methods: In this prospective single hospital study, we recruited 980 consecutive post-AMI patients (718 men, mean (SD) age 65.0 (12.2) years). Plasma measurements were made 3–5 days after chest pain onset. NTproBNP was determined using an in-house non-competitive immunoassay and Copeptin was detected using a novel commercial assay (BRAHMS AG). Patients were followed-up for the combined endpoint of death or heart failure.
Results: Median follow-up was 342 (range 0–764) days. Plasma copeptin was highest on admission (n = 132, p<0.001, day 1 vs 2–5) and reached a plateau at days 3–5. In the 980 patients, copeptin (measured at days 3–5) was raised in patients who died (n = 101) or were readmitted with heart failure (HF, n = 49) compared to survivors (median (range) pmol/l, 18.5 (0.6–441.0) vs 6.5 (0.3–267.0), p<0.0001). Using logistic regression analysis, copeptin (OR 4.00) and NTproBNP (OR 2.52), were significant independent predictors of death or HF at 60 days, with age and gender. The area under the receiver operating characteristic curves (AUC ROC) for copeptin (0.75) and NTproBNP (0.76) were similar. The logistic model with both markers yielded a larger AUC (0.82, compared to NTproBNP (p<0.04) or copeptin (p<0.01) alone respectively). Cox modelling predicted death or HF with the same variables (including log copeptin (HR 2.31), log NTproBNP (HR 2.83)), and past history of AMI and beta-blocker use. In patients stratified by NTproBNP (>median ∼900 pmol/l), copeptin above the median (∼7 pmol/l) was associated with poorer outcome (p<0.0005). Findings were similar for death and HF as individual endpoints.
Conclusion: The vasopressin system is activated post AMI. Copeptin may predict adverse outcome especially in those with an elevated NTproBNP (>∼900 pmol/l). A multimarker approach with copeptin and NTproBNP is more informative than either marker alone.
myocardial infarction; peptides; prognosis
209 KNOCKDOWN IN ZEBRAFISH SUPPORTS IMPORTANT ROLE FOR MYOCYTE STRESS 1 IN CARDIAC DEVELOPMENT AND FUNCTION
H. Mahadeva1, A. Mason1, N. Chong1, S. Shaw2, N. Samani1. 1Department of Cardiovascular Sciences, University of Leicester, Leicester, UK; 2Research Center, Massachusetts General Hospital, Massachusetts, USA
Introduction: Using molecular indexing, we previously identified and characterised a novel gene, designated myocyte stress 1 (ms1), which is upregulated within 1 h in the left ventricle following aortic banding in the rat. This suggests a possible role for ms1 in the initial signalling of the hypertrophic response. In subsequent work, we and others have shown that ms1 is expressed during embryonic cardiac development, is restricted to striated muscle and is transiently up-regulated during ischaemia-reperfusion in vitro. This suggests that ms1 may play a more widespread role in cardiac development and physiology. To investigate this further, in this study, we investigated the ms1 homologue in zebrafish.
Methods: Full length coding sequence of zebrafish ms1 (zms1) was amplified, cloned and sequenced. In situ hybridisation was performed using digoxigenin labeled RNA probes to determine sites of expression during zebrafish embryonic development. To assess the effect of knockdown of zms1, a 25mer antisense morpholino oligonucleotide was designed against the translation initiation site. A control morpholino with 5 mismatches was also designed. Morpholinos (12 ng) were injected into embryos at the 1 cell stage. The zebrafish ms1 ortholog encodes a protein of 346 amino acids. There is a high degree of homology to the H sapiens, M musculus, and R norvegicus orthologs.
Results: The earliest site of zms1 expression is the somites, where strong expression is noted by 16 somites (approximately 17 h post-fertilisation, or hpf). Expression is detectable in both chambers of the heart by 48 hpf. Other sites of expression include the developing brain, jaw structures and pectoral fins. Following injection of the antisense morpholino, by the third day of development (48–56 hpf), cardiac contractility was decreased, and the atrium was markedly enlarged; ventricular contraction was also impaired, but the ventricle was not as dilated as the atrium. These cardiac abnormalities resulted in significant pericardial oedema and decreased or absent circulation. At 56 hpf, 126/164 (77%) of embryos injected with 12 ng zms1 morpholino displayed abnormal phenotypes compared with 0/152 (0%) of embryos injected with control morpholino (χ2 = 194, p<0.001).
Conclusions: These findings directly confirm an important role for ms1 in cardiac development and function.
cardiac development; zebrafish; gene modification
210 EXPRESSION OF MYOCYTE STRESS 1, A NOVEL GENE INVOLVED IN CARDIAC DEVELOPMENT AND HYPERTROPHY IS REGULATED BY EVOLUTIONARILY CONSERVED GATA MOTIFS
S. Ounzain1, R. Peterson2, D. Menick2, N. Samani1, N. Chong1. 1University of Leicester, Leicester, UK; 2Gazes Cardiac Research Institute, South Carolina, USA
Introduction: Myocyte stress 1 (ms1) is a striated muscle specific actin binding protein that plays a central role in activating the MRTF-SRF transcriptional axis. In previous studies we have demonstrated that ventricular ms1 is transiently upregulated very early after pressure overload suggesting a possible role for ms1 in the initial signalling of the hypertrophic response. In subsequent work, we have shown that ms1 is expressed during embryonic cardiac development, with knockdown in zebrafish resulting in severe cardiac abnormalities. In order to further characterise ms1 function we have carried out a regulatory analysis to identify factors important for ms1 expression. Comparative in silico analysis identified several conserved cardiac motifs within the ms1 proximal promoter, with GATA binding sites being the most highly enriched. The cognate binding protein, GATA4, represents a key cardiac transcription factor central to cardiac development and homeostasis.
Methods and Results: To test the functionality of these sites we isolated the rat ms1 proximal promoter and cloned it into the luciferase reporter vector, pGL3-B. Transient co-transfection assays indicated that the ms1 promoter is exquisitely sensitive to ectopically expressed wild type and dominant negative forms of GATA4 in both cardiac and non-cardiac cell lines. Endogenous ms1 expression is also down-regulated by the over-expression of a dominant negative GATA4 as determined by quantitative real time RT-PCR. Chromatin immunoprecipitation (ChIP) assays confirm in vivo binding of GATA4 to the ms1 proximal promoter in adult cardiomyocytes.
Conclusions: The present findings suggest that ms1 is a novel bona fide target of GATA4. GATA4 is a key factor involved in cardiac hypertrophy and congenital heart defects. It will be of interest to investigate if any of the GATA4 disease phenotypes are a consequence of ms1 dysregulation.
gene regulation; cardiac hypertrophy; cardiac development
211 HETEROZYGOUS CARRIAGE OF THE KLOTHO KL-VS ALLELE IS ASSOCIATED WITH REDUCED RISK OF MYOCARDIAL INFARCTION
A. Whittaker1, S. Hetherington1, S. Brouilette1, R. Singh1, J. Thompson2, R. Steeds3, K. Channer3, N. Samani1. 1Department of Cardiovascular Sciences, University of Leicester, Leicester, UK; 2Department of Health Sciences, University of Leicester, Leicester, UK; 3Royal Hallamshire Hospital, Sheffield, UK
Introduction: Coronary artery disease and myocardial infarction (MI) develop as a consequence of complex gene-environment interactions and are age associated, suggesting that they are diseases of aging. Increased expression of the klotho gene in mice increases longevity and its absence is associated with the premature development of age-related phenotypes including arteriosclerosis. A functional variant of the human klotho gene termed the KL-VS allele is common in Western populations and has been associated with increased longevity in heterozygotes. We performed an association study to examine the effect of the KL-VS allele on the risk of myocardial infarction.
Methods: A total of 1445 subjects, comprising 736 MI cases and 709 controls were genotyped for the klotho KL-VS allele. The following phenotypic information was available: age, body mass index, total cholesterol level, smoking status at time of MI, history of diabetes mellitus and history of hypertension at time of MI. Since all the polymorphisms in the KL-VS allelic region are reported to be in completed linkage disequilibrium, the functional F352V polymorphism was used as a marker for determining the presence or absence of the KL-VS allele. Genotype was determined by use of the Taqman allelic discrimination technique.
Results: After adjustment for other variables, a significant protective effect of the KL-VS allele was seen in the heterozygous subjects (odds ratio (OR) 0.74 (0.57–0.97), p = 0.029), but not in rare homozygous subjects (OR 0.85 (0.38–1.88), p = 0.682). Further analysis revealed a gender difference in the effect in heterozygotes. In males, heterozygous subjects demonstrated a significant protective advantage (n = 974, OR 0.67 (0.50–0.91), p = 0.009), which was not seen in females (n = 391, OR 1.11 (0.67–1.97), p = 0.606). The effect in males was not modified by other risk factors for coronary artery disease. Our data suggest that heterozygous carriage of the klotho KL-VS allele confers a protective benefit against risk of myocardial infarction in white male subjects. Our findings are consistent with previously published data showing a heterozygous advantage of the KL-VS allele on human longevity. Taken in total, the findings indicate that further investigation of the role of klotho in coronary disease may identify novel mechanisms that could provide targets for drug development.
myocardial infarction; genetics; aging
212 APELIN EXHIBITS CARDIOPROTECTION AGAINST ISCHAEMIA REPERFUSION INJURY
J. Simpkin, D. Yellon, S. Davidson, S. Lim, A. Wynne, C. Smith. The Hatter Cardiovascular Institute, University College Hospital and Medical School, London, UK
Introduction: Apelin, the recently discovered ligand for the G-protein coupled APJ receptor has been shown to modulate cardiovascular function, fluid homeostasis and inflammation. Its beneficial actions as a positive inotrope and vasodilator have suggested a potential role in the treatment of heart failure. Its role in the context of ischaemia-reperfusion and its benefits in this clinical setting are not as yet established. Apelin is produced as a 77 amino acid pre-pro-protein peptide and as with other signalling peptides, is cleaved, to form the shorter biologically active isoforms. Evidence suggests that the shorter apelin-13 exhibits stronger activity than apelin-36.
Methods: The apelin-APJ signalling pathway activates the cell survival cascades Akt/PKB and p42/44 MAPK in various cell-based systems. These kinases have been associated with the so-called pro-survival Reperfusion Injury Salvage Kinase (RISK) pathway. We therefore hypothesised that apelin could protect the heart via the activation of the RISK pathway in an ischaemia-reperfusion (I/R). Both Langendorff and in vivo open chest murine, I/R heart models were used to examine the effects of apelin-13 and apelin-36 on infarct size. Western blot analysis was used to investigate the role of the anti-apoptotic signalling kinases PI3K/AKT and p42/44 MAPK. This was complemented with measurements of mitochondrial permeability transition pore (MPTP) opening, the induction of which seems to play a pivotal role in mitochondrial swelling and cell death.
Results: Both apelin-13 and apelin-36 reduced infarct size significantly (apelin-13 (1 µM) 31.4% (4.03)** and apelin-36 (1 µM) 38.4%±3.02* vs 52.03% (4.38) for control in the isolated heart model; apelin-13 (0.1 mg/kg) 27.8% (4.86)** and apelin-36 (0.27 mg/kg) 32.9% (4.36)* vs 48.9% (4.44) for control; in vivo model (**p<0.01 and *p<0.05). This protection was blocked in the isolated heart model by LY294002 and UO126 inhibitors of PI3K/AKT and p42/44 MAPK. Western blot analysis confirmed that apelin stimulated AKT and p42/44 phosphorylation, which was inhibited by LY294002 and UO 126. Additionally, apelin-13 and apelin-36 delayed MPTP opening and time to rigor, with the effect of apelin-13 being inhibited by LY294002 and MEK inhibitor 1, an alternative p44/42 blocker. The apparent isoform-dependent difference is in keeping with the current evidence that apelin-36 may function as a precursor to the more biologically active form, apelin-13. This is the first study to demonstrate that apelin induces cardioprotection via the PI3K/Akt and p42/44 MAPK anti-apoptotic pathways.
apelin; ischaemia/reperfusion; protection
213 HYPOXIC AND PHARMACOLGICAL POSTCONDITIONING PROTECTS THE HUMAN HEART BY ACTIVATING PHOSPHATIDYLINOSITOL-3-KINASE
N. Mudalagiri, D. Hausenloy, D. Yellon. The Hatter Cardiovascular Institute, UCL, London, UK
Introduction: Ischaemic postconditioning (brief intermittent episodes of ischaemia and reperfusion, at the onset of reperfusion) and pharmacological postconditioning (administration of erythropoietin (EPO) at the point of reperfusion) have been demonstrated to offer significant cardiac protection in animal studies. Although protection in these settings has been linked to activation of phosphatidylinositol-3-kinase (PI3K), the underlying mechanism of protection in the human heart has not been demonstrated. We hypothesised that both pharmacological and hypoxic postconditioning could protect the human myocardium and that the cardioprotective mechanisms involved were similar to that observed in the animal setting.
Methods: Isolated human atrial trabeculae removed from patients undergoing cardiac bypass surgery were suspended in an organ bath and exposed to 90 min of hypoxia followed by 120 min of reoxygenation. The hypoxic and pharmacological protocols for postconditioning consisted of brief periods of reoxygentation and hypoxia or the administration of erythropoietin at the point of reoxygenation, respectively. Cardiac function was assessed by measuring the developed force of contraction which was calculated as a percentage of the baseline force of contraction.
Results: Hypoxic postconditioning with 4 cycles of 30 seconds of reoxygenation and 30 seconds of hypoxia did not provide any cardioprotection (28.3% (3.4) vs 26.3% (2.4) for control). However, changing the postconditioning protocol to 4 cycles of 60 seconds of reoxygenation and 60 seconds of hypoxia provided significant cardiac protection (43.2% (3.1) vs 26.3 (2.4) for control, p<0.002). This protection was abrogated in the presence of the PI3K inhibitor LY294002 (27.4% (3.7) vs 26.3% (2.4) for control). Pharmacological postconditioning with EPO significantly improved the developed force of contraction when administered at reoxygenation (46.7% (1.7) vs 30.2% (2.2) for control, p<0.001). The cardioprotective effects of EPO were abrogated by the use of LY294002 (29.4% (2.5) vs 30.22% (2.2) for control). Hypoxic and pharmacological postconditioning provided very similar degrees of protection to that observed when preconditioning was used as a positive control (43.2% (3.1) (hypoxic postconditioning), 46.7% (1.7) (pharmacological postconditioning) and 45.4 (3.2) for preconditioning).
Conclusions: Our data demonstrate for the first time that both hypoxic and pharmacological postconditioning protects the human myocardium and that the observed protection is mediated by activation of a common factor, namely the prosurvival kinase, PI3K. These data therefore, supports the potential use of EPO as a pharmacolgical postconditioning agent and as a novel cardioprotective strategy when used alone or as an adjunct in the clinical setting alongside existing reperfusion therapies.
human; postcondition; erythropoietin
214 IMPROVEMENT IN VASCULAR FUNCTION WITH LOW-DOSE FOLIC ACID SUPPLEMENTATION: IMPLICATIONS FOR FOLATE THERAPY AND DIETARY FORTIFICATION
C. Shirodaria, C. Antoniades, J. Lee, C. Jackson, J. Francis, M. Robson, C. Ratnatunga, R. Pillai, S. Neubauer, K. Channon. University of Oxford, John Radcliffe Hospital, Oxford, UK
Background: Folic acid appears to improve vascular function. We have previously shown that 5-methyltetrahydrofolate (5-MTHF), the active metabolite of folic acid, has beneficial effects on endothelial function by reducing peroxynitrite-induced oxidative stress and improving nitric oxide bioavailability. However, recent clinical trials have found no additional clinical benefit from folic acid therapy in vascular disease patients from a folate-fortified population. We therefore compared the effects on vascular function of low dose folic acid therapy (achievable with dietary folate fortification) and high dose folic acid therapy in a non-folate fortified population, and determined the relationship between plasma folate and both plasma and vascular tissue concentrations of 5-MTHF.
Abstract 214
Methods: In a double-blind placebo-controlled trial, 56 patients (mean age 63 (1) years) with coronary artery disease undergoing coronary bypass surgery were randomised to receive folic acid 400 µg/d or 5 mg/d, or placebo, for 7 weeks. Plasma folate and 5-MTHF levels were measured at baseline and prior to CABG. 5-MTHF levels were measured in tissue samples of internal mammary artery (IMA) and saphenous vein (SV). Changes in aortic arch pulse wave velocity (a measure of arterial stiffness) and brachial artery flow-mediated dilatation (FMD; a measure of endothelial function) were quantified by high-resolution cine MRI (1.5T).
Results: Baseline plasma folate levels were in keeping with a non-fortified population. Both aortic pulse wave velocity and FMD were improved after folic acid 400 µg/d and 5 mg/d, but no additional improvement was seen in the 5 mg/d group (table 1). Plasma folate and 5-MTHF levels increased significantly in the 5 mg/d-treated group compared to the 400 µg/d group (fig A). Vascular tissue 5-MTHF levels were similarly increased in both treatment groups compared with placebo (fig B).
Conclusion: Despite a large difference in plasma levels, vascular tissue 5-MTHF levels are similar after both low- and high-dose folic acid therapy, leading to similar improvements in arterial stiffness and endothelial function. Low-dose folic acid therapy, achievable through dietary fortification, may be a useful therapeutic strategy in non-folate fortified vascular disease populations. However, folic acid therapy at high dose, or in folate-fortified populations, is unlikely to confer additional clinical benefit.
folic acid; MRI; endothelial function
215 SUDDEN ARRHYTHMIC DEATH SYNDROME: DIAGNOSTIC YIELD OF CLINICAL SCREENING IN FAMILY MEMBERS AT THE HEART HOSPITAL, UNIVERSITY COLLEGE LONDON, 2003–6
P. Lambiase1, J. Kaski1, E. Firman1, P. Elliott1, A. Ahmed1, A. Chow1, S. Hughes2, M. Sheppard3, M. Lowe1, W. McKenna1. 1Heart Hospital, UCL, London, UK; 2UCL, London, UK; 3Royal Brompton Hospital, London, UK
Background: Sudden arrhythmic death syndrome (SADS) arises through disorders of ion channel function or structural heart disease. It accounts for over 400 deaths in the UK per annum. The role of family screening is becoming increasingly recognised in the primary prevention of SADS. To date there has been no comprehensive analysis of the diagnostic yield and efficacy of a family screening approach in SADS index cases where the postmortem heart is structurally normal after expert pathological review.
Methods and Results: 118 SADS families where the SADS victim died between 1 and 35 years of age were evaluated in a systematic family screening programme between 2003–6. All SADS index cases had a structurally normal heart after expert review. All studied relatives underwent resting, signal averaged ECG, 24-h Holter, exercise ECG with V02 max, transthoracic echocardiography and an ajmaline challenge test after initial clinical screening. The most common modes of death were rest in 28%, sleep in 25% and exercise in 18%. An inherited electrical cause of SADS was identified in 41 of the 118 families (35%)—20 Brugada, 18 long QT syndrome (LQTS), 3 catecholiminergic polymorphic ventricular tachycardia (CPVT). Structural heart disease was identified in 5 ARVC and 2 DCM families. 26 ICDs have been implanted in affected family members—4 LQTS, 7 Brugada, 2 CPVT, 2 ARVC, 2 DCM and 9 on clinical grounds without a definitive diagnosis. The ECG (37%) and ajmaline challenge test (49%) had the highest diagnostic yield in families with a positive diagnosis.
Conclusion: A systematic screening approach in relatives of SADS victims has a high diagnostic yield of 35% despite the index case having a structurally normal heart at post mortem. Electrical causes of SADS predominate in these families. These findings demonstrate that a systematic clinical screening programme in SADS families is both achievable and effective. The full impact of gene testing upon diagnostic yield is awaited.
SADS; gene; family screening
216 ELECTROPHYSIOLOGICAL AND ANATOMIC CHARACTERISATION OF SITES RESISTANT TO ELECTRICAL ISOLATION DURING CIRCUMFERENTIAL PULMONARY VEIN ABLATION FOR ATRIAL FIBRILLATION: A PROSPECTIVE STUDY
P. Kistler1, K. Rajappan1, S. Yen Ho2, M. Morpher1, S. Harris1, D. Abrams1, D. Gupta1, S. Sporton1, R. Schilling1. 1The Department of Cardiology, St Bartholomew’s Hospital and Queen Mary University, London, UK; 2National Heart and Lung Institute, Imperial College, London, UK
Background: Complex pulmonary vein (PV)–left atrial connections may make achieving electrical isolation (EI) by wide encirclement of the pulmonary veins (WEPV) during catheter ablation (CA) challenging. We examined the anatomical and technical features associated with resistance to electrical isolation during PV EI using WEPV in a prospective study.
Methods: 101 (mean age 56 (11) years) consecutive patients with symptomatic AF (paroxysmal 63, persistent 38) underwent first-time CA using electroanatomic mapping with CT integration (registration error 2.4 (0.5) mm). Following double trans-septal puncture WEPV was performed. Next, using a circular mapping catheter sites of earliest PV breakthrough were identified. If no electrogram was present at this site CA was performed inside the WE line. All sites of EI were tagged. Anatomic studies of the corresponding regions of the venoatrial junction in 24 adult hearts were then performed.
Results: Sites resistant to EI were located at the inferior quadrant (p<0.001) for the right superior PV (RSPV), superior quadrant (p<0.001) for the right inferior PV (RIPV) and the inferior and anterior quadrants (p<0.001) for the left superior PV LSPV) (fig). EI was significantly less frequent at the posterior quadrant (p<0.001) for the left inferior PV (LIPV) (fig). One reason for this distribution was that CA was necessary on the intervenous ridge inside the WE on the right in 51% and on the left in 41% of patients, resulting in simultaneous EI of both right PVs in 42% and both left PVs in 24%. Another was that the ridge between the LPV and left atrial appendage (LAA) was a commonly resistant site. The importance of the LPV/LAA ridge was investigated by anatomic studies which demonstrated considerable variation in the narrowest width (3–23.7 mm) and transmural thickness (1–5 mm) in this region.
Conclusion: Sites of EI after WEPV have a preferential distribution determined by anatomic features. CA on the intervenous ridge is required in a significant proportion of patients to achieve EI. Atrial folds and ridges result in thicker myocardium creating technical and anatomic challenges for achieving transmural lesions.
catheter ablation; atrial fibrillation; pulmonary vein anatomy
217 RECOGNITION OF ECG ABNORMALITIES ASSOCIATED WITH ATRIOVENTRICULAR CONDUCTION DEFECTS
J. McComb, C. Plummer. Freeman Hospital, Newcastle upon Tyne, UK
Introduction: We have investigated some of the potential reasons for the low pacemaker implantation rate in the UK, and have demonstrated failure to recognise class I/IIa pacemaker indications in some patients. It is not clear whether this is due to lack of knowledge of pacemaker indications alone, or failure to interpret ECGs correctly.
Method: ECGs and a brief clinical history were presented to 132 internal medicine physicians, who were asked to describe the ECG abnormality and to state whether or not there was a pacemaker indication according to ACC/AHA 2002 guidelines. The 4 ECGs showed (1) complete heart block (CHB), heart rate <30 beats per minute (bpm); (2) 3:1 2° atrioventricular (AV) block, rate <30 bpm; Mobitz 2 AV block, with right bundle branch block (RBBB); trifascicular block (RBBB, left axis deviation and 1° AV block). All 4 patients had symptoms.
Results: ECG 1 (CHB): 64.6% recognised CHB: of these 95.7% recognised it as a pacing indication in a man with recurrent dizzy spells. 32.7% failed to recognise the rhythm, but despite this, 58.3% thought there was a pacing indication. 80.8% altogether recognised a pacing indication, regardless of whether they recognised the ECG diagnosis. ECG 2 (2° AV block): 44.7% recognised 3:1 2° AV block, but only 50.8% recognised this as a pacing indication in an elderly patient with palpitations. 47.7% misdiagnosed the rhythm, but 30.2% of these thought there was a pacing indication. In all, only 37.1% recognised a pacemaker indication. ECG 3 (Mobitz 2 AV block): Only 19.4% recognised Mobitz 2 AV block, and of these, only 63.2% thought there was a pacemaker indication in a patient with syncope. 63.3% did not recognise the rhythm, but despite this 22.6% thought there was a pacing indication. In all, 28.6% recognised a pacing indication. ECG 4 (trifascicular block): 34% recognised trifascicular block in a patient with falls. 75% of these recognised it as a pacing indication. 55.7% did not recognise the ECG diagnosis, but 11.9% of these recognised a pacing indication. In all, 33% recognised a pacing indication.
Conclusions: Although the majority of general physicians recognise CHB, they frequently fail to recognise ECG evidence of more subtle conduction disturbance, such as trifascicular block. Also, although they make a correct ECG diagnosis, they may not recognise it as a pacemaker indication. This lack of knowledge may contribute to low pacing rates.
AV block; pacemaker; ECG
218 LONG-TERM EFFECTS OF CARDIAC RESYNCHRONISATION THERAPY IN PATIENTS WITH CHRONIC ATRIAL FIBRILLATION
S. Chalil, K. Khadjooi, S. Muhyaldeen, R. Smith, F. Leyva. Good Hope Hospital, Sutton Coldfield, UK
Background: The benefits of cardiac resynchronisation therapy (CRT) for patients with heart failure and sinus rhythm are well established. Small studies have suggested that CRT may not confer similar benefits in patients with heart failure and chronic atrial fibrillation (AF).
Methods: Forty four consecutive patients with heart failure in chronic AF (mean age 70.0 (SD 11.1), NYHA class III or IV, LVEF<35%, QRS⩾120 ms) underwent CRT. Post-implantation programming included the sense-pace response, in which a sensed event in one ventricle leads to pacing of the other ventricle. These patients were compared to 115 age-matched patients with heart failure and sinus rhythm (SR) undergoing CRT. All patients underwent a clinical assessment, including 6-min walking distance and quality of life (Minnesota Living with Heart Failure questionnaire), and transthoracic echocardiography on the day before implantation, at 1 month, 3 months and 6 monthly thereafter.
Results: After a mean follow-up of 909 days for events, no difference emerged in the composite of death from any cause or an unplanned hospitalisation for a major cardiovascular event (MCE), the composite of death from any cause and unplanned hospitalisation with worsening HF, mortality from any cause or cardiovascular mortality (see table). Kaplan-Meier survival curves and Cox proportional hazards analyses failed to show a difference in these endpoints between the AF and the SR groups. Up to the last available follow-up, patients in AF improved symptomatically to the same degree as patients in SR, with respect to changes in NYHA class (1.9 (0.8) vs 2.1 (0.8), respectively, both p<0.0001), 6-min walking distance (92.7 (97.0) and 77.7 (106.2), respectively, both p<0.0001) and quality of life scores (−22.3 (23.9) vs 21.0 (23.2), respectively, both p<0.0001). The reduction in left ventricular end-diastolic volume was more marked in the AF group (22.3 ml, p = 0.0095) than in the SR group (8.65 ml, p = NS). The reduction in left ventricular end-systolic volume was also more marked in the AF group (28.3 ml, p = 0.001) than in the SR group (10.1 ml, p = 0.0668). Improvements in LVEF were more marked in the AF group (8.3%, p<0.0001) than in the SR group (2.6%, p = 0.042).
Conclusion: CRT in patients with chronic AF is associated with a long-term mortality and morbidity which is comparable to patients in sinus rhythm. The symptomatic benefit in terms of NYHA class, exercise capacity and quality of life is also comparable and the negative remodelling effects are more marked. Further studies are needed to determine whether this effect is partly due to sense-pace programming.
cardiac resynchronisation therapy; heart failure; atrial fibrillation
219 LONG-TERM SURVIVAL OF PATIENTS WITH A NEW DIAGNOSIS OF HEART FAILURE: A POPULATION BASED PROSPECTIVE COHORT STUDY
M. Roughton1, I. Mannan2, G. Sutton3, D. Wood3, K. Fox4, M. Cowie3. 1Royal Brompton & Harefield NHS Trust, London, UK; 2Faculty of Medicine, Imperial College, London, UK; 3National Heart & Lung Institute, Imperial College, London, UK; 4Charing Cross Hospital, London, UK
Background: Long-term survival of newly diagnosed heart failure patients is not well described. This study investigated the long-term survival prospects of patients with incident heart failure to determine the likelihood of survival and to develop a prognostic scoring system which might be used to predict patient mortality.
Methods: The London Heart Failure study is a cohort of 552 incident heart failure patients recruited between April 1995 and March 1998. All patients were followed up for all-cause mortality. Survival was estimated using a Kaplan–Meier survival curve. The expected survival of the cohort was estimated using age-sex matched predicted survival for the period 1996–2001 for South-East England, obtained from the Government Actuaries Department. This was then used to calculate standardised mortality ratios (SMR) to determine excess mortality attributable to heart failure. Cox proportional hazard modelling was used to determine clinical and demographic factors that were associated with survival.
Results: At the time of the current analysis 425 patients (77%) had died and the maximum follow up was 10.84 years with median (IQR) of 3.05 (0.48–8.01), representing 2224 person years of follow-up. Mortality immediately after diagnosis was high with 22% of patients dying within 3 months and 31% dead within a year of diagnosis. Survival at 10 years was 21%. The SMR for the first year after diagnosis was 745. Over the full period of follow-up the SMR of the cohort was 336. Six factors at initial presentation were independently associated with survival on Cox modelling: age, serum creatinine, lung crackles, NYHA class, diastolic blood pressure and serum sodium. The age of a patient at diagnosis was the factor most significantly associated with survival. Patients with levels of creatinine between 120 and 170 µmol/l, or over 170 µmol/l, were 1.46 (95% CI 1.49–1.52) and 3.17 (3.14–3.20) times more likely to die than patients with levels below 120 µmol/l. Patients with crackles throughout the lung fields were 1.50 (1.49–1.52) times more likely to die than those with no crackles. Those with a serum sodium <140 mmol/l were 1.22 (1.21–1.23) times more likely to die than those with a higher sodium, and patients with DBP <90 mmHg were 1.44 (1.43–1.44) times more likely to die than those with a higher BP. Patients with NYHA class IV were 1.69 (1.67–1.72) times more likely to die than those in Class II. The predictive power of the Cox model was high, with an area under the ROC curve of 0.80 (95% CI 0.75–0.84) at the latest follow-up time. A colour-coded clinical scoring chart was developed based on these 6 factors which gives the likelihood of survival at 1, 5 and 10 years after diagnosis.
Conclusions: Long-term survival with heart failure is possible. A simple clinical scoring system can be used to stratify mortality risk and identify patients for more aggressive therapy.
heart failure; prognosis; risk
220 INTRAVENTRICULAR DYSSYNCHRONY PREDICTS MORTALITY AND MORBIDITY FOLLOWING CARDIAC RESYNCHRONISATION THERAPY: A STUDY USING CARDIOVASCULAR MAGNETIC RESONANCE TISSUE SYNCHRONISATION IMAGING
S. Chalil1, B. Stegemann2, S. Muhyaldeen1, K. Khadjooi1, H. Sandman1, R. Smith1, F. Leyva1. 1Good Hope Hospital, Sutton Coldfield, UK; 2Medtronic Inc, Maastricht, the Netherlands
Background: Cardiac dyssynchrony is a predictor of mortality in patients with heart failure (HF). We aimed to assess a novel measure of left ventricular (LV) dyssynchrony, a cardiovascular magnetic resonance-tissue synchronisation index (CMR-TSI), in relation to QRS duration in patients with HF. A further aim was to determine whether CMR-TSI predicts mortality and major cardiovascular events (MCE) following cardiac resynchronisation therapy (CRT).
Methods: Radial wall motion data for up to 60 myocardial segments of a short-axis LV stack (steady-state free precession CMR sequence) were quantified. The segmental radial wall motion data (y) were fitted to an empirical sine wave function y = a + b * sin (t/RR + c). The mean segmental radial wall motion (a), the cyclic segmental radial wall motion amplitude (b) and the segmental phase shift of the maximum radial wall motion (c) were extracted from the fit. The CMR-TSI was calculated as the standard deviation of all segmental phase shift of the radial wall motion extracted from the fit. In substudy A, CMR-TSI was assessed in 66 patients with HF (mean (SD) age 60.8 (10.8) years, LVEF 23.9 (12.1)%) and 20 age-matched controls. In substudy B, CMR-TSI was assessed in relation to clinical events in 77 patients with HF and with a QRS ⩾120 ms undergoing CRT.
Results: In analysis A, CMR-TSI was higher in patients with HF and a QRS<120 ms (79.5 (31.2) ms, p = 0.0003) and in those with a QRS ⩾120 ms (105.9 (55.8) ms, p<0.0001) than in controls (21.2 (8.1) ms). At a cut-off of 40 ms, CMR-TSI achieved almost absolute discrimination between controls and patients with HF (area under receiver operator curve: 0.99, sensitivity 94%, specificity of 100%, p<0.0001), reflecting the lack of overlap in CMR-TSI between the groups. In analysis B, a CMR-TSI ⩾110 ms emerged as an independent predictor of the composite endpoints of death or unplanned hospitalisation for MCE (HR = 2.45 (95% CI 1.51 to 4.34, p = 0.0002)) or death from any cause or unplanned hospitalisation for HF (HR = 2.15 (1.23 to 4.14, p = 0.0060) as well as death from any cause (HR = 2.6 (1.29 to 6.73, p = 0.0061) and cardiovascular death (HR = 3.82 (1.63 to 16.5, p = 0.0007) over a mean follow-up of 763 days. At a cut-off of CMR-TSI⩾110 ms predicted cardiovascular death with a sensitivity of 93% and a specificity of 67% (p<0.0001). In multivariate Cox proportional hazards analyses, LV volumes, LVEF and QRS duration failed to emerge as predictors of these endpoints.
Conclusions: Myocardial dyssynchrony assessed by CMR-TSI is a powerful independent predictor of mortality and morbidity following CRT. This finding supports a role for CMR assessment of cardiac dyssynchrony in potential candidates for CRT.
cardiac resynchronisation therapy; heart failure; magnetic resonance imaging
221 ECHOCARDIOGRAPHIC OPTIMISATION OF INTER-VENTRICULAR DELAY IMPROVES EXERCISE PERFORMANCE COMPARED TO SIMULTANEOUS BIVENTRICULAR PACING
D. Fox1, R. Khattar2, A. Fitzpatrick2, A. Borg1, N. Clayton1, R. Beynon1, S. Williams1, W. Khan1, S. Shaw1, S. Roberts2, N. Davidson1. 1North West Regional Cardiac Centre, Wythenshawe Hospital, Manchester, Manchester, UK; 2Manchester Heart Centre, Manchester Royal Infirmary, UK, Manchester, UK
Background: Cardiac resynchronisation therapy (CRT) improves exercise capacity and prognosis in patients with congestive heart failure (CHF). Peak oxygen uptake (VO2max) is an objective measure of exercise capacity and correlates with survival. CRT devices can vary inter-ventricular delay by pacing either ventricle ahead of the other and echocardiographic studies have demonstrated acute haemodynamic benefits of sequential rather than synchronous ventricular stimulation. No previous data exist on the clinical effects of adjusting the inter-ventricular delay. We sought to establish whether echocardiographic optimisation of the inter-ventricular delay affects exercise capacity as measured by VO2max.
Methods: Thirty one patients with symptomatic CHF undergoing CRT (24 men, mean (SD) age 62.4 (9.5)), QRS >120 ms and LVEF <30% had a baseline cardiopulmonary exercise test (CPX). After implantation of a CRT device, patients underwent an echocardiographic study to assess 4 different settings of inter-ventricular delay. The optimal setting for each patient was determined by the maximal aortic velocity time integral (VTI). Patients were then randomised in a double blind fashion to 6 weeks each of active CRT with the four settings of inter-ventricular delay (using a constant A-V delay of 100 ms). The settings used were simultaneous right ventricular (RV) and left ventricular (LV) pacing (SIM), RV 20 ms ahead of LV (RV20), LV 20 ms ahead of RV (LV20) and LV 40 ms ahead of RV (LV40). After each paced period patients underwent repeat CPX. We calculated (1) mean VO2max for each of the four settings tested and (2) mean VO2max from each patient on the “VTI optimised” setting.
Results: Mean (SEM) baseline VO2max was 12.1 (0.6) ml/kg/min. Mean values of VO2max on each of the settings were: SIM: 13.5 (0.8), RV20: 13.1 (0.7), LV20: 13.7 (0.8) and LV40: 13.4 (0.8). Each of these was a significant improvement from baseline (p<0.01) but none of the 4 settings was significantly better than the others. The optimised interventricular delay produced a mean VO2max of 14.4 (0.8) which was superior to standard SIM (p = 0.0015).
Conclusions: Although all settings of inter-ventricular delay significantly improved VO2max from baseline, echocardiographic optimisation produced a significant improvement in VO2max above that seen with simultaneous biventricular pacing. Routine optimisation of the inter-ventricular delay could improve the functional response to CRT and reduce the number of “non-responders”.
inter-ventricular delay; biventricular pacing; sequential CRT
222 LONG-TERM LEFT VENTRICULAR LEAD STABILITY DURING BIVENTRICULAR PACING
J. Willis, D. Thomas, G. Webb, A. Penny, P. O’Callaghan, R. Anderson, Z. Yousef. University Hospital of Wales, Cardiff, UK
Background: Left ventricular (LV) lead placement during biventricular pacing (BiV) can be problematic due to anatomical reasons and because the LV lead lacks fixation mechanisms. As a result, concern has been raised about the long-term stability of the LV lead threshold. We therefore retrospectively examined the 12-month LV lead characteristics in patients undergoing BiV implantation at our institute.
Abstract 222
Methods: Details from BiV pacing records between Nov ‘98 and Aug 06 were extracted (n = 98, mean patient age 64 years, 80% male). For each case, we collected data on (a) aetiology of heart failure (ischaemic vs non-ischaemic cardiomyopathy), (b) lead type (unipolar vs bipolar), and (c) coronary sinus branch vein used (antero-lateral vs middle cardiac vs postero-lateral veins). The measure of LV lead stability (stability index) used in this study was the product of the measured LV lead threshold (volts) X Pulse Duration (msec). Stability index data for the three clinical variables are shown in the table at the time of lead implant, 24 h, 3 months and 12 months after implant.
Conclusion: Our experience suggests that overall long-term LV lead stability is excellent. Furthermore, LV lead stability does not appear to be influenced by the aetiology of heart failure or the coronary sinus branch vein used. Although the stability index of bipolar leads tends to be higher than unipolar leads, long-term stability of both leads are excellent.
biventricular pacemaker; lead stability; LV lead
223 EFFECT OF POSTEROLATERAL LEFT VENTRICULAR SCAR ON MORTALITY AND MORBIDITY FOLLOWING CARDIAC RESYNCHRONISATION THERAPY: A LATE GADOLINIUM ENHANCEMENT CARDIOVASCULAR MAGNETIC RESONANCE STUDY
S. Chalil1, S. Muhyaldeen1, K. Khadjooi1, R. Smith1, P. Jordan1, K. Patel2, F. Leyva1. 1Good Hope Hospital, Sutton Coldfield, UK; 2Sandwell and City Hospitals, Birmingham, UK
Background: Up to 30% patients treated with cardiac resynchronisation therapy (CRT) do not respond. It has been shown that in patients with a posterolateral (PL) left ventricular scar, CRT leads to suboptimal resynchronisation. This study explores the effect of a PL scar on mortality and morbidity following CRT.
Methods: Sixty two patients with heart failure due to coronary heart disease (age 67.3 (9.6) years (mean (SD), 45 male, NYHA class III or IV, LVEF⩽35%, left bundle branch block, QRS⩾120 ms) underwent late gadolinium enhancement cardiovascular magnetic resonance (LGE-CMR) for quantification of myocardial scar. Scar volume was expressed as a % of left ventricular myocardial volume. Patients were followed up for 741 (75–1602) days (mean (range)).
Results: 14/33 (42%) patients with a PL scar died, compared to only 2/29 (7%) in non-PL scar group (p = 0.0014). The presence of a PL scar, which was demonstrated in 33/62 patients, emerged as an independent predictor of the composite endpoints of cardiovascular death or unplanned hospitalisation for major cardiovascular events (HR = 2.57 (95% CI 1.58 to 4.8, p<0.0001) and cardiovascular death or hospitalisation for worsening heart failure (HR = 3.06 (1.63 to 7.7), p<0.0001) as well as cardiovascular death (HR = 2.63 (1.39 to 6.65), p = 0.0016). A transmural PL scar was the strongest predictor of all endpoints (all p<0.0001). 100% of patients in the non-transmural PL scar group were responders (improvement by ⩾1 NYHA class or 25% 6-min walking distance (6-MWD)), compared to 47% in the transmural PL scar group. 6-MWD and quality of life improved in the non-transmural PL scar group (p<0.001), but not in the transmural PL scar group. In patients with a PL scar, pacing over non-scar was associated with a lower mortality and morbidity (all p<0.05) as well as with a better response to CRT (responder rate: 94 vs 56%, p = 0.0112) than pacing over the scar.
Conclusions: A PL scar, detected using LGE-CMR, is associated with a worse clinical outcome following CRT, particularly if it is transmural. In patients with a PL scar, pacing over the scar carries a greater risk of mortality and morbidity than pacing over the non-scarred left ventricular free wall. This study highlights the role of CMR in the risk-stratification as well as in the selection of left ventricular pacing sites in patients with ischaemic cardiomyopathy undergoing CRT.
cardiac resynchronisation therapy; magnetic resonance imaging; cardiac dyssynchrony
224 AF MAY BEGET AF BUT DOES PAF BEGET PAF?
J. Silberbauer1, R. Veasey1, E. Cheek2, G. Lloyd1, A. Sulke1. 1East Sussex Hospitals NHS Trust, Eastbourne, UK; 2University of Brighton, Brighton, UK
Introduction: Atrial fibrillation cycle length (AF CL) correlates closely with atrial effective refractrory period (AERP). AERP is related to preceding heart rate (rate adaptation) and undergoes diurnal variation due to sympathovagal influences. Shortening of AERP (remodelling) is seen in paroxysmal atrial fibrillation (PAF) disease progression and predicts early recurrence after cardioversion. Non-random clustering and diurnal variation in paroxysmal atrial fibrillation onset is well described. We have modelled the factors affecting AF CL and PAF onset patterns.
Methods: 668 PAF episodes in 37 patients with advanced AF pacemakers were studied. Pacemaker AF episode diaries and Detailed Onset Reports were used for data collection. AF diaries provided time of episode onset, time of prior episode termination, current and previous episode duration. Detailed onset reports provided the preceding atrial cycle length, AF-initiating premature atrial contraction (PAC) coupling interval and high right atrial AF cycle length. All of these factors were statistically modelled (fig). Diurnal variation of PAF onset, and specifically early recurrence of AF (ERAF) and the relevance of rate adaptation and the PAC coupling interval were evaluated. A patient adjusted AF CL was used to account for variation between patients and within patients after multiple follow-up. The patient adjusted AF CL was derived by dividing the individual AF onset AF CL by the overall mean AF CL for each patient (thus values less than 1 represent shortening of the AF CL and greater than 1 the converse).
Results: Significant diurnal variation in AF-initiating PAC coupling intervals (p = 0.002), sinus rate (p = 0.04) and adjusted AF CL (p<0.0001) were noted. Mixed modelling showed the most important factors affecting the adjusted onset AF CL were the initiating PAC coupling interval, (p<0.0001), and the length of the prior AF episode, particularly if it was recent i.e. within the preceding 5 mins (p<0.0001). The preceding sinus rate only affected the adjusted AF CL in the absence of AF recurrence (p = 0.02). Furthermore, the initial adjusted PAF onset AF CL predicted the duration of the current AF episode (p<0.0001).
Conclusion: Correcting for diurnal variation, more rapid sinus rate and shorter AF-initiating coupling intervals cause a relative shortening of the AF onset AF CL. Rate-adaptation is therefore maintained in PAF. This effect is weaker if there has been a recent, especially long, episode of PAF suggesting that the prior AF episode is the main factor that causes a shortening of the AF CL. Shortening of the AF CL at the onset of PAF strongly predicts longer subsequent PAF episodes. Thus extended ERAF episodes cause a shortening of the AF CL and predispose to longer subsequent AF episodes, hence PAF does beget PAF.
atrial fibrillation cycle length; paroxysmal atrial fibrillation; early recurrence
225 ELECTROPHYSIOLOGICAL CHARACTERISTICS OF SYMPTOMATIC ATRIAL FIBRILLATION
R. Veasey1, J. Silberbauer1, E. Cheek2, A. Arya1, A. Sulke1. 1East Sussex Hospitals NHS Trust, Eastbourne, UK; 2University of Brighton, Brighton, UK
Introduction: The majority of atrial fibrillation (AF) episodes in patients with paroxysmal AF are known to be asymptomatic. The specific electrophysiological characteristics relating AF episodes and symptoms are poorly understood. Modern beat to beat pacemaker Holters provide extensive electrophysiological data during arrhythmia onset which can be correlated with patient symptoms.
Methods: Seventy nine patients (mean age 71 (8), 54% male) with symptomatic paroxysmal atrial fibrillation (PAF), AF burden of 1 to 50% and DDDRP pacemakers were enrolled. During the study period patients recorded symptom onset and duration. Mixed modelling accounted for time of day and interpatient variability.
Results: Corresponding Holter and symptom data were analysed (mean 51 days per patient). Overall 333 symptomatic atrial tachyarrhythmia episodes, 2305 asymptomatic atrial tachyarrhythmia episodes and 194 non-atrial tachyarrhythmia symptomatic episodes were identified giving a sensitivity of 12.6% and a positive predictive value of 63.2% for specific AF symptoms. Symptomatic AF was 3.8 times more likely during the day (p<0.001). Accounting for diurnal variation, symptomatic AF was associated with a shorter AF cycle length (CL) (p = 0.005), shorter PAC-initiating cycle length (p = 0.005), faster ventricular rate (p = 0.001), faster preceding heart rate (p = 0.006) and AF recurrence (p<0.001). Ventricular irregularity did not relate to symptoms (p = NS). Thus, a 25% increase in symptoms requires an increased AF duration of 4 h 5 mins, a mean sinus rate increase of 8 bpm preceding the PAF episode onset or a mean reduction in ventricular cycle length during AF of 63 ms. There was no circadian variation in PAF onsets for asymptomatic episodes. However, symptomatic episodes showed a significant increase in early recurrence AF diurnally with significant increase in sudden onsets nocturnally (fig).
Conclusions: There is significant circadian variability in AF cycle length, PAC initiating cycle length, AF ventricular rate and AF onset mechanisms in PAF. Furthermore, longer episodes, faster ventricular rate during AF, shorter PAC coupling intervals and shorter AF cycle length increase the likelihood of PAF being symptomatic.
electrophysiological characteristics; symptoms; paroxysmal AF
226 ALL-CAUSE AND CARDIOVASCULAR MORTALITY RELATED TO LONG-TERM RATE OR RHYTHM CONTROL STRATEGIES IN PATIENTS UNDERGOING SEDATION DC CARDIOVERSION FOR ATRIAL FIBRILLATION
A. Arya, J. Silberbauer, J. Vrahimides, G. Bordoli, J. Large, G. Lloyd, N. Patel, A. Sulke. Eastbourne DGH, Eastbourne, UK
Background: Debate over the benefits of rhythm versus rate control continues since the publication of studies showing equivocal outcomes between the two strategies. The purpose of this study was to assess the difference in mortality and morbidity between patients who achieved sinus rhythm following direct current cardioversion (DCCV) and those who relapsed into persistent AF, in a typical population of patients undergoing sedation cardioversion.
Methods: 770 patients, mean age 71.2 (10.3) years, who underwent 1013 sedation-cardioversions for atrial tachyarrhythmias were examined for all-cause and cardiovascular (CV) mortality with regard to rhythm status (sinus rhythm or persistent AF) at final follow-up. Clinical, echocardiographic parameters and safety and efficacy of the procedure were assessed.
Results: During mean follow-up of 36.3 (27.1) months (m), 56 deaths occurred (7.2%) in the AF group and 53 deaths (6.9%) in those who maintained sinus rhythm post-DCCV. There was no significant difference in all-cause or cardiovascular mortality between patients who maintained SR and those who did not, p = 0.11 and p = 0.60. Mean all-cause survival (SE) was 88.6 (2.2) m and mean cardiovascular survival was 101.8 (0.3) m in the AF group and 84.7 (2.9) m, 103.7 (1.5) m for those in SR (p = NS). However, age less than 75 years, p = 0.002 and use of sotalol and/or amiodarone, p = 0.007 were associated with improved all-cause survival. There were no independent predictors of all-cause mortality. Left ventricular function was the only independent predictor of cardiovascular mortality, p = 0.001, OR 0.8 (0.81–0.95).
Conclusions: Rhythm status post-DCCV does not influence long-term all-cause or cardiovascular mortality. Until sinus rhythm can be maintained effectively, DCCV can only be recommended for symptomatic patients.
atrial fibrillation; direct current cardioversion; mortality
227 “MINVPACE”: A STUDY COMPARING MINIMAL VENTRICULAR PACING AND PREVENTIVE ATRIAL FIBRILLATION ALGORITHMS IN THE TREATMENT OF PAF
A. Arya, R. Veasey, J. Silberbauer, C. Edwards, G. Lloyd, N. Patel, A. Sulke. Eastbourne DGH, Eastbourne, UK
Background: The beneficial effects of atrial pacing on paroxysmal atrial fibrillation (PAF) may be negated by increased ventricular pacing. This was a prospective randomised study evaluating the effect of pacing algorithms that minimise ventricular pacing (MVP) with and without anti-AF algorithms, on AF burden (AFB) in patients with PAF.
Methods: Using a single blind three-way cross-over design, patients with AF burden 1–70% with or without intermittent high grade AV block (AVB), implanted with pacemakers with MVP capability were enrolled. Three devices were assessed: Ela Symphony, Vitatron T70 and Medtronic Enrhythm. Patients were randomised to MVP with or without preventive AF algorithms or DDDR (AV delay (AVD) 150 ms) for 2 months per phase. The primary outcome measures were AFB and AF episodes/day. Secondary outcome measures examined the effect of ventricular and atrial pacing on AF burden.
Results: Sixty five patients were enrolled, of these, 32 (mean age 74.5 (7.8), 62.5% males) had an AF burden of 1–70% during the induction phase and completed all phases. Pacing indications were SSS in 82% and intermittent AVB in 18% of patients. There was no significant difference in AFB or AF episodes/day between the control phase DDDR, 14.0 (17.7)% 2.3 (2.6), and MVP, 14.7 (17.7)% 2.9 (5.0), or MVP + AF algorithms, 13.1 (17.5)% 4.3 (8.2), p = 0.85 and 0.84. Ventricular pacing was significantly higher during the DDDR (AVD150) phase, 82 (21)%, than in MVP 16 (27)% and MVP+algorithms 25 (33)%, p<0.001. Atrial pacing was greater during MVP+algorithms, 70 (25)% versus 57 (27)% in DDDR and 45 (27)% in MVP alone, p = 0.004. There was no significant correlation between V pacing and AF burden, p = 0.88.
Conclusion: Minimal ventricular pacing algorithms are highly effective in reducing ventricular pacing but do not reduce AFB in the short term. No additional benefit or adverse outcome was found with preventative anti-AF algorithms in combination with minimal ventricular pacing algorithms.
paroxysmal atrial fibrillation; ventricular pacing; algorithms
228 DELAYS TO PERMANENT PACEMAKER IMPLANTATION: AN EXPLANATION FOR LOW IMPLANTATION RATES IN THE UNITED KINGDOM?
M. Cunnington, C. Plummer, A. McDiarmid, J. McComb. Freeman Hospital, Newcastle upon Tyne, UK
Introduction: Permanent pacemaker (PPM) implantation rates in the UK are lower than in the US and many comparable European countries, the reasons for which are unclear. To investigate reasons for the low PPM implantation rate in the UK we examined the “patient journey”: how patients presented, were investigated and referred, from symptom onset to implantation.
Abstract 228
Methods: 120 consecutive patients undergoing PPM implantation at a single centre between 1/6/06 and 30/8/06 were studied. 16 receiving PPM for rate control in atrial fibrillation (AF) (without bradycardia indications) as part of an “ablate and pace” strategy and 9 receiving biventricular devices for cardiac resynchronisation were excluded. All hospital records (from referring and implanting centres) of the 95 included patients were reviewed. Data relating to symptom onset, documented pacing indication (defined by ACC/AHA 2002 guidelines), referral date and PPM implantation were recorded.
Results: See table. 48 patients (51%) had an emergency PPM: median delay from symptoms to PPM 14 days (range 0–13321). 47 had an elective PPM: median delay from symptoms to PPM 249 days (33–7505). 22/47 (47%) elective patients had prior hospitalisation with bradycardia-related symptoms and 25/47 (53%) had syncope. Delays were due to a variety of factors, and included failure to recognise PPM indications, unnecessary investigations, delays in sending letters and problems with the elective PPM waiting list. The longest delays were due to failure to recognise PPM indications. Overall, 26/95 (27%) had a documented Class I or IIA pacing indication previously overlooked. These included complete heart block (CHB) (n = 2); Mobitz II (3); bi/trifascicular block with syncope (7); sinus node disease (5); AF with pauses (7); carotid sinus hypersensitivity (2). Patients with CHB were more often paced as an emergency than those with other causes (median time from symptom to PPM 47 days (0–13321) vs 143 days (1–7505)).
Conclusions: There are significant delays to PPM implantation in the UK, longer in those treated electively than those managed as emergencies. The longest delays were due to failure to recognise PPM indications. Failure by hospital doctors to recognise pacing indications was common (27%), and by inference, other patients will have had a pacing indication overlooked and still not detected. This may contribute to the low implantation rate in the UK. Further education is required regarding pacing indications.
pacemaker; implantation; delays
229 RADIATION EXPOSURE AND PROCEDURAL DURATION: IMPLICATIONS FOR TRANSRADIAL AND TRANSFEMORAL CORONARY ANGIOGRAPHY
T. Lo, E. Fountzopoulos, B. Freestone, M. Gunning, J. Nolan. University Hospital of North Staffordshire, Stoke-on-Trent, UK
Introduction: Some studies suggest that the use of the radial access site is associated with increased radiation exposure and an extended procedure duration. The majority of these studies have poorly controlled variables, and the observed differences in radiation exposure can be accounted for by variation in operator experience, angiographic view selection and radiation protection protocol. A significant increase in transradial procedural duration would slow down laboratory throughput with implications for resource planning. The primary aim of this study was to systematically evaluate variation in radiation exposure to patients and operators during elective coronary angiography (CA) performed by an experienced femoral and radial operator, utilising a standardised approach and radiation protection protocol. The secondary aim was to evaluate access site specific components of procedural duration.
Methods: Patients undergoing first time elective CA performed by MG (femoral route) and by JN (radial route) were included prospectively. A standardised sequence of views of the coronary arterial system and left ventricle were performed for each procedure. Both operators applied optimised radiation protection methods and wore an additional electronic personal dosimeter (EPD) outside the protective lead apron just under the left clavicle. Operator and patient radiation exposure values were obtained from the EPD and the dose area product (DAP) reading from the x ray tube diamentor respectively at the end of each procedure. Procedural duration and time to ambulation were recorded.
Results: A total of 50 consecutive patients were studied. Baseline patient characteristics were similar for both groups, apart from a significantly increase in age in the radial group. Mean patient age, height (m), weight (kg) and BMI for the radial and the femoral group was 69.8 (8.1) and 61.4 (11.3), 1.66 (0.08) and 1.67 (0.1), 79.4 (14.0) and 86.5 (17.8), and 28.7 (4.7) and 30.9 (5.8) respectively. Although the procedural duration (min) was longer with the radial procedures than the femoral procedures (12.6 (2.8) and 7.2 (2.1), p<0.005), the time to ambulation (min) was significantly shorter with the radial procedures (6.16 (1.1) vs 257.2 (3.5), p<0.0001). Mean patient DAP (Gycm2) for the radial and the femoral procedures was 21.7 (6.9) and 22.4 (7.8) respectively, p = 0.69, and mean operator radiation exposure dose (µSv) was 6.5 (5.3) and 5.9 (5.6) respectively, p = 0.49.
Conclusion: This study demonstrates that transradial diagnostic CA performed by experienced operators employing meticulous radiation protection is not associated with an increase in radiation exposure to the patient or the operator. A small increase in radial procedure duration is offset by a large reduction in time to ambulation, implying an overall reduction in procedural workload.
radiation exposure; transradial coronary angiography; transfemoral coronary angiography
230 ARE CARDIOLOGISTS IMMORTAL?
Y. Yan1, K. C. Patel2, K. V. Patel3, P. Judge3, J. Patel3, S. Johal3, P. Do3. 1Sandwell Hospital, Birmingham, UK; 2Sandwell Hospital and University of Birmingham, Birmingham, UK; 3University of Birmingham, Birmingham, UK
Does medical discipline affect mortality? One is often led to believe that cardiac surgeons are immortal but what about the cardiologist. Are they immortal and should they work for longer, delaying retirement age as has been suggested recently? To look at this, we assessed the age and disease distribution of mortality of medical practitioners by undertaking a 7 year in-depth review of all reported obituaries of medical practitioners in the BMJ. 3342 obituaries between January 1997 and December 2004. The majority were obituaries of male doctors. Doctors who qualified in the developed world appeared to live longer (mean age of death of 78 (14) years) than those who qualified in Asia (mean age of death of 70 (16) years). Doctors from non-white-European ethnic groups did not live much beyond the current UK retirement age of 60 years (p = 0.03). There was no significant difference in longevity between doctors working the doctors in the primary care sector and those in the secondary care sector (p = 0.08). 12.5% of doctors died between the ages of 60 and 70 years and of these, nearly half died between the ages of 61 and 65 years. Cardiologists lived to the age of 73.4 (13) years. This was a shorter lifespan than dermatologists (76.5 (13) years) but longer than gastroenterologists (70 (16) years) and emergency physicians (57 (16) years). So what does this tell us? Perhaps the more sedentary a discipline, the longer one’s lifespan? It would be interesting to see if interventionists and non-interventionists differ in life expectancy! Retirement at ages of 65 years or above would disadvantage nearly 1 in 6 medical practitioners. Those likely to be most disadvantaged by a mandatory rise in any retirement age, in terms of reaping the reward of pension contributions, are those of a non white-European ethnicity. So, cardiologists are almost immortal, but still need to retire gracefully as is currently permitted!
mortality; cardiologist; retirement
231 A SIMPLE RISK MODEL FOR PREDICTING 30-DAY MORTALITY IN PATIENTS PRESENTING WITH ACUTE CORONARY SYNDROME
R. Das, C. Gale, N. Kilcullen, C. Morrell, J. Barth, A. Hall. BHF Heart Research Centre, Leeds, UK
Introduction: Patients with acute coronary syndromes (ACS) experience a wide range of cardiovascular outcomes. There is heterogeneity in their clinical presentation and investigations which makes clinical decision making difficult. Accurate risk assessment has been proposed to help identify groups of patients where more aggressive anti-thrombotic and interventional strategies should be targeted. We sought to develop a risk prediction model using admission characteristics to predict 30-day mortality in a contemporary UK population.
Methods: The study was designed as a prospective observational registry of patients admitted with ACS to 11 adjacent UK hospitals. 2499 patients with acute coronary syndrome (ACS) were identified during a six-month window period (28 April to 28 October 2003). Demographic, clinical and treatment variables were collected on all patients and their mortality status was monitored through the Office of National Statistics.
Results: A three variable model was developed based on age, heart rate and systolic blood pressure. This produced an individual probability of death by 30 days (P30 = 1/(1+exp(−L30) and L30 = −5.506 + (0.070 × age) +(0.006 × heart rate) −(0.016 × systolic blood pressure). The areas under the receiver operating characteristic curves for the three-factor model were 0.76 (95% CI 0.72 to 0.79) and 0.75 (95% CI 0.71 to 0.79) for the reference and test cohorts, respectively.
Conclusions: This risk model uses variables available when a patient first arrives to hospital that allows accurate prediction of 30-day mortality to aid risk stratification.
acute coronary syndrome; risk assessment; mortality
232 LOWER MORTALITY IN ACUTE MYOCARDIAL INFARCTION WHERE THROMBOLYSIS IS ADMINISTERED IN THE COMMUNITY
Y. Tan, C. Mavroudis, T. Khan, R. Butler, J. Nolan, M. Gunning. University Hospital of North Staffordshire, Stoke-on-Trent, UK
Introduction: Several studies report that pre-hospital thrombolysis (PHT) results in better short- and long-term outcome than in-hospital thrombolysis (IHT), in patients who presented with acute ST elevation myocardial infarction (AMI). The benefit of thrombolysis is directly related to expedience of administration and hence the rapid diagnosis and treatment in the pre-hospital setting is desirable. The shortcomings of IHT in achieving reperfusion in all cases may be related to delay between symptoms and administration. As part of an ongoing audit of treatment of AMI we evaluated outcomes in patients who received PHT and IHT.
Methods: Case notes of 213 patients with a diagnosis of Acute ST elevation myocardial infarction (AMI) treated with thrombolysis between year 2004–5 were reviewed as part of our ongoing audit of treatment and outcomes in MI.
Results: The median age was 64 years (range 33 to 95) and 168/213 (79%) were male. 90/213 (42%) patients received pre-hospital treatment in the ambulance and 110/213 (52%) patients were treated on admission to hospital. In 13/213 (6%) the location of thrombolysis was not specified. 179/213 (84%) received Reteplase alone, and 34/213 (16%) received Streptokinase. Only 31/213 (15%) patients underwent emergency coronary intervention within the first 6 hours. A total of 132/213 (62%) patients were ultimately investigated by angiography. All patients received aspirin but only 25/213 (12%) of patients were front-loaded with clopidogrel. Overall mortality on this index presentation was 27/213 (13%) and 2/213 (1%) subsequently died at 3 and 8 months following discharge respectively. Of those patients who died, only 7/29 (24%) received PHT while 22/29 (76%) received IHT. Thus the mortality rate for PHT is 7/90 (8%) and for IHT is 22/110 (20%). Of those who succumbed 11/29 (38%) were over the age of 80 years. In 14/29 (48%) there was complete failure of ECG resolution by 90 min post-thrombolysis; in 10/29 (34%) partial resolution was seen. Complete ECG resolution was only observed in one of the patients who died. A symptom-needle time of >90 min was recorded in 22/29 (76%) (median 2.5 h, range 1–24.5). Of those deceased patients who received in-hospital thrombolysis, only 10/22 (45%) had a door to needle time of <30 min. Only 2/29 of these patients underwent emergency PCI and 4/29 had intervention later on during the admission.
Conclusions: In our cohort a greater proportion of those who died following AMI had thrombolysis administration delayed until arrival in hospital. In this era of evolving treatment options for myocardial infarction, thrombolysis remains the front line choice in many centres in the UK. Our data suggest that ambulance crew delivered thrombolysis is preferable to any delay until admission. Any future comparative assessment of primary PCI should use pre-hospital thrombolysis as a comparator.
prehospital thrombolysis; in-hospital thrombolysis; acute ST elevation myocardial infarction
233 HYPERGLYCAEMIA, IN RELATION TO GENDER, AND MORTALITY AFTER ACUTE CORONARY SYNDROME
R. Cubbon1, A. Rajwani1, P. Grant1, S. Wheatcroft1, J. Barth2, M. Kearney1, A. Hall1. 1The University of Leeds, Leeds, UK; 2Leeds General Infirmary, Leeds, UK
Background: Diabetes mellitus (DM) and hyperglycaemia predict outcome after acute coronary syndrome (ACS). Recent work has suggested that women with DM have greater baseline cardiovascular risk and poorer outcome after ACS than men. The interaction between gender and abnormal glucose homeostasis in patients without diabetes is unexplored; we aimed to assess this relationship.
Methods: Retrospective analysis of data from the EMMACE-II (Evaluation of Methods and Management of Acute Coronary Events) prospective cohort study. Analysis included 1575 patients with confirmed ACS and no previous diagnosis of diabetes mellitus in 11 UK hospitals. Cox proportional hazards multivariable analysis was performed to assess the value of clinical variables, including hyperglycaemia (using random plasma glucose assessment) and gender, in predicting two year all-cause mortality.
Results: Gender and hyperglycaemia interacted in predicting mortality (p<0.001). In men mortality risk increased more steeply with incremental levels of glycemia than in women (fig) reaching significance at random glucose concentrations >11.1 mmol/l (hazard ratio 2.19, 95% CI 1.2 to 4.0). In both gender groups increasing glycemia predicted mortality at levels currently not recommended for acute therapeutic intervention (7.8–11.1 mmol/l).
Conclusions: In patients not known to have diabetes, hyperglycaemia is a concentration dependent predictor of long-term mortality after ACS; this effect is stronger in men than women. Ongoing research into these complex interactions is warranted; furthermore, post-ACS glycometabolic disturbance requires more effective management strategies in both men and women.
Acknowledgements: Dr Cubbon is supported by a British Heart Foundation Clinical PhD Studentship.
acute coronary syndrome; hyperglycaemia; gender
234 TEMPORAL TRENDS IN MORTALITY OF PATIENTS WITH DIABETES MELLITUS SUFFERING ACUTE MYOCARDIAL INFARCTION: A COMPARISON OF OVER 3000 PATIENTS BETWEEN 1995 AND 2003
R. Cubbon1, A. Rajwani1, S. Wheatcroft1, P. Grant1, C. Gale2, J. Barth2, R. Sapsford3, M. Kearney1, A. Hall1. 1The University of Leeds, Leeds, UK; 2Leeds General Infirmary, Leeds, UK; 3St James’s University Hospital, Leeds, UK
Background: Over the last decade advances in treatment for patients sustaining an acute myocardial infarction (AMI) have reduced mortality rates. We aimed to assess whether patients with diabetes mellitus (DM) have derived similar benefits as patients without DM.
Abstract 234 Mortality and survival data
Methods: Retrospective analysis of data from the EMMACE I and II (Evaluation of Methods and Management of Acute Coronary Events) prospective cohort studies. We compared baseline characteristics, management and survival of patients with and without DM (pre- or peri-admission diagnosis) who sustained an AMI (defined using WHO criteria) in 1995 (n = 1762) with a second group of patients who sustained an AMI in 2003 (n = 1642). All patients were followed up for 18 months or until death.
Results: Between 1995 and 2003 the prevalence of DM in AMI patients increased from 12.5 to 16.6% (p<0.001); these are lower rates than would be expected in such high-risk cohorts. Involvement of cardiologists, provision of secondary prevention agents and early revascularisation rates improved significantly in both groups. However, in 2003 a trend (p = 0.078) toward lower rates of early revascularisation was noted in patients with diabetes, compared to those without. Thirty-day mortality improved significantly (table; fig) in patients with and without DM (40% (p = 0.006) and 30% (p<0.001) relative reductions respectively). Despite this, there was no significant change in mortality at 18 months in patients with DM when comparing 1995 and 2003 (absolute mortality 38.0% vs 36.4% p = 0.71).
Conclusions: Screening for DM in the post-AMI setting appears suboptimal. Provision of evidence based care has improved equitably in patients with and without DM. However, whilst early post-AMI mortality has fallen in all patients, these improvements were only maintained in the longer term in those without DM; more effective treatment strategies are required for patients with diabetes post-AMI.
acute myocardial infarction; diabetes mellitus; temporal trends
235 RISK FACTORS IN PATIENTS WITH AN OUT-OF-HOSPITAL CARDIAC ARREST
A. Hamilton1, M. Moore1, K. Cairns2, A. Adgey1, F. Kee3. 1Regional Medical Cardiology Centre, Royal Victoria Hospital, Belfast, UK; 2Department of Applied Mathematics, Queen’s University of Belfast, Belfast, UK; 3Department of Epidemiology and Public Health, Queen’s University of Belfast, Belfast, UK
Objective: To determine the risk factors leading to death from out-of-hospital cardiac arrest (OHCA).
Methods: The Emergency Medical Service patient report forms from North and West Belfast were examined from 8/6/2005 to 28/3/2006 for any OHCA death as per Utstein criteria. The general practitioner (GP) records and the postmortem result were obtained.
Results: There were 131 cases of OHCA; 76 were male (58%), mean age 68 years. At the time of death 51 (39%) lived alone and 112 (85%) had an OHCA at home. The mean height was 160 cm and mean body weight 74.5 kg. The mean blood pressure when last assessed was 135/78 mmHg, with mean total cholesterol of 5.0 mmol/l. The GP register recorded a history of smoking in 72 (55%), hypertension in 63 (48%), hypercholesterolaemia in 42 (32%), and diabetes mellitus in 24 (18%) patients. The use of ACE inhibitors occurred in 61 (47%), aspirin in 56 (43%), statins in 54 (41%) and beta-blockers in 46 (35%) patients. A history of ischaemic heart disease was present in 48 (37%) patients and 31 (24%) had a previous documented myocardial infarct. The median time from the last GP attendance to death was 103 days (interquartile range 21–296 days). In only 6 (5%) cases was chest pain the reason for this attendance. The median time from the last hospital attendance to death was 154 days (interquartile range 48–665 days). The investigations performed included: 22 (17%) patients who had an exercise stress test, 11 (8%) myocardial perfusion scans and 28 (21%) patients with a previous coronary angiogram. A postmortem occurred in 42 cases. At postmortem there were 27 (64%) with ⩾moderate coronary atheroma in three coronary arteries. This was observed by the pathologist as >50% stenosis in a coronary artery. Left ventricular hypertrophy occurred in 26 (62%) cases.
Conclusion: OHCA remains difficult to predict with few patients presenting with prior chest pain to the GP. The high incidence of OHCA in individuals living alone at home will constrain improvements in survival.
cardiac arrest; risk factor; postmortem
236 RAPID ACCESS CHEST PAIN CLINIC REFERRALS FOR ANGIOGRAPHY: ROOM FOR IMPROVEMENT?
J. Tough, A. Thornley, A. Turley, B. Kunadian, R. Morley, M. Stewart, M. de Belder. The James Cook University Hospital, Middlesbrough, UK
Background: The Rapid Access Chest Pain Clinic (RACPC) is often the first point of contact with secondary care for patients with possible cardiac chest pain. Clear standards exist for times from referral to clinic attendance but there are no standards for follow on investigation and treatment. Many patients with positive investigations carried out in the RACPC may still have delays in undergoing angiography and revascularisation.
Abstract 236
Aims: To audit time spent awaiting angiography following both strongly positive (group 1: >2 mm ST depression or symptoms at less than 6 min) or positive/borderline positive (group 2: <2 mm ST depression or symptoms >6 min) exercise tolerance tests (ETT) and subsequently implement changes to limit these waits.
Results: Over the course of the audit 1479 patients were referred to the RACPC and all were seen within 14 days. Of these 116 had either a strongly positive (50) or positive/borderline ETT (66). The median waiting time for angiography for group 1 patients was 21.5 days ranging from 0–67 days. For group 2 patients with a positive ETT the wait was 62 days ranging from 1–174 days. These results demonstrated inequalities in access to angiography for patients undergoing ETT in our RACPC. We therefore set new standards for angiography following attendance at RACPC: angiography with a view to immediate angioplasty within 4 weeks for group 1 patients and angiography within 4 weeks for group 2 patients. Same-day booking of dedicated angiography slots was implemented. Pre-admission and consent protocols involving specialist nurses and day unit staff were also developed. Following the implementation of these system changes further assessment of our waiting times revealed a significant improvement in the median time from RACPC to angiography for both group 1 (6.5 days, range 0–19 days) and group 2 (14 days, range 0–63 days). The table shows waiting time by group at baseline and following implementation of the changes described (period 2), p<0.001.
Conclusions: Audit of waiting times in the setting of a RACPC can lead to significant improvements in the service offered to patients. Change in protocols including the dedication of specific slots on weekly angiography lists to RACPC patients has led to a significant decrease in median waiting times. To deliver optimum patient care it is important to set standards for both RACPC to angiography and RACPC to revascularisation waiting times.
rapid access chest pain clinic; angiography; waiting times
237 AGE-RELATED CHANGES IN CAROTID ARTERY LUMEN AND WALL VOLUME IN A POPULATION FREE OF CARDIAC RISK FACTORS
N. Keenan, D. Pennell. Royal Brompton Hospital, London, UK
Introduction: The aim of this study was to study the carotid artery wall volume as a function of age in subjects who were free from cardiovascular risk factors. MR is an excellent modality for imaging the arterial wall. It has mainly been used in late disease. It is sensitive in early disease however, and can detect subtle vessel wall thickening, such as occurs with aging.
Abstract 237
Methods: We recruited 89 healthy controls who were free of all vascular risk factors. There were 40 male subjects, with an average 18 subjects per decade between 20 to 70 years. We performed a CMR study of their carotid arteries using a 1.5T Siemens Sonata scanner and bilateral four channel surface coils. We acquired a stack of high-resolution fast spin echo images centred on the carotid bifurcation and perpendicular to the carotid artery bilaterally. Slice thickness was 2 mm, and we acquired 20 contiguous slices for each side. Using dedicated software we traced the internal and external carotid artery surfaces for each slice and hence measured the luminal area and the wall area for each slice. Adding together the 20 slices, we produced a 3D model of the carotid bifurcation, and measured the lumen volume, wall volume and total vessel volume for our standardised 4 cm length. We divided the total wall volume by the total vessel volume to calculated the wall/outer wall (W/OW) index enabling comparison between different subjects with varying sizes of carotid artery.
Results: Male and female results were analysed separately (table). In males, there was a strong and significant correlation between age and the volume of the carotid artery wall (r = 0.76), and this was also reflected in the W/OW ratio. The same was true for the females, with a weaker but still significant correlation coefficient (r = 0.52). Luminal volume was only weakly correlated with age in males (r = 0.35) and not significantly in females. The mean W/OW ratio for males was 32.6% and for females 31.7% (no significant difference).
Conclusion: We have demonstrated that in a normal population free from conventional vascular risk factors, there is a significant increase in carotid artery wall thickness with aging from 20 to 70 years. The more pronounced change in males is probably related to the protective effect of oestrogen on the female vasculature until the menopause. This provides further evidence for the Glagov phenomenon of external remodelling of the artery to accommodate atherosclerotic burden which prevents encroachment of the lumen, at least in the early stages. Hence the wall volume substantially increased with age in both sexes, without a corresponding decrease in the luminal volume. These results with a modest sample size show the power of carotid artery wall volume as measured by MR as a tool in vascular medicine. Reference normal data by age may enable MR carotid wall volume to become a risk stratification tool in at-risk populations.
cardiovascular magnetic resonance; atherosclerosis; carotid artery
238 STABILISATION OF CORONARY STENTS USING RAPID RIGHT VENTRICULAR PACING
D. O’Brien, W. Smith, R. Henderson. Trent Cardiac Centre, Nottingham City Hospital, Nottingham, UK
Aims: Excessive movement of coronary stents within the artery can make precise stent placement difficult. Inaccurate stent placement may result in “geographic miss” of the target lesion or may cover a previously uninvolved branch vessel. This study assessed the use of rapid right ventricular pacing to reduce stent motion to improve the accuracy of placement.
Abstract 238
Methods and Results: During percutaneous coronary intervention, if excessive stent movement prevented accurate stent placement, rapid right ventricular pacing was performed to reduce stent motion within the coronary artery during both stent positioning and deployment. Post-procedural angiograms were analysed by two independent operators to measure stent movement during sinus rhythm and during rapid right ventricular pacing. Rapid right ventricular pacing to stabilise the coronary stent and facilitate accurate stent placement was carried out in 10 patients, including 8 with stable angina, 1 with unstable angina, and 1 with acute myocardial infarction. Examples of stent motion in sinus rhythm and during rapid right ventricular pacing are shown in figure 1. The results of the QCA measurements for individual patients during sinus rhythm and rapid right ventricular pacing are shown in table 1 and figure 2. In all cases stent motion was reduced sufficiently by rapid right ventricular pacing to allow safe stent deployment. Mean stent excursion for all patients in sinus rhythm was 2.9 mm (SD 1.6) and during rapid right ventricular pacing this was reduced to 0.8 mm (SD 0.6) (p<0.001). Movement assessed by individual operators ranged from 0.7 to 6.5 mm during sinus rhythm and from 0.1 to 2.4 mm during right ventricular pacing. Reproducibility of measurements of stent movement between two observers was good as assessed using the method described by Bland and Altman (fig 3). No coronary, access site or pacing related complications were observed.
Discussion: Our review of the literature has identified no reliable method of stabilising intra-coronary stents. Rapid right ventricular pacing has recently been used to stabilise devices in the heart during non-coronary procedures, such as percutaneous valve interventions, but we are not aware of previous reports suggesting the use of this technique for the placement of coronary stents.
Conclusion: Rapid right ventricular pacing is an effective and safe method to reduce stent movement and facilitate accurate stent deployment. This simple technique can be easily applied in any interventional cardiac catheterisation laboratory without the need for additional training or equipment.
stent; coronary; pacing
239 SIMULTANEOUS KISSING STENTS (SHOTGUN STENTS) TO TREAT LEFT MAIN BIFURCATION STENOSIS
A. Siotia, A. Morton, J. Gunn. Sheffield Teaching Hospitals NHS Trust, Sheffield, UK
Background: There is no single, widely accepted interventional technique for treating left main stem (LMS) bifurcation stenosis. We performed a prospective, safety and feasibility study of treating such lesions with simultaneous kissing (“shotgun”) stent technique.
Methods: Eighty five consecutive patients with LMS bifurcation stenosis were treated using a simultaneous kissing stent technique. 6-month follow-up data were available for 78 patients and these were used in subsequent analysis. Drug-eluting stents (Taxus, Boston Scientific, Natick, MA) were used when technically feasible (75/78 cases). Balloon counterpulsation was used in 13 (17%) patients and 45 (58%) received abciximab. 21 (27%) patients were deemed not fit to undergo CABG and 7 (9%) patients were in critical state at the time of presentation. All patients were followed up clinically.
Results: Mean age was 66 (45–88) years, 58 (74%) were male, 56 (72%) were elective, 16 (20%) urgent and 6 (8%) emergency. In addition to LMS, an average of 1.9 vessels was diseased per patient and an average of 1.8 was treated. The procedure was technically successful in all cases. There were 3 (4%) in-hospital deaths all of which occurred in critically ill patients undergoing emergency procedures. At a mean follow-up of 14 (6) months, there were 4 (5%) deaths. These patients died at 1, 4, 7 and 10 months post procedure. 4 (5%) patients underwent repeat PCI for clinical restenosis. The remaining 67 (86%) patients remained well without any major adverse cardiac events. NYHA angina class was reduced from a mean of 2.7 pre-procedure to 1.4 at the most recent follow-up.
Conclusion: The simultaneous kissing stent technique for treating bifurcation disease of the LMS is safe and feasible. Medium term results are good. A randomised control trial with CABG should be considered.
percutaneous coronary intervention; left main stem; simultaneous kissing stents
240 TRANSCATHETER CLOSURE OF PARAVALVAR PROSTHETIC VALVE LEAKS USING THE AMPLATZER OCCLUDERS
J. DeGiovanni1, P. Ludman2, D. Hildick-Smith3, I. Malik4, S. Khogali5, M. Been6. 1Birmingham Children’s Hospital, Birmingham, UK; 2University Hospital Birmingham, Birmingham, UK; 3Royal Sussex County Hospital, Brighton, UK; 4St Mary’s Hospital, London, UK; 5Heart and Lung Centre, Wolverhampton, UK; 6Walsgrave Hospital, Coventry, UK
Introduction: Prosthetic valves have revolutionised the treatment of unreparable diseased cardiac valves. Mechanical valves are robust but not without problems. Around 2% develop paravalvar leaks spontaneously or following infection. Many patients would have had multiple previous operations and transcatheter intervention, if possible, is preferred but there are no devices specifically designed for this purpose. We attempted to close paravalvar leaks in symptomatic patients in 6 tertiary centres in the UK using Amplatzer occluders and we report our experience and results
Methods and Results: Between January 2004 and November 2006, 10 patients with mechanical prosthetic valves who had a paravalvar leak were considered for transcatheter closure using an Amplatzer occluder. These included 3 females and 7 males with ages ranging from 11 to 72 years. Four had aortic and 6 had mitral prosthesis; none had mutiple valves. The indication for closure was heart failure in 9 and haemolysis in 1. The defect was crossed in 9 cases, 8 of whom had a device implanted; in 1 patient, ischaemic changes occurred during balloon sizing and the procedure was terminated. Of the 8 devices implanted (3 aortic and 5 mitral), 7 were muscular Amplatzer occluders and 1 was a patent duct occluded. The aortic devices were placed via the radial (1), brachial (1) or femoral (1) arterial approach. The mitrals were placed through the femoral vein using trans-septal approach. All procedures were carried out under general anaethesia and with trans-oesophageal echocardiography. In 1 patient with an aortic leak, a PDA occluder was placed but this embolised in the left ventricle; the device was retrieved and replaced by a muscular device. The two patients who did not have a device went for surgery; one had a mitral valve replacement successfully but the other had an attempt at closure of the aortic leak but this led to gross ischaemia and the repair was reversed.
Conclusion: Paravalvar prosthetic leaks can cause symptoms and morbidity for which intervention is often required. Transcatheter repair is attractive and feasible for single prosthetic valves but there are no customised devices for this purpose. The Amplatzer Occluders are the best option at present but their use is “off label” and they are not ideal as small residual leaks remain in many patients. Apart from the devices, the delivery systems may need to be customised for these procedures. This technique adds another interventional procedure for structural heart disease and has become possible by gaining experience through other procedures for congenital and non-coronary heart disease
paravalvar prosthetic leaks; transcatheter repair; amplatzer occluders
241 ASSOCIATION OF PLAQUE THICKNESS WITH ENDOTHELIAL SHEAR STRESS IN THE LEFT MAIN CORONARY ARTERY BIFURCATION: IN VIVO STUDY USING 3D RECONSTRUCTION AND COMPUTATIONAL FLUID DYNAMICS
M. Papafaklis1, C. Bourantas2, P. Theodorakis3, C. Katsouras4, D. Fotiadis5, L. Michalis4. 1Michaelideion Cardiac Centre, University of Ioannina, Ioannina, Greece; 2Michaelideion Cardiac Center, University of Ioannina, Ioannina, Greece; 3Department of Materials Science and Engineering, University of Ioannina, Ioannina, Greece; 4Department of Cardiology, Medical School, University of Ioannina, Ioannina, Greece; 5Department of Computer Science, University of Ioannina, Ioannina, Greece
Introduction: Atherosclerotic plaque progression and thickness has been reported to be inversely correlated to endothelial shear stress (ESS), but no in vivo data exist on the role of ESS in the left main coronary artery bifurcation which is commonly diseased. Our aim was to investigate the relationship of plaque thickness (PT) with ESS in the left main coronary artery bifurcation using real three-dimensional (3D) reconstructed models.
Methods: Biplane angiography and intravascular ultrasound examination was performed in the left main (LM)–left anterior descending (LAD) and LM–circumflex (Cx) coronary arteries in five patients undergoing diagnostic catheterisation. The lumen and the outer vessel wall (media-adventitia border) of the coronary arteries were 3D reconstructed using a technique based on the fusion of angiographic and intravascular ultrasound data. Then, the LM-LAD and LM-Cx models were combined into a unified LM-LAD-Cx model, one for the lumen and one for the outer vessel wall for each patient. ESS was calculated by applying computational fluid dynamics to the 3D luminal LM-LAD-Cx model. PT in each LM coronary artery bifurcation was determined as the difference between the outer vessel wall and the lumen in 3D space. A linear mixed model controlling for patient-to-patient variation was used for estimating the relationship of PT with ESS.
Results: All five LM coronary arteries had no significant stenosis (mean diameter stenosis by quantitative coronary angiography: 24.9 (5.2)%). The mean cross-sectional plaque burden computed in the 3D models was 35.4 (5.9)% and the mean computed 3D plaque volume was 103.5 (44.1) mm3. The estimated intercept and slope for the relationship of PT with ESS were 0.89 mm (95% CI 0.44 to 1.35 mm, p = 0.01) and −0.19 mm/Pa (95% CI −0.25 to −0.14 mm/Pa, p<0.001) respectively.
Conclusions: PT is inversely related to ESS in the critical region of the left main coronary artery bifurcation.
intravascular ultrasound; angiography; shear stress
242 RADIAL ARTERY DIAMETER, ITS RESPONSE TO SUBLINGUAL GTN AND IMPLICATION FOR TRANSRADIAL CARDIAC CATHETERISATION
T. Lo, J. Nolan. University Hospital of North Staffordshire, Stoke-on-Trent, UK
Introduction: Cardiac catheterisation using the radial artery (RA) is associated with lower vascular complications and better patient comfort. This technique is, however, associated with a longer learning curve frequently related to difficulty in puncturing the RA. Detailed knowledge of RA diameter and its response to sublingual (S/L) GTN may help shorten part of the learning curve but such data are currently not available. This study aims to evaluate distal upper limb arterial diameter and response to S/L GTN.
Abstract 242 Table 1
Abstract 242 Table 2
Methods: Using a 10-MHz linear vascular transducer, ultrasound scan of both the right (R) and left (L) RA and ulnar artery (UA) at the wrist 1–4 cm proximal to both styloid processes were performed at rest and after 800 μg of S/L GTN. Blood pressure (BP) reading was recorded pre and post GTN. Patient characteristics including hand dominance, Allen’s test and wrist circumference (2 cm above the radial styloid process) were all recorded before the scan.
Results: Sixty patients were recruited. Baseline patient characteristics are shown in table 1. The diameters (mm) of the radial and ulnar arteries pre- and post-GTN are shown in table 2. Men had significantly bigger RA and UA than women. The RA was bigger than the UA in most men and women. The RRA was bigger than the LRA in 92% of women and 100% of men. GTN significantly increase the size of both the RA and UA. Mean % dilatation of the RRA, LRA, RUA and LUA in the women was 24.3 (7.9), 24.4 (9.1), 29.4 (11.8) and 32.7 (9.6) respectively, and was 15.6 (9.5), 18.3 (7.6), 18.3 (8.6) and 18 (6.8) respectively in men. There were no difference in BP pre and post S/L GTN and none of the patients experienced any hypotensive symptoms. Pre-GTN, only 36.7% and 13.3% of women had RRA bigger than 2.28 mm (external diameter of a 5F sheath) and 2.52 mm (external diameter of a 6F sheath), and 20% and 6.7% had a LRA bigger than a 5F and 6F sheath respectively. Post-GTN, these increased to 89.3% and 75% of RRA bigger than a 5F and 6F sheath, and 70.4% and 55.6% for LRA respectively. In men, 94.4% and 72.2% had RRA bigger than a 5F and 6F sheath respectively, and 78.9% and 52.6% for LRA respectively. Post-GTN, these increased to 100% and 88.2% of RRA bigger than a 5F and 6F sheath, and 93.3% and 87.5% for LRA respectively.
Conclusions: The RA is significantly smaller in women than men, with the majority of RA in women smaller than the external diameter of a 5F sheath prior to GTN. The RA is normally bigger than the UA and the RRA bigger than the LRA in both men and women. Sublingual GTN increases the size of the RA significantly and should make puncturing the RA easier, thereby shortening part of the learning curve associated with the transradial technique. Use of RRA with administration of GTN prior to all transradial cardiac procedures is the best policy.
radial artery diameter; GTN; transradial coronary procedures
243 THE RISK OF VENTRICULAR ARRHYTHMIA FOLLOWING ALCOHOL SEPTAL ABLATION FOR HYPERTROPHIC CARDIOMYOPATHY WITH SYMPTOMATIC LEFT VENTRICULAR OUTFLOW TRACT OBSTRUCTION
E. Smith, Z. Chen, A. Shetty, R. Ang, C. Knight. London Chest Hospital, London, UK
Background: Alcohol septal ablation (ASA) is a percutaneous alternative to surgical myomectomy for hypertrophic cardiomyopathy (HCM) patients with symptomatic left ventricular outflow tract (LVOT) obstruction refractory to medical therapy. However, myocardial fibrosis resulting from septal infarction may theoretically be a substrate for ventricular arrhythmias. This study investigated the incidence of ventricular arrhythmia following ASA.
Methods: Twenty five consecutive patients (15 male, mean age 55 (15) years) undergoing ASA at a single centre (September 2000–2005) were followed for a median of 47 (20–92) weeks. LVOT gradient was measured by echocardiography. Creatine kinase (CK) was measured 18–24 h post-ASA as a marker of infarct size. NYHA class was assessed pre procedure and at follow up. 24-h Holter monitoring was performed in 15 patients without an implantable cardioverter defibrillator (ICD), and by device interrogation in 5 patients with an ICD. (3 patients had an ICD in situ pre ASA, and 2 were implanted for primary prevention post ASA). Four patients had a permanent pacemaker in situ pre ASA. All subjects were established on beta blocker and/or calcium channel blocker therapy pre ASA. Three patients were on amiodarone. MACE included death, cerebrovascular accident, sustained ventricular arrhythmia, permanent pacing, or emergency cardiac surgery.
Results: Mean CK post ASA was 953 (484) mg/dl. LVOT gradient was significantly reduced and sustained at follow-up (fig). 72% of subjects were in NYHA class III or IV pre ASA, and 0% at follow-up. There were no deaths. Six patients (24%) required permanent pacemaker implantation (3 with pre-existing LBBB, 4 female). A single episode of asymptomatic non sustained (10 beats) broad complex tachycardia was recorded in 1 patient. There were no sustained ventricular arrhythmias. One patient developed persistent atrial fibrillation, and 1 had evidence of paroxysmal SVT. There were no further MACE episodes.
Conclusions: Alcohol septal ablation resulted in a sustained reduction of LVOT gradient, and significantly improved symptoms. Despite causing substantial myocardial necrosis, ASA did not lead to sustained ventricular arrhythmias. These data do not support the hypothesis that there is a high risk of malignant ventricular arrhythmias following ASA. The detection of lower risks of malignant arrhythmic complications in small proportions of ASA patients can only be established through multicentre registries, which should be a priority for centres performing this procedure.
alcohol septal ablation; hypertrophic cardiomyopathy; ventricular tachycardia
244 CORONARY COLLATERALS REMAIN RECRUITABLE FOLLOWING PERCUTANEOUS INTERVENTION
D. Perera, G. Kanaganayagam, M. Saha, R. Rashid, M. Marber, S. Redwood. St Thomas’ Hospital Campus, Kings College London, London, UK
Background: Rapid loss of collateral support has been reported following percutaneous coronary intervention (PCI), leaving the myocardium susceptible to subsequent infarction. However, well-developed collaterals have been found in normal hearts, suggesting that collaterals exist even in the absence of an ischaemic stimulus. We assessed the plasticity and determinants of collateral supply after PCI.
Methods: n = 60. Collateral flow index (CFI) was calculated as (Pw-Pv)/(Pa-Pv), by measurement of aortic, central venous and coronary wedge pressures (Pa, Pv, Pw). CFI was reassessed during transient balloon occlusion 5 min, 24 h and 6 months after PCI. We also evaluated the relation between collateral supply, lesion characteristics and circulating haemopoietic cells numbers, before and after successful PCI.
Results: CFI at baseline was 0.23 (0.10), with no change 5 min and one day later (0.21 (0.12), p = 0.62 and 0.22 (0.11), p = 0.96 respectively). At 6 months, CFI was 0.14 (0.07) or 63 (27)% of the baseline value (p<0.001). CFI was proportional to severity of the coronary lesion at baseline (r = 0.63, p<0.0001) but not 6-months after PCI (r = −0.04, p = 0.87). The number of circulating CD133+ and CD34+ cells were related to CFI 6-months following PCI (CD133: r = 0.59, p = 0.035 and CD34: r = 0.63, p = 0.037).
Conclusion: Coronary collateral flow remains undiminished for at least 24 h following PCI. Functional collateral support subsequently declines but does not regress completely.
collateral circulation; angioplasty; progenitor cells
245 COMPARISON BETWEEN PRESSURE DERIVED AND THERMODILUTION DERIVED FLOW RESERVE IN PATIENTS UNDERGOING PERCUTANEOUS CORONARY INTERVENTION
L. Blows, S. Perera, M. Behan, M. Marber, S. Redwood. St Thomas’ Hospital, London, UK
Background: Coronary flow reserve (CFR) is defined as the ratio of baseline to hyperaemic coronary flow and interrogates combined epicardial and microvascular resistance. It has been shown to be a predictor of the functional significance of an epicardial coronary lesion and an important prognostic indicator pre- and post-intervention. A recently validated technique employing thermodilution (assessed with the pressure wire) to establish CFR has been shown to correlate well with absolute flow reserve. In addition it is has been suggested that a surrogate value may be derived mathematically by dividing the square root of the hyperaemic pressure gradient across a stenosis by the square root of the baseline gradient.
Methods and Results: In this study we compared 100 paired measurements of pressure derived CFR with thermodilution derived CFR in 27 patients undergoing elective percutaneous intervention (hyperaemia achieved with adenosine 140 µg/kg/min via femoral vein). Mean (SD) age of patients studied was 60.7 (9.7) years. Baseline pressure gradient was 16.4 mmHg (11.8) and hyperaemic gradient 23.6 mmHg (14.5). CFR was 1.8 (0.9) using thermodilution and 1.3 (0.5) from pressure derived calculation. There was no significant relationship between pressure derived and thermodilution derived CFR values (r = 0.33) (see graph). However, separate analysis revealed a close correlation pre intervention between the measurements(r = 0.81, p<0.001), but none post intervention (r = 0.14, p = 0.29).
Conclusions: Pressure derived CFR provides a satisfactory correlate of true CFR pre-intervention, however following percutaneous intervention there is no relationship between a pressure derived index and that obtained using thermodilution techniques. This lack of the relationship likely reflects inadequate interrogation of the microvascular response to intervention.
flow reserve; pressure wire; coronary physiology
246 PREOPERATIVE NEUTROPHIL-LYMPHOCYTE RATIO AND OUTCOME FROM CORONARY ARTERY BYPASS GRAFTING
P. Gibson, B. Croal, B. Cuthbertson, G. Small, A. Ifezulike, G. Gibson, R. Jeffrey, K. Buchan, H. El-Shafei, G. Hillis. Aberdeen Royal Infirmary, Aberdeen, UK
Objectives: The aim of this study was to assess the prognostic utility of the neutrophil/lymphocyte (N/L) ratio in patients undergoing coronary artery bypass grafting (CABG).
Background: An elevated preoperative white cell count (WCC) has been associated with a worse outcome following CABG. Leukocyte subtypes, and in particular the N/L ratio, may, however, convey superior prognostic information. We hypothesised that the N/L ratio would predict the outcome of patients undergoing surgical revascularisation.
Methods: Baseline clinical details were obtained prospectively in 1938 patients undergoing CABG. The differential leukocyte count was measured a median of 1 day before surgery and patients were followed-up a median of 3.6 years later. The primary end-point was all-cause mortality.
Results: The preoperative N/L ratio was a powerful univariable predictor of mortality (hazard ratio (HR) 1.13, p<0.001). In a backward conditional model, including all other individual study variables, it remained a strong predictor (HR 1.08, p = 0.01). In a further model, including the European system for cardiac operative risk evaluation (EuroSCORE), the N/L ratio remained an independent predictor (HR 1.08, p = 0.008). Likewise, it was an independent predictor of cardiovascular mortality and predicted death in the subgroup of patients with a normal WCC (<10 × 109 per litre). This excess hazard was concentrated in patients with a N/L ratio in the upper quartile (N/L ratio>3.36).
Conclusion: An elevated N/L ratio is associated with a poorer survival after CABG. This prognostic utility is independent of other recognised risk factors.
coronary artery bypass grafting; leukocyte; survival
247 THE PREVALENCE AND PROGNOSTIC VALUE OF ATHEROSCLEROTIC RENAL ARTERY STENOSIS IN PATIENTS WITH LEFT VENTRICULAR SYSTOLIC DYSFUNCTION
C. Bourantas1, P. Loh1, D. Ettles2, R. de Silva1, E. Lukaschuk1, A. Tweddel1, A. Clark1, P. Nikitin1, J. Cleland1. 1Department of Academic Cardiology, Castle Hill Hospital, Cottingham, UK; 2Department of Vascular Radiology, Hull Royal Infirmary, Hull, UK
Background and aims: Atherosclerotic renal artery stenosis (RAS) is a common cause of renal dysfunction and associated with neurohormonal activation. These may have deleterious effect in patients with left ventricular systolic dysfunction (LVSD). However, the prevalence of RAS in patients with LVSD, its impact on treatment administration and prognostic significance are unclear.
Methods: 144 consecutive patients with left ventricular ejection fraction (LVEF) <50% and on stable treatment who underwent cardiac magnetic resonance imaging (CMR) were recruited to undergo a renal magnetic resonance angiography (MRA) at the same time. Their kidney sizes were measured and glomerular filtration rates (GFR) were estimated using MDRD formula. The patients were divided into 3 groups: A (GFR >60 ml/min/1.73 m2), B (40–60 ml/min/1.73 m2) and C (<40 ml/min/1.73 m2). RAS >50% was considered as clinically relevant.
Results: The number of patients in A, B and C were 51, 44 and 49 respectively. The mean age was 70 (10) years and 85% were men. 67% had ischaemic heart disease and 17% had diabetes. The mean LVEF was 32 (10)% and 22% had NYHA III/IV breathlessness. CMR measurements were similar among the 3 groups of patients. When compared to Groups A and B, C was older (75 (7) vs 63 (11) and 74 (8) years, p<0.001), had higher prevalence of unilateral or bilateral RAS (67% vs 22% and 39%, p<0.001) and unilateral or bilateral small kidney (43% vs 21% and 24%, p = 0.043), less likely to receive more than one renin-angiotensin-aldosterone blockers (RAASB) (6% vs 26% and 21%, p = 0.019) but had higher loop diuretic dose (66 (49) mg vs 38 (31) and 46 (35) mg furosemide equivalent, p = 0.018). The 18-month all-cause mortality rates in Groups A to C were 14%, 14%, 27% respectively, p = 0.029. In multiple Cox regression model, after adjustment for age, sex, RAASB, RAS or small kidney, Group C (HR 3.05; 95% CI 1.34 to 6.98, p = 0.03 compared to Group A) and LV end diastolic volume index (corrected for body surface area, HR 1.01; 95% CI 1.00 to 1.02, p = 0.003) were independent predictors of all-cause mortality. In 64 patients who had a repeat CMR within 18 months, the CMR measurements and their percentage change from the first scans were similar among all groups.
Conclusion: The prevalence of RAS is high in patients with LVSD and impaired renal function. These patients have higher mortality and less likely to tolerate optimal heart failure treatment. The results from ASTRAL study may clarify if percutaneous angioplasty and stent of RAS allows treatment optimisation and improve prognosis.
cardiac magnetic resonance imaging; renal artery stenosis; heart failure
248 UNCOMPLICATED OBESITY IS CHARACTERISED BY ALTERED SYSTOLIC AND DIASTOLIC MYOCARDIAL VELOCITIES AS ASSESSED BY PHASE CONTRAST MAGNETIC RESONANCE IMAGING
M. Ali1, O. Rider1, S. Petersen1, J. Francis1, M. Robson1, M. Robson1, C. Jackson1, B. Jung2, M. Robinson1, S. Neubauer1. 1Oxford Centre for Magnetic Resonance Research, Department of Cardiovascular Medicine, University of Oxford, Oxford, UK; 2Department of Diagnostic Radiology, Medical Physics, University of Freiburg, Freiburg, Germany
Introduction: The increasing prevalence of obesity poses a range of health-related and socioeconomic problems. The effects of uncomplicated obesity, a subgroup with no other cardiovascular risk factors, on the cardiovascular system have not been fully elucidated. Tissue velocities are highly sensitive indices of global or regional ventricular function.
Aim: To investigate whether subtle preclinical changes in cardiac function occur in uncomplicated obesity, this study aimed to characterise three-dimensional velocities of the left ventricle derived from cardiac MR scanning and compare these to normal-weight controls. We hypothesised that obesity alone leads to alterations in global left ventricular (LV) tissue velocities.
Methods: Thirty six obese individuals (19 men, 17 women, BMI 35.6 (SD 5.2)) selected on the basis of having no identifiable cardiac risk factors (non-smoking, normotensive, normocholesterolemic with non-diabetic range fasting glucose measurements) were compared to 34 healthy controls (19 men, 15 women, BMI 22.4 (SD 1.6)). All subjects underwent “tissue phase mapping” at 1.5 Tesla, a method of quantifying 3D tissue motion.
Results: There were no significant differences in age, gender distribution, blood pressure and heart rate between obese subjects and lean controls. LV volumes and ejection fraction were similar and within normal limits in both groups. All results were adjusted for the higher LV mass in the obese group (131.9 (29.6) g vs 107.4 (26.5) g, p<0.001) using univariate regression analysis, even though LV mass remained within the normal range. Significant systolic changes were seen in the obese group with reduced peak radial velocities (2.63 vs 2.95 cm/s, p = 0.005) and later time to peak longitudinal contraction rate (155.5 vs 119.7 ms after the end-systolic time, p = 0.004). Significant alteration in diastolic parameters was also seen. Peak diastolic radial velocities were significantly lower in the obese cohort (−3.10 vs −3.69 cm/s, p = 0.001). Diastolic maximal longitudinal relaxation rates were similar in both groups (6.23 vs 6.36 cm/s, p = 0.78) but were reached at a significantly later time-point in the obese cohort (504.6 vs 449.3 ms, p<0.001). This was in keeping with longer time to peak diastolic longitudinal strain rate in obesity (156.4 vs 134.8 ms, p = 0.002). No significant differences were shown in systolic (18.2 (6.5) vs 17.3 (6.1) cm/s, p = 0.849) and diastolic torsion rates (−15.0 (4.1) vs −14.0 (5.9) cm/s, p = 0.089) between obese and lean subjects.
Conclusions: Cardiac tissue velocities in an obese group without comorbid risk factors reveal the true effects that obesity alone induces on heart motion. Our results demonstrate altered myocardial contraction and relaxation patterns in otherwise healthy obese people, independent of their higher LV mass. Obesity thus has a direct effect on cardiac function independent of frequently associated comorbidities such as hypertension, diabetes or hypercholesterolemia.
uncomplicated obesity; tissue phase mapping; myocardial velocities
249 TROPONIN-I CONCENTRATIONS 72 H AFTER MYOCARDIAL INFARCTION ARE A RELIABLE PREDICTOR OF INFARCT SIZE AND MICROVASCULAR OBSTRUCTION: A CMR IMAGING STUDY
J. Younger1, S. Plein1, J. Barth2, M. Sivananthan2, J. Ridgway2, S. Ball1, J. Greenwood1. 1Leeds University, Leeds, UK; 2Leeds General Infirmary, Leeds, UK
Objectives: To use late gadolinium enhanced cardiac magnetic resonance imaging (LGE-CMR) to investigate the utility of a single measurement of troponin I, 72 h after myocardial infarction (72-h troponin-I), as an predictor infarct size and presence of microvascular obstruction (MVO), compared to serial creatine kinase (CK), and 12-h troponin-I measurements.
Abstract 249 Infarct size and biomarker concentration according to the presence of microvascular obstruction
Methods: Ninety seven patients underwent LGE-CMR at 3.7 (1.4) days after medically treated first acute myocardial infarction (AMI). Serum troponin-I concentrations were measured at 12 and at 72 h after admission, in addition to serial CK levels. A cumulative dose of 0.2 mmol/kg gadolinium-DTPA was administered and late gadolinium hyper-enhancement imaging was carried out at least 10 min after the final injection.
Results: Ninety three patients, of whom 71 had received thrombolysis, completed the CMR study. Peak CK, 12-h troponin-I, and 72-h troponin-I were available in 93, 37, and 64 patients respectively, and were related to acute infarct size (r = 0.74, p = 0.0001; r = 0.56, p = 0.0003; r = 0.62, p<0.0001 respectively). Infarct mass was larger, and serum biomarkers demonstrated higher values, in the group with MVO compared to those without MVO (peak CK 3085 (1531) vs 1471 (1135), p<0.001; 12-h troponin-I 58.3 (46.9) vs 33.4 (40.0), NS (p = 0.13); 72-h troponin-I 11.5 (9.9) vs 5.5 (4.6), p<0.005). The correlation between the extent of MVO and 12-h troponin-I was not significant, in contrast to the other serum biomarkers (peak CK r = 0.44, p<0.0001; 12-h troponin-I r = 0.17, p = NS; 72-h troponin-I r = 0.45, p = 0.0002).
Conclusion: A single measurement of 72-h troponin-I is superior to 12-h troponin-I, and equivalent to serial creatine kinase measurement in the estimation of myocardial infarct size and the prediction of MVO.
cardiac MRI; troponin; microvascular obstruction
250 SEVERITY OF CARCINOID HEART DISEASE AND RELATIONSHIP WITH NT-PROBNP
S. Bhattacharyya1, C. Toumpanakis2, M. Caplin2, J. Davar1. 1Department of Cardiology, Royal Free Hospital, London, UK; 2Neuroendocrine Tumour Unit, Royal Free Hospital, London, UK
Introduction: Carcinoid heart disease (CHD) is characterised by endocardial and valvular plaque deposition, thickening of valve leaflets as well as chordae and subvalvular apparatus causes reduced excursion, retraction and non coaptation of valve leaflets associated with valvular regurgitation and stenosis. Valvular abnormalities can affect both the right and left sided cardiac valves. Severity of CHD affecting each valve as well as the number of heart valves involved varies. N-terminal fragment brain natriuretic peptide (NT-proBNP) is raised in severe carcinoid heart disease. We assessed the variation in severity of CHD and whether NT-proBNP correlates with the severity of carcinoid heart disease.
Methods: 100 patients with mid-gut carcinoid tumour underwent transthoracic echocardiography (TTE). Transoesphageal echocardiography was undertaken if information on valve structure could not be obtained satisfactorily on TTE imaging. 21 patients with CHD were identified. Severity of carcinoid heart disease was scored. Each valve was individually scored (fig 1) and the sum of all four valves produced a total carcinoid score. NT-proBNP was measured in all patients prior to echocardiography.
Results: Median carcinoid score was 25 (range 5–39). One third of patients with CHD had one affected valve, 38% two valves, 19% three valves and 2 patients (10%) had all carcinoid involvement of all four cardiac valves. Median NT-proBNP in patients with CHD was 1347 pg/ml (interquartile range 406–3389). NT-proBNP positively correlated with carcinoid score. Spearman rank correlation coefficient r = 0.88, p<0.0001 (fig 2).
Conclusion: There is a wide variation in severity of CHD. The majority of patients with CHD have involvement of one or two valves. NT-proBNP correlates with the severity of carcinoid heart disease. This may provide a medium for monitoring patients with carcinoid heart disease.
valvular; carcinoid; brain natriuretic peptide
251 ECHOCARDIOGRAPHY FOR CARDIOMEGALY IDENTIFIED IN CHEST X RAY: AN AUDIT OF 625 PATIENTS
S. Sulfi1, D. Balami1, A. Suliman1, R. Archbold2, A. Kapur2, K. Ranjadayalan1, A. Timmis2. 1Newham University Hospital, London, UK; 2London Chest Hospital, London, UK
Background: Cardiomegaly identified on the chest x ray has important prognostic correlates. It is a common indication for transthoracic echocardiography (TTE). We have analysed the frequency with which TTE is requested for this indication and its diagnostic usefulness.
Methods: Data were collected prospectively from patients undergoing TTE in a district general hospital from 1997–2006. 24 400 echocardiograms were analysed. All TTE reports were entered and stored electronically on a purpose built database. The database was interrogated with multiple structured queries.
Results: Of the 24 400 TTE studies performed over the 9-year period, 625 (2.6%) were undertaken for cardiomegaly as one of the indications. The requests were divided into the following groups: (1) cardiomegaly without any symptoms or findings pertaining to cardiovascular system (n = 323); (2) cardiomegaly with non-specific cardiac related symptoms, for example, shortness of breath (n = 210); (3) cardiomegaly with specific cardiac abnormalities, for example, abnormal ECG (n = 92). Clinically relevant abnormalities were found in 43/323 studies in group 1 (13.3%), 62/210 studies in group 2 (29.5%) and 42/92 in group 3 (45.7%).
Conclusion: Cardiomegaly is not a common indication for TTE in a district general hospital setting, contrary to popular perception. The diagnostic yield from TTE studies in this group of patients is high, particularly in patients with associated cardiac symptoms and abnormal ECGs. Even isolated cardiomegaly without associated abnormalities can provide enough diagnostic yield to justify the cost and manpower use.
cardiomegaly; echocardiogram; diagnostic utility
252 CT ATTENUATION CORRECTION OF SPECT MYOCARDIAL PERFUSION SCINTIGRAPHY IMPROVES DIAGNOSTIC ACCURACY
G. Wright, K. Cockburn, G. Davies, G. Avery, A. Tweddel. Hull & East Yorkshire Hospitals NHS Trust, Cottingham, UK
Introduction: Myocardial perfusion imaging is a standard technique to assess the functional impact of coronary disease. Image quality may be limited by attenuation of counts from the heart by intervening tissue such as breast. This non-uniform attenuation results in artifacts on SPECT myocardial perfusion scintigraphy (MPS), which can reduce diagnostic accuracy. Previous attempts to correct for attenuation have had limited success, possibly due to the low quality attenuation maps acquired using transmission sources. Hybrid SPECT/CT systems give the possibility of acquiring high quality attenuation maps with the potential for more accurate attenuation correction (AC). The aim of this study was to determine whether CT based AC can reduce artifacts and hence improve the diagnostic accuracy of SPECT MPS.
Methods: Seventy four SPECT images of a Tc99m filled myocardial phantom within an anthropomorphic torso phantom were acquired on a GE Infinia gamma camera. Hawkeye-CT images were acquired for AC. Breast attenuation was simulated in 55 studies by adding 2, 4 or 6 saline bags to the torso phantom. One myocardial defect (50 studies) or 2 defects (12 studies) were simulated anteriorly, laterally, inferiorly, septally or apically. Defects were either filled with activity at 50% of the myocardial concentration (n = 60) or no activity (n = 14). The liver insert of the torso phantom was filled with the same concentration of Tc99m as the myocardium for 24 studies and at 2.5 times the myocardium for 26 studies. Images were reconstructed using iterative reconstruction with AC, and filtered back projection without AC. Corrected and non-corrected images were reported by a single experienced observer on separate occasions after randomisation, blinded to the presence or absence of defects but aware of the simulated breast size and whether AC had been performed. Images were divided into five segments (lateral, anterior, septal, inferior and apical), giving a total of 740 segments. Each segment was scored for the presence of a defect using a five point scale (5 = definitely abnormal, 1 = definitely normal). These scores were used to perform receiver operator characteristic (ROC) analysis.
Results: The area under the ROC curve obtained from attenuation corrected images was significantly higher than for non-corrected images (0.99 (0.01) vs 0.95 (0.02), p = 0.04). Although visually the anterior wall was most improved by AC, the inferior wall improved predominantly in terms of sensitivity (88% vs 58%) and specificity (100% vs 100%). Improvement was also seen in the sensitivity of the septal region (100% vs 75%) at specificities of 98% and 95%.
Conclusions and Implications: Attenuation correction using low-resolution Hawkeye-CT improved diagnostic accuracy in this phantom study. It was particularly helpful in the area associated with subdiaphragmatic attenuation and thus is likely to be beneficial in clinical SPECT MPS studies performed with Tc99m.
CT attenuation correction; SPECT; myocardial perfusion imaging
253 CAN WE RELY ON TISSUE VELOCITY PROFILES WHEN STUDYING LEFT VENTRICULAR DYSYNCHRONY?
M. Marciniak, A. Baltabaeva, A. Marciniak, C. Parsai, B. Bijnens, G. Sutherland. St George’s Hospital, London, UK
Background and Aims: Variations in regional systolic velocity profiles (SVP) have been widely used to assess cardiac dyssynchrony. However, regional longitudinal SVPs have a non-uniform pattern. SVPs in the septal and inferior walls are similar being monophasic with an early systolic peak. In contrast, SVPs in the anterior and lateral walls differ, being biphasic with two systolic peaks. Thus when assessing the timing of delayed contraction in the anterior and lateral walls it is important to know what each peak represents. Ventricular interaction could be responsible for the early deceleration of the first peak in anterior and lateral wall motion and could explain the biphasic systolic pattern. We postulated that early cessation of the first systolic motion and appearance of a second shortening motion in the anterior and lateral walls may be due either to a combination of cardiac twisting around the long axis of the heart and interaction with RV contractile function rather than local myocardial shortening. We investigated the relation between regional peak systolic velocities in the right ventricular free wall (RV), septum (SEP) and lateral wall (LW).
Methods: In 38 normals (mean age 42 (11) years) long axis regional SVPs were obtained from the basal segments of RV, SEP and LW. Time to maximal deceleration of the first peak was measured in the lateral wall and its relation to RV peak velocity determined. In addition the time to peak Vel in all walls was calculated.
Results: The timing of peak systolic Vel in the RV corresponded to the end of deceleration of the first peak in the LW SVP (0.200 (0.03) vs 0.203 (0.03) sec, p = NS). There was a consistent and significant difference between the time to first peak systolic Vel in LW vs RV (0.119 (0.02) vs 0.200 (0.03) sec, p<0.001) with the SEP peak systolic Vel in an intermediate position at 0.142 (0.03) sec (p<0.001 vs RV and p<0.001 first peak in LW). There was strong and positive correlation (r = 0.91, p<0.0001) between the timing of peak systolic Vel in the RV free wall and the end of deceleration of the first peak in the LW.
Conclusions: This study showed that the early cessation of the first peak systolic velocity and second velocity peak in the LW wall is due to motion induced by RV contraction. and does not represent LV contractile function. Therefore measurement of cardiac synchronisation should not be based on velocities profiles.
tissue velocity imaging; dysynchrony; echocardiography
254 HIGH SPATIAL-RESOLUTION MYOCARDIAL PERFUSION MR IMAGING USING K-T SENSE
S. Plein1, S. Ryf2, P. Boesiger2, J. Greenwood1, A. Radjenovic1, S. Kozerke2, J. Schwitter3. 1University of Leeds, Leeds, UK; 2ETH and University of Zurich, Zurich, Switzerland; 3University Hospital Zurich, Zurich, Switzerland
Introduction: First-pass myocardial perfusion MR imaging requires high temporal resolution, high in-plane spatial resolution and multislice myocardial coverage. Conventional MR pulse sequences can only partially meet these requirements. Echo-planar imaging or parallel data acquisition methods have therefore been applied to myocardial perfusion MR imaging, but provide only relatively modest acceleration. The recently proposed method k-t SENSE allows substantially more acceleration factors. These can be invested in high spatial resolution. Here we investigate the clinical applicability of high-resolution k-t SENSE accelerated myocardial perfusion MR imaging in patients with coronary artery disease.
Abstact 254
Methods: Twenty patients (16 male, 4 female, mean age 56 years) underwent adenosine stress MR imaging within 14 days of an x ray angiogram on a 1.5T Philips MR system. A saturation recovery segmented gradient echo pulse sequence was used (TR: 2.7–3.1 ms, TE: 0.9–1.1 ms, flip angle: 15°, k-t factor of 5 with 11 k-t interleaved training profiles, 4 slices acquired sequentially over 2 RR intervals, spatial resolution 1.5×1.5×10 mm3, 0.1 mmol/kg Gadovist (Schering)). Image quality was graded on a scale of 1 (poor) to 4 (excellent). Occurrence of all artifacts was recorded and graded from 1 (none) to 4 (images non-diagnostic). Dark-banding artifacts were recorded separately (1 none to 4 severe). Perfusion data were reviewed visually and perfusion defects reported using the AHA classification. Diagnostic accuracy of MR perfusion analysis to detect coronary artery stenosis of >70% on QCA of the x ray angiogram was determined for patients as a whole and for individual coronary vessels.
Results: All studies were completed successfully. Mean image quality score was 3.3 with one study graded as non-diagnostic. The most commonly observed artifacts were due to respiratory motion (occurring in 7 patients). Dark banding artifacts were seen in half of the image data sets but were limited to the endocardial border in the diastolic images and measured no more than one pixel. Sensitivity to detect significant CAD on a patient basis was 92%. With 4 false-positive studies, specificity was 57% on a patient level. Sensitivity and specificity of CMR perfusion imaging to localise disease to specific coronary vessels ranged from 75% to 100%. Two of the 4 patients with “false positive” MR perfusion studies showed circumferential subendocardial hypoperfusion and had significant left ventricular hypertrophy.
Conclusions: k-t SENSE accelerated imaging is feasible in. Good breathholding is essential for image quality. At a k-t acceleration factor of 5, a spatial resolution of 1.5 mm can be achieved. Potentially, hypertensive microvascular disease can be identified as circumferential subendocardial ischaemia and may have been the cause for the relatively low specificity in this study.
MRI; perfusion; ischaemia
255 THE EFFECT OF GROWTH HORMONE UPON CARDIAC FUNCTION AND EXERCISE CAPACITY IN PATIENTS WITH ADULT ONSET GROWTH HORMONE DEFICIENCY
J. Windram1, S. Gonzalez2, L. Ingle1, N. Nikitin1, A. Clark1, S. Atkin2. 1Academic Cardiology, Hull Royal Infirmary, Hull, UK; 2Department of Academic Endocrinology, Hull Royal Infirmary, Hull, UK
Introduction: There is increasing evidence that growth hormone (GH) has an important role in cardiac growth and function. Abnormalities in cardiac function and exercise capacity have been observed in patients who have GH deficiency (GHD). In our study cardiac MRI (CMR) was used to investigate the effects of GH replacement therapy on cardiac function and cardiopulmonary exercise testing (CPET) was used to assess change in exercise capacity.
Methods: Seventeen subjects with adult GHD (mean age 48.4 (14.6) years, 10 males) were enrolled into a double blind, placebo controlled, crossover designed trial of 6 months duration. Patients then continued with GH therapy open labelled for another 6 months. Assessments were made at four time points: baseline: midway through the crossover trial; at the end of the crossover trial and again 6 months later. Recombinant human GH (Humatrope) was given as a daily injection of 0.4 mg. Insulin like growth factor-1 increased significantly during GH therapy demonstrating that an endocrine effect was induced. The average time between diagnosis of GH deficiency and entry into the trial was 2.8 years. No patient had received GH before entry into the trial. Cardiac structure and function was assessed by means of cardiac MRI (Phillips 1.5 Tesla) at each assessment point. A CPET was performed within a week of the CMR study on all patients.
Results: At baseline ejection fraction (EF) was 72.5 (5.3)%, end diastolic volume (EDV) was 132.4 (31.8) ml, end diastolic mass (EDM) was 145 (22) g, and end diastolic mass corrected for body surface area (EDM/BSA) was 69.1 (10) g/m2. No significant change was observed in either EF (p = 0.5), EDV (p = 0.97), EDM (p = 0.87) or EDM/BSA (p = 0.84) with GH therapy. At baseline subjects had a peak oxygen consumption (pVO2) of 26.21 (6.2) ml/min/kg, minute ventilation-carbon dioxide production slope (VE/VCO2) of 27.6 (3.9), anaerobic threshold (AT) of 15.4 (4.2) ml/min/kg and an exercise duration of 698 (10.8) s. No significant change was observed in pVO2 (p = 0.5), VE/VCO2 (p = 0.9), AT (p = 0.98) or exercise duration (p = 0.9) during the study.
Conclusion: Growth hormone therapy was found to be safe and without serious side effects in patients who are GH deficient. No beneficial effects were noted however upon cardiac function or exercise capacity.
growth hormone; cardiac mri; cardiopulmonary exercise testing
256 GENETIC LINEAGE TRACKING OF HAEMATOPIETIC CELLS USING THE CRE/LOX SYSTEM TO INVESTIGATE THE ROLE OF ENDOTHELIAL PROGENITOR CELLS IN NORMAL VASCULAR DEVELOPMENT AND AFTER VASCULAR INJURY IN MICE
A. Wragg1, J. Mellad2, H. San2, A. Mathur1, M. Boehm2. 1The London Chest Hospital, London, UK; 2National Institutes of Health, Bethesda, USA
Introduction: It has been suggested that bone marrow (BM) may be a source of endothelial progenitor cells (EPCs) although it has been questioned whether haematopoietic cells can actually differentiate into endothelium. Monocytes have been suggested as being the source of EPCs. As the original cell specific markers of BM derived cells are believed to change after the cells adopt a different phenotype, we adopted a genetic lineage tracking approach using the Cre/Lox system to permanently mark a cell’s origin, independently of its present protein markers. We focused on tracking the fate of CD45 + and LysM + cells (expressed on myeloid cells) to investigate if these cells differentiate into endothelial cells under injury and non-injury conditions.
Methods: The floxed R26R-lacZ locus was used as a reporter gene for genetically labelling and tracking cells. R26R-lacZ transgenic mice were crossed with mice expressing Cre recombinase under the control of the CD45 and LysM promoters. B-gal expression in leucocytes were analysed using flow cytometry. Fractions of cells were analysed using specific antibodies for lymphocytes, monocytes, granulocytes and haematopoietic stem cells. Femoral arteries from CD45 and LysM ancestry mice were analysed for A-Gal expression. To investigate the role of CD45 and LysM cells after injury mice were submitted to vascular wire injury.
Results: CD45 ancestry mice had low labelling of CD45 + cells. Despite all leucocytes expressing CD45 only 23% of cells were actually labelled with LacZ which was similar across HSCs, T and B lymphocytes, myelo-monocytic cells and granulocytes. In addition LysM ancestry mice have subsets of lymphocytes and HSCs labelled with LacZ. This would imply that LysM cre is not an exclusive myelo-monocytic marker and not all CD45 cells are labelled as intended. To determine whether CD45 and LysM cells contribute to endothelial cells during mouse development, we analysed sections from femoral arteries of CD45 and LysM ancestry mice. No B-Gal expressing cells in the endothelium were detected. Some positive cells within the lumen of vessels or in the adventitia/perivascular space were detected, presumably circulating CD45+ leucocytes or tissue macrophages. This indicates that it is unlikely that CD45+ or LysM+ cells differentiate into endothelial cells as part of normal development. However, in CD45 and LysM ancestry mice we found significant infiltration of labelled cells after wire injury. Some cells were inflammatory although cells lining the lumen of the vessels clearly have an endothelial morphology. This would indicate that CD45 ancestry cells may have adopted an endothelial phenotype after vascular injury.
Conclusion: Based on experiments utilising the Cre-Lox system CD45 and LysM haematopoietic cells do not appear to contribute to normal vascular development but they do participate in blood vessel repair after injury. This would imply that EPCs are important in disease states rather than normal homeostasis.
endothelial progenitor cells; vascular injury; Cre/Lox system
257 DEVELOPMENT AND CHARACTERISATION OF VIRAL VECTORS TARGETED TO ATHEROSCLEROTIC PLAQUES
K. White1, H. Buening2, J. McVey3, G. Murphy4, L. Work1, M. Hallek2, S. Nicklin1, A. Baker1. 1BHF Glasgow Cardiovascular Research Centre, University of Glasgow, Glasgow, UK; 2Clinic I for Internal Medicine and Center for Molecular Medicine, University of Cologne, Cologne, Germany; 3Haemostasis and Thrombosis, MRC Clinical Sciences Centre, Imperial Collage London, London, UK; 4Department of Oncology, Cambridge University, Cambridge Institute for Medical Research, Cambridge, UK
Introduction: Atherosclerosis is a leading causes of death in the developed world, mainly as a result of plaque rupture leading to occlusive thrombus formation and myocardial infarction. Targeted delivery of biological agents selective for atherosclerotic plaques would provide a useful agent for treatment and/or imaging of atherosclerosis. Adeno-associated virus 2 (AAV2) is a commonly used gene therapy vector, however it has a broad tropism and following systemic administration mediates inefficient transgenes delivery (transduction) to vascular cells. AAV2 tropism can be altered using small targeting peptides identified by phage display. Therefore insertion of atherosclerotic plaque targeting peptides into the receptor binding site of the virus capsid may create a vector detargeted from its natural tropism and retargeted to regions of atherosclerosis.
Methods: Previously, phage display in ApoE-/- mice identified several peptides that selectively bind to atherosclerotic plaques.1 We engineered two peptides, CAPGPSPSKC (putative receptor glucose regulated protein 78) and CNHRYMQMC (putative receptor membrane type 1 matrix metalloproteinase (MT1-MMP)) into the receptor binding domain of the AAV2 capsid to produce AAV-CAP and AAV-CNH. Modified viruses expressing the LacZ and eGFP reporter genes were produced and their ability to mediate vascular-specific gene delivery was tested.
Results: In a non-vascular cell line (HeLa) that does not express the putative receptors for the viruses, neither of the peptide-modified viruses produced significantly higher levels of transduction than control unmodified AAV2. AAV-CNH transduced murine, rat and human endothelial cell lines 10–100-fold higher than control AAV2 (p<0.05). AAV-CNH transduction was mediated through a proteasome-insensitive pathway, suggesting that peptide insertion alters both receptor binding and trafficking of the virus. In addition, AAV-CNH transduced cells overexpressing the putative receptor MT1-MMP at significantly higher levels than control cells. Surface plasmon resonance confirmed that the vector binds to MT1-MMP in a dose-dependent manner whereas no interaction could be detected with unmodified AAV2. Next, modified AAV vectors were further characterised in vivo in the ApoE-/- mouse model of atherosclerosis. 28 days post-intravenous injection of the vectors real-time PCR was used to detect virus in tissues. Compared to control AAV2, substantially higher levels (10–100-fold) of AAV-CAP and AAV-CNH were detected in the brachiocephalic artery and aorta (sites of atherosclerotic plaque formation), with reduced levels in all other organs examined, including liver, spleen, lungs and heart.
Conclusions: These results suggest that the tropism of AAV2 based vectors can be substantially altered to create atherosclerotic plaque targeted vectors that will be useful for targeted gene delivery to atherosclerotic tissue.
atherosclerosis; gene therapy; AAV2
1
258 ELEVATED CIRCULATING ENDOTHELIAL PROGENITOR CELLS IN HEALTHY ADULT OFFSPRING OF SUBJECTS WITH CORONARY ARTERY DISEASE
A. Whittaker, J. Moore, M. Vasa, S. Stevens, N. Samani. Department of Cardiovascular Sciences, University of Leicester, Leicester, UK
Introduction: Vascular endothelial injury and dysfunction is the initial feature of atherosclerosis, leading to inflammatory cell recruitment and plaque formation. Endothelial progenitors cells (EPCs), identified by coexpression of CD34/AC133/KDR surface markers, are capable of endothelial repair and neovascularisation. CD34+KDR+ EPCs represent a more mature form while AC133+KDR+ cells are thought to represent a more immature form of EPC. Circulating EPCs are reduced in subjects with coronary artery disease (CAD). However, whether this is a cause or effect of CAD is unknown. We measured the number of circulating CD34+KDR+ and AC133+KDR+ cells in the healthy offspring of subjects with CAD and healthy controls.
Abstract 258
Methods: Fifty one subjects, comprising 27 offspring of parents with severe premature CAD (<65 years, documented at angiography) and 24 age- and gender-matched offspring of healthy subjects from the general population were studied. The mean age of the subjects was 30 years (range 19–43 years) and all were healthy with no personal history of cardiovascular disease. Duplicate samples of 100 μl peripheral venous blood were incubated with either anti-CD34 and anti-KDR, or anti-AC133 and anti-KDR antibodies. Samples were analysed by fluorescent activated cell sorting with lymphocyte gating. 100 000 total events per CD34+KDR+ sample and 200 000 total events per AC133+KDR+ sample were recorded. Dual positive cells were taken to represent EPCs and recorded as a percentage of the lymphocyte population. Isotype controls were used for each antibody. Serum stromal cell derived factor-1α (SDF1α) and vascular endothelial growth factor (VEGF) concentrations were measured by ELISA.
Results: Circulating EPCs were grouped into tertiles (undetectable (1), low level (2), and high level (3)) for statistical analysis. Offspring of parents with CAD had significantly more circulating CD34+KDR+ and AC133+KDR+ cells than offspring of healthy controls (p = 0.032 for CD34+KDR+; p<0.001 for AC133+KDR+ cells). On adjusted logistic regression analysis CD34+KDR+ group, AC133+KDR+ group and BMI were the only significant predictors of case/control status in the offspring (table). There were no differences in serum SDF1α or VEGF between offspring of healthy or CAD parents.
Conclusions: Our results of increased circulating EPCs in offspring of subjects with CAD compared with offspring of healthy subjects may at first sight seem paradoxical as CAD has been associated with reduced EPCs. Although the offspring of children with CAD had no clinically apparent coronary disease they could have occult vascular damage and the raised EPC level could reflect a necessary repair response. If this is the case, then our results suggest that elevated EPCs, particularly of the immature AC133+KDR+ type, may represent a biological marker of future risk of CAD in healthy young adults.
endothelial progenitor cells; healthy adult offspring; potential biomarker
259 IGFBP-1 PROTECTS AGAINST OBESITY-INDUCED VASCULAR DYSFUNCTION BY PRESERVATION OF INSULIN SIGNALLING
V. Ezzat1, S. Wheatcroft2, E. Duncan1, J. Sethi3, A. Shah1, M. Kearney2. 1King’s College London, London, UK; 2University of Leeds, Leeds, UK; 3University of Cambridge, Cambridge, UK
Introduction: The insulin-like growth factor-I (IGF-I) axis plays an important role in the regulation of glucose homeostasis and has also been implicated in the development of cardiovascular disease. We have previously shown in a murine model of obesity that IGF-I levels increase as insulin sensitivity decreases and that there is an accompanying decrease in IGF-I sensitivity in both peripheral tissue and the vasculature. Transgenic mice (TG) overexpressing human IGF binding protein–1 (hIGFBP-1) are protecting against these changes despite the development of obesity. We have now assessed changes in native IGFBP-1 expression and protein levels in wild type mice (WT) in obesity; in addition we have further characterised the changes in vascular phenotype during the development of obesity in both WT and TG and attempted to unravel the molecular mechanisms underlying these changes.
Methods: Male C57 Bl/6 mice received an obesogenic or standard chow diet from weaning. Native hepatic IGFBP-1 expression was measured by real-time RT-PCR and circulating protein levels by ELISA. TG overexpressing hIGFBP-1 and their WT littermates were also fed either the obesogenic or chow diet. Systolic blood pressure was measured in all four groups by tail cuff plethysmography. Western blot analyses were performed on muscle and aorta cells of Akt phosphorylation at Thr308 from animals following either saline or insulin injection.
Results: WT receiving a high-fat diet demonstrate significantly decreased insulin sensitivity. In this study we found also that native IGFBP-1 expression and protein levels were significantly decreased (p<0.01). Obese WT became hypertensive compared to chow fed controls (p<0.02) however TG fed a high-fat diet remained normotensive (fig 1, p<0.001). In muscle and aorta, where we have previously demonstrated evidence of insulin and IGF-I resistance in in vivo and ex vivo studies, there was a marked decrease in Akt phosphorylation in high-fat fed WT (fig 2(A), p = 0.02). In obese TG however, there was a strong trend to increased Akt phosphorylation compared to WT counterparts in both muscle and aortic tissue (fig 2(B), p = 0.3 and p = 0.2 respectively), which is consistent with the effects of insulin and IGF-I seen during tolerance testing and in the organ bath.
Conclusions: This work further emphasises the importance of the IGF-I axis in the development of obesity and insulin resistance, and supports the concept of IGFBP-1 as vasculoprotective molecule in this context. These data suggest that this effect may be mediated by the preservation of the insulin signalling pathway.
This work was supported by the British Heart Foundation.
IGF-I; insulin; hypertension
260 PRESENCE OF ATHEROSCLEROSIS DETERMINES THE VASCULAR BUT NOT THE CARDIAC EFFECTS OF EXERCISE TRAINING THROUGH ENDOTHELIAL NOS ACTIVITY
J. de Bono1, D. Adlam1, M. Zhang1, D. Paterson2, K. Channon1. 1Department of Cardiovascular Medicine, University of Oxford, Oxford, UK; 2Department of Physiology, Anatomy and Genetics, University of Oxford, Oxford, UK
Introduction: In patients with vascular disease, regular exercise training is associated with improved prognosis and enhanced nitric oxide signalling. However there is little evidence that athletes who exercise regularly have better vascular function than normal healthy controls. In this study, mouse models have been used to investigate the molecular mechanisms underlying the beneficial effects of exercise on vascular disease.
Methods: We used a custom-made facility to measure the vascular response to exercise in both healthy C57Bl6 mice and hypercholesterolaemic Apo-E knockout mice. Mice were exercised using a voluntary running wheel. Simultaneous measurements of blood pressure in exercising mice were performed using radiotelemeters.
Results: In healthy wild type animals, three weeks’ exercise training had no effect on amount of aortic endothelial nitric oxide synthase (NOS) protein, NOS activity or on the concentration of the critical cofactor for NOS, tetrahydrobiopterin (BH4) within the aorta. Neither shorter (8 days) or longer (6 weeks) periods of exercise training had any effect on vascular NOS function in healthy mice. There was minimal effect of exercise training on systemic blood pressure at any time point. However exercise training had clear physiological effects elsewhere in these mice leading to bradycardia, cardiac hypertrophy and increased muscle citrate synthase activity. In contrast exercise training in ApoE-KO mice led to a significant rise in vascular NOS activity accompanied by increased eNOS protein in male mice and raised BH4 concentration in female mice.
Conclusion: The beneficial vascular effects of exercise are only seen in animals with pre-existing vascular disease. Healthy mice do not enhance their vascular NO signalling pathways nor reduce their blood pressure in response to regular exercise, despite marked physiological adaptations to exercise in the heart, musculature and autonomic nervous system.
exercise; nitric oxide synthase; vascular disease
261 VENOSELECTIVITY OF NITRITE: EVIDENCE FAVOURING HYPOXIC RELEASE OF NITRIC OXIDE
A. Maher1, P. Gunaruwan1, K. Abozguia1, T. Palin1, P. James2, M. Frenneaux1. 1University of Birmingham, Birmingham, UK; 2University of Wales, Cardiff, UK
Background: Nitric oxide may act locally or may undergo one of several metabolic conversions in the blood, including conversion to nitrite. It has been proposed that in hypoxic conditions nitrite can be reduced to nitric oxide resulting in vessel dilation. We reasoned that if this is correct then in vivo nitrite would have a more marked dilator effect in capacitance than in resistance vessels. To investigate this we simultaneously studied the effects of intra-arterial infusion of nitrite upon forearm blood flow (FBF) and venous capacitance in healthy volunteers.
Methods: We studied 11 healthy volunteers. Following a baseline infusion of 0.9% saline we infused sodium nitrite at incremental doses of 314 nmol/min, 784 nmol/min, 3.14 μmol/min and 7.84 μmol/min, measuring forearm blood flow (FBF) using standard strain gauge plethysmography and forearm venous volume (FVV) using radionuclide plethysmography from which volume-pressure relationships were generated. Changes in FBF, and in FVV in the infused arm were corrected for those in the control arm. Plasma nitrite was measured at each stage in venous blood from both arms.
Results: Nitrite produced a venodilation (corrected for the control arm) of (mean (SEM)) 8.2% (4.0%), 10.3% (2.8%), 20.6% (4.2%) and 37.7% (4.9%) at 314 nmol/min, 784 nmol/min, 3.14 μmol/min and 7.84 μmol/min respectively (p<0.001). The increase in FBF was not significant (FBF-ratio increased from 1.2 (0.2) to 1.8 (0.2) (p = NS)). Venous plasma nitrite increased from 602 (67) nm at baseline to 2840 (186) nm at peak dose (p<0.01) and from a baseline of 624 (61) nm to 54893 (9532) nm at peak dose (p<0.01) in the control and infused arms respectively.
Conclusions: Nitrite is a potent dilator of venous capacitance vessels at concentrations where arterial blood flow is only modestly affected. While at peak dose the plasma nitrite levels are supranormal and hence represent a pharmacological effect, a significant venodilation is seen at a dose of 400 nmol/min which is accompanied by plasma nitrite levels close to the normal physiological range. This is potentially relevant in conditions such as chronic heart failure, in which subtle changes in pre-load can result in significant effects on cardiac output.
nitric oxide; nitrite; veins
262 OVEREXPRESSION OF HEPATOCYTE GROWTH FACTOR ACCELERATES MINERALISATION OF HUMAN SMOOTH MUSCLE CELLS IN VITRO
Y. Liu, F. Wilkinson, A. Heagerty, A. Canfield, M. Alexander. University of Manchester, Manchester, UK
Introduction: Vascular calcification is a predictor of adverse clinical events and there is growing evidence to indicate it is a regulated process similar to osteogenesis. However, the precise mechanism underlying the process of mineralisation in soft tissues is still unclear. Hepatocyte growth factor (HGF) is a mesenchyme-derived pleiotropic factor, upregulated in atherosclerotic lesions. Recent studies have shown that HGF is produced by osteoblasts and is a key player in bone metastasis of mouse mammary cancer. The aim of our study is to establish the role of HGF and its receptor, c-Met in vascular calcification and to establish if the effects can be blocked by a HGF antagonist, NK4.
Methods: Immunohistochemistry was used to determine the presence of HGF/c-Met in calcified atherosclerotic arteries. Human smooth muscle cells (hSMCs) explanted from femoral arteries were used as our in vitro model of calcification. Mineralisation was determined using alizarin red staining and quantified using a 45Ca incorporation assay, alkaline phosphate (ALP) assay and western blot analysis.
Results: We demonstrate that c-Met is highly expressed within atherosclerotic lesions and co-localises with α-smooth muscle-actin+cells. Adenoviral-mediated overexpression of HGF (AdHGF) in hSMCs cultured in osteogenic-inducing media (2.6 mM Ca2++ 5 mM β-glycerophosphate) accelerates mineralisation, which is detected after 8 days, compared to 28 days in hSMCs infected by control virus (AdBgl). The in vitro studies demonstrate that high levels of HGF increases calcium incorporation and activity of ALP by 2.0 (0.4)-fold and 3.3 (0.8)-fold (p<0.05), respectively at 8 days. Western blot analysis shows that AdHGF upregulates c-Met after 48 h and downregulates c-Met at 8 days when mineralisation is detected, suggesting involvement of HGF/c-met signalling in the process of hSMC osteogenic differentiation. Furthermore, preliminary data suggest that AdNK4 slows the progression of hSMC mineralisation when grown in osteogenic-inducing media.
Conclusions: These results show that overexpression of HGF significantly accelerates hSMC mineralisation in vitro and the HGF antagonist, NK4, decreases this process. Current studies are investigating the downstream signalling pathway involved in HGF-induced hSMC calcification. This work could have important implications for therapeutic intervention to attenuate calcification in the vessel wall.
vascular calcification; hepatocyte growth factor; c-Met
263 PAR-1 CAUSES ARTERIAL VASODILATATION VIA A TETRAETHYLAMMONIUM-SENSITIVE ENDOTHELIUM-DERIVED HYPERPOLARISING FACTOR IN MAN
N. Lang, I. Gudmundsdottir, N. Boon, D. Newby. 1University of Edinburgh, Edinburgh, UK; 2Royal Infirmary of Edinburgh, Edinburgh, UK
Background: As well as playing an important enzymatic role in the coagulation cascade, thrombin exerts major vascular effects through the activation of protease activated receptor type 1 (PAR-1). We have recently demonstrated that PAR-1 agonism causes arterial vasodilatation in man through an unknown mechanism. We examined the role of endothelium-derived hyperpolarising factor (EDHF), and specifically calcium-activated potassium channels (KCa), in PAR-1 induced vasodilatation.
Methods: Bilateral forearm blood flow was measured by venous occlusion plethysmography in 16 healthy volunteers who attended on two occasions. Intra-arterial tirofiban (1.25 μg/min) was co-infused throughout both studies to counteract PAR-1 induced platelet aggregation. Protocol 1: Intra-brachial SFLLRN (PAR-1 agonist; 5–50 nmol/min), bradykinin (BK; 30–300 pmol/min) and sodium nitroprusside (SNP; 2–8 μg/min) were infused sequentially. In a double blind randomised crossover design (n = 8), agents were co-infused with tetraethylammonium (TEA; a KCa antagonist) or saline placebo. Protocol 2: Protocol 1 was repeated but EDHF activity was isolated by inhibiting the synthesis of prostacyclin (PGI2) and nitric oxide (NO) on both visits (n = 8). PGI2 synthesis was inhibited using oral aspirin (600 mg). NO synthesis was inhibited with intra-arterial NG-monomethyl-L-arginine (L-NMMA; 8 μmol/min). In order to reverse the basal vasoconstriction caused by L-NMMA, intra-arterial SNP was up titrated (0.09–0.45 μg/min) to restore baseline blood flow and co-infused throughout the study to maintain the “NO clamp”.
Results: Neither TEA nor tirofiban affected baseline blood flow in either protocol. In Protocol 1, TEA caused a significant attenuation of PAR-1 agonist and BK induced vasodilatation (p<0.03 for both). In Protocol 2, TEA abolished PAR-1 agonist evoked, EDHF mediated vasodilatation (p = 0.01). It attenuated, but did not abolish, vasodilatation to BK (p<0.001). Endothelium-independent vasodilatation to SNP was unaffected by TEA.
Conclusions: PAR-1 mediates arterial vasodilatation via mechanisms including EDHF in man. The EDHF component of PAR-1 induced vasodilatation requires functional KCa and can be inhibited using TEA. In contrast, BK acts via an EDHF mechanism that is only partially sensitive to TEA-induced KCa blockade. Wider understanding of the vasomotor actions of PAR-1 will help inform the clinical development of novel anti-thrombin and PAR-1 antagonist therapies.
endothelium; protease activated receptor; endothelium derived hyperpolarising factor
264 ENDOTHELIAL FUNCTION, INFLAMMATION AND SERUM LIPID IN PATIENTS WITH CORONARY ARTERY DISEASE TREATED WITH STATINS
S. Agarwal, J. Allen, A. Murray, I. Purcell. Freeman Hospital, Newcastle upon Tyne, UK
Introduction: Endothelial dysfunction has been recognised in various stages of atherosclerosis and occurs prior to the development of overt coronary artery disease (CAD). Inflammatory markers and serum lipids including lipoproteins may play an important role in endothelial dysfunction and atherosclerosis. Endothelial dependent vasodilatation (EDV) in response to local hyperthermia measured by laser Doppler flowmetry can be used as a non-invasive tool to assess systemic microvascular endothelial function. Statins are known to improve endothelial function and reduce inflammation.
Abstract 264 Subject characteristics
Aims: To assess endothelial function using laser Doppler flowmetry, measure serum lipids and high sensitive CRP (hsCRP) in patients with CAD treated with statins.
Methods: Twenty five healthy subjects and 25 patients with CAD undergoing elective coronary angioplasty were studied. Endothelial dependent vasodilatation was assessed by laser Doppler flow in response to controlled local heating of the skin to 41°C. Serum lipids including serum cholesterol, low-density lipoprotein (LDL), high-density lipoprotein (HDL), triglycerides, apolipoproteins A1 and B and highly hsCRP were measured. Patients with CAD were treated with statins for a minimum duration of 6 weeks before the study while none of the controls received statin treatment.
Results: Subject characteristics and lipid profile are shown in the table. Body mass index (BMI) was higher in patients (29 (4) kg/m2) compared with controls (26 (3) kg/m2), p = 0.001. Eight patients had diabetes, 7 had hypertension. One control had hypertension. Peak vasodilatation by hyperthermia was significantly higher in the controls (median 94.8, interquartile range 75–137 AFU) compared to the patients (median 55, interquartile range 45–66 AFU; p<0.000). Serum cholesterol, LDL, HDL and apolipoprotein A1 were significantly lower and serum hsCRP was higher in patients with CAD.
Conclusion: Cutaneous microvascular endothelial function is impaired in patients with CAD despite treatment with statins. HDL, apoliporotein A1 and hsCRP predicts endothelial function in CAD patients treated with statins.
endothelial function; lipids; statins
265 COMBINATION THERAPY FOR SCLERODERMA ASSOCIATED PULMONARY ARTERIAL HYPERTENSION
P. Kabunga1, D. Bloore1, C. Das1, C. Handler1, F. Vrapi1, C. Denton2, C. Black2, C. Smith3, J. Coghlan1. 1Department of Cardiology Royal Free Hospital, London, UK; 2Department of Rheumatology Royal Free Hospital, London, UK; 3Department of Primary Care and Population Sciences, Royal Free & University College Medical School, London, UK
Introduction: We have previously reported that starting Bosentan as first-line therapy in scleroderma associated pulmonary arterial hypertension (SSC-PAH), then adding prostanoids if there is no improvement improves survival in SSC-PAH, compared to previous monotherapy with prostanoids. From January 2004 we have had access to Sildenafil a type 5 phosphodiesterase inhibitor for the treatment of SSC-PAH. The prognostic impact of adding Sildenafil in combination with Bosentan is unclear from previous studies. We wanted to evaluate whether adjunctive Sildenafil therapy was superior or equal to patients treated with Bosentan + prostanoids.
Methods: Between January 2002 and December 2005 we studied 90 consecutive SSC-PAH patients at the Royal Free Hospital, London. 56 patients were treated with Bosentan monotherapy between 2002–3 (Bosentan group) and 34 patients (Bosentan + Sildenafil group) between 2004–5 were also treated with Bosentan as preferred first line treatment but Sildenafil added if after 3 months the mean pulmonary arterial pressure (mPAP) remained ⩾40 mmHg or there was no improvement in six minute walk distance (SMWD) or WHO functional class by one grade. Patients in both groups received anticoagulation (Warfarin), Digoxin, diuretics (loop diuretics and Spironolactone), oxygen (at least 16 h in every 24-h period) and prostanoids (Iloprost, Epoprostenol, or Treprostinil) as clinically necessary. 44% of patients in the Bosentan group were given prostanoids and 3% of patients in the Bosentan + Sildenafil group were given prostanoids, mean time to prostanoids therapy 434 and 30 days respectively. One-year survival measured from the date of diagnosis by right heart catheterisation, SMWD at 4 months and WHO functional class at 10 months were compared in the two groups.
Results: Survival at 1 year in the Bosentan group was 89.3% (95% CI 78.1% to 96.0%) and 94.1% (95% CI 80.3% to 99.3%), p = 0.70 in the Bosentan + Sildenafil group. In the Bosentan group, 4 patients had an improvement in WHO functional class of one grade; 34 patients remained in the same functional class and 14 patients had a decline in functional class. In the Bosentan + Sildenafil group, 8 patients had an improvement in functional class, 20 patients remained in the same functional class and 6 patients had a decline in functional class, p = 0.10. Median (range) change in SMWD at 4 months: +9 m (−410 to +205 m) in the Bosentan group. In the Bosentan + Sildenafil group the median (range) change in SMWT at 4 months: +27 m (−225 to +207 m), p = 0.39.
Conclusion: Adjunctive Sildenafil in combination with Bosentan shows a trend towards improved six minute walk distance, functional class and survival in the treatment of systemic sclerosis associated pulmonary arterial hypertension.
pulmonary arterial hypertension; systemic sclerosis; combination therapy
266 SUCCESS AND CLINICAL OUTCOME OF CATHETER ABLATION FOR SUPRAVENTRICULAR TACHYCARDIA IN PATIENTS WITH SEVERE PULMONARY HYPERTENSION WITHOUT CONGENITAL HEART DISEASE: A CASE SERIES REPORT
R. Showkathali, M. Alzetani, J. Grapsa, P. Nihoyannopoulos, L. Howard, D. Lefroy, J. Gibbs. 1Hammersmith Hospital, London, UK; 2Hammersmith Hospital and Imperial College, London, UK
Introduction and Aim: Supraventricular arrhythmias are poorly tolerated in patients with severe pulmonary hypertension because of their already critically low cardiac output in sinus rhythm. Early effective therapy that minimises the risk of recurrence of the arrhythmia is needed to restore sinus rhythm. Anti-arrhythmic drugs are often unsatisfactory because of the risk of recurrent arrhythmia and a negative inotropic effect with some agents. The aim of this study was to measure the clinical outcome of catheter ablation (CA) of regular supraventricular tachycardia (SVT) in severe pulmonary hypertension (PH) without congenital heart disease (CHD).
Methods: Ten consecutive (6 female, 4 male) patients with a primary diagnosis of severe PH without CHD who underwent catheter ablation for SVT in our institution between September 2001 and March 2006 were identified and their baseline characteristics were recorded. They were followed up to identify recurrence of arrhythmia and symptom improvement. We also compared their 6-minute walk distance (6MWD) and echocardiographic measurements before and 3 months after ablation.
Results: Of the 10 patients with mean age of 52 (17) years (range 20–70), 7 patients had idiopathic pulmonary arterial hypertension (PAH), 2 had chronic thromboembolic pulmonary hypertension, and 1 had associated PAH (L tryptophan use). All were known to have severe pulmonary hypertension (average mean pulmonary artery pressure was 57 (12) mmHg with mean cardiac index of 1.9 (0.6 l)/min/m2) and presented acutely with symptomatic deterioration associated with the onset of arrhythmia. Nine underwent ablation for atrial flutter and one for atrioventricular nodal re-entry tachycardia (AVNRT). Their median procedure time was 115 min (range 55–200). All catheter ablation procedures were successful immediately, but the patient with AVNRT had recurrence at 1 month with successful repeat procedure. The mean and median follow-up periods were 16 and 11 (range 3–45) months respectively. All patients had improvement in their symptoms. Their 6MWD improved significantly 3 months after the ablation, compared to pre ablation (pre-ablation mean, 256 m; post-ablation mean, 312 m, p = 0.050), with no significant difference in echocardiographic measurements of right atrial volume (p = 0.122), right ventricular Doppler index (p = 0.618), eccentricity index in systole (p = 0.775), diastole (p = 0.343), maximum TR velocity (p = 0.671) or estimated right atrial pressure (p = 0.443).
Conclusion: The success rate of CA for SVT in patients with severe PH without CHD is high with low recurrence of the index arrhythmia during the follow-up period. There was significant improvement in their 6MWD after successful catheter ablation. For patients with severe PH and SVT, CA should be considered as first-line therapy.
pulmonary hypertension; supraventricular tachycardia; catheter ablation
267 TYPE 2 DIABETICS ON CHRONIC LISINOPRIL THERAPY EXHIBIT GRADUAL REACTIVATION OF VASCULAR TISSUE ANGIOTENSIN I TO ANGIOTENSIN II CONVERSION
D. Sharman, A. Morris, A. Struthers. Division of Medicine & Therapeutics, Ninewells Hospital, Dundee, UK
Objectives: This study was designed to assess whether vascular tissue angiotensin I (AI) to angiotensin II (AII) conversion reactivates over time in patients with type 2 diabetes treated with chronic angiotensin converting enzyme (ACE) inhibitors.
Background: Vascular tissue AI/II conversion has been shown to reactivate over time in patients with chronic heart failure (CHF) on chronic lisinopril therapy but no data exist that this occurs in the many other non-CHF patients who take ACE inhibitors. We therefore studied this in type 2 diabetics.
Methods: Over 18 months, we followed 30 patients with type 2 diabetes and a previous cardiovascular event or one other major risk factor but without heart failure, who were treated with chronic lisinopril therapy. Vascular tissue AI/II conversion was studied using sequential infusions of inert AI and vasopressive AII into the brachial artery. The response was assessed through forearm venous occlusion plethysmography at baseline, 9 and 18 months after an initial run in period of 2 months. The mean daily dose of lisinopril used was 20 mg and the average duration of ACE inhibitor therapy before the study was 2.3 years (0–7 years). Study patients had been diagnosed with diabetes for 7.1 years (1–14 years) and had a mean HbA1c of 7.2% (6.4–8.6%).
Results: Vascular tissue AI/II conversion was significantly increased at 18 months compared to baseline (p = 0.01), reflecting a reduction in vascular ACE inhibition over time as previously observed in CHF patients. The percentage change in forearm blood flow (FBF) in response to AI infusion was 61% greater at 181 months compared to baseline. FBF response to AII infusion was unchanged over the study period (p = 0.326).
Conclusions: Vascular tissue AI/II conversion does indeed gradually reactivate in patients with type 2 diabetes with a cardiovascular risk factor in the absence of heart failure. This demonstrates a gradual loss of the cardioprotective and renoprotective effects of ACE inhibition over time in diabetics and provides a mechanistic rationale to counter this effect by always combining an AII receptor blocker with an ACE inhibitor in diabetes mellitus.
diabetes; ACE; reactivation
268 CHRONIC HEART FAILURE PATIENTS ON LISINOPRIL VERSUS RAMIPRIL THERAPY EXHIBIT NO DIFFERENCE IN THE REACTIVATION OF VASCULAR TISSUE ANGIOTENSIN I TO ANGIOTENSIN II CONVERSION
D. Sharman, A. Struthers. Division of Medicine & Therapeutics, Ninewells Hospital, Dundee, UK
Objectives: This study was designed to assess whether the reactivation of vascular tissue angiotensin I (AI) to angiotensin II (AII) conversion over time in patients with chronic heart failure (CHF) treated with chronic angiotensin converting enzyme (ACE) inhibitors is due in part to the tissue binding avidity of the ACE inhibitor used.
Background: Vascular tissue AI/II conversion has been shown to reactivate over time in patients with CHF on chronic lisinopril therapy, a moderately tissue bound ACE inhibitor. We therefore studied CHF patients on chronic lisinopril versus ramipril which by contrast is a highly tissue bound ACE inhibitor.
Methods: Over 18 months, we followed 30 patients with CHF due to left ventricular systolic dysfunction. 15 were randomised to lisinopril and 15 to ramipril therapy. Vascular tissue AI/II conversion was studied using sequential infusion of inert AI and vasopressive AII into the brachial artery. The response was assessed through forearm venous occlusion plethysmography at baseline, 9 and 18 months, after an initial run in period of 2 months. The mean daily dose of lisinopril used was 19.3 mg versus 10 mg of ramipril. The average duration of ACE inhibitor therapy prior to the study was 2.9 years versus 3.3 years respectively. The mean NYHA class was 1.9 in the lisinopril group and 2.0 in those treated with ramipril.
Results: Vascular tissue AI/II conversion was not significantly different at 18 months compared to baseline (p = 0.763) in the lisinopril versus the ramipril treated groups. Furthermore, there was no significant evidence of vascular ACE reactivation in either group, as previously seen in patients with chronic heart failure. The percentage change in forearm blood flow (FBF) in response to AI infusion was non-significant in both the lisinopril (p = 0.461) and ramipril (p = 0.232) groups at 18 months compared to baseline. Forearm blood flow response to AII infusion was unchanged in both groups over the course of the study.
Conclusions: The previously observed reactivation of vascular ACE over time on ACE inhibitors appears no longer to be seen. This could be because of the newer treatments often used in CHF such as beta blockers, spironolactone or statins, all of which can influence vascular ACE indirectly.
heart failure; ACE; reactivation
269 THE EFFECT OF BLOOD PRESSURE REDUCTION ON RENAL FUNCTION IN PATIENTS WITH ESSENTIAL HYPERTENSION
S. Lim, J. Patel, G. Lip. City Hospital, Birmingham, UK
Background: The relation between raised arterial blood pressure and renal impairment is well documented. However, the nature of this relation between blood pressure and renal function in patients with essential hypertension without pre-existing renal disease is controversial. While some cohort studies showed that elevated blood pressure at baseline predicted the development of renal failure, the lack of blood pressure measurements in the intervening years is clearly a limitation. In this study, we hypothesised that blood pressure on treatment is not associated with the decline in renal function in patients with essential hypertension without pre-existing renal disease.
Abstract 269
Comparison of estimated ICERs for ezetimibe vs statin (in £000s)
Methods: We tested this hypothesis in a cohort study with yearly measurements of blood pressure and renal function over 5 years. Renal function was estimated from serum creatinine using the Cockroft-Gault formula—estimated glomerular filtration rate (eGFR). We excluded patients with known renal disease or eGFR of less than 60 ml/min at baseline. Patients with secondary or malignant hypertension were excluded. We divided patients into Group I (eGFR>90 ml/min) and Group II (61–90 ml/min).
Results: We recruited 314 patients, 111 in Group I and 203 in Group II (table). There was no difference in the two groups by gender, ethnicity, diabetes and smoking history. Baseline eGFR correlated significantly with diastolic blood pressure, serum triglycerides, but inversely related to HDL cholesterol and pulse pressure (all p<0.01). Only pulse pressure was significantly associated with baseline eGFR on regression analysis (p = 0.006). At follow-up, there was a significant and sustained reduction in blood pressure with treatment in both groups (p<0.001) and improvements in serum cholesterol, triglycerides and HDL cholesterol with statin therapy (table). Renal function declined in both groups with no significant difference in the change in eGFR relative to baseline between the groups. On linear regression analysis in a model that included variables independent of each other (ie, model A included systolic, model B included diastolic and model C included pulse pressures respectively) and variables independent of the eGFR equation, there was no significant association between blood pressure (systolic, diastolic or pulse pressure) and the change in eGFR. Indeed, none of the blood pressure or metabolic variables independently predicted the change in eGFR on follow-up.
Conclusion: On-treatment blood pressure was associated with eGFR but did not predict the decline in renal function. Hence, our data support an associative but not a causative relationship between blood pressure and renal function in patients with essential hypertension without pre-existing renal disease.
hypertension; renal function; glomerular filtration rate
270 PATIENTS WITH HEART FAILURE AND CHRONIC OBSTRUCTIVE PULMONARY DISEASE MAY BE INAPPROPRIATELY DENIED BETA-BLOCKERS
N. Hawkins1, S. Jenkins1, M. MacDonald2, J. McMurray3, F. Dunn1. 1Stobhill Hospital, Glasgow, UK; 2Glasgow Royal Infirmary, Glasgow, UK; 3Western Infirmary, Glasgow, UK
Background: Chronic obstructive pulmonary disease (COPD) is a frequent comorbidity in heart failure (HF) and a perceived contraindication to β-blockade. We examined the prevalence of severe COPD, and the extent to which β-blockade is inappropriately withheld.
Methods: We reviewed discharge summaries, pulmonary function tests (PFTs) and echocardiograms of 449 consecutive ICD10 coded HF admissions to a large urban hospital. Miscoding, re-admissions, and patients with preserved systolic function were excluded (n = 24, 108 and 55 respectively). COPD severity was classified using Global Initiative for Chronic Obstructive Lung Disease guidelines.
Results: Seventy five of 262 patients (29%) had a physician diagnosis of COPD; PFTs were measured in 53 (71%). 41% of the 75 patients with COPD received β-blockers. In 19%, β-blockers were contraindicated or considered inappropriate for reasons other than COPD—these included bradycardia, conduction disturbance, hypotension, severe peripheral arterial disease or advanced malignancy and dementia. The remaining 40% did not receive β-blockers. 13% had severe airflow obstruction (fig). 27% had milder obstruction or no documented PFTs and may have been inappropriately denied treatment with a β-blocker.
Conclusion: Patients with HF and COPD often tolerate or have alternative reasons precluding β-blockade. Only a minority have severe airflow obstruction. Many of the remainder have β-blocker therapy inappropriately withheld.
heart failure; pulmonary function; beta-adrenergic receptor blockers
271 MEASURING RESPONSE TO CLOPIDOGREL IN PATIENTS UNDERGOING CORONARY INTERVENTION: A COMPARISON OF TWO METHODS
R. Good1, A. McGarrity1, H. Miller1, T. James2, A. McConnachie3, W. Hillis1, A. Goodall2, K. Oldroyd1. 1Western Infirmary, Glasgow, UK; 2University of Leicester, Leicester, UK; 3University of Glasgow, Glasgow, UK
Background: Individual variation in response to clopidogrel has been demonstrated and there is evidence that this may influence outcome following coronary intervention, including stent thrombosis. There is no “gold standard” method to assess this variation but phosphorylation of vasodilator stimulated phosphoprotein (VASP-P) is thought to directly reflect inhibition of the platelet P2Y12 receptor, the target of clopidogrel. However, if clinical decisions are to be made in the acute setting a rapid and reliable point-of-care assay is required.
Methods: We compared the flow cytometric assessment of VASP-P (Biocytex, France) with a novel point-of-care assay (VerifyNow P2Y12, Accumetrics, USA) for the assessment of clopidogrel response in 201 patients undergoing coronary intervention. Blood was collected in 3.2% sodium citrate, from patients immediately prior to coronary intervention. All patients were taking aspirin 75 mg/day and had been loaded with clopidogrel 600 mg at least 2 h before sampling. None of the patients had received GpIIbIIIa inhibitors within 14 days. In a subset of 54 patients, baseline samples were obtained prior to clopidogrel loading.
Results: In patients established on clopidogrel therapy, VASP-P Platelet Reactivity Index (PRI %) ranged from 0–90.6% (mean 55.4%) and VerifyNow P2Y12 %inhibition ranged from 1–97% (mean 43.9%.) Correlation between the assays was good (r = 0.71) (fig 1). Baseline testing of 54/201 patients confirmed that 90% of patients show a response to clopidogrel therapy (fig 2). Furthermore, in these assays, baseline platelet ADP response did not predict the extent of platelet inhibition by clopidogrel.
Conclusion: Both assays confirm a wide variation in individual response to clopidogrel and good correlation. However, before being incorporated into clinical practise, the ability of these assays to predict clinical outcome needs to be assessed.
clopidogrel; coronary artery disease; coronary artery stenting
272 EVALUATION OF THE INTRODUCTION OF ANTI-PLATELET CARDS FOR PATIENTS POST-PERCUTANEOUS CORONARY INTERVENTION
A. Pottle, J. Breen, T. Joseph, S. King. Harefield Hospital, Harefield, UK
Introduction: Percutaneous coronary intervention (PCI) and insertion of a stent or stents is now a frequently used treatment for the management of obstructive coronary disease. Dual anti-platelet therapy is required both pre and post procedure for the prevention of stent thrombosis and this is generally managed with a combination of aspirin and clopidogrel. The duration of treatment after stent placement is dependant on the type of stent used and whether the patient is treated routinely or as an emergency. In our institution dual anti-platelet therapy is recommended for 4 weeks after bare-metal stent placement (1 year after acute coronary syndrome (ACS) or ST segment elevation myocardial infarction (STEMI)), and 1-year after drug eluting stent placement.
Background: There have been previous reports of patients suffering from acute stent thrombosis caused by premature cessation of dual anti-platelet therapy. To reduce the risk of this and in an effort to improve the compliance and knowledge of patients regarding their drug therapy, we decided to produce “anti-platelet cards” to be given to the patients pre-discharge.
Methods: Two anti-platelet cards were created—one for bare metal stents and the other for drug eluting stents. Each contains patient demographic data, the date the stent was inserted and the minimum length of time that dual anti-platelet therapy should be continued. Hospital contact details are also on the cards. The relevant card is given to the patient before discharge by one of the cardiology nursing team. Patients are advised to carry the card with them at all times. The cards were introduced on 1 August 2006. A prospective audit was then carried out for 3 months from September 2006 in the outpatient clinic at the first visit 4–6 weeks post-procedure to evaluate the use of the cards.
Results: Ninety patients were reviewed at the 4–6 week appointment in the nurse-led post PCI clinic. In 75 patients (83%), it was documented in the notes that the anti-platelet card had been given to the patient. 73 patients (81%) had the card with them at the clinic visit. 7 patients said they had a card but had left it at home (8%), 3 patients had completed their course of clopidogrel and no longer carried the card. Four patients had never received an anti-platelet card. In a further 3 cases there was no documentation on the audit as to whether the patients had a card or not.
Conclusions and Implications: A total of 92% of patients in this audit still had the anti-platelet card at the first clinic visit or had carried the card for the prescribed period of time (3 patients had completed the 4 week course of clopidogrel when seen in clinic). Patients were aware of the need to continue to carry the card and the importance of continuing dual anti-platelet therapy for the prescribed period of time. It is hoped that the use of these cards will help prevent patients stopping treatment prematurely.
anti-platelet; stent; nurse-led care
273 LEFT ATRIAL REMODELLING AND REGIONAL DEFORMATION IN MILD TO MODERATE HYPERTENSION
A. Baltabaeva1, M. Marciniak2, B. Bijnens1, F. He2, T. Antonios2, G. MacGregor2, G. Sutherland1. 1St George’s Hospital, London, UK; 2St George’s University London, London, UK
Objectives: To quantify changes in left atrial (LA) volume (LAV) and strain/rate (S/SR) during cardiac cycle and relate these to changes induced by increased afterload and left ventricular filling pressure (LVFP) in mild to moderate hypertension (MMH).
Background: Changes in LAV and contractility, resulting from raised LVFP in hypertension, have currently no standard quantitative indices. Regional LA deformation parameters assessed by tissue Doppler derived S/SR imaging are feasible and provide a quantitative measure of LA deformation.
Methods: In 74 hypertensive individuals and 34 age-matched normotensive subjects (mean age 49 (1.4) vs 44.2 (2.1) years) echo studies were performed, including measurements of LAV during reservoir, conduit and pump phases and standard indices reflecting LV filling. S/SR was measured in the lateral LA wall. Total deformation (S TOTAL) and the contribution to early (S E-index) and late (S A-index) filling were calculated.
Results: Hypertensives had significantly increased LAV during all phases. Only LAV CONDUIT was significantly correlated both with ventricular hypertrophy and parameters of diastolic function. Significant increase in regurgitant volume into pulmonary veins (PV REVERS) in hypertensives correlated with BP and LAV CONDUIT. In hypertensives S TOTAL was significantly higher (54.9 (2.6) vs 45.5 (2.7)%, p<0.03) and S E-index was lower (p<0.001). This was compensated for by an increased S A-index (p<0.001) and SR during atrial contraction (−4.9 (0.2) vs −2.9 (0.3) 1/s, p<0.001). S A-index correlated significantly with BP (r = 0.4; p<0.001) and PVREVERS (r = 0.3; p<0.001).
Conclusions: LAV CONDUIT reflects best changes in LA function due to raised LVFP. Hypertensive atrial dilatation is related to increase in PV REVERS. LA S/SR offers a clinically valuable approach to detecting subclinical atrial dysfunction in MMH.
hypertension; atrial remodelling; strain imaging
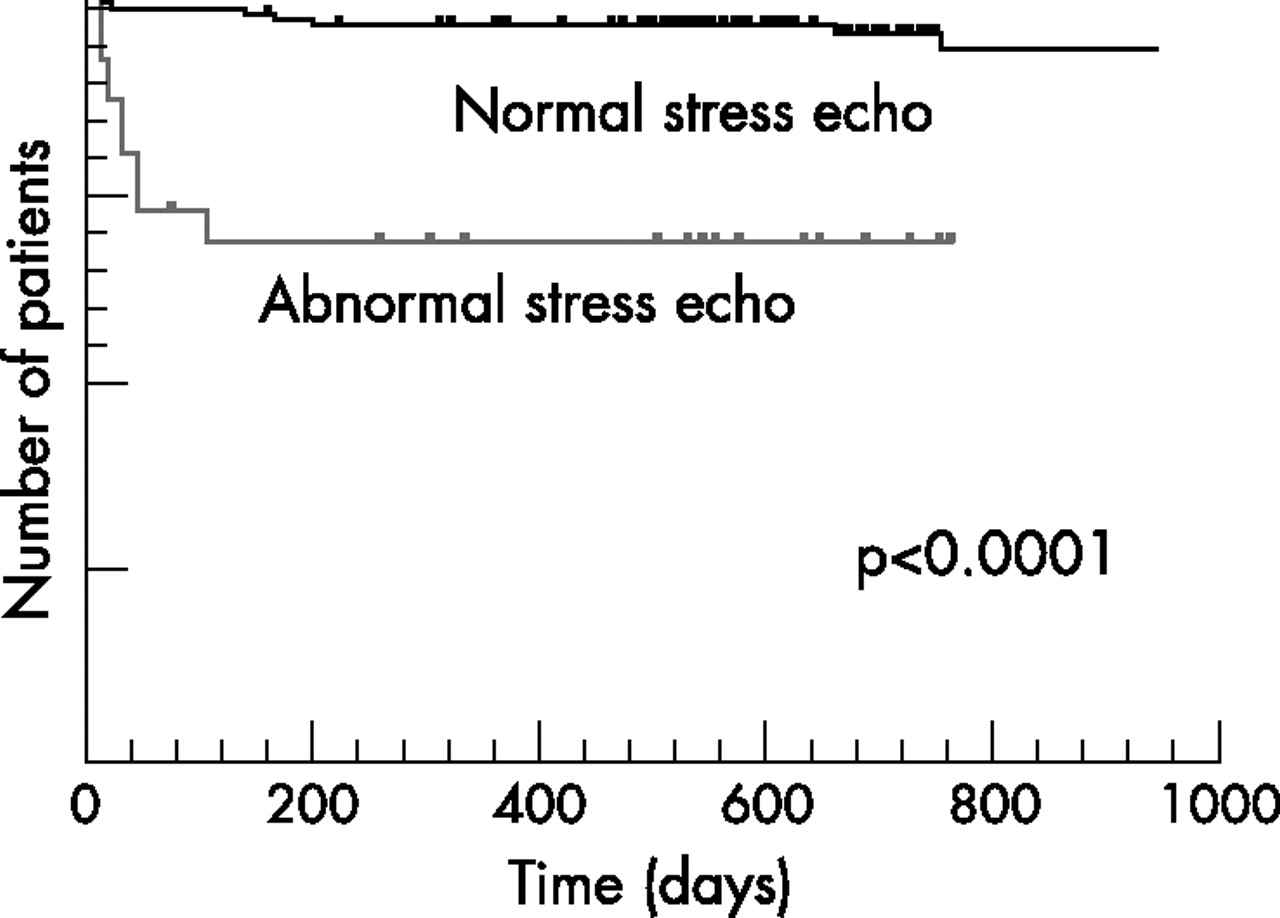
Abstract 012.

Abstract 013.

Abstract 014.

Abstract 017.

Abstract 018.
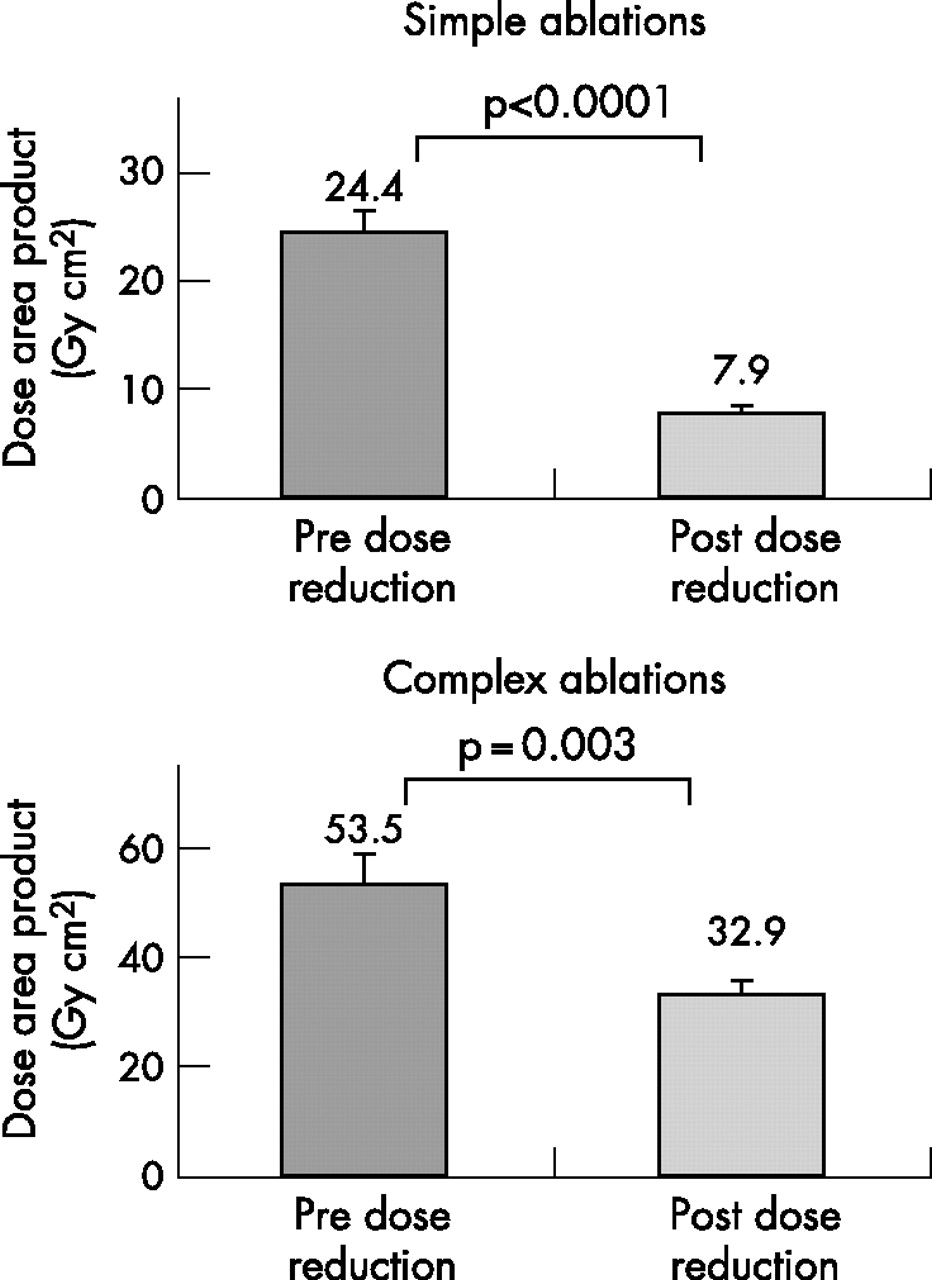
Abstract 027.
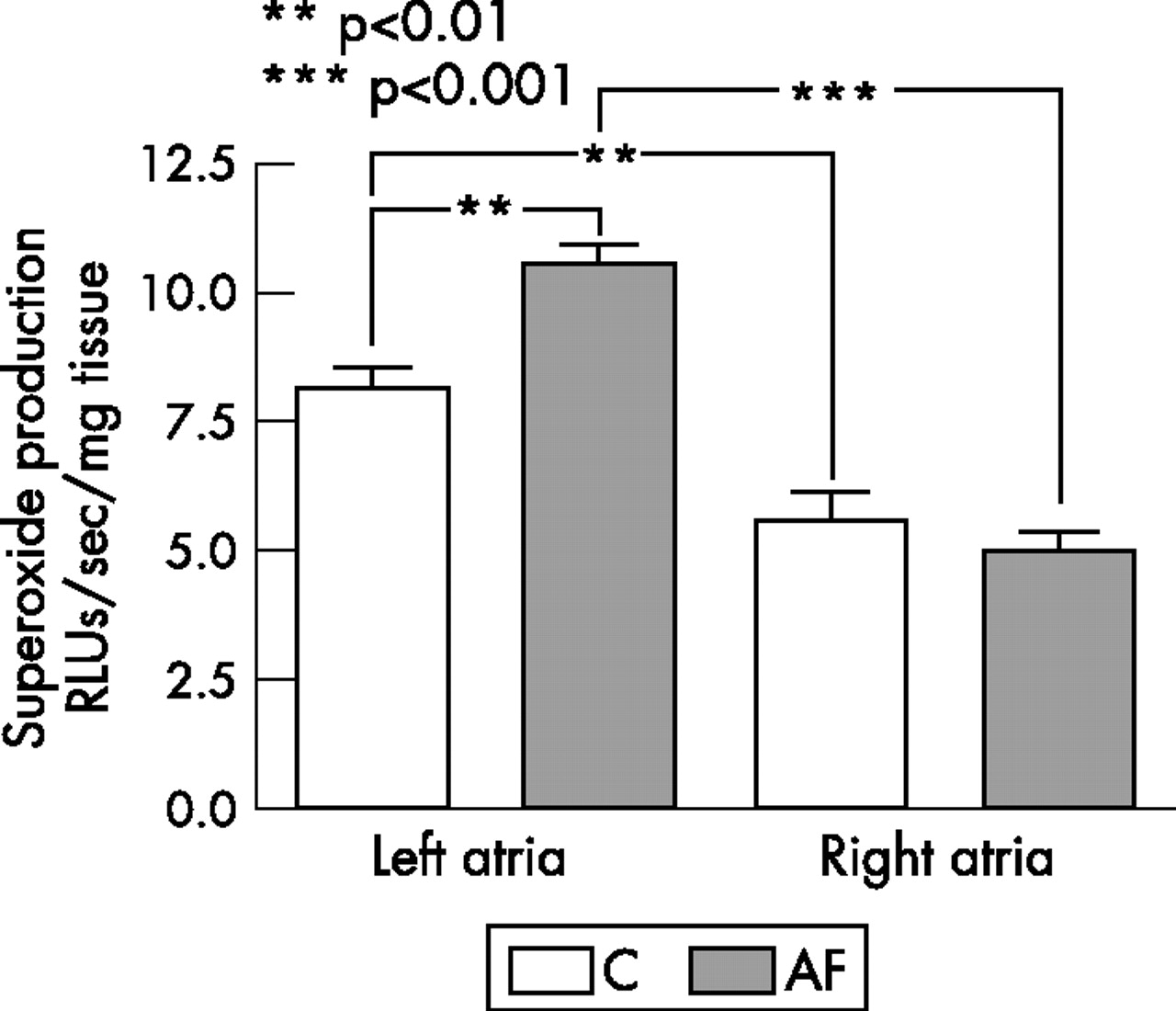
Abstract 033.

Abstract 044 Figure 1.

Abstract 044 Figure 2.

Abstract 048.

Abstract 053 Figure 1.

Abstract 053 Figure 2.
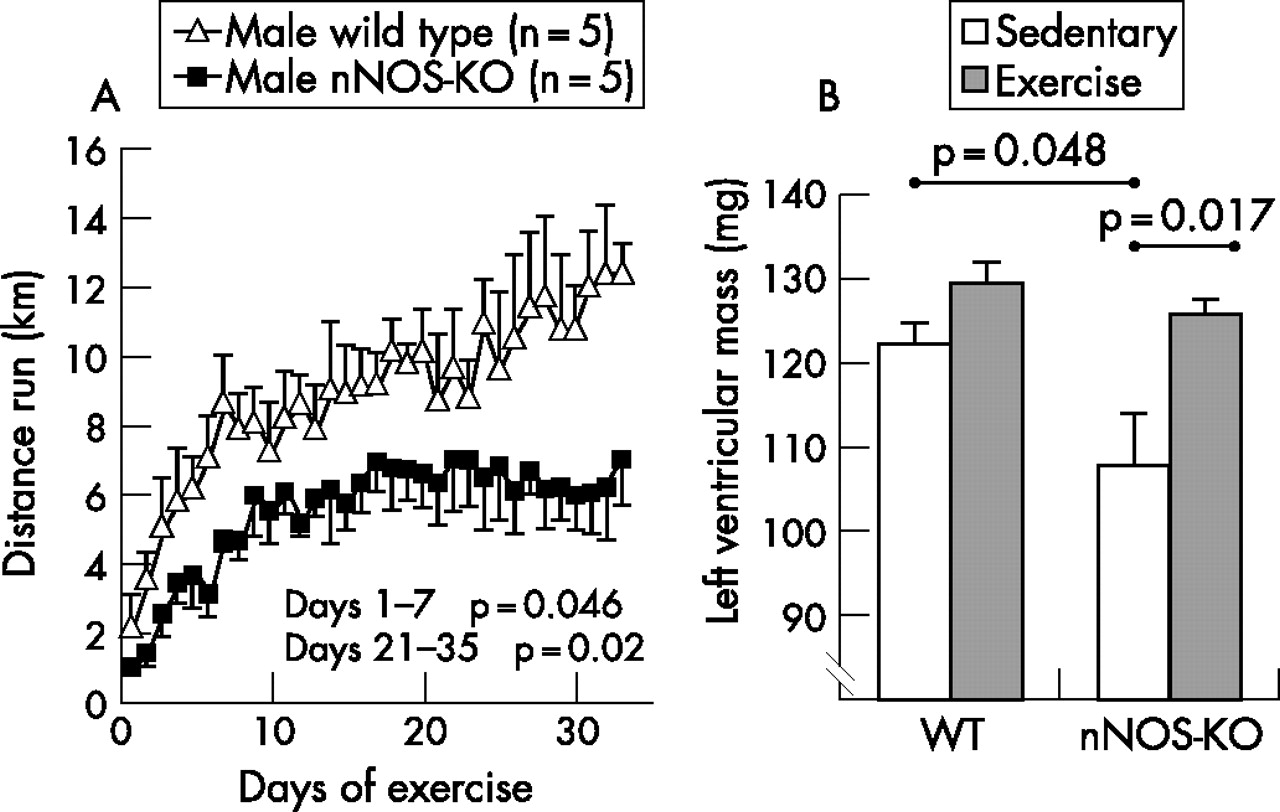
Abstract 056 (A) Daily distance run by trained animals: male nNOS-KO 6.5 km (1.0), male WT 11.3 (1.3), n = 5–6 per group; p = 0.02. (B) LV mass: sedentary WT 122 (2) mg; exercise WT 129 (2) mg, p = 0.059.

Abstract 078.

Abstract 082.

Abstract 085.
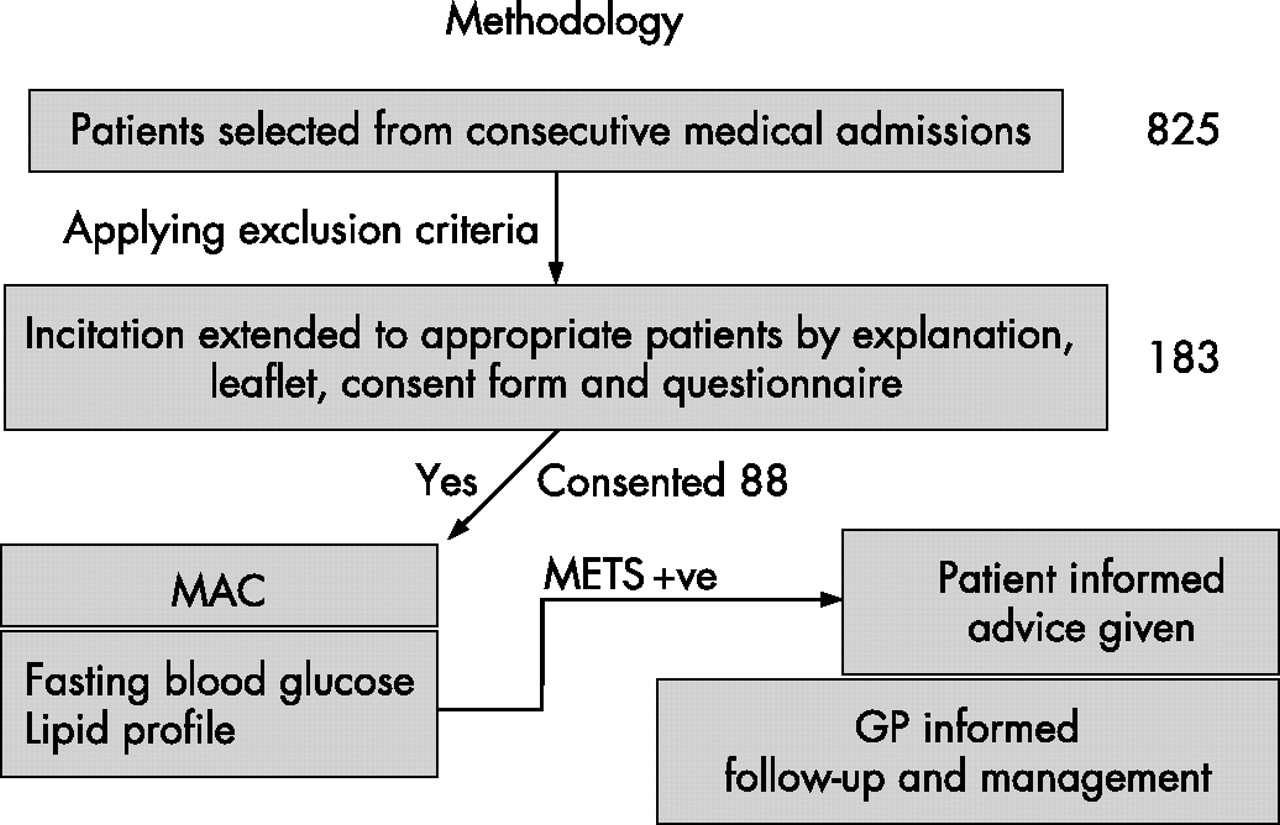
Abstract 084.

Abstract 088 Figure 1.
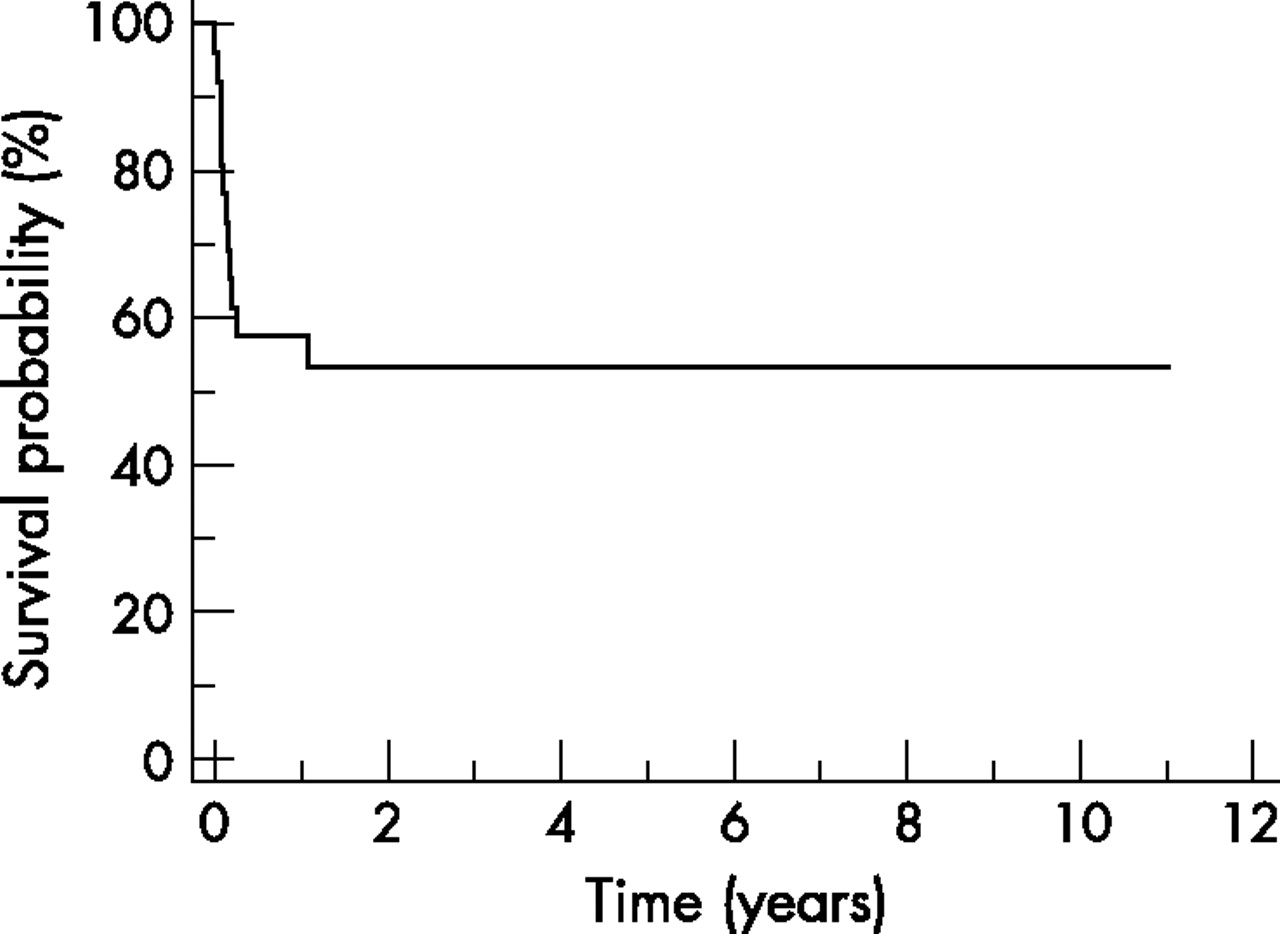
Abstract 088 Figure 2.

Abstract 091.
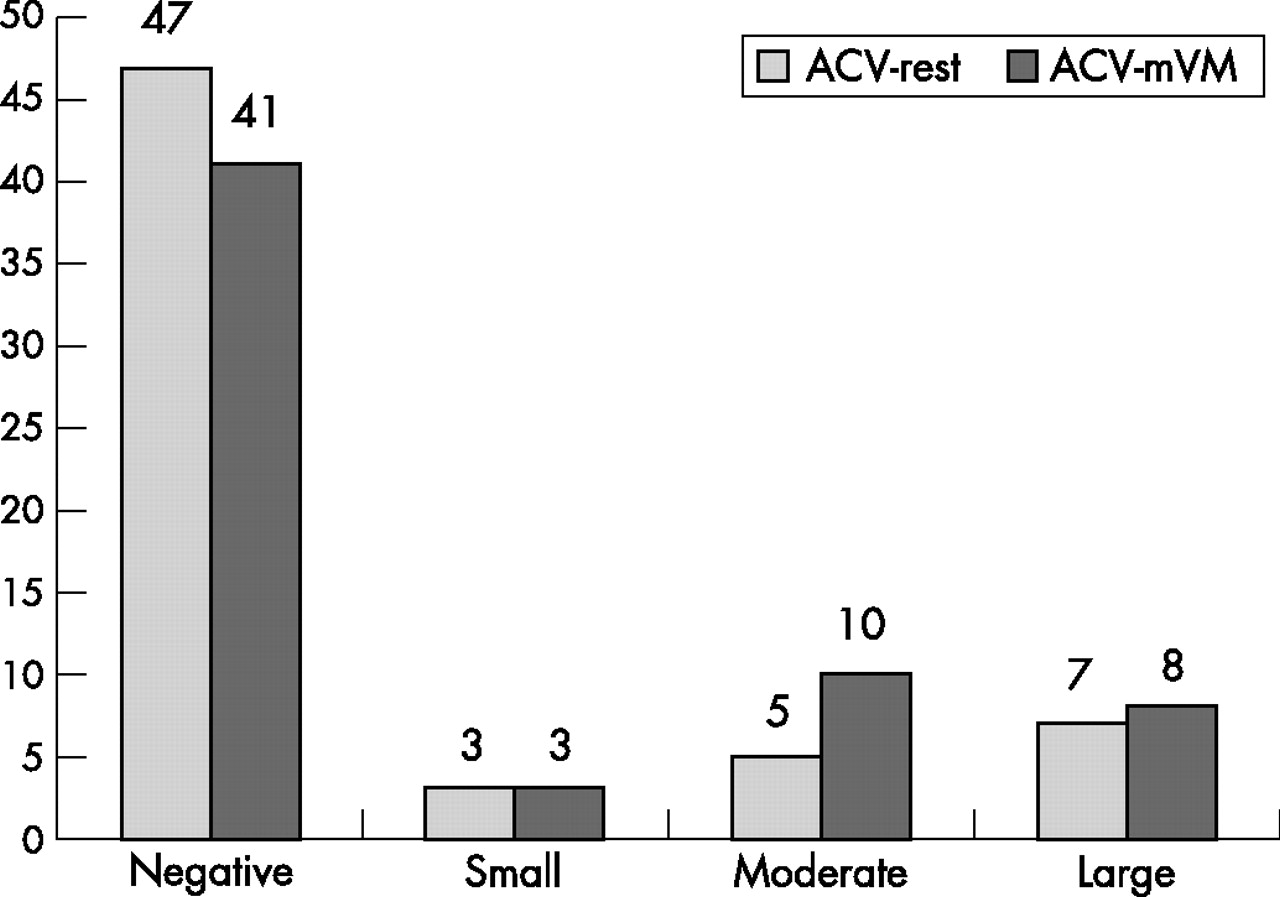
Abstract 094 Figure 1 Effect of mVM on PFO detection with antecubital (AV) administration of contrast.

Abstract 094 Figure 2 Effect of mVM on PFO detection with femoral (FV) administration of contrast.

Abstract 106 Two year all-cause mortality hazard ratios associated with secondary prevention agent usage in groups with and without diabetes mellitus. Hazard ratio is displayed as logarithmic value. ACEi refers to ACE inhibitor use.

Abstract 109 Figure 1.

Abstract 109 Figure 2.

Abstract 113.

Abstract 120 Figure 1.

Abstract 120 Figure 2.

Abstract 124.

Abstract 126.

Abstract 128 Figure 1.

Abstract 128 Figure 2.

Abstract 129 Figure 1.

Abstract 129 Figure 2.

Abstract 130.

Abstract 135.

Abstract 138.

Abstract 139.

Abstract 140.

Abstract 141.

Abstract 142 Figure 1.

Abstract 142 Figure 2.

Abstract 144.

Abstract 146 Figure 1 Top: Left anterior oblique (LAO) view of 3D volume rendered image of the heart, left atrium (shaded), thoracic spine and fossa ovalis marker sphere (white dot). Bottom: corresponding fluoroscopic image of the transseptal sheath (TS) at the level of the fossa ovalis.

Abstract 146 Figure 2 Top: Right anterior oblique (RAO) view of 3D volume rendered image of the heart, left atrium (shaded), thoracic spine and fossa ovalis marker sphere (white dot). Bottom: corresponding fluoroscopic image of the transseptal sheath (TS) at the level of the fossa ovalis.

Abstract 148 Figure 1.

Abstract 148 Figure 2.

Abstract 149 Example images from 3 patients showing (A) left marginal vein; (B) coronary sinus; (C) anterior interventricular vein.

Abstract 150 Figure 1 Targeted MRI coronary angiography sequences from three patients.

Abstract 150 Figure 2 3D and multiplanar reconstructions of the WHCA data set. The anomalous left main stem (arrow) arises with the right coronary and runs between the aorta (Ao) and RVOT.

Abstract 154.

Abstract 164 Figure 1.

Abstract 166 Figure 2.

Abstract 166 Figure 1.

Abstract 166 Figure 2.

Abstract 167.

Abstract 169.

Abstract 179 Figure 1.

Abstract 179 Figure 2.

Abstract 180.

Abstract 187 Figure 1.

Abstract 187 Figure 2.

Abstract 190 Figure 1.

Abstract 190 Figure 2.

Abstract 198.

Abstract 199 Figure 1.

Abstract 199 Figure 2.

Abstract 200.

Abstract 216.

Abstract 221 *p<0.01 vs baseline; **p = 0.0015 vs SIM.

Abstract 224.

Abstract 225.

Abstract 233 Mortality risk comparing gender groups across glycaemic range.

Abstract 234 Group survival. Kaplan–Meier survival curves for cohorts with and without diabetes in 1995 and 2003. Highlighted area represents the temporal improvement in survival.

Abstract 238 Figure 1.

Abstract 238 Figure 2.

Abstract 238 Figure 3.

Abstract 243.

Abstract 249 Examples of short axis LGE-CMR in three separate patients. The white asterix shows normal myocardium; solid black arrows indicate infarcted (hyper-enhanced) myocardium; solid white arrow indicates microvascular obstruction as a black core within an area of hyperenhancement. (A) Anteroseptal infarction (white) of the endocardium with some sparing of the epicardial layer. (B) Transmural inferior myocardial infarction. (C) Transmural infarction of the anterior and septal myocardial walls with evidence of microvascular obstruction.

Abstract 250 Figure 1.

Abstract 250 Figure 2.

Abstract 259 Figure 1.

Abstract 259 Figure 2.

Abstract 270.

Abstract 271 Figure 1.

{kind=link}
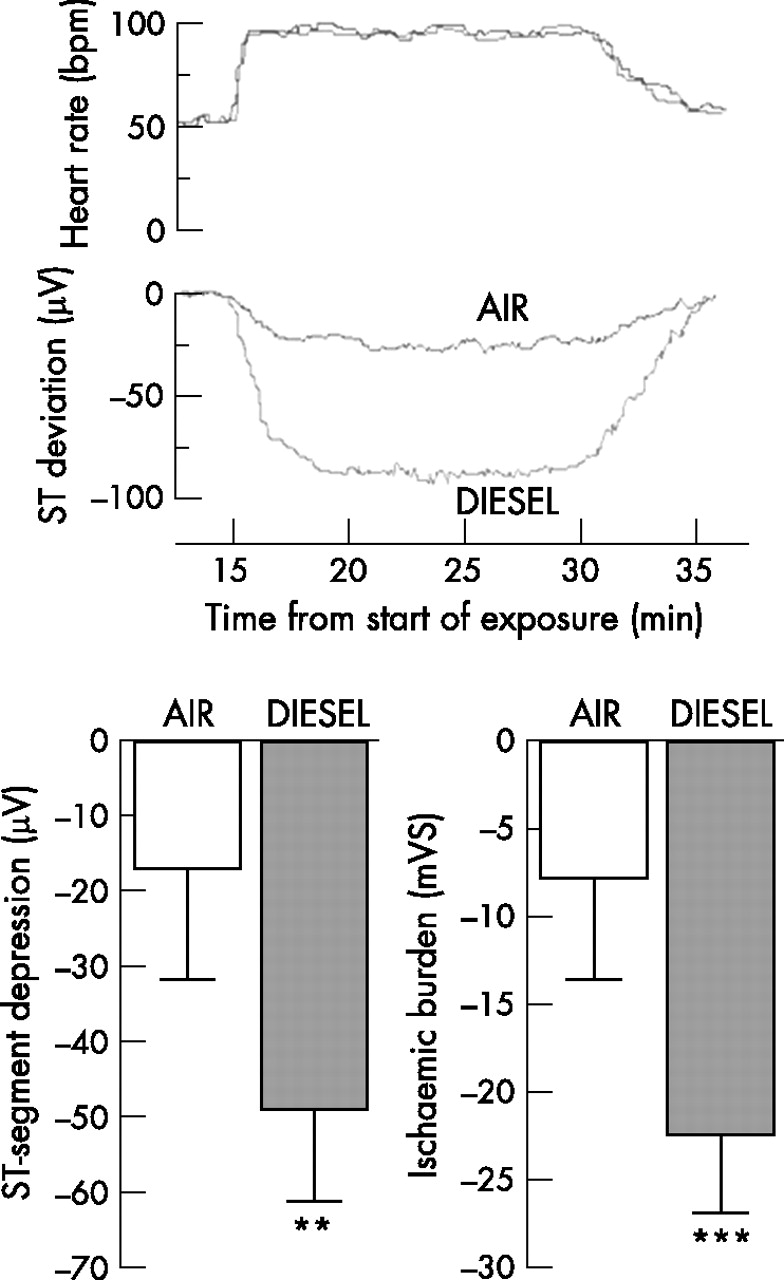{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
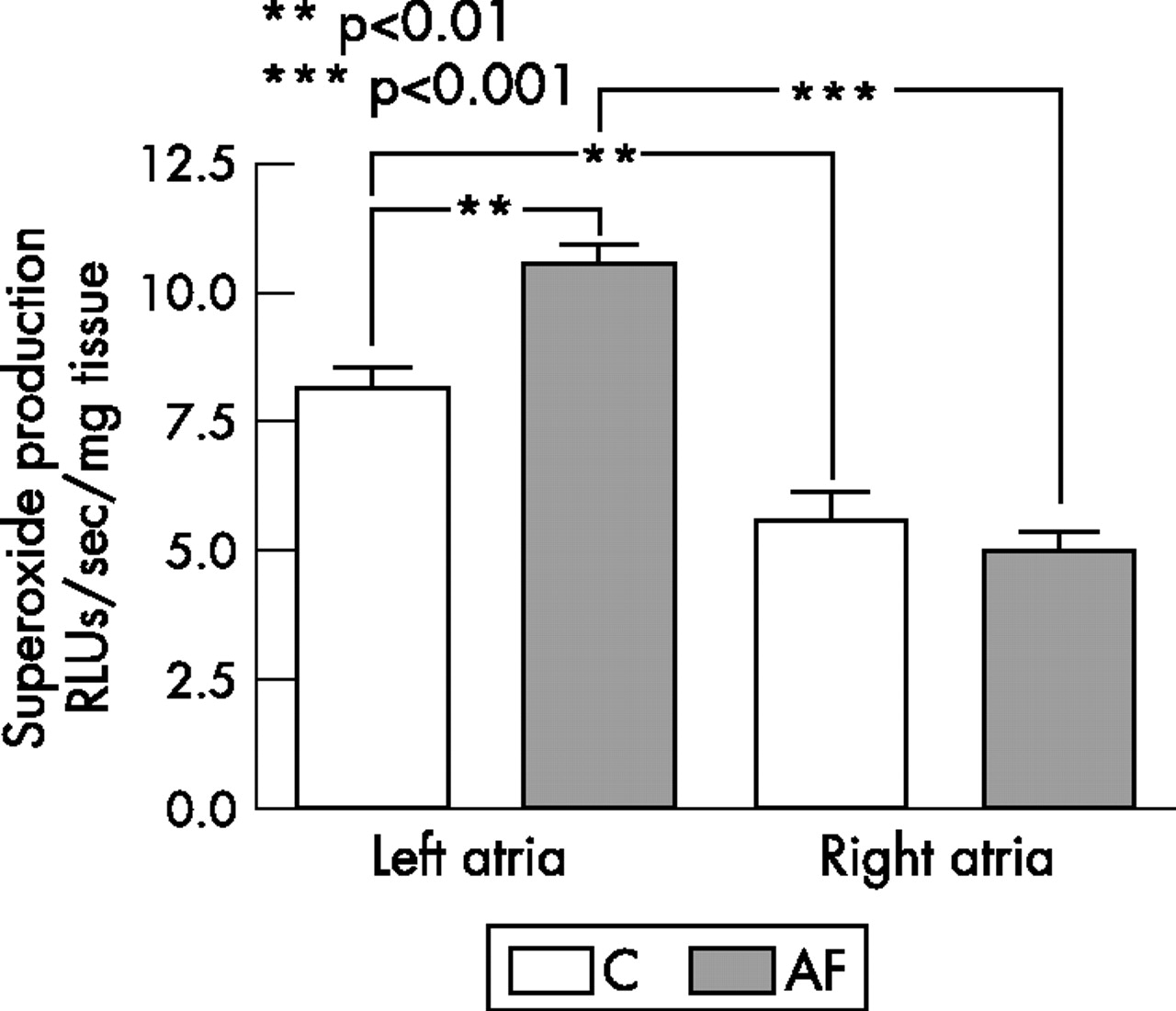{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
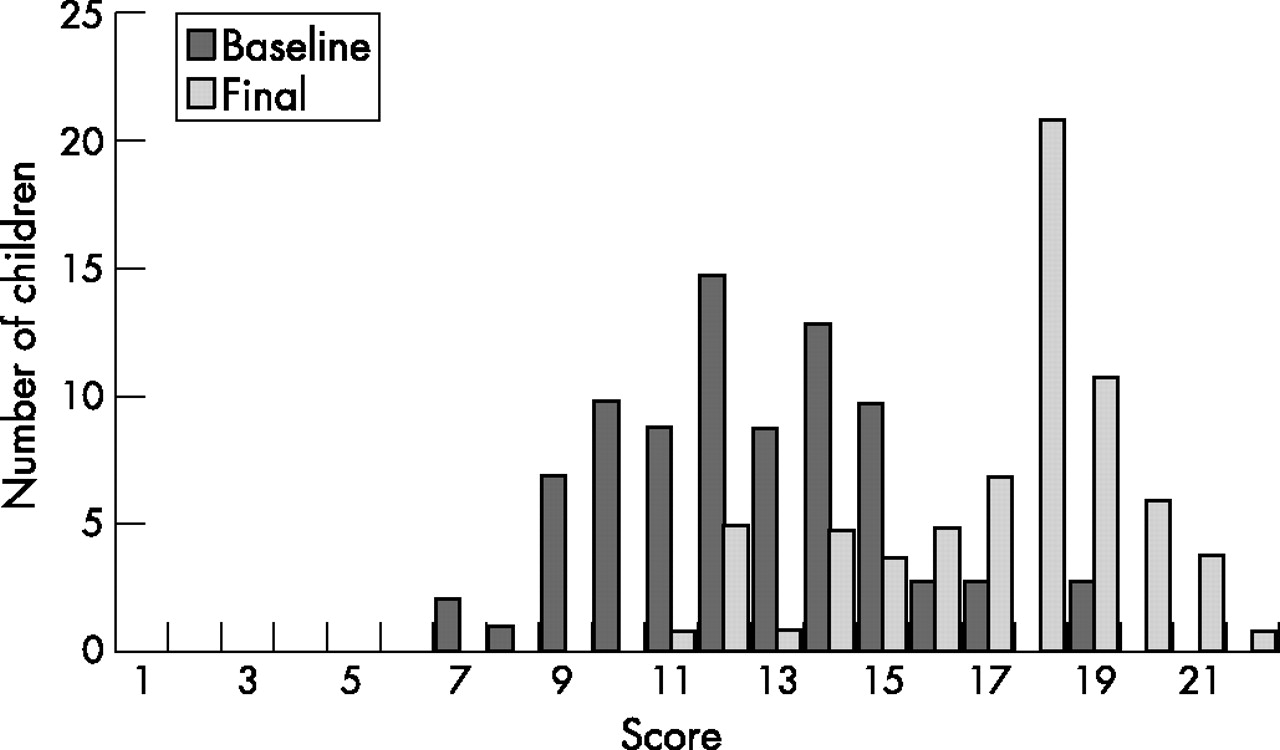{kind=link}
{kind=link}
{kind=link}
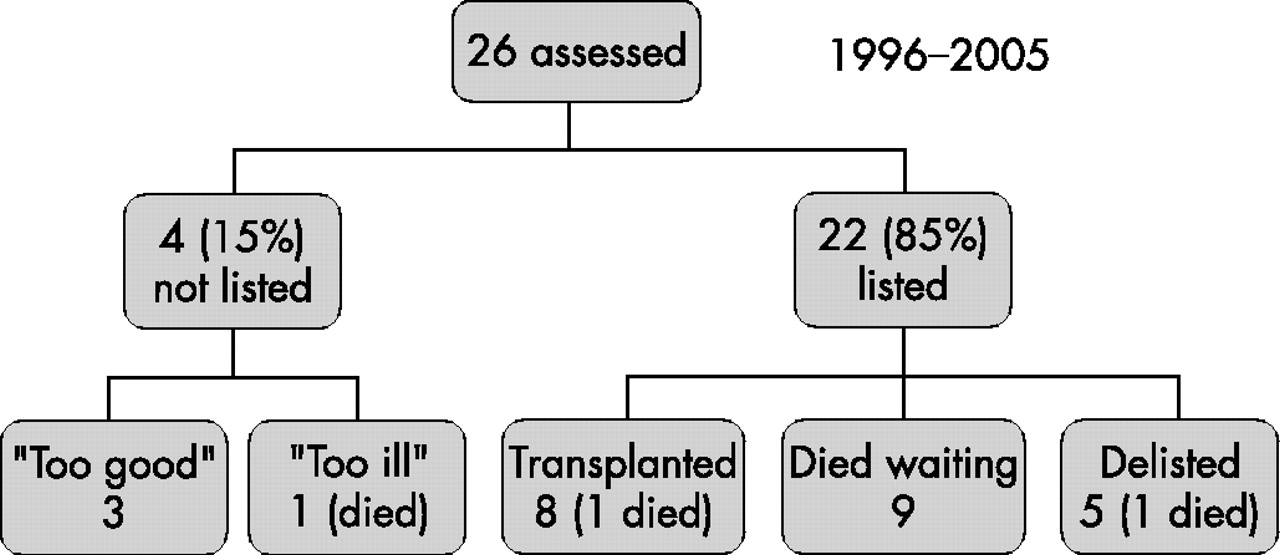{kind=link}
{kind=link}
{kind=link}
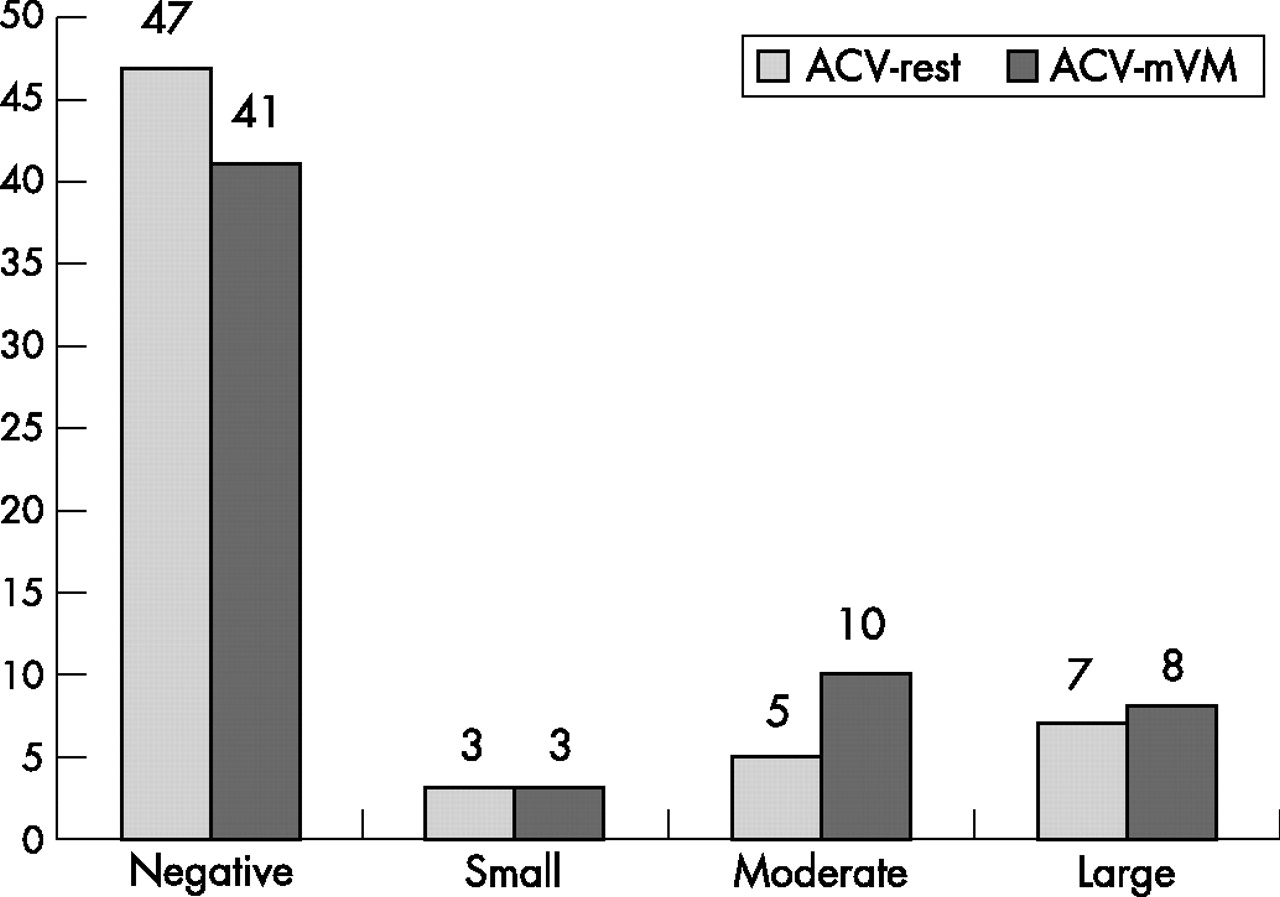{kind=link}
{kind=link}
{kind=link}
{kind=link}
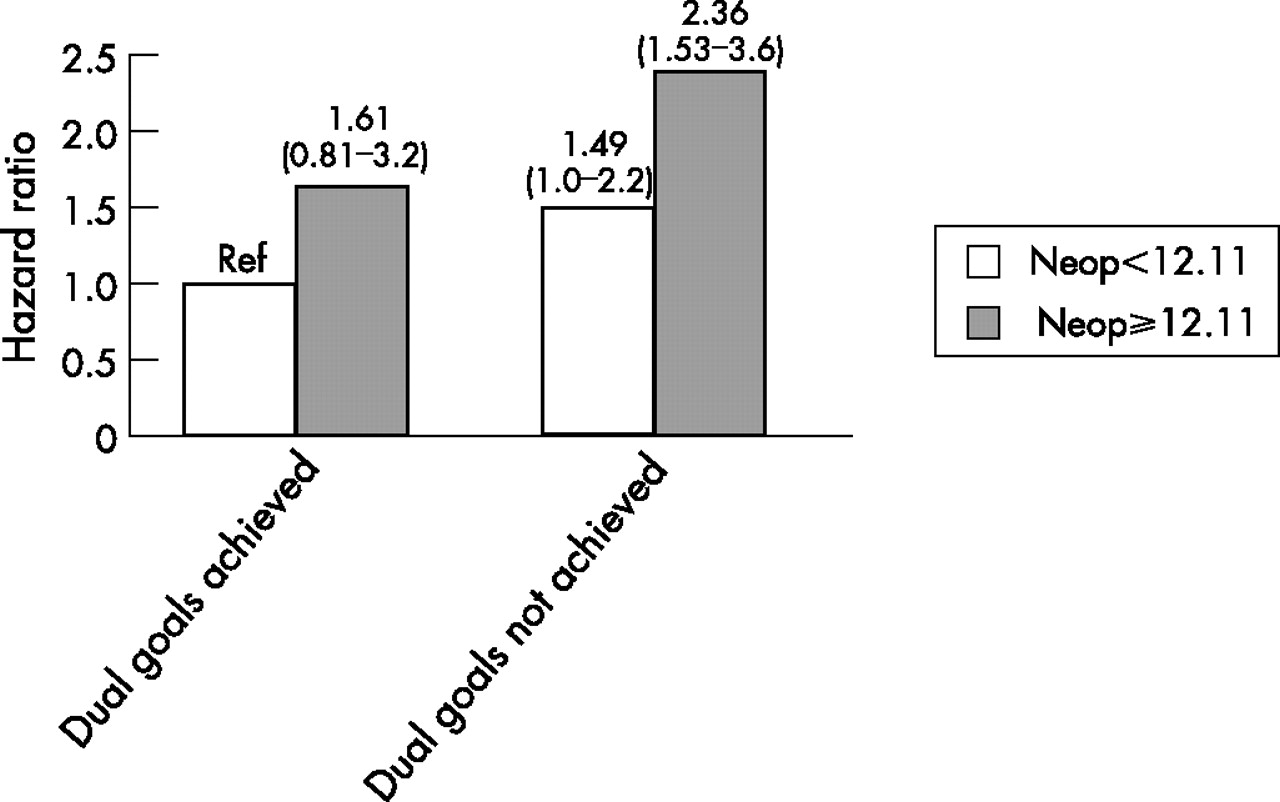{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract 271 Figure 2.