Article Text

Abstract
Objective: To evaluate whether adding comorbid conditions to a risk model can help predict in-hospital outcome and long-term mortality after percutaneous coronary intervention (PCI).
Design: Retrospective chart review
Setting: Academic medical centre.
Patients: 7659 patients who had 9032 PCIs.
Interventions: PCI performed at Mayo Clinic between 1 January 1999 and 30 June 2004.
Main outcome measures: The Mayo Clinic Risk Score (MCRS) and the coronary artery disease (CAD)-specific index for determination of comorbid conditions in all patients.
Results: The mean (SD) MCRS score was 6.5 (2.9). The CAD-specific index was 0 or 1 in 46%, 2 or 3 in 30% and 4 or higher in 24%. The rate of in-hospital major adverse cardiovascular events (MACE) increased with higher MCRS and CAD-specific index (Cochran–Armitage test, p<0.001 for both models). The c-statistic for the MCRS for in-hospital MACE was 0.78; adding the CAD-specific index did not improve its discriminatory ability for in-hospital MACE (c-statistic = 0.78; likelihood ratio test, p = 0.29). A total of 707 deaths after dismissal occurred after 7253 successful procedures. The c-statistic for all-cause mortality was 0.69 for the MCRS model alone and 0.75 for the MCRS and CAD-specific indices together (likelihood ratio test, p<0.001), indicating significant improvement in the discriminatory ability.
Conclusions: Addition of comorbid conditions to the MCRS adds significant prognostic information for post-dismissal mortality but adds little prognostic information about in-hospital complications after PCI. Such health-status measures should be included in future risk stratification models that predict long-term mortality after PCI.
Statistics from Altmetric.com
A third of the population in the USA aged 65–79 years and 70% of the population aged ⩾80 years have at least one comorbid condition.1 Comorbid conditions increase the risk of disability and mortality over and above the risk from individual diseases.2 3 Because patients frequently present with multiple comorbid conditions at the time of percutaneous coronary intervention (PCI) and because technical advances in PCI now allow sicker patients to be treated, it is likely that patients’ comorbid conditions will have greater influence on their long-term outcomes after PCI. As the burden of coronary artery disease (CAD) and revascularisation shifts toward older sections of the population, the assessment of comorbid conditions must be prioritised in the risk assessment models developed for PCI.
Earlier attempts to incorporate this important factor into risk assessment models have been hampered by the lack of uniform definitions of comorbid conditions. The recent development of constructs to define comorbid conditions relevant to patients with CAD may better illuminate the prognostic importance of their presence and severity on the patients’ PCI outcomes.4 At present, however, most risk prediction models that are developed to determine outcome after angioplasty focus on in-hospital complications after PCI.5–10 Lack of inclusion of comorbid illnesses is likely to be a substantial barrier to the further evolution of prognostic models of follow-up events and may limit our ability to inform patients of the expected outcomes after treatment.
There is a critical need for development of models to assess long-term adverse outcomes. Most current models restrict the prediction to either in-hospital or short-term outcomes. We previously developed and validated the Mayo Clinic Risk Score (MCRS), which accurately predicts in-hospital major adverse cardiovascular events (MACE) and contains several variables that are linked to long-term outcomes.8 11 Its value in prediction of long-term outcome has not yet been evaluated. We previously demonstrated significant improvement in the discriminatory ability of the existing prediction models for myocardial infarction (MI) with the addition of comorbid illnesses.12 The aim of the present study was to evaluate the usefulness of the MCRS in prediction of long-term events and whether the addition of comorbid conditions to the MCRS provides additional information to predict in-hospital and long-term mortality in patients undergoing PCI.
PATIENTS AND METHODS
Study group
Since 1979, patients undergoing PCI at the Mayo Clinic have been prospectively enrolled in a longitudinal follow-up registry. Patients in this registry have undergone follow-up evaluations by trained study coordinators at 6 months, 1 year and then annually after their PCI. For this study, we reviewed 9259 consecutive PCI procedures performed in 7847 patients at Mayo Clinic Rochester between 1 January 1999 and 30 June 2004. One hundred and eighty-eight patients with 227 procedures did not allow research use of their records and were excluded, leaving 9032 observations for analysis. The Mayo Clinic Institutional Review Board approved the study.
Quantifying comorbid conditions
Information on comorbid conditions was collected at the time of the index PCI and was abstracted from the patients’ medical records for this study. The method for developing the CAD-specific index has been previously described.4 Briefly, the CAD-specific index was developed to assess and determine the prognostic influence of comorbid conditions, from a cohort of 1471 patients with CAD who underwent coronary angiography between 1985 and 1989 and were followed up through 2000 in the Duke Databank for Cardiovascular Diseases. After the final model was determined, a weight for each comorbid condition was derived using the log hazard ratios from the model (table 1). A weight of 2 was assigned to diabetes mellitus and weights for the other conditions were calculated relative to diabetes and rounded to the nearest integer. Weight 1 was given to current smoker, hypertension, or history of stroke or transient ischaemic attack (TIA); weight 2 corresponds with diabetes mellitus, chronic obstructive pulmonary disease, peripheral vascular disease, tumour, lymphoma, or leukaemia. Weight 3 was given to patients with diabetes mellitus with sequelae, 5 to metastatic solid tumour and 7 to patients with moderate to severe renal disease. In this study we separated the patients into three groups: those with a CAD-specific index score of 0 or 1; those with a score of 2 or 3 and those with a score of ⩾4 (maximum score observed is 21).
Mayo clinic risk score
The MCRS model (table 1) incorporates five clinical variables (older age, non-elective intervention, renal disease, cardiogenic shock and New York Heart Association class III or greater heart failure symptoms) and three angiographic variables (angiographic thrombus, left main coronary artery disease, or multivessel disease) that accurately predict in-hospital complications.8 The weighted integers (range 0–27) group the patients undergoing PCI into different risk categories: 0–5, very low risk; 6–8, low risk; 9–11, moderate risk; 12–14, high risk and ⩾15, very high risk.
Clinical outcomes
In-hospital MACE included death, Q-wave MI, stroke or TIA, or need for emergent coronary artery bypass grafting surgery. TIA was defined as loss of neurological function caused by ischaemia with abrupt onset persisting for ⩽24 h and clearing without residual signs. Stroke was defined as a loss of neurological function caused by an ischaemic event persisting longer than 24 h or leaving residual signs. Diabetes mellitus with sequelae was defined as renal disease, retinopathy, peripheral neuropathy, gastroparesis or peripheral circulatory disease documented in the medical history. Multivessel disease was defined as stenosis of >70% in more than one major epicardial coronary artery or one of their major branches. The only follow-up event documented was time to all-cause mortality, as was used in the original CAD-specific index for comorbid conditions. The follow-up data were censored after the point of last contact. If the presence of a component risk factor was unknown, it was treated as not present.
Patient outcome data were stratified into short-term (in-hospital) and long-term outcomes. We evaluated the influence of comorbid conditions (CAD-specific index) on the ability of MCRS to predict short-term outcome. Furthermore, we investigated (a) whether known determinants of short-term outcome (ie, MCRS) can also provide prognostic information for long-term mortality and (b) whether information about comorbid conditions can provide incremental long-term prognostic information over and above that determined by the factors that predict in-hospital outcome (MCRS).
Statistical analysis
Continuous variables are summarised as means (SD). Discrete variables are presented as frequencies. Because data were missing for some variables, percentages were calculated based on the number of PCIs with information available. Kaplan–Meier methods were used to estimate survival rates during follow-up. The Spearman rank correlation was used to estimate the association between the MCRS and the CAD-specific index. The Cochran–Armitage test for trend was used to evaluate increasing event rates across the risk score indices. Logistic regression models were used to assess associations with in-hospital MACE.
Cox proportional hazards regression models were used to analyse time to all-cause mortality on long-term follow-up among patients with a successful PCI (defined as <50% residual stenosis in at least one treated lesion, with no in-hospital death, Q-wave MI, or coronary artery bypass grafting). Successful PCIs were used because poor long-term outcome is already expected for those with poor short-term outcome—that is, unsuccessful PCI. If patients had multiple successful PCIs within the study period, only the earliest was used for the follow-up analysis of all-cause mortality. The additional prognostic value of the CAD-specific index, when the MCRS was already accounted for, was tested by comparing a model with both scores with the model with the MCRS alone.
RESULTS
The mean (SD) age of 7659 patients undergoing 9032 PCIs was 67 (12) years and 71% were men (table 2). Eighty-two per cent had a history of hyperlipidaemia, 72% had hypertension, 25% had diabetes mellitus (32% of these with sequelae), 3% had renal disease, 11% had congestive heart failure on presentation and 11% had peripheral vascular disease. Sixty-six per cent of PCIs were either urgent or emergent and 51% were multivessel interventions (table 2). All characteristics were similar for the subset of patients with successful PCI.
The MCRS and the CAD-specific index scores (table 1) were determined for each patient at the time of each PCI procedure (n = 9032). The mean (SD) MCRS score was 6.5 (2.9). Thirty-eight per cent of the patients were in the very low MCRS group, 42% were in the low-risk group, 15% had moderate risk, 3% had high risk and 2% had very high risk. Forty-six per cent had a CAD-specific index of 0 or 1, 30% had a score of 2 or 3 and 24% had a score of 4 or higher.
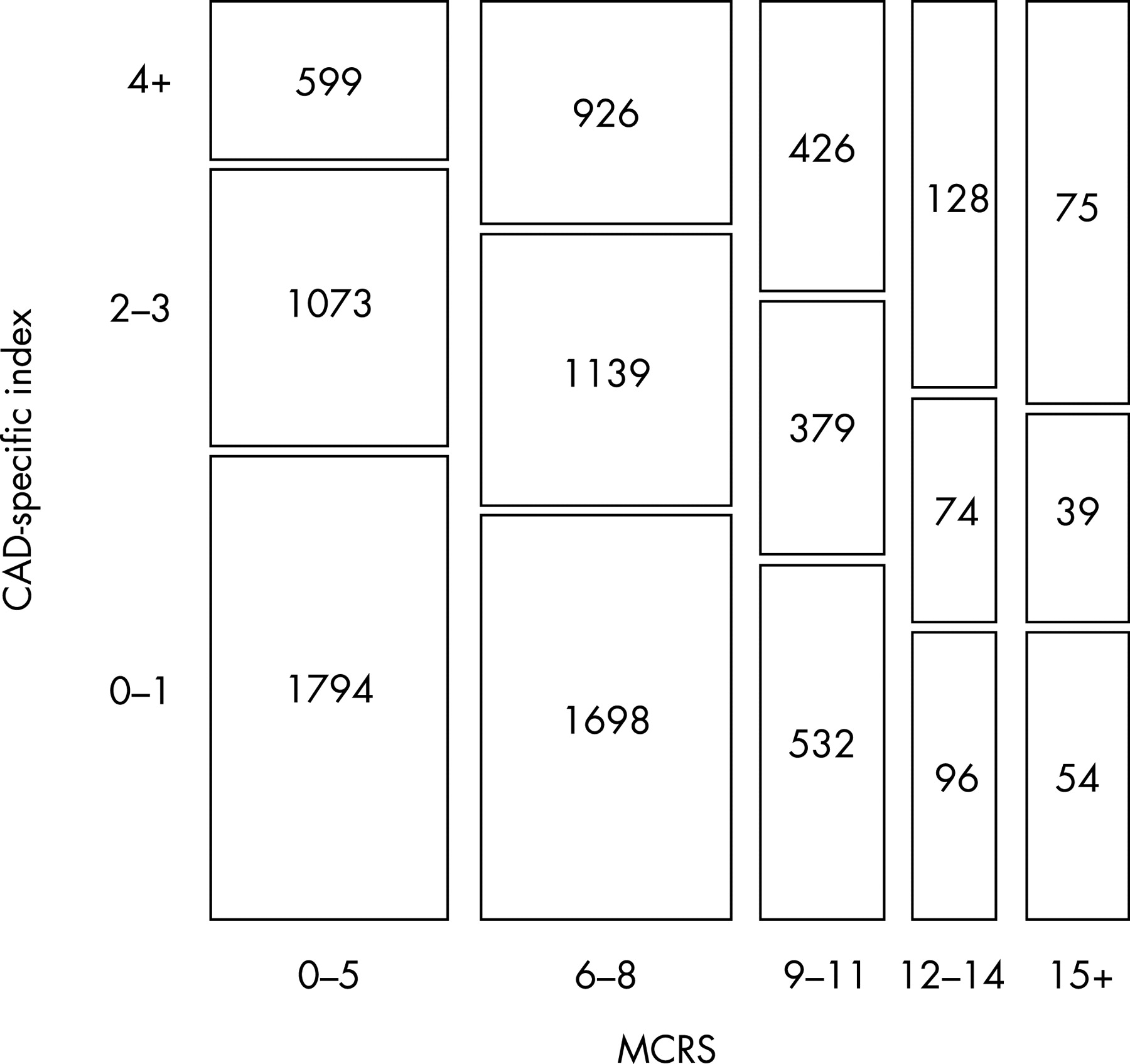
Figure 1 depicts the association of the MCRS and the CAD-specific index. More than half of the patients with a lower MCRS (0–5) had a CAD-specific score of 0 or 1, which indicates few associated comorbid conditions. Only 17% of patients with an MCRS of 0–5 had a CAD-specific index score of ⩾4. In contrast, 44% of patients in the high and very high risk MCRS subgroups had a CAD-specific index of ⩾4, which indicates a higher prevalence of comorbid conditions in the high-risk groups. Patients who were high risk for PCI but with few comorbid conditions had more in-hospital MACE (11/122 (9%)) than patients who were low risk for PCI with several comorbid conditions (0/69 (0%)) (p = 0.01). However, long-term survival is similar between these two groups; 2-year mortality was 6.9% for those high risk for PCI with few comorbid conditions and 5.4% for those low risk for PCI with several comorbid conditions (p = 0.4). Although the prevalence of comorbid conditions was greater with a higher MCRS, the Spearman rank correlation coefficient between the MCRS and the CAD-specific index was low (rs = 0.142), which indicates weak association between the MCRS and the CAD-specific index.
In the cohort, 330 patients (4.3%) had in-hospital MACE. The incidence of MACE increased with higher MCRS and higher CAD-specific index (Cochran–Armitage test for trend, p<0.001 for both models). The c-statistic for the MCRS for in-hospital events was 0.78 (95% CI 0.75 to 0.81). The addition of the CAD-specific index to the MCRS did not improve its discriminatory ability for in-hospital MACE (c-statistic = 0.78, 95% CI 0.75 to 0.81; likelihood ratio test, p = 0.29).
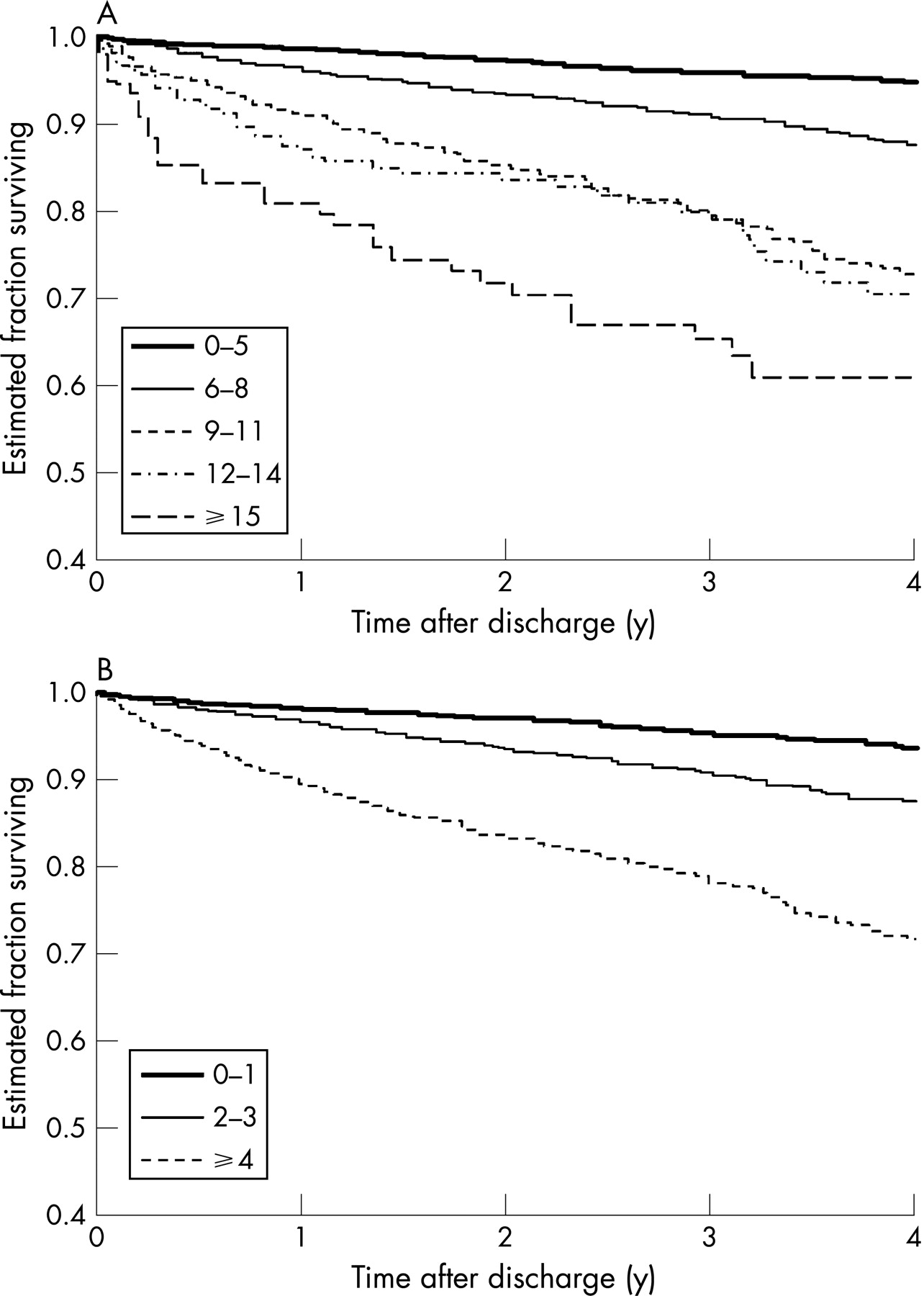
A total of 707 deaths after dismissal occurred in 7253 patients after 7253 successful procedures. The median length of follow-up for these procedures was 3.0 years; 75% of the patients had at least 13 months of follow-up. The Kaplan–Meier survival curves for the MCRS groups (fig 2A) and the CAD-specific index groups (fig 2B) indicated worse survival in patients with higher MCRS at the time of PCI and in patients with higher CAD-specific comorbid condition index scores. Cox regression models indicated that the hazard ratios for follow-up mortality had a quadratic (curved) relationship with the MCRS and CAD-specific index. With higher index scores, subsequent increases did not produce as large an increase in the hazard ratio (table 3).

{kind=link}
{kind=link}
The addition of the CAD-specific index to the MCRS significantly increased the ability to predict death after successful PCI. The c-statistic for all-cause mortality was 0.69 (95% CI 0.67 to 0.71) for the MCRS model alone (including linear and quadratic parameters) and 0.75 (95% CI 0.73 to 0.77) for the model with both the MCRS and the CAD-specific index (both linear and quadratic). The likelihood ratio test for the significance of adding the CAD-specific index terms to the model was χ2 = 43.1 with 2 df (p<0.001), indicating significant improvement in the discriminatory ability of the model.
DISCUSSION
This study demonstrates the significant incremental prognostic information obtained from adding comorbid conditions to an existing risk model for patients undergoing PCI, particularly for long-term survival. The comorbid condition measurement, however, did not significantly improve the predictive ability for in-hospital complications after PCI.
Comorbid conditions and outcome in patients with cardiovascular disease
Comorbid conditions are defined as the concurrent presence of two or more medically diagnosed diseases in the same person. The prevalence of comorbid conditions increases with age and their presence is associated with higher healthcare use, disability and mortality.2 3 13 The Charlson index, comprising 12 chronic conditions and, more recently, the CAD-specific index are common examples of the instruments available for more systematic and comprehensive inclusion of comorbid conditions into risk prediction models. Both models provide powerful tools to predict all-cause mortality.14 For this study, we chose the latter because it was developed and designed from data on patients with documented CAD.4 15 Both models have been shown to predict long-term survival in a spectrum of disease patterns with CAD. Comorbid conditions routinely serve as prognostic determinants for patients with CAD presenting with chronic stable angina or acute coronary syndrome.12 16–18 The important role of comorbid conditions in predicting post-MI outcomes was underlined by the report of the Cooperative Cardiovascular Project, which focused on Medicare beneficiaries.17 We recently evaluated the TIMI (thrombolysis in MI) and PREDICT (Predicting Risk of Death in Cardiac Disease Tool) scores in a geographically defined cohort of patients with MI from Olmsted County, Minnesota, USA, and demonstrated the important incremental value of comorbid conditions and ejection fraction for risk stratification.12
CAD is increasingly becoming a disease of the elderly, such that comorbid conditions are expected to affect outcome after PCI. However, comorbid conditions are not routinely included in current risk-outcome analyses in patients with CAD. Comorbid conditions are less prevalent in the young and are less likely to be included in any of the scores derived from clinical trials, which typically include younger people.19 In addition, the similarity in clinical presentation in patients with comorbid conditions and patients with frailty and disability blurs the prognostic distinction derived from these diagnoses.20–22 The current models for prediction of outcome in patients undergoing PCI or presenting with acute coronary syndromes use considerable weighting of clinical presentation, measures of left ventricular function and angiographic disease, such that these models are likely to be more predictive of early hazard.
Comorbid conditions and risk stratification models for PCI
Current risk prediction models for PCI were developed without consideration or systematic inclusion of comorbid conditions.5 6 8–10 23 24 In this study, we gained no additional prognostic information for in-hospital complications after PCI with the addition of comorbid conditions; the in-hospital events were largely determined by acuity of presentation, left ventricular dysfunction, age and angiographic variables. During follow-up, the significant improvement in the discriminant accuracy of the MCRS with the addition of the CAD-specific index underlines the importance of comorbid conditions in determining long-term survival after the index PCI.
Although the prevalence of comorbid conditions was greater with a higher MCRS, the association between the MCRS and the CAD-specific index was weak. Thus, both models appear to provide complementary long-term prognostic information. Additionally, the relationship between outcome and the index of interest is quadratic (non-linear), indicating that there may be a threshold of concomitant risks at which additional risks have little effect on outcome. Identification of factors associated with post-dismissal mortality after successful PCI may encourage more frequent surveillance, more intensive medical management or consideration of alternative strategies.
Limitations
This study is limited by its retrospective design. Only those comorbid illnesses defined by the CAD-specific index were included in the analysis. New comorbid conditions (eg, diabetes mellitus) may have developed in some patients on follow-up, further complicating the analysis. The c-statistic of 0.75 after inclusion of CAD-specific comorbid conditions indicates good discrimination by the MCRS model. However, other unmeasured variables may further improve the discriminatory ability of the current model. All-cause mortality was the only follow-up event measured and from this study we cannot extrapolate our results to cardiovascular mortality or other MACE.
CONCLUSIONS
In conclusion, this study showed that the addition of comorbid conditions to the MCRS adds significant prognostic information for post-dismissal, all-cause mortality but adds little prognostic information for in-hospital complications after PCI. Patients’ comorbid conditions must be included in future risk stratification models that predict long-term mortality after PCI.
REFERENCES
Footnotes
Competing interests: None declared.
Ethics approval: The Mayo Clinic Institutional Review Board approved the study
See Editorial, p 1366