Article Text

Abstract
Background: Epidemiological studies suggest that “diastolic heart failure” (DHF) is common and has a prognosis similar to that of systolic heart failure (SHF). We wanted to assess whether patients with breathlessness who were being treated for DHF had objective evidence of cardiac impairment and exercise limitation.
Methods: Consecutive patients with a clinical diagnosis of chronic heart failure completed a standardised 6-minute walk test (6-MWT) and underwent an echocardiographic examination to determine the presence of major structural heart disease (MSHD). N-terminal pro-brain natriuretic peptide (NT-proBNP) was measured to determine degree of cardiac pathology.
Results: 568 patients were identified with SHF (75.7% males) and 104 with DHF (54.7% males). They were compared with 400 healthy controls (matched with DHF group for age, sex and body mass index (BMI)). Controls (median (interquartile range); 43 (20–62) pmol/l)) and DHF patients (27 (13–67) pmol/l) had significantly lower NT-proBNP levels compared to SHF patients (178 (82–422) pmol/l). There was no difference in NT-proBNP levels between controls and DHF patients (p = 0.348). There was no correlation between BMI and NT-proBNP in either DHF (r2 = 0.03; p = 0.287) or SHF (r2 = 0.02; p = 0.346) patients. Both SHF and DHF patients reported similar degrees of breathlessness. 6-MWT distance (p = 0.973) was similar between SHF and DHF patients. DHF patients had a higher BMI (p<0.0001).
Conclusion: Patients being treated for a clinical diagnosis of DHF have the same self-reported symptoms and 6-MWT performance as patients with SHF, yet have normal NT-proBNP levels. Their perception of their symptoms is out of proportion to their evidence of cardiac pathology.
Statistics from Altmetric.com
Epidemiological studies suggest that heart failure with normal ejection fraction (HeFNEF), often labelled “diastolic heart failure” (DHF) is common, and has a prognosis similar to that of systolic heart failure (SHF).1–3 On the face of it, this observation sits oddly with the observation in large trials that increasing left ventricular ejection fraction (LVEF) is strongly predictive of better outcome in heart failure populations.4–6 Previous work has suggested that patients with HeFNEF have alternative explanations for symptoms of breathlessness.7 8 Trials of medication in patients with DHF have found it difficult to recruit,9 suggesting that DHF may be less common than epidemiological work would suggest. A further problem is the definition of DHF itself. The diagnosis of HeFNEF requires there to be heart failure (although that can be difficult to diagnose) whereas a diagnosis of DHF requires some objective abnormality of diastolic function to be present.10 Despite the availability of guidelines,11 many clinicians feel uncomfortable with diagnosing DHF when many of the abnormalities might represent natural ageing.
We wanted to explore the possibility that HeFNEF might have a further potential explanation—namely, that some individuals may perceive themselves to be breathless while having no significant structural heart disease. If such individuals have normal LVEF, they may be labelled as having HeFNEF, and if (perhaps as a consequence of ageing or hypertension) they have some abnormality of diastolic function, they might be labelled as having DHF. The aim of the present study was to assess whether breathless patients who were being treated for DHF had independent evidence of cardiac impairment using B-type natriuretic peptide and whether they had objective evidence of exercise limitation.
METHODS
In all, 1095 consecutive patients referred with breathlessness to a community heart failure clinic were initially identified. Patients were categorised into one of the following groups: normal, SHF, DHF, right heart disease (RHD), severe LV hypertrophy (LVH) and left-sided valvular disease.12 Diagnostic criteria for SHF and DHF were as follows:
SHF: an LVEF ⩽40% or a qualitative assessment of LV systolic impairment of greater than mild severity and/or marked LV dilatation (>41 mm/m2) unless secondary to severe valve regurgitation.
DHF: the presence of both left atrial dilation (>25 mm/m2)13 and LVH (both interventricular septal thickness and posterior wall thickness >11 mm).14
SHF was considered the dominant cause of HF whenever it was observed. DHF was not diagnosed when important SHF, RHD or valve disease was present.
Heart failure was diagnosed when there was an abnormality of cardiac function, either SHF or DHF, and when there was no other explanation for their symptoms. For the purposes of our study, patients with RHD, atrial fibrillation, severe LVH and left-sided valvular disease were removed from the analysis. Table 1 shows the clinical characteristics of both groups.
Routine echocardiographic assessment was performed on all patients including M-mode, two-dimensional images, and colour flow Doppler recordings using a “Vivid 5” (GE Healthcare, UK) system operating at 3.4 MHz. Measurements were taken in accordance with American Echocardiography Society/European Association of Echocardiography guidelines.15 16 Echocardiography was carried out by one of three trained operators. LV systolic function was assessed by attempted measurement of LVEF using Simpson’s biplane method in all subjects, and in all subjects by estimation on a scale of normal–mild–mild-to-moderate–moderate–moderate-to-severe–severe impairment. LV function was assessed by a second operator blind to the assessment of the first; where there was disagreement on the severity of LV dysfunction, the echocardiogram was reviewed jointly with the third operator and a consensus reached.
It is not possible to compare degrees of diastolic dysfunction with degrees of systolic dysfunction and describe patients as having similar severity of cardiac malfunction. We therefore wanted to establish an independent measure of cardiac pathology; and chose to collect blood for N-terminal pro-brain natriuretic peptide (NT-proBNP) analysis in our patients. NT-proBNP is well established as a marker of cardiac dysfunction and prognosis.17–19 Blood samples were collected by venepuncture into 6-ml EDTA tubes. Samples were centrifuged at 4°C; plasma was then removed and frozen at −80°C before analysis. Samples were analysed using the Roche NT-proBNP electrochemiluminescent assay and testing performed on an Elecsys 1010 analyser (Roche diagnostics, Mannheim, Germany). Assay precision, analytical sensitivity, interferences and stability have all been previously described.20
Patients were asked to grade their symptom severity based on the New York Heart Association (NYHA) classification by ticking a box describing their symptoms on first presentation. To assess exercise capacity, each patient performed a 6-minute walk test (6-MWT) following a standardised protocol.21 22 A 15-metre flat, obstacle-free corridor, with chairs placed at either end was used. Patients were instructed to walk as far as possible, turning 180° every 15 metres in the allotted time of 6 minutes. During the 6-MWT, patients were able to rest, if needed, and time remaining was called every second minute. Patients walked unaccompanied so as not to influence walking speed. After 6 minutes, patients were instructed to stop and total distance covered was calculated to the nearest metre. Standardised verbal encouragement was given to patients after 2 minutes and 4 minutes. To determine if chronic obstructive pulmonary disease (COPD) was present, patients performed a spirometric assessment, and the best of three manoeuvres was recorded. In order to exclude respiratory disease, patients were excluded if their FEV1/FVC ratio was <70%. All diagnostic tests and the patient interview were performed within a two-week period.
Recent studies23–25 have shown significantly lower circulating BNP levels in overweight and obese patients with advanced SHF compared with lean patients. Patients diagnosed with DHF often have a higher body mass index (BMI), and might therefore have a low NT-proBNP. We therefore included a healthy control group matched for age and BMI to the DHF group to determine the influence of BMI and age on NT-BNP independent of cardiac function. Patients with no evidence of cardiac, respiratory or musculoskeletal limitation were randomly recruited from two local GP practices and from patients presenting to the heart failure clinic but found to have no abnormality on echocardiography allowing a diagnosis of either SHF or DHF (table 1).
Statistical analysis
Variable distribution was tested using the one-sample Kolmogorov–Smirnov test. Data are presented as median and interquartile range (IQR). Normality was examined by plotting histograms of residuals. SHF and DHF were compared using independent samples t tests. We used the Spearman’s coefficient to correlate BMI and NT-proBNP data. A Kaplan-Meier curve was constructed to determine differences in mortality between SHF and DHF. A Cox proportional hazards model was used to develop predictor models for all-cause mortality using all baseline variables (table 1). All variables in table 1 were included as potential univariate predictors (entry for multivariable model p<0.1). Analysis was performed using SPSS (Chicago, IL, USA) for Windows, version 12.0 statistical software. One of the statistical issues to address is the problem of multiple testing in multivariable linear regression, when many variables are present and the possible inflation of type I error. There is no consensus among statisticians on what procedure to adopt to allow for multiple comparisons.26 Hence, we followed the recommendation of Perneger and reported unadjusted values.27
RESULTS
From the original 1095 patients, 423 were excluded because they were diagnosed with neither SHF nor DHF; 568 patients had SHF, and 104 had DHF. DHF patients were more likely to be female (45.3% vs 24.3%; p = 0.0001) and be older (median (IQR)) (75 (68–82) years vs 74 (68–80) years; p = 0.047). Spirometric variables were the same in both groups (p = 0.214). Patients with DHF had a significantly higher body mass index (BMI; p<0.0001). DHF patients had significantly lower NT-proBNP levels (median (IQR)) 27 (13–67) pmol/l compared to 178 (82–422) pmol/l in SHF (p = 0.0001). There was no correlation between BMI and NT-proBNP in either DHF (r2 = 0.03; p = 0.287) or SHF (r2 = 0.02; p = 0.346) patients; 70.2% of DHF patients were prescribed a loop diuretic or thiazide. There was no difference in any of the variables in table 1 between those patients with DHF on diuretic therapy and those not (data not shown). Four hundred healthy controls were matched for age, sex and BMI with the DHF group. NT-proBNP levels were higher in controls, though not significantly, than in DHF patients (p = 0.182), and were lower than in SHF patients (p = 0.001). There was no correlation between NT-proBNP and BMI in the control group (r2 = 0.02; p = 0.142).
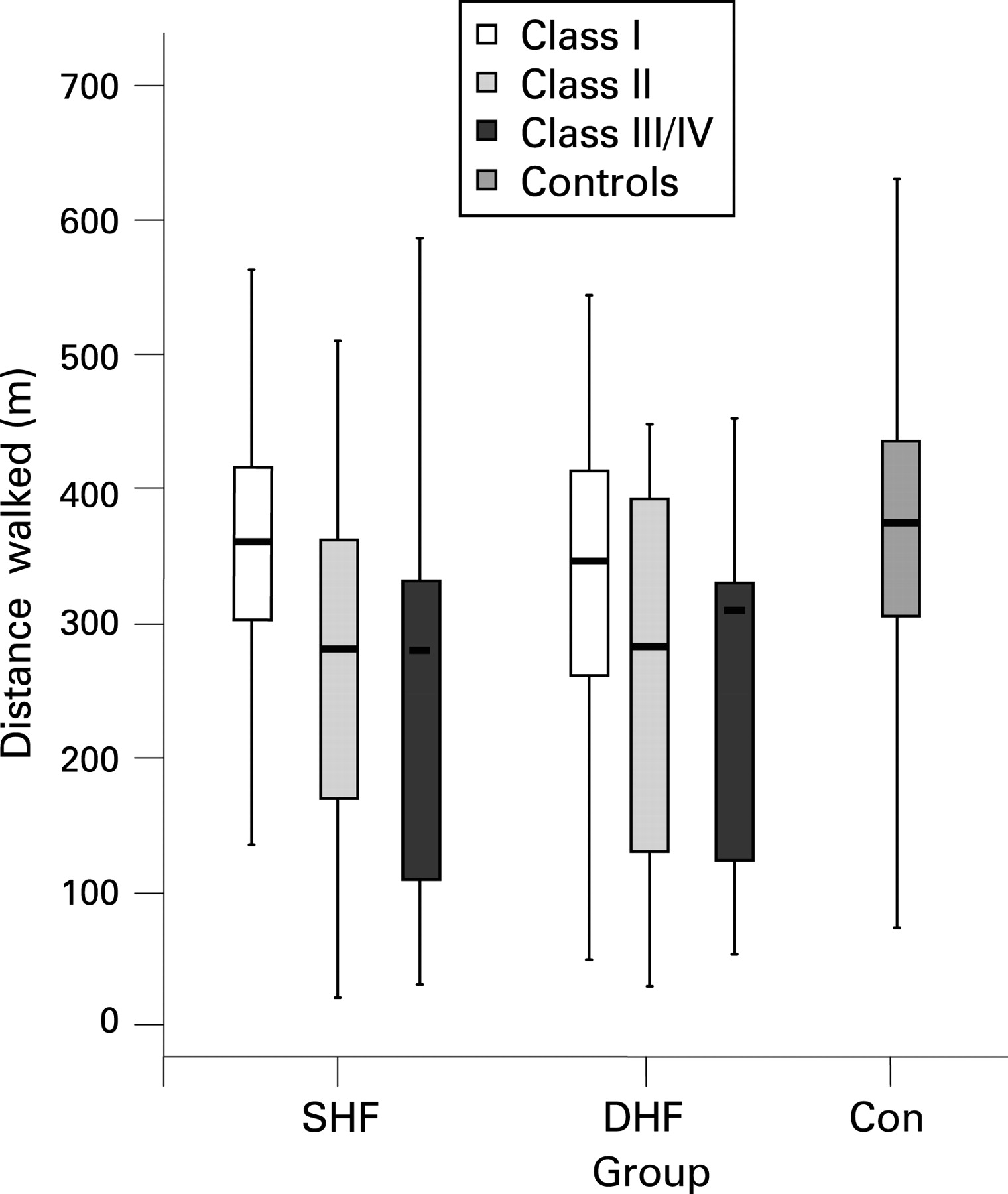
The distribution of NYHA class of symptoms between the SHF and DHF groups was the same (fig 1). Figure 2 shows that NT-proBNP levels were lower in patients with DHF regardless of NYHA class of symptoms. The 6-MWT distance was the same in both SHF and DHF patients (p = 0.973), both overall and in each NYHA class of symptoms (fig 3).


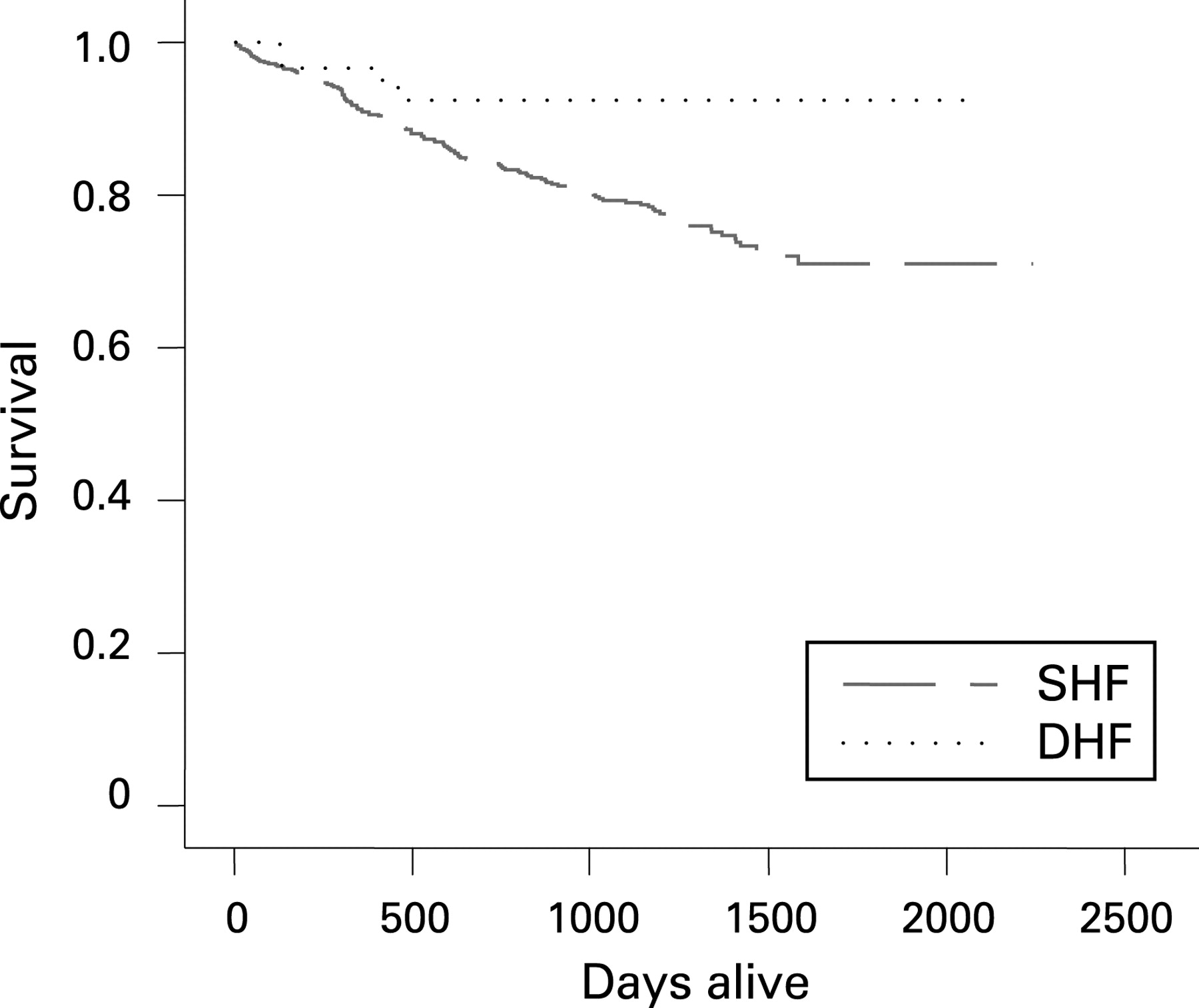
Of an initial population of 672 patients, 124 died (112 SHF and 12 DHF) representing a crude death rate of 18.5%. In surviving patients, the median follow-up time was 36.5 (IQR 32.3–40.5) months. The Kaplan-Meier curve shows a significant difference in survival (χ2 = 4.028; p = 0.045) between SHF and DHF (fig 4). Univariate predictors of all-cause mortality were decreasing BMI, increasing age, decreasing 6-MWT distance, rising NT-proBNP and decreasing FEV1 in all patients (table 2). Diagnostic group (SHF and DHF) was not a univariate predictor of mortality. Univariate predictors were the same when dichotomised for SHF and DHF groups (increasing age, decreasing 6-MWT, decreasing FEV1). Only NT-proBNP included in the SHF group was not included in the DHF group (table 2). Each candidate’s univariate predictors were included in the final Cox multivariable model of which three independent predictors of all-cause mortality were identified; increasing age, decreasing 6-MWT distance and rising NT-proBNP (table 3).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
DISCUSSION
Patients presenting with symptoms of breathlessness acquire diagnostic labels to account for their symptoms. In the absence of objective LV systolic dysfunction or another cause for signs of breathlessness many patients acquire the label HeFNEF and are further diagnosed as DHF where variables measuring diastolic events are seen to be abnormal. We have thus examined two groups of symptomatic patients, those with LV systolic dysfunction and those with similar symptoms as shown by NYHA classification and 6-MWT distance, and evidence of abnormal diastolic function on echocardiography. Our main finding is that despite the similarity of the symptoms and the limitation in 6-MWT performance, DHF patients had markedly less objective evidence of cardiac disease in the form of changes in NT-proBNP. Indeed, there was almost no overlap between the two groups.
DHF patients had a higher BMI than SHF patients. Deconditioning and altered diastolic function with elevated filling pressures may contribute to dyspnoea. Powell and colleagues28 analysed the association between BMI and LV structure and diastolic function in 4281 CHF patients. Haemodynamic data showed an association between a higher BMI and increased LV end-diastolic pressure. The authors concluded that diastolic dysfunction may contribute to the prevalence of heart failure in obese patients. It is possible that an increased BMI was a factor for the perceptions of breathlessness in our DHF patients, but the matched control group had similar BMI and no symptoms. We found that DHF patients were older and more likely to be female than SHF patients (a frequently reported observation in heart failure epidemiology reports).1–3 Previous studies have shown that female CHF patients perceive dyspnoea differently from males.29 Being female has been shown to be predictive of symptom prevalence in CHF,30 which may contribute to our findings.
Previous studies23–25 have suggested that BNP is inversely related to BMI, so it may be that the low values of BNP in our DHF group were caused by obesity. However, we found no correlation between BMI and circulating NT-proBNP levels in the SHF and DHF groups or controls. The healthy controls matched for BMI have the same BT-proBNP as the DHF group. We therefore think that lower NT-proBNP levels reflect less cardiac dysfunction in our patients.
Previous authors31 have suggested that a raised BNP is a feature of “diastolic heart failure”, but that is not what we have found. If a requirement for a raised BNP is incorporated into the definition of DHF, then manifestly the patients we describe here do not have DHF. However, patients such as those we describe are commonly labelled as having DHF on the basis of abnormal cardiac structure and evidence of exercise impairment. We suspect that our patients’ symptoms may not be cardiac in origin, but have no other explanation for those symptoms other than to suggest that the patients’ perception of breathlessness is out of proportion to an objective measure of cardiac dysfunction in the shape of NT-proBNP. The need for repeated attempts32 to define DHF attests to the difficulty of being certain that a cardiac abnormality is present.
Other authors have suggested that “HeFNEF” may, in fact, not primarily be an abnormality of diastolic function, but reflect abnormal ventriculo-arterial coupling.33 These issues will only be resolved with a robust clinical definition of heart failure. It may be that natriuretic peptide measurement provides the independent proof that the heart is abnormal and may thus be the cause of symptoms—although it is noteworthy that the requirement for raised BNP does not form part of the case definition for DHF in the latest guidelines.34 Those patients with breathlessness and “abnormal diastolic function” on echocardiography would be spared a heart failure diagnosis. We suggest that the starting point for the case definition for heart failure should start with a raised BNP, with the echocardiogram defining the type of heart failure.
Limitations
The NT-proBNP levels reported in our study are relatively low, which may reflect the fact that most patients at inclusion were already on treatment for heart failure. Furthermore, differences in the definition of diastolic dysfunction make comparisons between studies difficult. The diagnosis of diastolic dysfunction using echocardiographic criteria has inherent difficulties. Several methods exist, including mitral inflow Doppler analysis, colour flow propagation and tissue Doppler analysis. However, none is ideal for accurately establishing or quantifying diastolic dysfunction. In order to address these limitations, we required harder evidence to support the diagnosis of DHF including the presence of both LVH and LA dilation. As a result, some patients with “milder” forms of diastolic dysfunction may not have been detected. It may be that in some of the DHF patients, NT-proBNP had previously been raised and had fallen in response to heart failure treatment. However, these patients all remained symptomatic despite therapy, implying that heart failure (if present) had not been completely treated. A strict definition of the cardiac pathology in our manuscript might have to be “heart failure with LVH and LA enlargement” rather than DHF, and so our results should properly be applied only to the subset of “DHF” patients meeting these criteria. We also noted that 70.2% of patients were prescribed a diuretic at their first presentation to the heart failure clinic so were not yet necessarily on maximal medication
In conclusion, in patients with a clinical diagnosis of DHF who are being treated have the same self-reported symptoms and 6-MWT performance as patients with SHF, yet have normal NT-proBNP levels. DHF patients were more likely to be female, older and have a higher body mass index which may explain to some degree why their perception of symptoms is out of proportion to their cardiac pathology.
REFERENCES
Footnotes
Competing interests: None.