Article Text

Abstract
Background: Although higher blood pressures are generally recognised to be an adverse prognostic marker in risk assessment of cardiology patients, its relationship to risk in chronic heart failure (CHF) may be different.
Objective: To examine systematically published reports on the relationship between blood pressure and mortality in CHF.
Methods: Medline and Embase were used to identify studies that gave a hazard or relative risk ratio for systolic blood pressure in a stable population with CHF. Included studies were analysed to obtain a unified hazard ratio and quantify the degree of confidence.
Results: 10 studies met the inclusion criteria, giving a total population of 8088, with 29 222 person-years of follow-up. All studies showed that a higher systolic blood pressure (SBP) was a favourable prognostic marker in CHF, in contrast to the general population where it is an indicator of poorer prognosis. The decrease in mortality rates associated with a 10 mm Hg higher SBP was 13.0% (95% CI 10.6% to 15.4%) in the heart failure population. This was not related to aetiology, ACE inhibitor or β blocker use.
Conclusion: SBP is an easily measured, continuous variable that has a remarkably consistent relationship with mortality within the CHF population. The potential of this simple variable in outpatient assessment of patients with CHF should not be neglected. One possible application of this information is in the optimisation of cardiac resynchronisation devices.
Statistics from Altmetric.com
High mortality and poor quality of life continue to characterise a diagnosis of heart failure despite maximal pharmacological treatment.1 The number of patients with heart failure will continue to rise as the population ages and survival from myocardial infarction continues to improve.
Effective measures of prognosis are required to aid doctors with the timing of introduction of treatments and may also be useful as a measure of response to these treatments. Echocardiography and cardiopulmonary exercise testing have been shown to provide a useful measure of prognosis in this condition. However, the availability of these tests is still limited and repeated testing for individual patients is often restricted by time and cost constraints.
Systolic blood pressure (SBP) is by contrast, a simple bedside test which is recorded routinely at most cardiology appointments, can be tracked longitudinally over time and requires minimal equipment and training to assess. It therefore has the potential to be a simple method of assessing prognosis to enable doctors to target treatment and potentially assess the impact therapies.
While it is well recognised that high SBP is an adverse prognostic marker in risk assessment of most cardiac patients,2 3 its relationship with mortality in the population with chronic heart failure (CHF) is less clear. Management of heart failure includes use of angiotensin converting enzyme inhibitors (ACEi) and β blockers, both of which have been shown to improve prognosis in heart failure but which also lower the blood pressure. A large cohort study in patients admitted to hospital with acute heart failure showed that lower blood pressure is associated with a higher mortality.4
However, within the population with chronic heart failure, little prospective information has been collected to examine the relationship between SBP and mortality. A retrospective cohort study showed that a lower SBP was associated with higher mortality, although it suggested that there is a non-linear, possibly J-shaped relationship between SBP and mortality.5 Several small studies, but no large-scale studies, have looked at the relationship between mortality and SBP.
Blood pressure is intrinsically related to the heart’s ability to pump, and the mean arterial blood pressure is proportional to the cardiac output. Therefore, physiologically, there is a strong case for blood pressure as a marker of prognosis in heart failure.
This study therefore aimed to examine and quantify the relationship between SBP and mortality for stable patients with CHF.
METHODS
A literature search was performed using the key words “heart failure” and “prognosis” or “mortality” using the Embase and PubMed databases. These search terms were chosen to minimise bias so that studies that did not focus on blood pressure as the primary outcome measure and studies in which there was a non-significant relationship between blood pressure and mortality would be included.
The inclusion criteria were studies performed in a population with CHF with patients who were medically stable for at least 1 month before entry into the trial and had appropriate investigations confirming their diagnosis. Patients had to have had their SBP measured at the start of the trial.
Studies that provided sufficient statistical data to calculate the univariate mortality hazard ratio for a known unit change in SBP were included and authors for studies that did not include sufficient information were contacted to see if further information was available. Two reviewers assessed each of the papers identified. There were no disagreements between the reviewers over selection of papers or extraction of data.
Statistical analysis
The univariate hazard ratios for mortality and 95% confidence intervals were extracted from each of the included studies. Since different papers quoted mortality hazard ratios for different units of SBP, such as 1 standard deviation, the results were standardised to a 10-unit increase in SBP. To do this, the formula

was applied where HRx is the hazard ratio quoted in the source document and x is the increase in SBP in mm Hg. So, for example, for a 5-unit increase in SBP with a hazard ratio of 0.91, x = 5 and HRx = 0.91, giving a standardised hazard ratio of 0.83 per 10-unit increase in SBP. The confidence intervals for each hazard ratio were recalculated in the same way.
A fixed effects statistical analysis model was used to pool the data. Each study was assigned a relative weight, calculated from the reciprocal of the square of the width of the confidence interval, where the confidence interval was expressed in logarithmic units for a 10-unit increase in SBP. The hazard ratios for each study were then expressed in log units, and the weighted mean was calculated from the sum of the log of the hazard ratio per unit SBP multiplied by the weighting for each study. The logarithmic width of the confidence interval for the weighted mean was 1/√(Σweight).
Two studies (Huynh14 and Davos12) met the inclusion criteria but the lower limit of the hazard ratio for mortality had been rounded so that it was equal to the point estimate for the hazard ratio—for example, 0.99 (0.99 to 1.00). The authors were unable to supply more precise figures, so it was decided to assign a lower limit confidence interval so that the confidence intervals were symmetrical in logarithmic space around the point estimate. This enabled these studies to be entered into the analysis.
Heterogeneity was also assessed across the studies. To do this, 1/SE (a measure of precision) was plotted against ln(hazard ratio per 10-unit SBP). The Spearman rank test was then used to calculate whether there was any relationship between these variables.
RESULTS
Identification of reports
The Medline and Embase searches for heart failure and prognosis returned 7132 citations, 10 of which met the inclusion criteria (table 1). This gave a total population of 8088, with 29 222 person-years of follow-up. The mean SBP across the included studies was 124.9 mm Hg.
Relationship between SBP and mortality in CHF
In all of the studies of CHF, a higher blood pressure was found to be associated with a better prognosis. The degree of benefit conferred by a 10 mm Hg higher blood pressure varied between studies. We pooled the data to produce a consensus estimate and quantify its confidence intervals.
The pooled value for all studies included in the analysis gave a hazard ratio of 0.885 (95% CI 0.87 to 0.90) for a 10 mm Hg higher SBP in the population with CHF (fig 1). This equates to a decrease in mortality of 13.0% (95% CI 10.6% to 15.4%) for a 10 mm Hg higher SBP. For a 1 mm Hg higher SBP, the decrease in mortality is 1.2%. In the lowest tertile of papers (mean SBP 109), a 10 mm Hg higher SBP equated to an 18% decrease in mortality, with a 10% decrease in mortality per 100 mm Hg higher SBP in the top tertile.

Influence of ACE inhibitor and β-blocker use
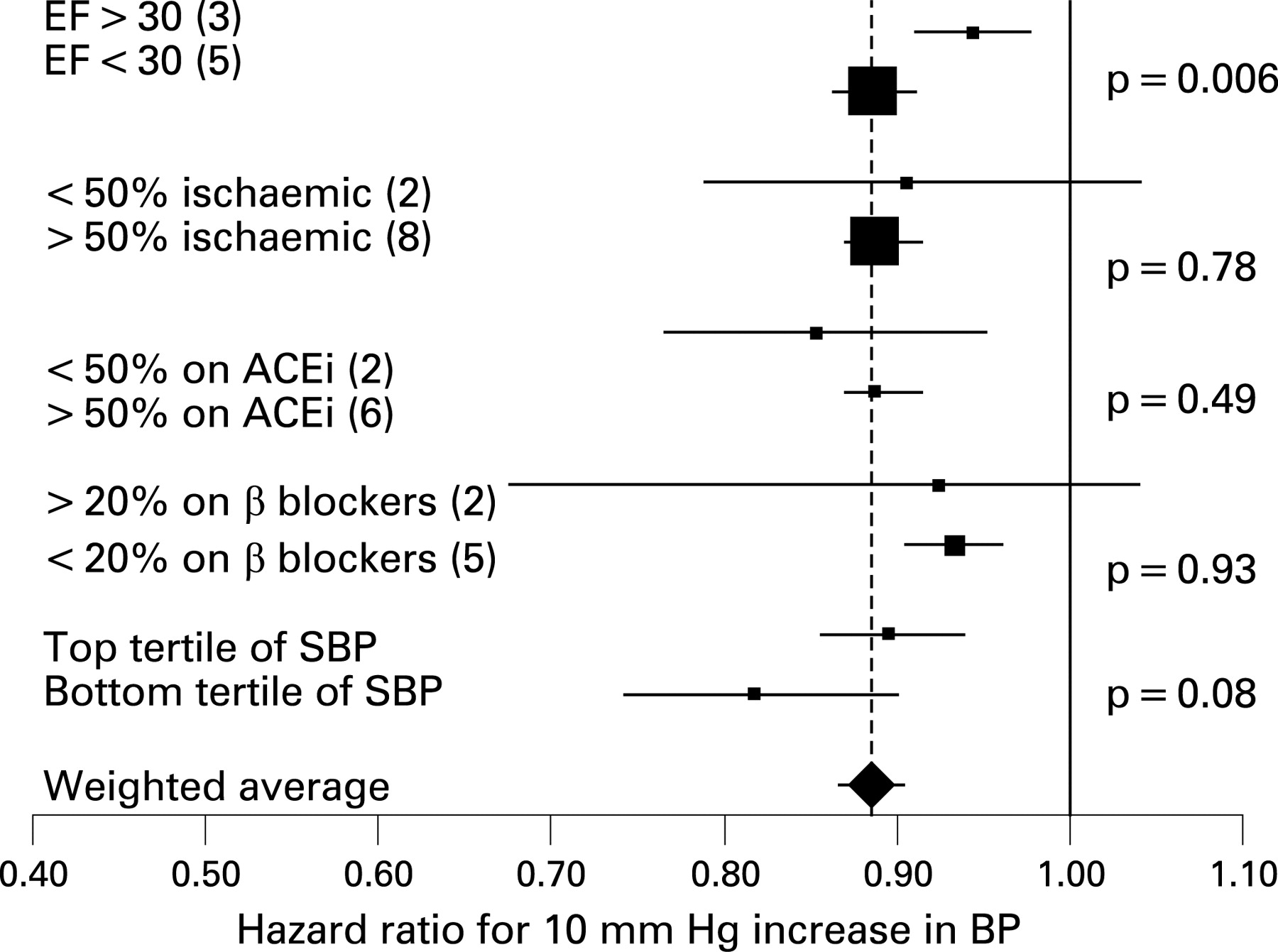
Despite the difference in pharmacological treatments between studies, there was no significant difference in the relationship between SBP and mortality on subgroup analyses for patients receiving different doses of β blockers (p = 0.93) or ACE inhibitors (p = 0.49) (fig 2).

Ischaemic versus non-ischaemic causes of heart failure
The pooled value for mortality did not differ significantly when comparing predominantly ischaemic with predominantly non-ischaemic aetiologies (p = 0.78). Division of studies dichotomously based on ejection fraction, however, did show a significantly different hazard ratio relating mortality and blood pressure (p = 0.006, fig 2).
Heterogeneity between studies
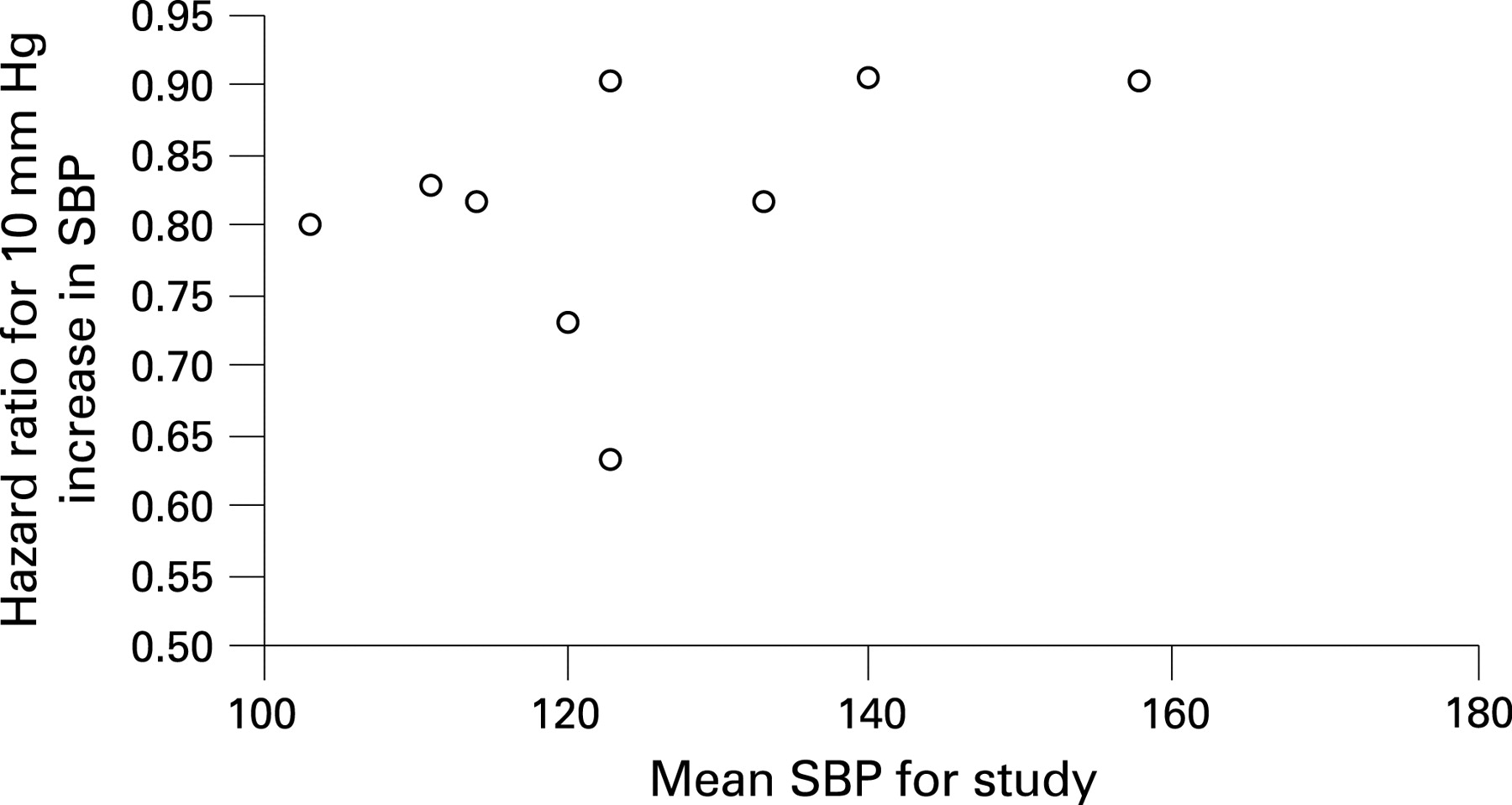
The Spearman rank test for heterogeneity showed no significant evidence of heterogeneity between studies. On comparison of hazard ratio for a 10-unit change in SBP for studies divided into tertiles by mean SBP within the study showed a non-significant difference in hazard ratio for the highest tertile compared with the lowest tertile (p = 0.08) There was a non-significant association between mean SBP within a study and standardised hazard ratio (per 10-unit change in SBP) for that study (p = 0.26, fig 3).
{kind=link}
{kind=link}
{kind=link}
Comparison with non-heart failure studies
Five relatively recent meta-analyses of the relationship between blood pressure and mortality in the general and/or hypertensive population were identified.2 3 6–8 This gave a total of over 12 million person-years of follow-up. The references for individual trial data were extracted. The large studies and meta-analyses of their results all showed a consistent relationship between SBP and mortality such that a higher SBP conferred a poorer prognosis in the non-heart failure population.9–11
DISCUSSION
In this study we have found that a higher SBP is consistently associated with a more favourable prognosis within the population with CHF. This is in contrast to the rest of the cardiac population, where a higher SBP is an adverse risk factor. This relationship was most marked in populations with a lower starting SBP.
Physiological relationship between SBP and mortality in CHF
A close relationship between SBP and mortality in CHF might be expected from consideration of cardiac physiology. The mean arterial blood pressure (MABP) is determined by the cardiac output (CO), the systemic vascular resistance (SVR) and the central venous pressure (CVP):
MABP = (CO × SVR) + CVP
In patients with cardiac disease but intact ventricular systolic function, the MABP is mostly determined by peripheral vasoconstriction. Therefore, if the systolic function is intact, a higher blood pressure indicates poorer elasticity of the arteries. As shown in numerous meta-analyses,6 23 in patients without heart failure, a higher SBP is associated with a poorer prognosis.
The situation is entirely different within the population with CHF. In these patients, a low blood pressure reflects a low ejection fraction and cardiac output. The blood pressure is low because the heart is unable to pump any more vigorously to raise it. Therefore a higher blood pressure is associated with a decreased mortality as it serves as an indirect measure of cardiac function.
The MABP lies between the systolic and diastolic blood pressures. We chose to focus on SBP as there were no data on MABP in the studies analysed. Our study found a close and consistent relationship between SBP and mortality in CHF, with a higher SBP reflecting a better cardiac output and therefore more favourable prognosis.
Bedside measures of prognosis in heart failure
To link SBP to cardiac output, we should recognise that it is the difference between SBP and CVP that the heart is generating. Accordingly, poor cardiac function may result in low SBP or high CVP, or both. The prognostic value of high CVP has long been recognised clinically, and in recent years has been shown to have a close association with mortality.21 The chief attraction in blood pressure monitoring, however, is the relative reliability of measurement, even by people with relatively brief training.
Quantification of the relationship between SBP and mortality
The pooled value for all studies included in the analysis gave a decrease in mortality of 13.0% (95% CI 10.6% to 15.4%) per 10 mm Hg higher SBP. The effect of a higher SBP is most marked in populations with a lower starting SBP, with an 18% lower mortality in the lowest tertile (mean SBP 109) and a 10% decrease in the highest tertile (mean SBP 145) per 10 mm Hg higher SBP. It is likely that the magnitude of effect associated with an increase in SBP continues to diminish such that a 10 mm Hg increase from 160 to 170 mm Hg would confer a much smaller decrease in mortality, if any. Studies included in this analysis had a maximum SBP of 158 (Huynh14), where there was a non-significant association between SBP and mortality. It may be that a level of blood pressure is reached beyond which a further increase confers an adverse prognosis, with a J-shaped relationship between SBP and mortality.
Pharmacological effects on SBP
There are many factors that influence both blood pressure and mortality in the population with CHF. Most drugs used in management of heart failure (β blockers, ACEi, diuretics) all serve to decrease blood pressure. In a patient with heart failure and low blood pressure, it is difficult to establish whether the blood pressure is low because of the advanced stage of the disease with poor cardiac output or whether it is low because the patient is being intensively managed pharmacologically.
The studies included in this analysis had a range of blood pressures and a heterogeneous sample of blood pressure lowering drugs. Despite this, there was a consistent relationship between SBP and mortality. On subgroup analysis, the only factor shown to affect this relationship significantly was ejection fraction. This was in keeping with previous studies on heart failure, which have shown that low blood pressure is an adverse prognostic sign in patients with impaired systolic function but that it may in fact be a marker of good prognosis in those with intact systolic function.22
The lack of significant effect of pharmacological treatment on the relationship between blood pressure and mortality suggests a very powerful relationship between SBP and cardiac output, such that it overcomes confounding factors of medical treatment. This is also illustrated by the relatively consistent relationship between SBP and mortality despite a heterogeneous population with varying degrees of medical optimisation.
Systolic and diastolic heart failure
The studies included in this meta-analysis had a mean ejection fraction of 28.3, indicating a population of predominantly systolic heart failure. The study by Huynh, however, has a mean ejection fraction of 42.5, with only 36% men and an average SBP of 158 mm Hg. Additionally, 23% of patients in the study by Koike had a hypertensive aetiology with a mean SBP of 140 and no EF reported. Hypertension is a common aetiology in diastolic heart failure,23 and these two studies may represent a population with predominantly diastolic heart failure. Interestingly, these are the only two studies identified where the relationship between SBP and mortality is not significant (HR = 0.99–1.0 in Huynh and HR = 0.99–1.023 in Koike). Exclusion of these two studies does not alter the mean SBP per 10-unit change in SBP, as both studies have relatively small numbers.
Implications for clinical practice
While measurement of SBP is clearly not a substitute for measurements of left ventricular ejection fraction and other markers more closely associated with cardiac output, its attraction lies in its simplicity. SBP can be routinely measured at all outpatient visits and changes in SBP can be charted to monitor disease progression. While echocardiographic data may not exist before instigation of pharmacological treatment, SBP measurements would have been taken. The prognostic implications of changes in SBP over time have not been assessed in any study of which the authors are aware; however, this would be useful information to collect.
Effect of antihypertensive drugs on SBP and cardiac output
While we have shown a close relationship between blood pressure and mortality, it is obviously not our intention to suggest that antihypertensive drugs should be omitted in patients with heart failure. This study is entirely in keeping with the finding that many drugs that improve prognosis in systolic heart failure act to reduce blood pressure, including ACEi, angiotensin receptor blockers and β blockers. The key reason is that across a population of patients with heart failure fully treated with these drugs the difference between their blood pressures is driven to some extent by differences in cardiac output.
The action of adding a prognostically beneficial vasodilator to a patient’s treatment has the primary effect of reducing systemic vascular resistance, allowing the cardiac output to increase and the blood pressure to decrease. The cardiac output increase (which might be witnessed as an increase in ejection fraction) is beneficial, and the fall in blood pressure is a manifestation of the relief of intense vasoconstriction.
If our study were to be extrapolated to changes in blood pressure, it must be emphasised that it would only be possible to do this if there were no changes in vasodilator drugs. As long as the drug regimen were stable, a rise in blood pressure might be a good sign after implantation (or optimisation) of a cardiac resynchronisation therapy device.
Potential relevance to haemodynamic optimisation of cardiac resynchronisation therapy
This consistent finding across studies in heart failure lends indirect support to the concept of haemodynamic optimisation of cardiac resynchronisation therapy with non-invasive blood pressure monitoring. Rapid and reproducible algorithms for such optimisation are now available.24–26 These potentially extend the haemodynamic improvements already achieved from simply switching on the device. The landmark trials with cardiac resynchronisation therapy showed an increase in blood pressure, paralleling the improvements in symptoms and survival, for patients entered into the device arm. For example in the COMPANION trial, patients in the resynchronisation arm initially gained approximately 2 mm Hg SBP in comparison with the control arm, and went on to have a 18% relative reduction (95% confidence interval 1% increase to 42% reduction) in the combined end point of morbidity and mortality.27 Similarly the CARE-HF trial showed, at 3 months, that the increment in blood pressure attributable to being in the device arm was 5.8 (95% CI 3.5 to 8.2) mm Hg, and the mortality reduction was 37% (95% CI 23% to 49%).28
In each case, the increase in SBP is likely to represent an improvement in cardiac output as a result of the resynchronisation. Since the SBP in patients with heart failure, unlike in the general population, is more closely governed by the cardiac output than peripheral resistance, this increase in SBP is likely to reflect an improved cardiac output and ejection fraction.
Whether increased blood pressure is a reasonable proxy for long-term outcomes has, however, been doubted, because of the general perception in cardiology that lower blood pressures are better. In this study, it becomes clear that increase in SBP, be it from resynchronisation itself or its optimisation, need not be assumed to be adverse, and might readily be beneficial. Of course, specific trials would be needed to determine this beyond doubt.
Study limitations
This type of study has many limitations. The populations chosen were heterogeneous, with a range of ejection fractions and mean systolic blood pressure, aetiologies and drugs, and were carried out at different time points. However, there was no significant association between hazard ratio and mean SBP for the studies included (p = 0.16), which gives reassurance that the key findings are not being driven by a small subset of patients.
Additionally, with studies of different sample sizes there may be effects apparent in small studies that disappear with larger populations. However, there was no evidence of a relationship between size of study and hazard ratio (p = 0.09). For identification of studies to include in the analysis, there is also the problem of publication bias, where studies that did not find a significant relationship between mortality and blood pressure are less likely to publish their data. This was dealt with by using a search strategy that did not only return studies that looked at blood pressure and mortality, but found all studies that reported mortality data in a population with heart failure.
CONCLUSION
This study has shown that there is a close relationship between SBP and mortality in the population with CHF. This is contrary to the majority of cardiac disease, where a high SBP is an adverse prognostic sign. Quantitative awareness of this relationship between SBP and mortality may be of use in assessment or sequential follow-up of patients or where more extensive testing such as echocardiography is not available. It also gives indirect support to the concept of monitoring SBP as a simple haemodynamic marker during non-invasive haemodynamic optimisation of cardiac resynchronisation.
Acknowledgments
All authors contributed to the planning and analysis of the study, and interpretation of the results as well as to the writing of the paper. CER, ZIW and JED designed and performed the literature search and studies for inclusion. MF, EAF and CHM contributed to the statistical analysis of the results. JM and DPF designed and managed the overall study and planned the analysis methods. All authors approved the final manuscript. Guarantor—DPF.
REFERENCES
Footnotes
Competing interests: None.
All researchers were independent of funders during the writing of this paper.