Article Text

Abstract
Background The combination of hydralazine and isosorbide dinitrate has been shown to provide incremental clinical benefits in patients with systolic heart failure (sHF) treated with “optimal” therapy (including an ACE inhibitor and beta-blocker). This drug combination is described to provide “balanced vasodilatation” (isosorbide dinitrate acting predominantly on veins, hydralazine on arteries). However, evidence for the latter is sparse. We examined the relative potency of hydralazine in large-calibre vessels from sHF patients and investigated its purported ability to reduce vascular superoxide (never before examined in humans).
Methods We studied 20 patients with sHF who were undergoing elective coronary artery bypass surgery. All recruited patients were receiving “optimal” sHF therapy. Internal mammary artery (IMA) was available in 10 cases. Distal segments of left IMA and saphenous vein (SV), which were harvested at the time of surgery, were collected for use in vascular studies. Vasodilatation was examined using standard organ bath techniques; cumulative concentration response curves to hydralazine (1 nmol/l to 10 μmol/l) were constructed in vessels preconstricted with phenylephrine (3 μmol/l) and mantained in physiological conditions. Basal superoxide production was measured using lucigenin chemiluminescence in SV (n = 10) and IMA (n = 10) pre-incubated with hydralazine (1 μmol/l). A xanthine/xanthine oxidase system was used to quantify the data. Plasma concentrations of hydralazine are 0.1–1 μmol/l in patients taking therapeutic doses.
Results Maximum relaxation achieved to hydralazine was 26.2 ± 5.81% in SV compared with 45.35 ± 4.25% in IMA (p = 0.032). However, there was only slightly less venous than arterial dilation at “therapeutic” concentrations (0.1–1 μmol/l) (see fig 1). Basal superoxide production was reduced significantly in both IMA (1.20 ± 0.25 vs 0.70 ± 0.20 nmol/mg per minute, p = 0.014) and SV (0.72 ± 0.08 vs 0.63 ± 0.07 nmol/mg per minute, p = 0.037), which were pre-incubated with hydralazine (fig 2). Although hydralazine had only modest vasodilator action at “therapeutic” concentrations, this effect was observed in both veins and arteries to a similar degree.
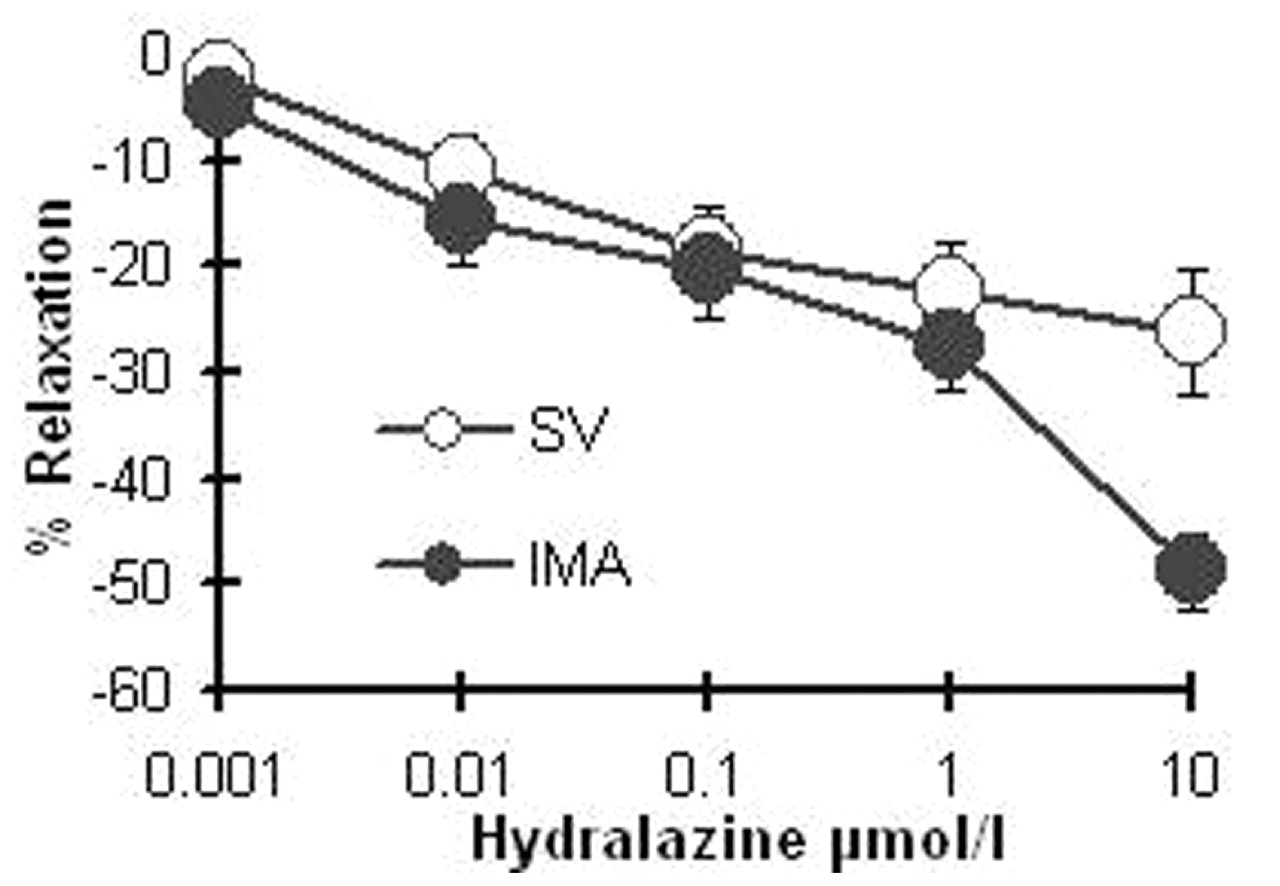
Cummulative concentration response cueves to hydralazine in human saphenous vein (SV) and internal mammary artery (IMA). Results are expressed as mean ± SEM.

{kind=link}
{kind=link}
Effect of hydralazine (Hyd) on basal superoxide production in human internal mammary arteries (IMA; n = 10) and saphenous veins (SV; n = 10). Results are expressed as nmol/mg per minute and are shown as mean ± SEM.
Conclusions We have demonstrated, for the first time in human blood vessels, that hydralazine reduces vascular superoxide production, potentially a novel and therapeutically significant mechanism of action, which may enhance nitric oxide-mediated vasodilatation. These data suggest that the therapeutic effects of hydralazine are not simply dependent on arterial vasodilatation and direct vasodilator activity, and that the observed clinical benefits of combination therapy with isosorbide dinitrate may be partly explained by favourable effects on vascular superoxide production.