Article Text

Abstract
Introduction Transcoronary pacing for the treatment of bradycardia during percutaneous coronary intervention (PCI) may have advantages over standard practice transvenous pacing, but the optimal technique and pacing efficacy have not been fully investigated. Transcoronary pacing using the coronary guidewire may be quicker to establish urgently and would avoid the procedural risks of venous access and positioning a standard “temporary wire” in the right ventricle provided the technique is a reliable method of pacing while the PCI equipment is in use. We developed a porcine model to examine the feasibility and efficacy of transcoronary pacing during PCI.
Methods Eight pigs under general anaesthesia underwent unipolar transcoronary pacing with a standard floppy guidewire in a coronary artery (as the cathode) and a skin patch electrode (as the anode). We examined the effect of: (1) skin patch position (groin vs anterior or posterior chest wall); (2) an angioplasty balloon on the guidewire and (3) which coronary artery was “wired” on the efficacy of pacing as assessed by the threshold and the reliability of pacing capture in comparison with the same parameters obtained during “standard” transvenous pacing in the same animals.
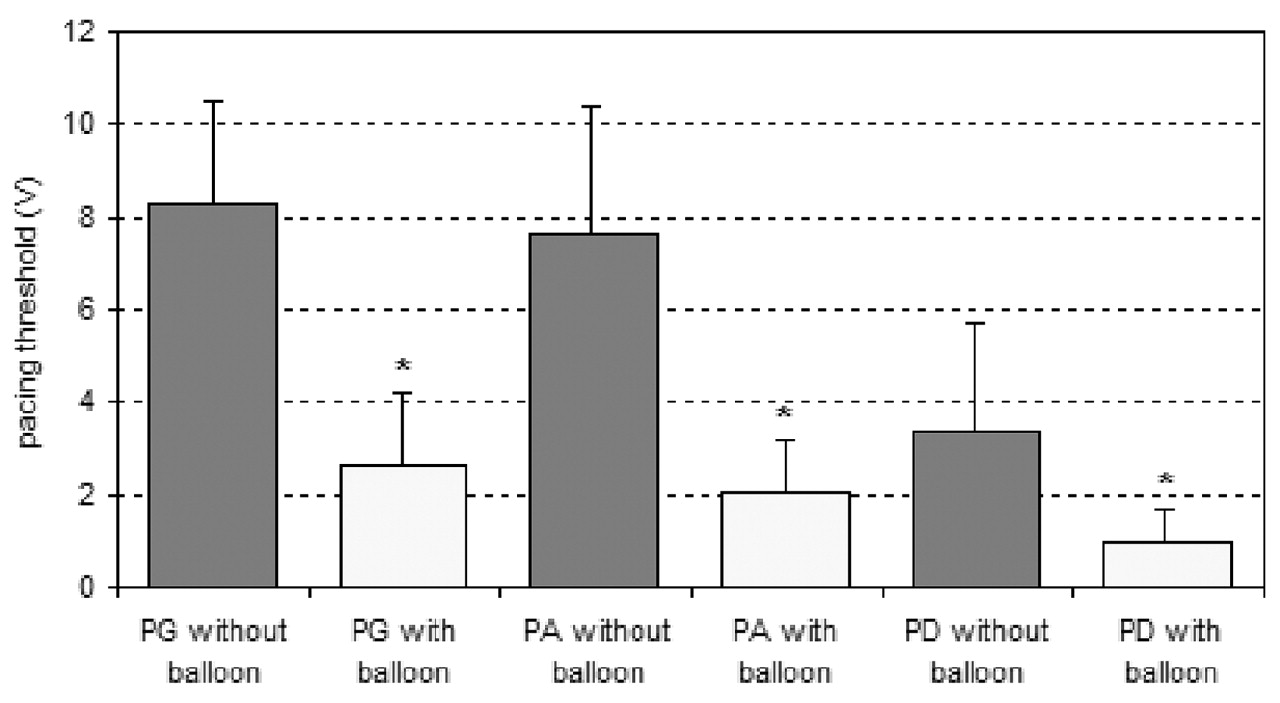
Results Pacing efficacy (the percentage of captured beats to pacing impulses delivered) using the bare guidewire and a maximum output of 10 V was 37.5% while using a skin patch in the groin but was 100% with a posterior chest wall patch. The pacing thresholds were 8.3 ± 2.2 V and 3.4 ± 2.4 V with the patch in these sites, respectively. Positioning a standard monorail angioplasty balloon over the guidewire significantly increased pacing efficacy to 100% (irrespective of the target vessel or patch location) and significantly reduced pacing thresholds (p<0.05) to 2.7 ± 1.5 (with a groin patch) and 1.0 ± 0.7 V (with a posterior chest wall patch). Using the “optimal” setup for transcoronary pacing (ie, a posterior chest wall patch and angioplasty balloon use) pacing thresholds were similar to those obtained with standard bipolar transvenous pacing (1.2 ± 0.8 V). We did not observe any adverse effects of coronary pacing. Skeletal muscle contraction was produced at maximum pacing output levels (see fig).

{kind=link}
PA, anterior chest wall patch; PD, posterior chest wall patch; PG, groin patch; *p<0.05 with versus without balloon.
Conclusions The location of the skin patch during transcoronary pacing is important. With a posterior chest wall skin patch in place, 100% pacing efficacy was achieved irrespective of which coronary artery was undergoing PCI and of the presence of an angioplasty balloon on the guidewire. The use of an angioplasty balloon lowers the pacing threshold and improves pacing efficacy. This pig model examines the practicalities of transcoronary pacing and shows the technique can yield thresholds and pacing efficacy comparable to the “standard” transvenous approach. This technique may play a role during PCI, particularly in the emergent situation.