Article Text

Abstract
Objective To examine the association between unrecognised myocardial infarction (MI) as detected by electrocardiography and the long-term risk of heart failure.
Design The Rotterdam Study is a prospective population-based cohort study of the general population of a suburb of the city of Rotterdam, The Netherlands.
Participants At baseline 2581 men and 3724 women aged ≥55 years were classified on the basis of electrocardiography, interview and clinical data into those with recognised MI, those with ECG-based unrecognised MI and those without MI. The participants were followed-up for incident heart failure, death or end of the study period on 12 October 2006.
Results During a median follow-up time of 13.2 years, 823 cases of heart failure occurred, of which 403 in men. Independently of cardiovascular risk factors, recognised and unrecognised MIs yielded HRs of developing heart failure in men of 2.6 (95% CI 2.0 to 3.3) and 2.1 (95% CI 1.5 to 2.9), respectively. In women, recognised MI was associated with heart failure (HR=2.8; 95% CI 1.9 to 4.1), whereas unrecognised MI was not significantly related to the risk of heart failure (HR=1.1; 95% CI 0.7 to 1.7).
Conclusion Unrecognised MI detected by electrocardiography yields a long-term risk of heart failure equivalent to recognised MI in men, but is not significantly related to heart failure in women. In the light of the high incidence of both unrecognised MI and heart failure in the elderly, it may be worthwhile for both doctors and patients to improve responsiveness to typical and atypical symptoms of MI.
- Epidemiology
- coronary artery disease
- electrocardiography
Statistics from Altmetric.com
Introduction
A substantial proportion of all myocardial infarctions (MIs), particularly in the elderly, is asymptomatic or escapes clinical attention. This proportion ranges from 21% to 33% in men and 26% to 54% in women.1–7 Although many studies have shown that these so-called unrecognised MIs carry an equal or larger risk of cardiovascular and total mortality compared with recognised MIs, cardiovascular morbidity after unrecognised MIs has been little studied.3–6 8 Studies found that compared with recognised MI, unrecognised MI less often led to angina pectoris, and that it carried an equal risk of recurrent MI and a higher risk of cerebral small vessel disease and stroke in men. On the other hand, unrecognised MI was associated with a lower risk of recurrent MI and stroke in women.5 6 9 10 Only the Framingham Heart Study reported on the risk of heart failure, observing an increased risk of heart failure after unrecognised MI compared with recognised MI in men. No significant differences were found in women.6
Recent epidemiological studies have shown that the lifetime risk of developing heart failure for men and women of 50–55 years of age is 20–33%.11 12 The incidence of heart failure shortly after a MI has increased over the past decades by 74%, leading to steeply increasing rates of hospitalisation and associated costs.13 14 Moreover, heart failure is associated with a severe reduction in health-related quality of life, and life expectancy after the diagnosis of heart failure is substantially reduced, with a 5-year mortality between 45% and 65%.12 15 16
Coronary artery disease, and in particular MI, is known to be one of the most common causes of heart failure in the elderly.17–19 However, the long-term risk of heart failure after unrecognised MI has been studied less extensively, especially during the past decades, where extensive progression in cardiovascular treatment strategies has been made.
We examined the long-term risk of heart failure after unrecognised MI, detected by electrocardiogram (ECG), for men and women aged ≥55 years in a prospective population-based cohort study with more than 13 years of median follow-up.
Methods
Study design, setting and population
This study is part of the Rotterdam Study, a prospective, population-based cohort study of 7983 men and women aged ≥55 years (78% of the eligible population), living in a well-defined suburb of the city of Rotterdam, The Netherlands. The rationale and design of the study have been described elsewhere.20 Baseline data were collected from 1990 until 1993. Because our study focused on unrecognised MI at baseline and future risk of heart failure, we excluded people with prevalent heart failure at baseline (n=248) and people who did not visit the research centre and therefore did not have an ECG recorded (n=898). Thirty-six participants withdrew their informed consent for follow-up. Digitised ECGs or clinical data on MI status were missing in 496 participants, which left 6305 people eligible for this study. ECGs were missing owing to technical problems or lack of sufficient personnel to operate the ECG device.
The study was approved by the medical ethics committee of the Erasmus MC, Rotterdam, The Netherlands. Participants provided written informed consent to participate in the study and for information to be obtained from treating doctors.
Assessment of MI by electrocardiography
ECGs were processed by the Modular ECG Analysis System (MEANS) to obtain ECG measurement and interpretation.21 To determine MI, MEANS uses an extensive, but comprehensive, set of criteria that is derived from the Minnesota code.22 Subsequently, two research doctors blinded for other clinical information validated the ECGs selected by MEANS. A cardiologist, who specialised in ECG methodology, ascertained the final diagnosis of MI. The diagnosis of MI using MEANS is mainly driven by pathological Q waves and auxiliary criteria, such as QR ratio and R-wave progression. ST-T changes were not considered as criteria for MI by MEANS, but were taken into account by the clinicians validating and ascertaining the diagnosis of MI based on ECG. Assessment of recognised MI status was done as reported previously for the Rotterdam Study.23 Based on this procedure, we classified participants at baseline as follows: a history of ‘recognised MI’ included people with self-reported MI confirmed by clinical data, with or without ECG characteristics matching a MI. A history of ‘unrecognised MI’ included all participants without documented or self-reported MI, but with ECG characteristics matching a MI. All unrecognised MIs were therefore Q-wave MIs. People without indication of MI on ECG and no medical documentation of an earlier MI, were classified as having ‘no MI’.
Assessment of covariates
In the Rotterdam Study, assessment of anthropometrics, cardiovascular risk factors and use of drugs has been described previously.9 Diabetes mellitus was defined as a non-fasting serum glucose level >11.0 mmol/l and/or the use of oral blood glucose-lowering drugs or insulin.
Assessment of heart failure
Prevalent heart failure at the baseline examination in the Rotterdam Study was assessed using a validated score based on the definition of heart failure of the European Society of Cardiology.24 Using this method, information on the presence of heart failure at baseline was available for all participants. Cases of incident heart failure were obtained by continuously monitoring participants of the Rotterdam Study during follow-up as described previously.12 The date of incident heart failure was defined as the day of the first occurrence of symptoms suggestive of heart failure, or the day of receipt of a first prescription for a loop diuretic or an ACE inhibitor, whichever came first. The diagnosis of heart failure was classified as definite, probable, possible, or unlikely. In accordance with the criteria of the European Society of Cardiology, only definite and probable cases were included in the analysis. A total of 169 possible and unlikely cases were not considered as heart failure events in the analysis.12 24
Statistical analysis
All analyses were performed for men and women separately. Baseline characteristics were compared using Student t test for continuous data and χ2 test for categorical data.
First, we constructed age-adjusted, heart failure-free survival curves using Cox proportional hazard analyses. Second, we used Cox proportional hazard analyses to calculate HRs for the risk of heart failure for recognised MI and unrecognised MI.25 We used the ‘no MI’ group as reference category. In model 1 we adjusted for age. In model 2, we additionally adjusted for the following cardiovascular risk factors: systolic blood pressure, diastolic blood pressure, use of antihypertensive drugs (defined as ACE inhibitors, β blockers, diuretics, antiadrenergic agents, or calcium channel blockers), body mass index, diabetes mellitus, current and past smoking, serum total cholesterol and serum high-density lipoprotein-cholesterol. Participants were censored at the time of occurrence of heart failure, death, loss to follow-up, or the end of the study period on 12 October 2006. In addition, we repeated all analyses, censoring participants when an incident MI occurred during follow-up. This was done to eliminate any possible distorting effects of incident MI during follow-up, since the risk of heart failure is highly elevated shortly after a MI.26 Approximately 5% of the participants had missing values for one or more cardiovascular covariates. These missing values were handled by single imputation using an expectation-maximisation algorithm.27 All measures of association are presented with 95% CIs. We used the level of significance of p<0.05 for all statistical analyses. Data were analysed using the SPSS statistical package, version 15.0 (SPSS Inc).
Results
Table 1 shows the baseline characteristics of the study population for men and women separately. Women represented 59.1% of the participants. At the start of the study mean (SD) age was 67.8 years (8.0) for men and 69.3 years (9.2) for women. The 2581 men were classified as follows: 150 men had a previously unrecognised MI based on their ECG, 258 a recognised MI and 2173 no MI. For the 3724 women in the study the corresponding numbers were 177, 94 and 3453, respectively. People with a MI of any type were on average older, and had lower levels of serum high-density lipoprotein-cholesterol. Systolic and diastolic blood pressure was on average higher in the unrecognised MI group than in the other groups. In general, people with a recognised MI used antihypertensive drugs much more frequently. Smoking and diabetes mellitus was noticed more frequently in men with any type of MI in comparison with the no MI group. Women with unrecognised MI had on average a higher body mass index than in the other groups. During a median follow-up of 13.2 years (interquartile range 7.6–14.3 years), eight participants were lost to follow-up, 2105 participants died, and 823 cases of incident heart failure occurred, of which 403 in men. The total number of heart failure events in each category of exposure is shown in table 2.
Baseline characteristics of the study population
Hazard ratios (HRs) for developing heart failure
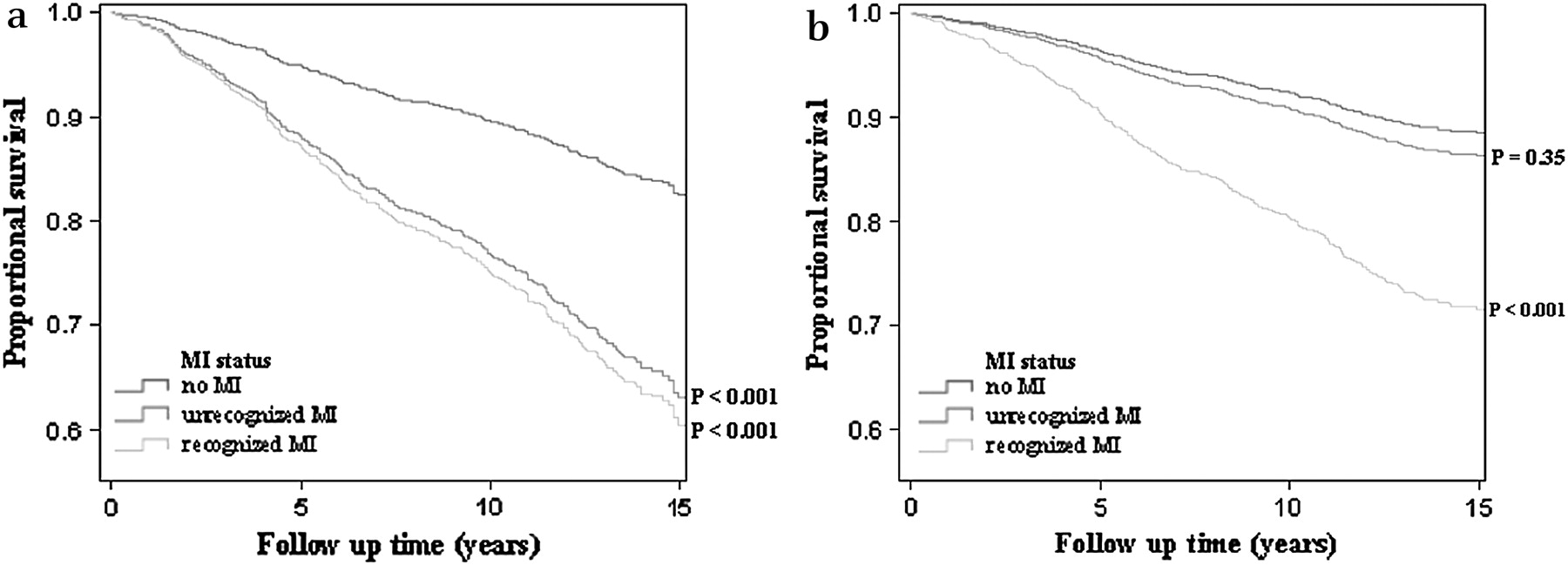
Figure 1 displays age-adjusted, heart failure-free survival for men (figure 1A) and women (figure 1B). Cumulative incidences of heart failure after 15 years of follow-up were 17% for no MI, 37% for unrecognised MI and 39% for recognised MI in men. Women had lower cumulative incidences of heart failure of 11% for no MI, 13% for unrecognised MI, and 28% for recognised MI after 15 years of follow-up. Table 2 displays the results of the age-adjusted and multivariate-adjusted models for the risk of heart failure. Men with recognised MI or unrecognised MI had an age-adjusted HR for developing heart failure of 2.6 (95% CI 2.0 to 3.3) and 2.4 (95% CI 1.7 to 3.3), respectively. Additional adjustment for cardiovascular covariates did not alter the estimate for recognised MI and slightly decreased the estimate for unrecognised MI (HR=2.1; 95% CI 1.5 to 2.9). Women with a recognised MI had a nearly threefold increased age-adjusted risk of developing heart failure (HR=2.8; 95% CI 1.9 to 4.1), which did not change after adjustment for cardiovascular risk factors. However, unrecognised MI in women was not significantly associated with age-adjusted risk for heart failure (HR=1.2; 95% CI 0.8 to 1.8), or after additional adjustment for cardiovascular risk factors (HR=1.1; 95% CI 0.7 to 1.7).

{kind=link}
(A) Age-adjusted heart failure-free survival curves for men. (B) Age-adjusted heart failure-free survival curves for women. MI, myocardial infarction.
When censoring 367 of the participants at the occurrence of an incident MI during follow-up, estimates of the HRs for recognised MI and unrecognised MI were virtually unchanged.
Discussion
Our results indicate that in men the long-term risk of developing heart failure after an unrecognised MI, as detected by ECG, is equivalent to the long-term risk of heart failure after experiencing a recognised MI. Women with a recognised MI have a long-term risk of heart failure similar to men with a recognised MI, but women with unrecognised MI, as detected by ECG, do not seem to be more prone to the development of heart failure in later life.
Previous studies
In our study we focused on heart failure, whereas nearly all other studies on the prognosis of unrecognised MI examined a combination of cardiovascular outcomes.3–5 8 The Framingham Heart Study was the only one to evaluate heart failure after unrecognised MI as a separate outcome in the past.6 This study reported 10 year age-adjusted incidences of heart failure in men of 34.4% after unrecognised MI and 23.3% after recognised MI. In women, incidences of heart failure of 12.6% and 23.6% were found for unrecognised MI and recognised MI, respectively. These incidences seem to be in line with our findings, since in our study the 10-year age-adjusted incidences of heart failure in men were 23% and 25% for unrecognised MI detected by ECG and recognised MI, respectively. In women, incidences of 9% for unrecognised MI detected by ECG and 20% for recognised MI were found. These similar incidences after MI are in accordance with a recent report from the Framingham Heart Study, indicating that the 5-year incidence of heart failure after surviving an initial MI beyond 30 days without heart failure has not changed over the past three decades.13
We found a HR of developing heart failure of 2.6 to 2.8 for recognised MI in men and women, respectively. The Cardiovascular Health Study reported on the relation between prevalent coronary heart disease and heart failure, indicating a nearly twofold increased risk.17 However, in this study coronary heart disease comprised recognised MI and also a history of angina pectoris and revascularisation procedures, which are less strongly associated with heart failure.
Gender differences
Our observation that ECG-based diagnosis of unrecognised MI is associated with an increased long-term risk of heart failure equivalent to that of recognised MI in men, but no increased risk in women is remarkable and needs some elaboration. This gender difference has been consistently described in other studies on the prognosis of unrecognised MI based on ECG investigating an array of cardiovascular outcomes—namely, stroke, cerebral small vessel disease, recurrent MI and death of cardiovascular origin.6 9 10 28 A plausible explanation might be that especially in women ECG abnormalities not caused by coronary artery disease can be mistaken for MI because of difficulties with ECG lead placement owing to breast tissue.28 This misclassification would cause an overestimation of unrecognised MI in women, which is in line with the observed larger proportions of unrecognised MI out of all MI in women (65%) compared with men (37%).1–3 5–7 This line of thought is further supported, to some degree, by the favourable overall cardiovascular risk profile of the women in the unrecognised MI group in comparison with the recognised MI group. The women in the unrecognised MI group were significantly more adipose than women without MI or with recognised MI, with consequently higher possibility of difficulties with ECG interpretation, which also supports this hypothesis (table 1).
Strengths and limitations
Strengths of our study include the availability of 823 cases of incident heart failure in a population-based setting, with standardised measurements and a long and virtually complete follow-up. Furthermore, at baseline we did not inform the participants or their treating doctors about the finding of an unrecognised MI on their ECG. This reflects the thought at that time that unrecognised MI was less severe than recognised MI, reinforced by lack of evidence that treatment after unrecognised MI could prevent subsequent cardiovascular events. Our study therefore adequately reflects the situation in the general population. During the past few years in the Rotterdam Study, we have started to report findings of unrecognised MI to the participants and treating doctors.
However, our study also has some limitations. First, we chose to examine prevalent MI to be able to compare the effect of unrecognised MI with recognised MI on the risk of heart failure, since we did not know the actual date of the event of an unrecognised MI. To be able to make a fair comparison between the risks of heart failure after unrecognised MI and after recognised MI, we chose the baseline of our study as the start of follow-up in all participants. Therefore our results only reflect the long-term risk of heart failure. Second, like in all epidemiological studies on unrecognised MI based on ECG, some misclassification may have occurred at baseline. Unrecognised non-Q-wave MI or those with a Q wave that has disappeared over time, will not have been detected as unrecognised MI, but classified as no MI.
Clinical implications
Findings of an unrecognised MI on routine ECG are relatively common in the elderly and our results indicate a comparable long-term risk of heart failure after unrecognised MI and recognised MI in men.1 Our results further suggest that the risk of heart failure after surviving a (un)recognised MI has not substantially decreased over the past two decades, despite great progress in cardiovascular treatment strategies. This merits some concern in a time period in which the rapid ‘ageing of the population’ causes overall incidences and costs of heart failure to rise extensively, partially owing to the improved survival after MI.13 14
Our results underline the importance of enhanced alertness for atypical symptoms of MI. Doctors should be aware that a large number of patients with unrecognised MI do experience ‘sounds of silence’: atypical symptoms such as dyspnoea, fatigue or palpitations.29 Moreover, patients often misattribute symptoms and their significance. Unrecognised MI may therefore not reflect the heart so much as the perception of the patient.30 Better information on typical and atypical symptoms of MI could increase the rate of people seeking medical attention, the first and most essential step in the chain of diagnosis. Even though we did not find a relation between ECG-based unrecognised MI in women and heart failure, we do believe that women as well as men will benefit from a better focus on atypical symptoms of MI.
Conclusions
The high incidence of unrecognised MI detected by ECG in the elderly and its equivalent risk of heart failure compared with recognised MI in men, underlines the importance of enhanced alertness for typical and atypical symptoms of MI by both doctors and patients. The inability to show an association between unrecognised MI in women and incident heart failure adds to the existing suggestion that women are more prone to misclassification of unrecognised MI based on ECG.
Acknowledgments
The authors thank all the participants and staff of the Rotterdam Study, as well as the general practitioners and pharmacists of the Ommoord district for help with data collection and validation.
References
Footnotes
Funding This study is supported by The Netherlands Organisation for Scientific Research (NWO) [VICI 918-76-619]. The Rotterdam Study is supported by Erasmus MC; Erasmus University Rotterdam; Netherlands Organization for Health Research and Development (ZonMw);the Research Institute for Diseases in the Elderly (RIDE); the Ministry of Education, Culture and Science; the Ministry of Health, Welfare and Sports; the European Commission; and the Municipality of Rotterdam.
Competing interests None.
Patient consent Participants provided written informed consent to participate in the Rotterdam Study and to obtain information from treating doctors.
Ethics approval The study was approved by the medical ethics committee of the Erasmus MC, Rotterdam, The Netherlands.
Provenance and peer review Not commissioned; externally peer reviewed.