Article Text

Abstract
Background To examine the effect of serum testosterone levels on survival in a consecutive series of men with confirmed coronary disease and calculate the prevalence of testosterone deficiency.
Design Longitudinal follow-up study.
Setting Tertiary referral cardiothoracic centre.
Patients 930 consecutive men with coronary disease referred for diagnostic angiography recruited between June 2000 and June 2002 and followed up for a mean of 6.9±2.1 years.
Outcome All-cause mortality and vascular mortality. Prevalence of testosterone deficiency.
Results The overall prevalence of biochemical testosterone deficiency in the coronary disease cohort using bio-available testosterone (bio-T) <2.6 nmol/l was 20.9%, using total testosterone <8.1 nmol/l was 16.9% and using either was 24%. Excess mortality was noted in the androgen-deficient group compared with normal (41 (21%) vs 88 (12%), p=0.002). The only parameters found to influence time to all-cause and vascular mortality (HR ± 95% CI) in multivariate analyses were the presence of left ventricular dysfunction (3.85; 1.72 to 8.33), aspirin therapy (0.63; 0.38 to 1.0), β-blocker therapy (0.45; 0.31 to 0.67) and low serum bio-T (2.27; 1.45 to 3.6).
Conclusions In patients with coronary disease testosterone deficiency is common and impacts significantly negatively on survival. Prospective trials of testosterone replacement are needed to assess the effect of treatment on survival.
- Coronary artery disease
- epidemiology
- gender
- HRT
Statistics from Altmetric.com
Men have more than twice the risk of dying from coronary disease than women, an effect that persists after controlling for cardiovascular risk factors.1 It has been assumed that testosterone is deleterious to the male cardiovascular system and contributes to the vascular risk. In fact, there is little evidence that endogenous testosterone is an adverse risk factor but the role of testosterone status and replacement therapy on male health is controversial.2
High doses of exogenous anabolic steroids are undoubtedly associated with cardiac disease,3 but high endogenous testosterone levels within the normal range do not appear to be harmful. Indeed, low rather than high testosterone levels in men are associated with several cardiovascular risk factors including an atherogenic lipid profile, insulin resistance, obesity and a prothrombotic fibrinolytic profile.4 5 Studies in male animals have shown that castration or induced hypogonadism increases atherosclerosis and testosterone replacement abrogates this.6 7 In addition, testosterone has beneficial effects in men with cardiac disease. Testosterone is a potent coronary vasodilator, an effect mediated by a calcium channel antagonist action, and consequently has benefits on the angina threshold, particularly in men with low baseline testosterone.8 9 Testosterone therapy reduces total cholesterol, fat mass, waist circumference and pro-inflammatory cytokines associated with atherosclerosis, diabetes and the metabolic syndrome.10–12 Testosterone also improves functional capacity and insulin resistance in men with heart failure.13 14
In an ageing male population low serum total testosterone is common and has a prevalence of 30% in men over the age of 60 years.15 Testosterone deficiency may cause undesirable effects such as loss of bone and lean body mass, increased adiposity, low energy and impaired physical and sexual function. Until recently, these effects were viewed as the natural physiology of ageing; however, four recent major studies have found low testosterone to be associated with increased all-cause mortality after controlling for baseline morbidity and age.16–19 The effect of testosterone on mortality is independent after adjustment for baseline covariates; the EPIC-Norfolk study17 excluded men with cardiovascular disease and cancer at baseline and yet found that all-cause mortality and cardiovascular mortality was increased for every 6 nmol/l reduction in serum testosterone. Low testosterone status is therefore associated with mortality and vascular mortality, yet no study has specifically examined patients with established cardiovascular disease. This is important because men with manifest coronary artery disease are at a higher risk of cardiovascular mortality and represent a patient population prone to testosterone deficiency. In addition, those men with angina, chronic heart failure or diabetes may derive particular symptomatic benefit from androgen replacement therapy.10 12 20 21
This study had two aims, first to assess the impact of testosterone status on all-cause mortality in men with pre-existing coronary disease, and second to identify the prevalence of biochemical testosterone deficiency in men with coronary disease. Our hypothesis was that low serum testosterone would be associated with an adverse survival.
Methods
Subjects and design
This was a prospective follow-up cohort study; subjects were recruited from male patients undergoing elective coronary angiography in a tertiary cardiac referral centre between June 2000 and June 2002. The study was approved by the local research ethics committee and all subjects gave written informed consent. Patients were approached before 09:30 hours on the morning of the procedure and asked to complete a questionnaire detailing history and medication. Height and weight were measured and body mass index (BMI) calculated, venous blood was taken for the same day measurement of C-reactive protein (CRP) and the remaining serum was sealed and frozen at −20°C until assayed.
Patients were excluded from the study if they had malignancy, chronic inflammatory disease, myocardial infarction within the past 3 months, recent or current infection or uncontrolled heart failure, as these conditions are all associated with the suppression of testosterone production, or if they were taking sex hormone manipulating therapy. Similarly, in a predefined protocol exclusion, subjects were also excluded from further analysis if they had a serum CRP level above 10.0 mg/l, even in the absence of clinical evidence of inflammation, because inflammatory disorders are associated with the suppression of testosterone production.
The result of each angiogram was reported by the patient's cardiologist at the time of the angiogram and before any measurement of the testosterone level. Significant coronary artery disease was defined as 70% or greater stenosis in any epicardial coronary artery or 50% or greater stenosis of the main stem of the left coronary artery. Coronary plaque was defined as diffuse coronary atheroma not fulfilling these criteria. Normal coronary arteries were defined as smooth coronary vessels free of surface irregularities or stenoses. Left ventricular function was classified as normal or as mild, moderate or severely impaired by assessment of left ventriculography at the time of angiography or by echocardiography using standard echocardiographic techniques. Patients with normal coronary arteries were excluded from the main analyses. Serum levels of total testosterone (TT) and bio-available (bio-T) testosterone were determined. Bioavailable testosterone was used because this value measures the free and albumen-bound testosterone and is a more accurate assessment of the biologically active component than total testosterone, especially in older men.22
It is recognised that anticipatory stress may affect testosterone levels. To determine the validity and reproducibility of hormone testing on the day of angiography, the first 50 eligible individuals were asked to return to the hospital outpatient department between 08:00 and 09:30 hours, 2 weeks after angiography. Blood was taken for repeat measurement of TT, and comparison made with the sample taken on the day of angiography. In addition, subject anxiety was assessed by the widely used Spielberger state–trait anxiety inventory, form Y and the cognitive–somatic anxiety questionnaire. These assess individual stable anxiety-proneness. The difference between the testosterone level on the day of angiography and at follow-up was correlated with anxiety scores to assess whether patients' tendency to perceived stress was associated with falsely low testosterone on the day of angiography.
Patient data were electronically flagged for death certification at the Office of National Statistics, UK. All death certificates issued in the UK on study patients were copied to the research office. The information available was limited to patient details, date of death, postmortem reports (if performed) and the given cause of death by the certifying physician. In October 2008 after 145 deaths, the database was subject to the present analysis. Vascular mortality was defined as any death in which the primary cause was related to atherosclerotic vascular disease, heart failure or unheralded cardiac arrest (International Classification of Disease (version 10) codes I20-25, I70-71, I42.0, I46 and I50).
Hypogonadism is a clinical syndrome complex comprising symptoms and biochemical evidence of testosterone deficiency.23 Laboratory ranges differ between hospitals but at our institution, testosterone replacement is recommended in men with a total TT level less than 8.1 nmol/l or a bio-T testosterone level less than 2.6 nmol/l. Therefore hypogonadism was defined as a bio-T level of less than 2.6 nmol/l or a TT level of less than 8.1 nmol/l. The range of TT less than 15.1 nmol/l was also analysed as this group with borderline low total testosterone levels require further evaluation in standard endocrine practice.
Assays
Serum TT was measured in duplicate by ELISA (DRG Instruments Gmbh, Germany). Bio-T was measured by the method of Tremblay and Dube.24 CRP was measured by routine hospital assay. The intra-assay and interassay coefficients of variation of the assays were: TT less than 6% and less than 5%; bio-T less than 5% and less than 8%.
Statistical analysis
The relationship between testosterone status and mortality was determined using Cox proportional hazard regression. Initial unadjusted analyses were performed; each covariate was then added to the model to examine the effect on mortality. Finally, a multivariate regression model was constructed using all variables in a forward stepwise approach to determine which factors had influence after adjustment. Survival curves adjusted for these baseline variables were constructed to illustrate the effect of testosterone on mortality. The prevalence of hypogonadism was calculated from the raw data. Clinical predictors of biochemical hypogonadism were determined by regression. Categorical data were compared between groups using the χ2 test. Values are expressed as a percentage of each group or as mean±SD unless stated. Correlations were performed using Spearman's rank correlation (rS) or Pearson correlation (rP) as appropriate. All analyses were performed using SPSS version 14.5. Significance was sought at the 0.05 level.
Results
Reproducibility/reliability of the index blood test
In the first 50 subjects with coronary artery disease, the TT level was 12.4±6.2 nmol/l. On repeat testing, the mean testosterone level was 12.2±5.0 nmol/l, p=0.72 with close correlation between the two samples (rP=0.89, p=0.0002). There was a strong correlation between the Spielberger state–trait anxiety inventory and cognitive–somatic anxiety questionnaire scores (rS=0.70, p<0.01) but no relation of either score with the difference between the testosterone level on the day of angiography and at repeat testing (rS=−0.20, p=0.30; rS=−0.30, p=0.20). The validity of hormone testing on the day of angiography was therefore accepted.
Baseline data
A total of 1165 eligible men was approached, 17 refused to participate so 1148 men were recruited, 70 were excluded from all analyses because of elevated CRP (>10 nmol/l) and 148 were excluded from the primary predetermined analyses because of normal coronary arteries. This left a cohort of 930 men on whom the main analyses were performed. These men were followed up for a mean of 6.9±2.1 years after recruitment. In the coronary disease group there were 129 deaths, of which 73 were vascular deaths; the equivalent figures for the non-coronary disease group were 16 and eight. The baseline data are shown in table 1, this is further divided into men with bio-T less than 2.6 nmol/l—a level specific for testosterone deficiency.
Baseline data
Impact on mortality
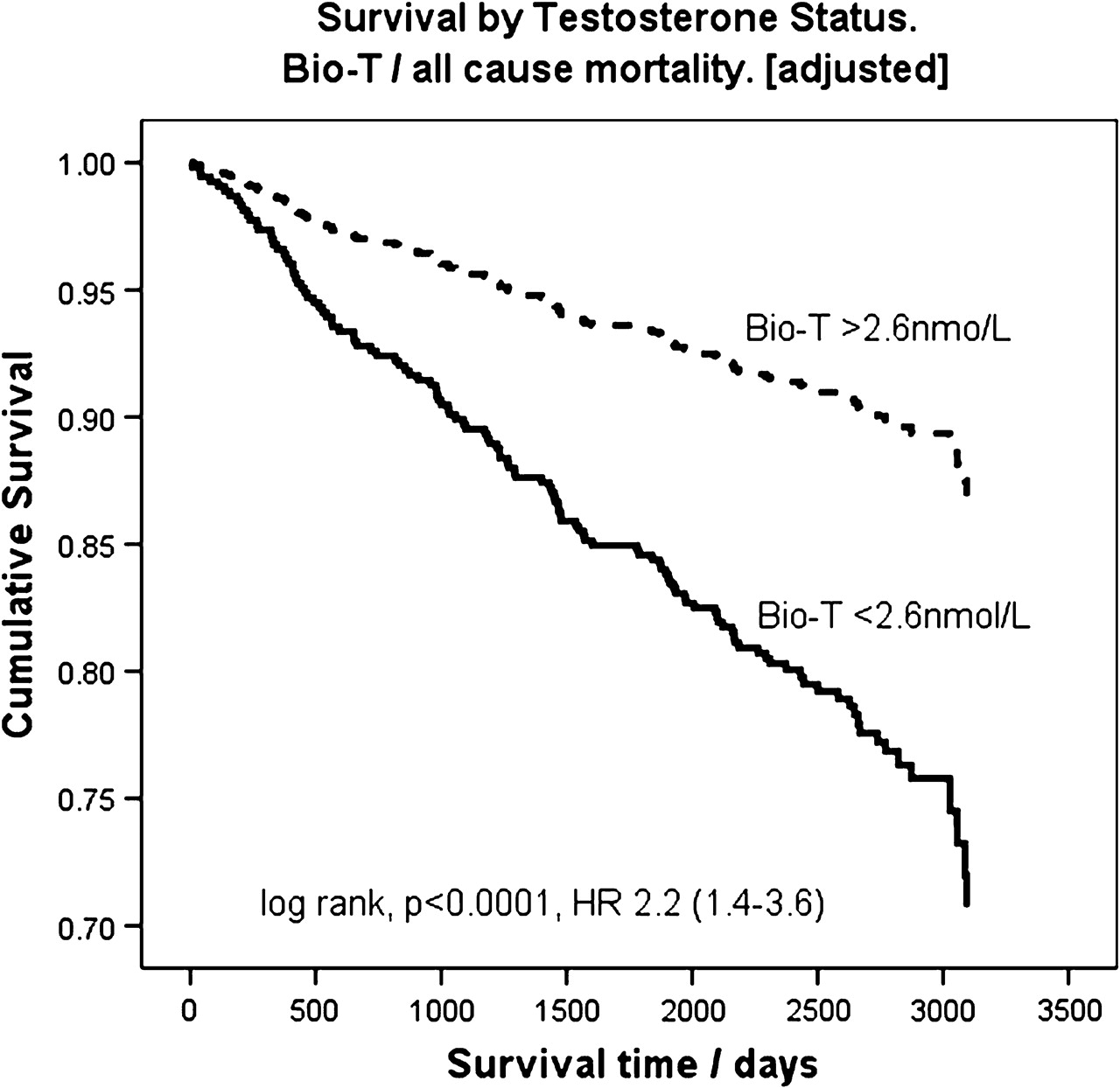
In the multivariate analysis using all baseline variables in a forward conditional regression model the only parameters found to influence time to all-cause mortality (HR ± 95% CI) were left ventricular dysfunction (3.85; 1.72 to 8.33), aspirin therapy (0.63; 0.38 to 1.0), β-blocker therapy (0.45; 0.31 to 0.67) and low serum bio-T (2.27; 1.45 to 3.6). An adjusted survival curve of patients with low baseline bio-T(<2.6 nmol/l) shows a significant hazard imparted by a low bio-T level for all-cause (figure 1) and vascular mortality (figure 2). The full analysis was repeated on the whole cohort including those men with normal coronary arteries. The results were substantially the same except the presence of normal coronaries was associated with a favourable HR (0.56; 0.31 to 1, p=0.05).
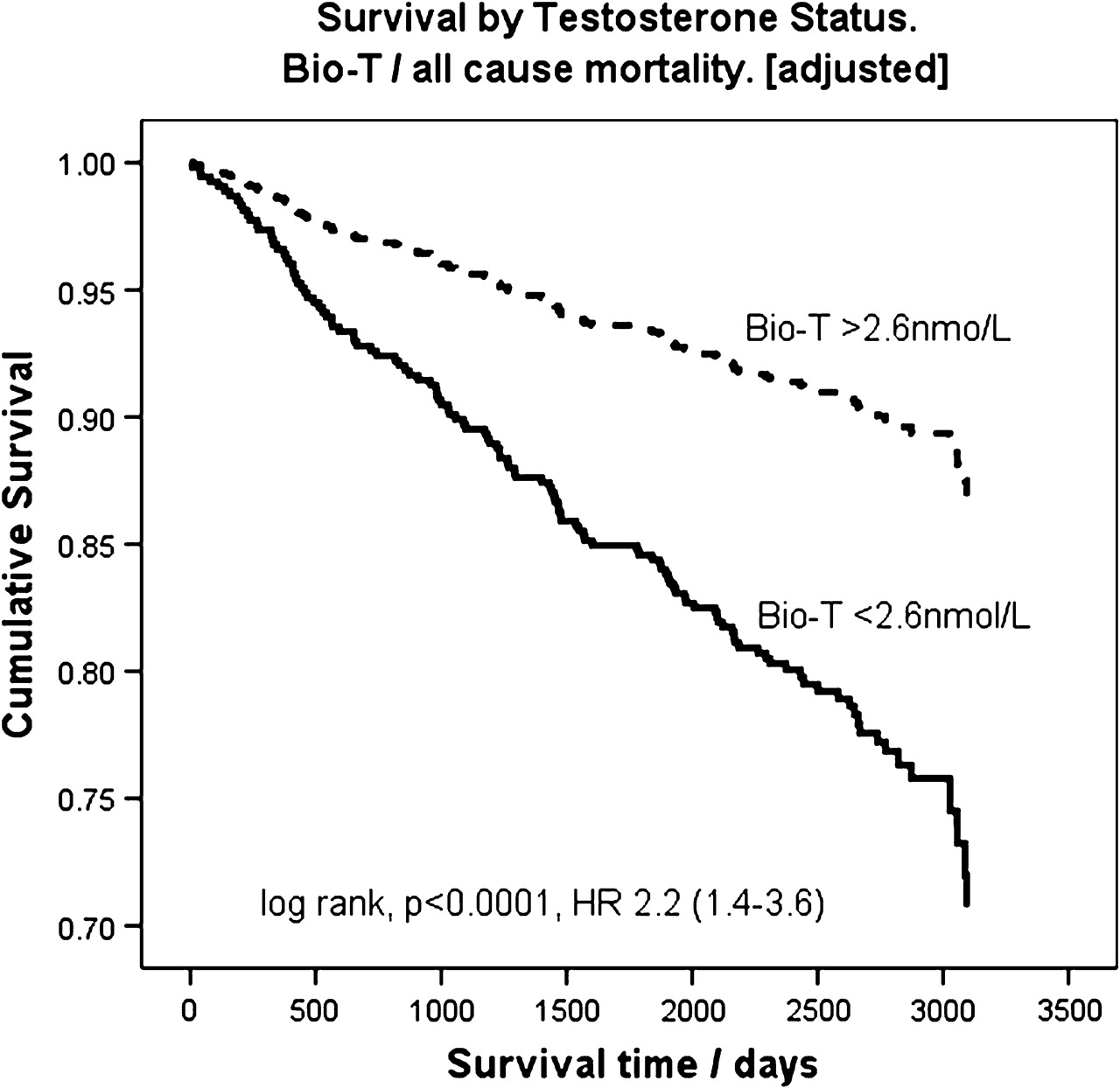
Shows a survival curve of all-cause mortality based on baseline bio-available testosterone (bio-T). The solid line represents patients with baseline bio-T less than 2.6 nmol/l, the broken line represents patients with bio-T greater than 2.6 nmol/l. HR, hazard ratio.
{kind=link}
{kind=link}
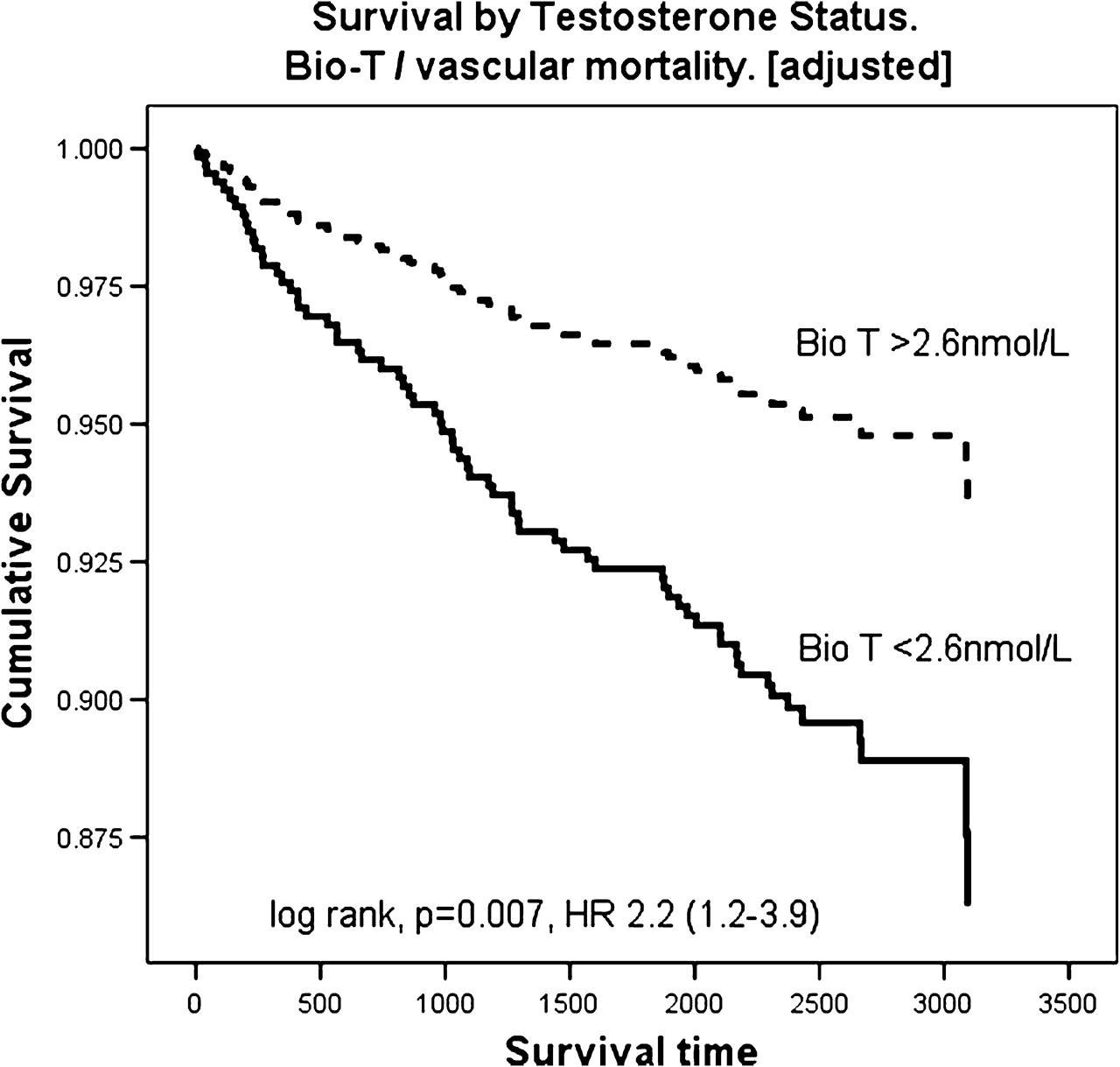
Shows a survival curve of vascular mortality based on baseline bio-available testosterone (bio-T). The solid line represents patients with baseline bio-T less than 2.6 nmol/l, the broken line represents patients with bio-T greater than 2.6 nmol/l. HR, hazard ratio.
Total testosterone and mortality
In the multivariate analysis the serum total testosterone was inversely associated with mortality TT (0.96; 0.9 to 1). A baseline TT level of less than 15.1 nmol/l showed an increased all-cause hazard of 1.86 (1.1 to 3.2) and vascular mortality of 2.5 (1.2 to 5.3). However, the conventional cut-off of TT of less than 8.1 nmol/l did not demonstrate a significant survival hazard in the coronary disease cohort for all-cause mortality although this value approached significance 1.6 (0.95 to 2.85).
Prevalence of hypogonadism in men with coronary disease
The overall prevalence of biochemical testosterone deficiency in the coronary disease cohort using bio-T less than 2.6 nmol/l was 20.9%, using TT less than 8.1 nmol/l was 16.9% and using either was 24%.
On logistic regression with all variables included, predictors of low serum bio-T (<2.6 nmol/l) were age (OR 1.03; 1.0 to 1.1, p=0.003), BMI (OR 1.06; 1.0 to 1.1, p=0.004) and former smoking (OR 0.59; 0.4 to 0.9, p=0.005). The predictor of a low TT was only BMI (OR 1.14; 1.1 to 1.2, p=0.0001). Predictors of either low TT or bio-T were age (OR 1.02; 1.0 to 1.04, p=0.04), BMI (OR 1.09; 1.04 to 1.13, p=0.0001) and former smoking (OR 0.64; 0.5 to 0.9, p=0.01).
Comparison of the coronary with the non-coronary disease groups found no significant difference in the prevalence of biochemical testosterone deficiency; (22% vs 20.9% for bio-T <2.51 nmol/l, 19% vs 14.1% for TT <8.1 nmol/l, 28% vs 24% for either; χ2 in each case p>0.13).
Discussion
Our data suggest that the prevalence of biochemical testosterone deficiency is common in men with coronary disease and is present in 24% of this sample. The present data have confirmed that low endogenous bio-T is related to all-cause and vascular mortality in a coronary disease population. TT is weakly associated with survival and a cut-off of TT of less than 15.1 nmol/l is related to increased mortality. Therefore, we also conclude that borderline low levels of TT may also adversely impact on survival. The relationship of low bio-T to mortality is significant with only β-blocker therapy and left ventricular dysfunction having greater statistical influence on survival in the multivariate model. Importantly, the impact on survival was maintained after controlling for all baseline factors such as age, BMI, co-existent medication comorbidity and smoking. Testosterone levels themselves were significantly associated with BMI, age and former cigarette smoking, but the effect on mortality was still present after adjustment for these factors.
What is the implication of this finding? Our data cannot determine if low testosterone levels cause increased mortality or are merely a marker of risk due to underlying disease. Testicular function is suppressed in many acute and chronic diseases; our study did not have a healthy control group because the normal coronary artery group had a high level of valvular disease, left ventricular dysfunction and other comorbidities such as hypertension and diabetes. However, at inclusion, few if any subjects were acutely ill as they were selected before day case elective angiography; subjects with recent acute coronary syndromes, uncontrolled heart failure or elevated CRP were excluded. Within the confines of our data the severity of underlying disease does not influence endogenous serum testosterone as there was no effect on testosterone levels imparted by increasing the number of diseased coronary vessels or the presence and severity of left ventricular function. We have not measured the total burden of coronary atheroma but this is reported to be related to testosterone levels in one study.25
Our data expand on and are entirely consistent with previous studies of testosterone status on mortality. In previous studies the exclusion of patients with cardiovascular disease or the exclusion of all deaths within the first 519or 2 years17did not weaken the relationship of low testosterone with mortality, in fact the HR increased. The inference from these data is that testosterone is not just a marker of poor health—should this be the case the relationship of testosterone and mortality ought to weaken following the exclusion of early deaths, whereas the reverse is seen. Our data confirm that high-risk patients with documented vascular disease are subject to similar hazards associated with low serum testosterone in other studies.
What is the pathophysiology of low testosterone status and the apparent increased mortality of atherosclerotic disease? Animal data show that testosterone deficiency accelerates atheroma and replacement prevents this;6 7 human follow-up studies have shown an increased progression of atheroma in men with lower testosterone.26–28 These data therefore suggest that testosterone deficiency is associated with progressive atherosclerosis and replacement, in animals at least, prevents this; the precise mechanism by which testosterone impacts on atheroma remains unclear.
Abnormal testosterone status is common, the prevalence of biochemical testosterone deficiency in the coronary disease cohort was 20.9% using bio-T less than 2.6 nmol/l, 16.91% using TT less than 8.1 nmol/l and 24% using either, a figure similar to other studies.15 The present data also raise the issue of borderline testosterone deficiency. We have shown an excess mortality in men with TT of less than 15.1 nmol/l, a level higher than most accepted definitions of hypogonadism. It is recognised that TT is not a specific test to determine androgen status because the total testosterone assay includes free testosterone, the loosely bound albumen fraction and the relatively tightly bound (inactive) sex hormone-binding globulin fraction. Bio-T seems to be more specific for detecting pathological deficiency and mortality as low levels less than 2.6 nmol/l predict mortality, whereas borderline levels do not. A low level of bio-T (<2.6 nmol/l) is therefore likely to be abnormal, whereas a high level of TT (>15.1 nmol/l) is likely to be normal. An indeterminate TT (8.1–15.1 nmol/l) is difficult to interpret: the bio-available testosterone may be pathologically low or normal. In line with accepted practice, we advocate assays to measure free or bioavailable testosterone in this subset. If these are not available formulae have been derived to estimate these, but these should be validated with the local laboratory.9 29
We have demonstrated that testosterone deficiency is associated with premature death in a cohort of patients with vascular disease; many of these patients died and will continue to die from cardiovascular disease. There is ongoing debate over the risk–benefit ratio of testosterone replacement in patients who are testosterone deficient, and there is still a concern among doctors that testosterone replacement therapy might increase the risk of vascular disease. Despite this there has been a huge increase in testosterone prescriptions in the past two decades,30 and there is scientific plausibility and a plethora of trials showing benefit in terms of risk factor modification and symptoms (reviewed in Jones et al).4 If androgen deficiency is part of the underlying pathophysiology of atherosclerotic disease in men, then the serum testosterone level could be viewed as a modifiable risk factor. Physiological testosterone replacement is an inexpensive and well-tolerated therapy but does require careful monitoring.23
A prospective outcome study of testosterone replacement on mortality is the logical next step. These trials should target high-risk populations such as men with cardiac disease or diabetes because these men have most to gain, their event rates are higher and any influence of therapy positive or adverse is more likely to be demonstrated within the confines of a clinical trial.
Limitations
This was a longitudinal follow-up study; the data from our subjects were only recorded at the time of angiogram and at death. We do not have data on subsequent revascularisations performed, changes in pharmacotherapy, insulin resistance, mood or vascular events other than related to the index mortality. It is possible that any or all of these may influence both mortality and serum androgen levels. In addition, patients may have been commenced on testosterone replacement therapy by other physicians although this number is likely to be very small.
Acknowledgments
The authors thank the following colleagues for permitting the recruitment of their patients into the study: Dr W Baig, Dr RJ Bowes, Dr S Campbell, Dr J Gunn, Dr R Muthusamy, Dr C Newman, Dr GDG Oakley, Dr L O'Toole, Dr G Payne, Dr W Rhoden, Dr BT Saeed, Dr JN West and Dr NM Wheeldon. The authors also wish to acknowledge Miss Joanne Nettleship and Miss Joanne Hall for performing the majority of the total and bio-available testosterone assays.
References
Footnotes
Funding This study was funded by the South Sheffield Charitable Trust.
Competing interests None.
Patient consent Obtained.
Ethics approval This study was conducted with the approval of the South Yorkshire local research and ethics committee.
Provenance and peer review Not commissioned; externally peer reviewed.