Article Text

Abstract
Objectives Five drug classes have been shown to improve the prognosis of acute myocardial infarction in clinical trials: aspirin, β-blockers, statins, renin angiotensin system (RAS) blockers and thienopyridines. We aimed to assess whether the benefits of combining these drugs (termed optimal medical therapy, OMT), will result in a reduction of mortality in clinical practice.
Design Nationwide registry
Setting Hospitals with a cardiology unit or internal medicine department.
Patients 5353 patients with acute myocardial infarction. At hospital discharge 89% received aspirin, 90% β-blockers, 84% statins, 81% RAS blockers, 70% a thienopyridine and 46.2% OMT.
Interventions Pharmacotherapy
Main outcome measures OR with 95% CI for mortality from myocardial infarction were calculated and adjusted for patient risk at baseline.
Results Total mortality was reduced by 74% in patients receiving OMT (adj OR 0.26; 95% CI 0.18 to 0.38) versus patients receiving one or no drug. This was consistent in subgroups defined by STEMI/NSTEMI, diabetes and gender. Mortality was also reduced in patients receiving 2–4 drugs (adj OR 0.49; 95% CI 0.35 to 0.68), diabetic patients being the only subgroup with no significant effect. Analyses on the relative importance of either component revealed that withdrawal of β-blockers (adj OR 0.63; 95% CI 0.34 to 1.16) and/or a combination of aspirin/clopidogrel (adj OR 0.59; 95% CI 0.20 to 1.17) abolished the risk reduction conferred by OMT.
Conclusions OMT over 1 year was associated with a significantly lower mortality of patients with acute myocardial infarction in clinical practice. However OMT is provided to less than half of eligible patients leaving room for substantial improvement.
- Guidelines
- myocardial infarction
- registry
- mortality
Statistics from Altmetric.com
Introduction
Acute myocardial infarction (AMI) is a major cause of morbidity and mortality. Community studies conducted before the advent of percutaneous coronary intervention, thrombolysis and refined pharmacotherapy have consistently shown overall case fatality rates of about 50% in the first month, half of these occurring within the first 2 hours after initial presentation.1
While out-of-hospital mortality has changed little over the past few years, in-hospital and long-term mortality of patients surviving until hospital admission is on the decline.2 Recent studies have shown an overall 1-month mortality of 4–6%.3 4 In the TRITON TIMI 38 trial the overall death rate in patients with acute coronary syndromes after 15 months was as low as 3.1%.5
For the secondary prevention of vascular events clinical trials have shown that five drug classes substantially improve the prognosis of patients with acute myocardial infarction: aspirin, β-blockers, statins, renin angiotensin system (RAS) blockers and thienopyridines. Optimal medical therapy (OMT) consisting of these five drug classes has the potential to substantially lower long-term mortality. The use of these drugs in clinical practice is however less than optimal with 89% receiving aspirin, 90% β-blockers, 84% statins, 81% RAS blockers and 70% a thienopyridine at hospital discharge in the recent SAMI (Secondary prevention after Acute Myocardial Infarction) registry.6 After 1 year the prescription rate was substantially lower. On the other hand using OMT is of particular importance for clinical practice where 11% have recurrent myocardial infarction within 1 year and mortality remains much higher than in the general population with a RR of 2.1 (95% CI 1.9 to 2.5) for the first 30 days and 5.6 (95% CI 5.1 to 6.2) thereafter.7 Further, it is of importance since patients in clinical practice are at an increased overall cardiovascular risk than those in clinical trials.8
We therefore analysed the proportion of patients being treated with OMT in clinical practice and its impact on mortality overall and in subgroups defined by the presence of ST deviations (STEMI vs NSTEMI), diabetes and gender.
Methods
SAMI was a nationwide registry in 79 hospitals with a cardiology unit or an internal medicine department in Germany. Methods have been described in detail previously.6 In short, SAMI was initiated and performed as a prospective multicentre study conducted by the ALKK-study group (Arbeitsgemeinschaft Leitender Kardiologischer Krankenhausärzte). The registry study design was approved and authorised by the ethics commission of the Ärztekammer Westfalen-Lippe and the Westfälische Wilhelms Universität Münster. Patients were consecutively documented at admission, hospital discharge and after a follow-up of 1 year. Oral but not written informed consent, because of the non-interventional design of the registry, was obtained before inclusion in the study.
Study population
Between February 2003 and October 2004 a total of 5353 consecutive patients hospitalised for an episode of acute ST-elevation myocardial infarction (STEMI) or acute non-ST-elevation MI (NSTEMI, symptoms lasting <24 hours) according to ESC (European Society of Cardiology) definition were enrolled. Further definitions: (1) cardiogenic shock was defined as any of the following: hypotension with systolic blood pressure <90 mm Hg as a result of reduced left ventricular ejection fraction with a need for catecholamines. Signs of left ventricular failure with dyspnoea and signs of congestion. (2) Heart failure was defined as any of the following: dyspnoea with signs of congestion. Peripheral oedema was regarded as a sign of right heart failure.
The procedures of documented diagnostic measures were defined as well (ECG at rest, ejection fraction (EF), diagnostic tests in ischaemia, coronary angiography).
Pharmacotherapy
Optimal medical therapy (OMT) in this paper is defined as receiving ACE inhibitors/ angiotensin-receptor blockers (ARBs), β-blockers, statins, aspirin, clopidogrel unless contraindicated. In case one component was contraindicated, patients receiving all indicated therapies were optimally treated from a clinical perspective but were not included in the current analysis. Practice guidelines at the time of SAMI recommended the use of aspirin and β-blockers in all patients with acute coronary syndrome (ACS) without contraindications.9–11 All patients were considered to be eligible for antiplatelet/anticoagulant therapy unless they had a history of life-threatening bleeding, coagulopathy or thrombocytopenia. All patients were considered to be eligible for β-blockers unless they had significant bradycardia (heart rate <50 beats/min) or hypotension (systolic blood pressure <90 mm Hg). ACE inhibitors or ARBs were considered to be indicated in all patients with STEMI and in patients with non-ST-elevation ACS who had hypertension, diabetes or heart failure. Contraindications to ACE inhibitors were hypotension and severe renal dysfunction (serum creatinine >221 μmol/l in men or >177 μmol/l in women). Because accumulating evidence suggests no threshold below which lipid-modifying medication is ineffective and contraindications are rare, all patients with ACS were considered to be eligible for statin therapy.12 13
Data collection
Baseline demographic data, previous medication, patients' status, early diagnostic procedures, risk factors/concomitant diseases and therapeutic procedural data were obtained at hospital admission. The intra-hospital clinical course and diagnostic procedures, final diagnosis, secondary preventive steps, complications and patient status were recorded as hospital discharge. After 1 year patient status was explored including cardiovascular events and current pharmacotherapy by patient questionnaires.
Statistical analysis
The collected data were verified with respect to formal and contextual accuracy depending on performed measurement variance and logical dependence. In the case of absent or inconclusive information hospitals were contacted for further data. The completeness of collected variables was between 95% and 99%, except for ‘manifestation of infarction’ (86.4%) and some laboratory data during the acute phase (77.3%–96.0%). The biometric evaluation of the data was performed in a descriptive and exploratory way. For continuous variables the number of patients, average value, and SD, median, minimum and maximum were determined. For categorical variables percentage frequencies were determined. OR were calculated with 95% CI and adjusted for age, cardiac arrest on presentation, heart rate, systolic blood pressure, Killip class, ST-segment deviation, abnormal cardiac biomarkers, serum creatinine, previous myocardial infarction (MI), heart failure and in-hospital revascularisation.
Results
A total of 5353 patients with acute myocardial infarction were included into the SAMI registry. Eighty-four per cent received statins, 89% aspirin, 70% clopidogrel, 90% β-blockers and 81% RAS-blocking agents at hospital discharge. Overall, 46.2% of patients received OMT (figure 1). Patients receiving OMT were younger, more frequently male, had more risk factors like nicotine abuse, hypertension and dyslipidaemia and had more often received CABG in the past (table 1). On the other hand a history of stroke or known PAD was more frequent in patients not receiving OMT (suboptimal therapy at discharge). There was a higher frequency of previous stroke (11.5% vs 5.7% in patients with OMT) and/or PAD (12.1% vs 6.9%) in this patient subgroup.

Prescription of drugs having been shown to be effective in the secondary prevention of vascular events after myocardial infarction (% of all patients eligible for drug prescription). CSE, cholesterol synthesis enzyme inhibitors; RAS, renin angiotensin system.
Baseline demographic and clinical characteristics
In-hospital management
Patients not receiving optimal medical therapy at discharge more often showed complications such as heart failure and resuscitation at admission (28.0% and 7.6%, respectively) or during the course of the hospitalisation (25.7% and 4.2%, respectively). More patients having the LAD stented received OMT (37.7% vs 33.1%, p=0.003). For details see table 2.
In-hospital management
OMT and 1-year mortality
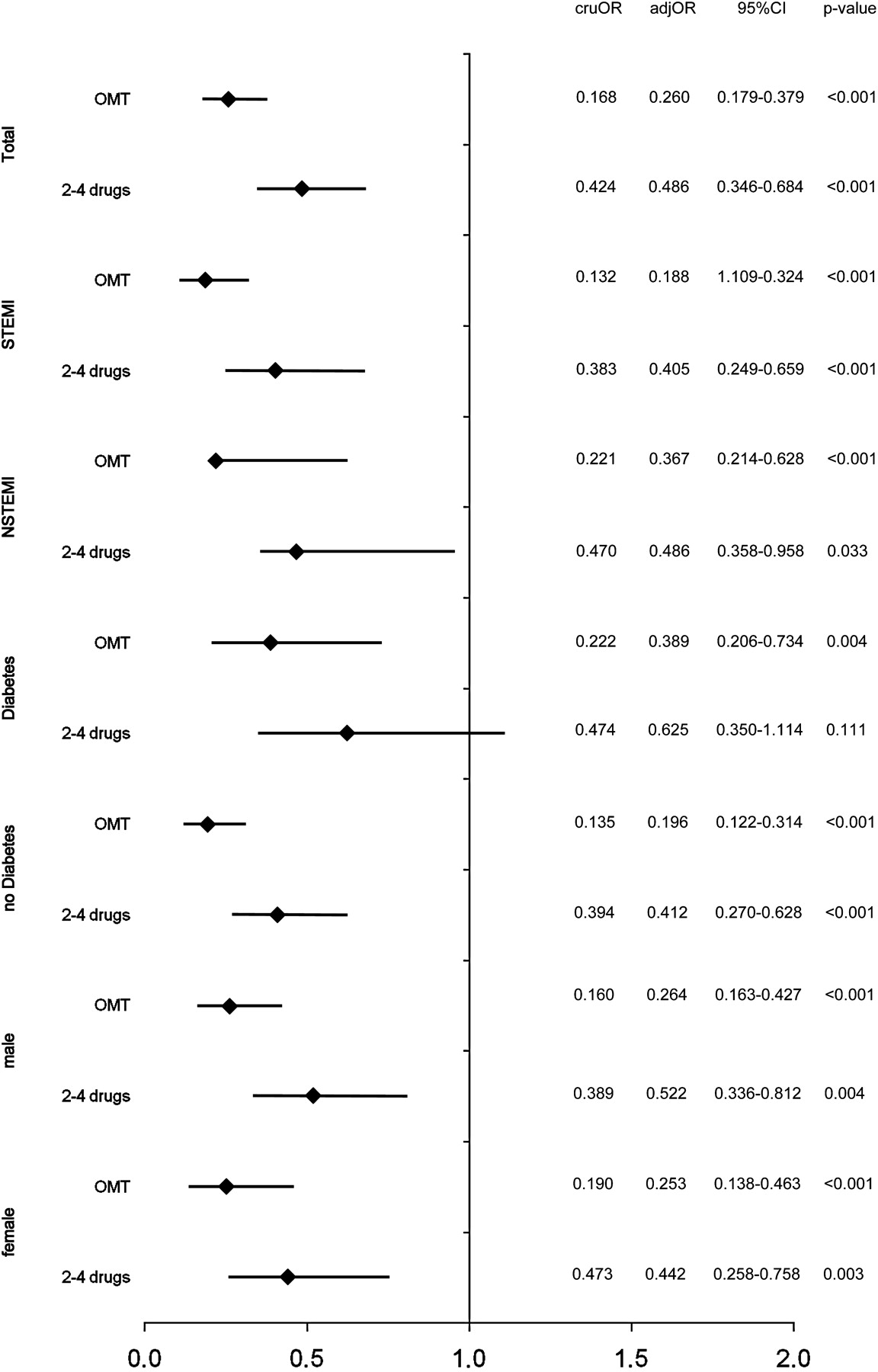
Figure 2 shows that OMT was strongly associated with a better survival 1 year after acute myocardial infarction. The OR for mortality was lower in patients receiving OMT (adj OR 0.260; 95% CI 0.179 to 0.379) compared to no or one drug (p<0.001). The effect of OMT was consistent in subgroups of patients defined by the type of MI (STEMI vs NSTEMI), the presence or absence of diabetes and in both genders.

Univariate and multivariate analysis—independent predictors of 1-year mortality overall, STEMI/NSTEMI, diabetes/non-diabetes, male/female. Adj OR, adjusted OR (adjustment for age, cardiac arrest on presentation, heart rate, systolic blood pressure, Killip class, ST-segment deviation, abnormal cardiac biomarker, serum creatinine, previous MI and heart failure and in-hospital revascularisation); cruOR, crude OR; NSTEMI, non-ST-elevation myocardial infarction; OMT, optimal medical therapy; STEMI, ST-elevation myocardial infarction.
Mortality was also reduced in patients receiving 2–4 drugs (adj OR 0.486; 95% CI 0.346 to 0.684) compared to no or one drug (p<0.001), the effect was nominal but the CI overlapped indicating non-significance. This trend was observed in every subgroup of patients defined. In patients with diabetes the effect of 2–4 drugs was not significantly reduced against 0–1 drugs (p=0.111).
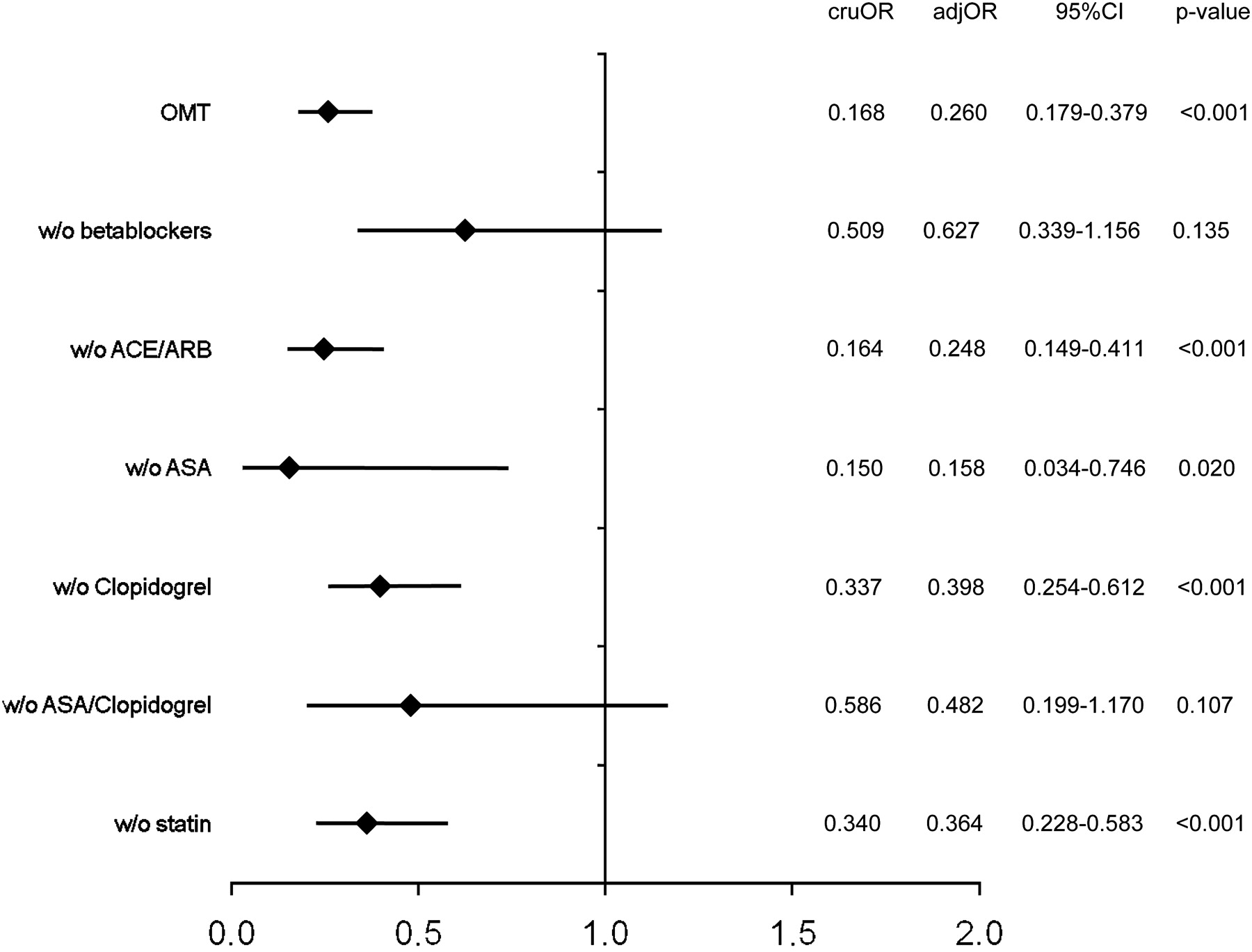
In figure 3 the relative importance of OMT components on mortality after AMI is displayed. The effect of OMT was still significantly preserved after withdrawal of either RAS-blocking agents, clopidogrel and a statin with CI overlapping with the one of OMT. The withdrawal of β-blockers (adj OR 0.627; 95% CI 0.339 to 1.156) and of the aspirin/clopidogrel combination (adj OR 0.428; 95% CI 0.199 to 1.170) however resulted in a non-significant lowering of mortality compared to using only no or one drug.

{kind=link}
{kind=link}
{kind=link}
Optimal medical therapy (OMT) and the effect of withdrawing specific components. adjOR, adjusted OR (adjustment for age, cardiac arrest on presentation, heart rate, systolic blood pressure, Killip class, ST-segment deviation, abnormal cardiac biomarker, serum creatinine, previous MI and heart failure and in-hospital revascularisation); ARBs, angiotensin receptor blockers; ASA, aspirin; cruOR, crude OR; OMT, optimal medical therapy.
Discussion
The secondary prevention of cardiovascular and cerebrovascular events as well as mortality is a key effort in the medical management of acute myocardial infarction. Long-term survival has been substantially improved over the past few years, but mortality rates in clinical practice are still higher than in randomised controlled trials. SAMI was able to document that use of OMT was associated with an increased 1-year survival. Total mortality was reduced by 74% in patients receiving OMT, which was consistent in subgroups of patients defined by STEMI/NSTEMI, diabetes and gender. However less than 50% of patients received such an optimal combination of all five drug classes, leaving substantial room for improvement.
Optimal medical therapy use
The majority of patients received aspirin, β-blockers, statins, RAS-blocking agents or clopidogrel at hospital discharge. Although the initial prescription rates of single components of OMT were encouraging, a subset of these patients discontinued treatment during the course of follow-up: At 1 year 84.0% of patients received β-blockers (90% at hospital discharge), 67.5% ACE inhibitors and 11.7% ARBs (81% at least one of them at discharge), 87.7% either clopidogrel or aspirin (89% aspirin, 70% clopidogrel) and 76.8% lipid-lowering agents (84%). Unfortunately we were, for example, not able to follow the decline in clopidogrel and provide a mean duration of prescription, but the transition of patients from the initial hospitalisation back into primary care may represent a critical transition point. At this point adequate long-term medication has to be ensured.11 14–16
A further aspect to consider in evaluating the benefits of optimal medical therapy is within-class differences in the risk-benefit ratio of drugs and that the use of high doses might provide additional benefit in organ protection. Examples of this are available for thienopyridines, for which different ratios of benefits and risk have been reported per drug and drug dose,5 for the choice of ACE inhibitors/ARBs with a differential effect on morbidity and mortality17 and for statins for which a different potential to lower cholesterol values has been reported.
Optimal medical therapy
There are an abundant number of studies documenting the underuse of evidence-based pharmacotherapy in the secondary prevention of vascular events after AMI.14 18–22 However there are far fewer studies documenting the role of optimal medical therapy on long-term survival in clinical practice.11 23–25
In the most recent report, Yan et al documented OMT use in 51.8% of patients in the Canadian ACS II registry (2002–3), which is compatible with our data.11 They further documented an absolute increase of 23% over the previous Canadian ACS I registry (1999–2001) at which time 28.9% of patients received OMT (p<0.001).
In their registry OMT use (all five drug classes) was associated with an 46% risk reduction (adj OR of 0.54) in comparison with using no or one drug. The use of two or three drugs was again associated with a less pronounced but still significant risk reduction of 35% vs no or one drug (OR 0.65). Both comparisons were highly significant. The effect size in the Canadian registry pointed into the same direction with on average greater reduction in mortality in SAMI. Furthermore the proportion of high-risk patients in SAMI receiving OMT was higher than that in the two Canadian registries.
Limitations
The present dataset describes the course and outcome of a large sample of patients with either STEMI or NSTEMI in 79 hospitals throughout Germany and thus gives a pretty complete picture of clinical practice in Germany. Inherent in the observational study design, however, are a number of restrictions. Since this is not a randomised trial subjects who are more likely to get OMT may differ in variables (health awareness, exercise, social status) not obtained with the clinical case report form and bias arising from these differences can not be accounted for. Further to this, groups under consideration have been formed on the basis of variables that are themselves prone to bias. Therefore there is no possibility of differentiating whether differences in therapy led to a different outcome or patient characteristics leading to a particular choice of therapy might have influenced this outcome. Finally the analysis presented in this paper may be compromised by below optimal completeness of data (85%). Data for critical endpoints were however available in 95% of cases, making a systematic distortion of results unlikely.
Conclusions
Secondary prevention of cardiovascular events is a cornerstone of the long-term prognosis of acute myocardial infarction. OMT with statins, aspirin, clopidogrel, β-blockers, ACE inhibitors/ARBs over 1 year was crude and, after adjusting for confounding baseline variables, associated with a significantly lower mortality. It is however prescribed in less than 50% of cases and every effort should be made to increase its use.
Acknowledgments
We acknowledge the active participation of 79 hospitals and their staff throughout Germany. A full list of participating hospitals has been published.6
References
Footnotes
Funding The study has been funded by Solvay Pharma.
Competing interests SAMI was funded by an unrestricted educational grant from Solvay Arzneimittel, Hannover, Germany. Solvay had no active role in the preparation of neither this analysis nor the decision to publish the manuscript. UT, JS and PB have been actively involved in advisory boards and have received research grants of different pharmaceutical companies producing cardiovascular drugs for patients with acute myocardial infarction. The statistical analyses were performed by NB who is a named author on this manuscript.
Ethics approval This study was conducted with the approval of the Ärztekammer Westfalen-Lippe and the Westfälische Wilhelms Universität Münster.
Provenance and peer review Not commissioned; not externally peer reviewed.