Article Text

Abstract
Introduction Repeat revascularisation after coronary angioplasty and stenting is well recognised, a feature of most prospective trials of percutaneous intervention (PCI) and is a major difference reported in trials comparing surgical to percutaneous revascularisation strategies. We investigated outcomes and repeat procedures in some 25 000 consecutive patients over 9 years from a UK teaching hospital.
Methods Between January 2001 and August 2009, 24 521 patients presented to the John Radcliffe Hospital Oxford for coronary angiography. Revascularisation procedures in the follow-up period were analysed using the procedural database, stored angiographic images and from casenote review.
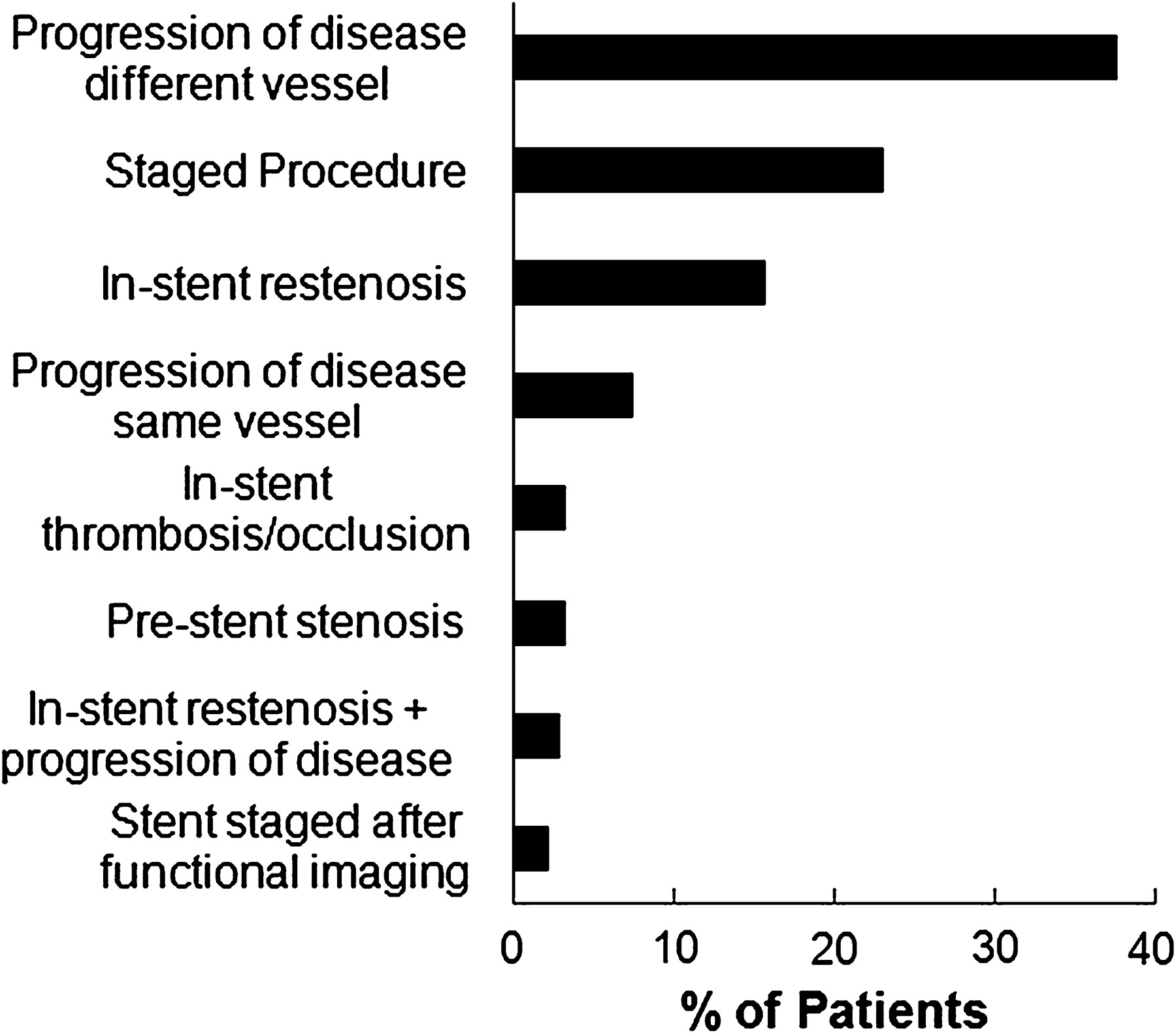
Results 10 697 (43.6%) underwent PCI with stenting, 832 (3.4%) PCI alone, 4589 (18.7%) coronary artery bypass surgery (CABG) and 8133 (33.2%) medical treatment. Two thousand four hundred and seventy-seven of the 10 697 stented patients (23.2%) returned for a second angiogram and 1314 (12.3%) underwent further stenting and 211 (2.0%) CABG over a median follow-up of 4.25 years (IQR 2.13–6.13 years). Three hundred and eighty-four patients (29.2%) of those requiring a second stenting procedure underwent a third angiogram during the follow-up period and 161 (12.3%) underwent further stenting and 33 (2.5%) CABG. Rates of stenting for the fourth, fifth and sixth procedures were respectively 21%, 24% and 38% representing 0.3%, 0.1% and 0.02% of the initial stented cohort (Abstract 130 Figure 1). 59.9% of repeat PCI stenting procedures were elective, 38.1% urgent and 1.5% primary. Clinical indications for repeat stenting are shown in Abstract 130 Figure 2. A minority of patients (15.7%) required restenting for in-stent restenosis with most patients returning either with disease progression in an unstented area (45.2%) or for staged PCI (25.2%). Stent thrombosis as an indication for repeat stenting was rare (3.3%). Of those requiring restenting, 37.2% patients received drug eluting stents (DES) in their first stenting procedure and 62.8% received bare metal stents (BMS) alone. 5.4% of patients had both DES and BMS in the same procedure. This did not differ significantly from the ratio of DES/BMS in those patients undergoing stenting who did not require further revascularisation in the follow-up period (39% DES, 61% BMS, 14.8% both DES and BMS). 19.3% people requiring a second stenting procedure had multi vessel stenting at first PCI.

Patient undergoing multiple restenting procedures.
{kind=link}
{kind=link}
Most common indications for restenting procedures.
Conclusion and Implications This study shows that in a large unselected ‘real world’ cohort of patients undergoing stenting, a substantial minority of patients undergoing a first stenting procedure will require repeat assessment (23%) and/or repeat stenting (12%). However the driving force behind repeat stenting procedures is progression of disease distant from the site of the first stent (45%) and staged PCI (25%) rather than isolated stent-related restenosis which accounts for under 16% of second stenting procedures and thus a minority of restenting cases.
- percutaneous intervention
- restenosis
- stenting