Article Text

Abstract
Objective The acute administration of high-dose erythropoietin (EPO) on reperfusing ischaemic myocardium has been reported to halve myocardial infarct (MI) size in preclinical studies, but its effect in ST elevation myocardial infarction patients undergoing primary percutaneous coronary intervention (PPCI) remains unknown. We investigated whether high-dose EPO administered as an adjunct to PPCI reduces MI size.
Design Double-blinded, randomised, placebo-controlled.
Setting Single tertiary cardiac centre.
Patients Fifty-one ST elevation myocardial infarction patients undergoing PPCI.
Interventions Patients were randomly assigned to receive either a single intravenous bolus of EPO (50 000 IU) prior to PPCI with a further bolus given 24 h later (n=26) or placebo (n=25).
Main outcome measures MI size measured by 24 h area under the curve troponin T and cardiac magnetic resonance imaging performed on day 2 and at 4 months.
Results EPO treatment failed to reduce MI size (troponin T area under the curve: 114.6±78 μg/ml EPO vs 100.8±68 μg/ml placebo; infarct mass by cardiac magnetic resonance: 33±16 g EPO vs 25±16 g placebo; both p>0.05). Unexpectedly, EPO treatment doubled the incidence of microvascular obstruction (82% EPO vs 47% placebo; p=0.02) and significantly increased indexed left ventricular (LV) end-diastolic volumes (84±10 ml/m2 EPO vs 73±13 ml/m2 placebo; p=0.003), indexed LV end-systolic volumes (41±9 ml/m2 EPO vs 35±11 ml/m2 placebo; p=0.035) and indexed myocardial mass (89±16 g/m2 EPO vs 79±11 g/m2 placebo; p=0.03). At 4 months, there were no significant differences between groups.
Conclusions High-dose EPO administered as an adjunct to PPCI failed to reduce MI size. In fact, EPO treatment was associated with an increased incidence of microvascular obstruction, LV dilatation and increased LV mass.
Clinical Trial Registration Information http://public.ukcrn.org.uk/search/StudyDetail.aspx?StudyID=4058 Unique Identifier=Study ID 4058.
- Erythropoietin
- primary percutaneous coronary intervention
- ST-elevation myocardial infarction
- cardiac MRI
- microvascular obstruction
- MRI
- coronary intervention
- myocardial viability
- reperfusion
Statistics from Altmetric.com
- Erythropoietin
- primary percutaneous coronary intervention
- ST-elevation myocardial infarction
- cardiac MRI
- microvascular obstruction
- MRI
- coronary intervention
- myocardial viability
- reperfusion
Introduction
Despite recent advances in primary percutaneous coronary intervention (PPCI), the morbidity and mortality of ST-elevation myocardial infarction (STEMI) patients remain significant. This may be due, in part, to the presence of lethal myocardial reperfusion injury, a phenomenon in which the reperfusion of ischaemic myocardium induces further cardiomyocyte death, thereby limiting the beneficial effects of myocardial reperfusion by PPCI.1 Therefore, novel cardioprotective agents capable of reducing lethal myocardial reperfusion injury are required to realise the full benefits of reperfusion therapy, limit myocardial infarct (MI) size, preserve cardiac function and improve clinical outcomes in these patients.
There is considerable evidence that the cytokine erythropoietin (EPO) exerts pleiotropic effects beyond that of haematopoiesis, which include both neuroprotection and cardioprotection.2 In preclinical studies, a number of beneficial pleiotropic effects of EPO have been reported, including stimulation of neovascularisation, beneficial peri-infarct and myocardial remodelling as well as direct cellular protective effects, which, by activating a number of cell survival pathways, render the myocyte more resistant to ischaemia–reperfusion injury.2 The acute administration of high-dose EPO at the time of reperfusion has been reported in animal models to reduce MI size by approximately 50%.2 Initial pilot studies in patients have demonstrated safety with high-dose EPO.3 4 Whether EPO is beneficial in STEMI patients when administered as an adjunct to PPCI remains unknown.
Methods
Patient selection
This study received local Ethics Committee approval and was carried out in accordance with the University College London Hospital Trust guidelines. Between July 2007 and August 2009, we conducted a randomised, double-blinded, placebo-controlled trial of STEMI patients referred to a single tertiary cardiac centre for PPCI. We obtained written informed consent from all patients who entered the study. Patients were included if they presented for PPCI within 12 h of onset of symptoms and had the following ECG criteria (≥2 mm ST-elevation in chest ECG leads, ≥1 mm ST-elevation in contiguous limb leads or new-onset left bundle branch block), were under 80 years old with a single-vessel culprit lesion and had Thrombolysis in Myocardial Infarction grade 0 and Rentrop collateral grade 0 on coronary angiography. Exclusion criteria included abnormal renal function (serum creatinine >120 μmol/l), known thromboembolic disorder, malignant disease, multivessel disease, cardiogenic shock and cardiac arrest. Patients were excluded from cardiac magnetic resonance (CMR) imaging if they had any metal implants which rendered CMR unsafe or if they were claustrophobic.
Procedures
Eligible consenting patients were randomly allocated to receive either EPO treatment or placebo prior to PPCI. A computer-generated blocked randomisation list was prepared in advance of the trial. Treatment allocation was undertaken by a Clinical Research Fellow (not involved with assessing clinical outcomes or the PPCI procedure) using sealed opaque envelopes. The patient, the PPCI operator and the assessor of clinical outcomes were blinded to the treatment allocation.
The EPO treatment arm comprised 50 000 IU of rhEPOβ (NeoRecormon, Roche Ltd., Welwyn Garden City, UK) in 10 ml 0.9% saline, whereas the placebo comprised 10 ml 0.9% saline. Either was administered via a peripheral intravenous cannula over 2 min prior to any device crossing the occluded vessel during PPCI, with an additional rhEPOβ dose or placebo administered via the same route 24 h following PPCI. Once reconstituted, the solutions appeared identical. The dose of rhEPOβ was obtained from a previously published proof-of-concept clinical study which suggested that rhEPOβ (33 000 IU) administered daily for 3 days (total dose 99 000 IU) may be beneficial in patients with stroke.3 PPCI was undertaken according to the cardiologists' preference, although thrombolytics and adenosine were not used. Blood samples for troponin T and creatine kinase-MB (CK-MB) were taken prior to PPCI and 6, 12 and 24 h post-procedure. Blood samples for haemoglobin, haematocrit, platelet count, prothrombin time and renal function were taken at baseline and at 2 days post-PPCI.
The primary endpoint was MI size as determined by late gadolinium enhancement (LGE) CMR. Secondary endpoints included 24 h area under the curve (AUC) serum CK-MB and troponin T, myocardial salvage index and CMR-determined left ventricular (LV) volumes, mass and ejection fraction and the presence of microvascular obstruction (MVO).
CMR imaging
CMR imaging was performed at a median of 2 days from PPCI (range 1–6 days) and repeated at 4 months using a 1.5 T scanner (Avanto-Siemens, Erlangen, Germany). LV function and volumes were assessed by standard steady-state free precession technique. Consecutive short-axis views were obtained by encompassing the LV from base to apex; vertical and horizontal long-axis views were acquired. Typical image parameters were as follows: echo time (TE) 1.16 ms, repetition time (TR) 2.73 ms, flip angle 65°, matrix 144×192, slice thickness 7 mm, gap 3 mm. A velocity-encoded aortic flow map was acquired to confirm LV volumes. Rest myocardial perfusion images were evaluated with a first-pass technique using a T1-weighted multishot gradient echo-planar inversion-recovery sequence (TR 2.6 ms, TE 1.1 ms, inversion time (TI) 200 ms, flip angle 12°, slice thickness 10 mm). Three short-axis slices (basal, mid-cavity and apex) were obtained injecting 0.2 mmol/kg gadolinium (Dotarem; Guerbet SA, Paris, France) at 2 ml/s followed by a 20 ml saline flush into an anterocubital vein. Early gadolinium enhancement images were acquired 1–2 min after gadolinium injection with a fixed TI of 440 ms. Two-dimensional slices in LV short axis were imaged with no interslice gap (TR 7.0 ms, TE 4.9 ms, flip angle 23°). LGE images were acquired in long- and short-axis views with a segmented inversion-recovery fast gradient echo sequence 10 min after the contrast injection. Sequence parameters were as follows: TR 8.9 ms, TE 4.9 ms, flip angle 25°, slice thickness 7 mm, gap 3 mm. The TI was optimised to null normal myocardium.
CMR analysis
All CMR images were analysed by an experienced CMR reader (A.J.L. or J.H.). All LV volume data were independently and blindly analysed by both readers. LV ejection fraction (LVEF) and end-systolic and end-diastolic volumes and mass were calculated from segmentation of the LV and indexed to body surface area. The rest perfusion, early gadolinium enhancement and LGE images were assessed qualitatively for the presence or absence of MVO as an area of hypoenhancement on the early and LGE scans (see figure 1). MI mass was measured by manual segmentation of areas of LGE and analysed by concordance between the two readers. In case of discordance, blinded review by a level III accredited CMR reader (J.C.M. or D.J.H.) was performed. Analysis was performed using OsiriX (version 3.5.1) software. Interobserver variability was calculated.
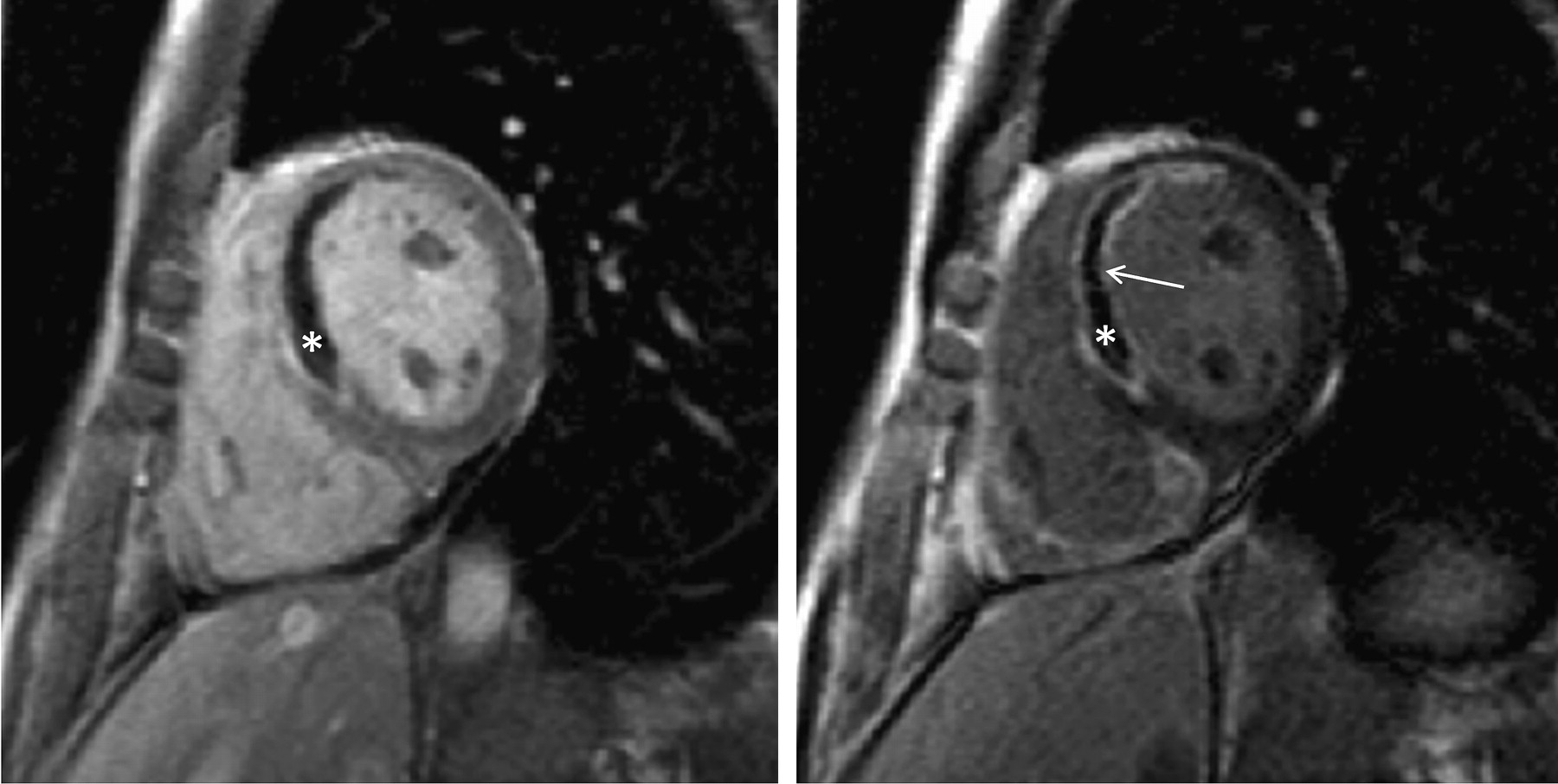
Representative images of an initial CMR scan displaying early gadolinium enhancement revealing evidence of microvascular obstruction (left panel*) and late gadolinium enhancement (right panel) depicting a transmural myocardial infarct (arrow) with a core of microvascular obstruction (*).
Determining the myocardial salvage index
When assessing the efficacy of a reperfusion treatment strategy, it is essential to express MI size (IS) as a percentage of the area at risk (AAR). In this study, the AAR was quantified using both coronary angiography (modified Bypass Angioplasty Revascularisation Investigation (BARI) and Alberta Provincial Project for Outcome Assessment in Coronary Heart Disease (APPROACH) jeopardy scores)5 and the acute CMR scan (infarct endocardial surface area (Infarct-ESA)).5 As a measure of the AAR, Infarct-ESA has been validated against the BARI and APPROACH scores5 and T2-weighted imaging of myocardial oedema.6 Myocardial salvage index was calculated as follows: (AAR−IS)/AAR.
Statistical analysis
Descriptive statistics were computed to summarise the relevant features of the data. An unpaired t test was used to test the differences in means in the EPO versus placebo groups for continuous data, and 95% CIs were calculated for the difference of the means between the EPO and placebo groups. The assumptions of the t test were examined using residuals analysis. A sensitivity analysis was performed where individual patients had Studentised residuals greater than two SDs by omitting these patients from the analysis and examining the impact to the mean difference and 95% CIs. A Bland–Altman plot was used to calculate the difference and limits of agreement between the two observers for each continuous clinical measurement. The number of measurements falling outside the limits of agreement was used as a heuristic guide to agreement. A paired t test of the measurements was used to formally test that the difference of the means of the two measurements was zero. In addition, the reliability (intraclass correlation) was computed for each continuous clinical measurement. A κ statistic was calculated to measure the observer agreement for categorical clinical measurements. For categorical data, a Z-test of proportions was used to test the equality of the proportion of patients in the EPO group versus the control group. An approximate 95% CI for the difference in the proportions in the two groups was also calculated.
At study conception, a sample size of at least 44 patients in total was determined based on the following assumptions: (a) a 36% reduction in 72 h total CK release from 326 095 to 208 984 arbitrary units; (b) power of at least 80%; (c) an SD of 135 846 arbitrary units and (d) significance declared at the two-sided 5% level.7 However, due to the nonspecificity of total CK measurements along with the advent and validation of CK-MB and troponin T, these were measured instead. However, with the advent of newly presented data, we were able to retrospectively validate the sample size of the study using the endpoint of CMR-assessed MI size. The infarct-limiting effects of ciclosporin A were investigated in a similar cohort of patients. A sample size of at least 40 patients in total was determined based on the following assumptions: (a) a 20% reduction in mass of MI as measured by CMR scan from 46 g to 37 g; (b) power of at least 80%; (c) an SD of 10 g and (d) significance declared at the two-sided 5% level.8
All analyses were done with Stata V.11 or SPSS statistical software V.15.0.
Results
Figure 2 shows the trial profile. One hundred and ten patients were screened for inclusion in the study, with 51 patients randomised to receive either placebo (n=25) or rhEPOβ (n=26). The treatment group characteristics are summarised in table 1. There was good agreement using the three different scores to measure the AAR. Table 2 summarises the AAR scores and the main results. MI size was assessed by 24 h AUC serum troponin T (114.6 μg/ml EPO vs 100.8 μg/ml placebo (95% CI −29.7 to 57.3)) and CK-MB (4682 U/l EPO vs 3649 U/l placebo (95% CI −563 to 2629)) and by the initial (33 g EPO vs 25 g placebo (95% CI −2.8 to 17.7)) and follow-up (18 g EPO vs 12 g placebo (95% CI −0.6 to 11.2)) CMR scans.

{kind=link}
{kind=link}
Trial recruitment profile.
Patient characteristics
Clinical outcomes
Unexpectedly, at the initial CMR scan, the presence of MVO was almost doubled in the EPO-treated group when compared to placebo. Furthermore, there was an increase in indexed LV end-systolic and end-diastolic volumes and mass in the EPO-treated group compared to placebo. There were no significant differences between the groups in terms of the LV stroke volume index and LVEF and the myocardial salvage index. There were no significant differences in the CMR endpoints on the 4-month follow-up scan, although there was a trend to increased IS and reduced LVEF in the EPO-treated group compared to placebo.
There was good to excellent agreement between observers with the intraclass correlation ranging from 0.7 to 0.95.
All serious adverse events were reported to the safety committee and investigated. There was no significant difference in adverse events between the two groups. There were no deaths in the eligible patients randomised to EPO. There was one death in the placebo group during a subsequent PCI to the nonindex vessel. There were five admissions to hospital for evaluation of chest pain in the EPO group and one in the placebo group, none of which were deemed a new acute coronary syndrome. There were two planned PCI procedures in both groups and one planned coronary artery bypass graft surgery in the EPO group. One LV apical thrombus was found at 4 months in the EPO group.
Discussion
The major findings of this double-blinded, randomised clinical trial are that the administration of high-dose rhEPOβ as an adjunct to PPCI had no beneficial effects in terms of MI size, myocardial salvage index or LVEF. In fact, the findings suggest that rhEPOβ may actually be detrimental in this setting, as it almost doubled the incidence of MVO. Furthermore, it was associated with acute LV dilatation and an acute increase in myocardial mass. On the 4-month follow-up CMR scan, there were no significant differences between the treatment groups.
It is well established that in STEMI patients successfully treated with PPCI, the presence of MVO is associated with worse clinical outcomes.9 10 MVO can be detected in about 30%–40% of PPCI patients using echocardiography11 or CMR,10 12 even in the presence of Thrombolysis in Myocardial Infarction grade III coronary artery flow post-PPCI. In our study, in patients treated with rhEPOβ, the incidence of MVO detected by the initial CMR scan was dramatically increased from 47% in placebo to 82%, a finding which might be expected to be associated with worse clinical outcomes. Importantly, factors which are known to impact on the development of MVO such as the presence of comorbid conditions, antiplatelet and anticoagulant therapy and MI size were not significantly different between the two treatment groups. MVO results in poor myocardial perfusion despite epicardial coronary artery revascularisation, and its development has been attributed to a variety of factors including distal embolisation, endothelial dysfunction, leucocyte migration and plugging and platelet aggregation.13 The mechanism underlying the increased incidence of MVO following PPCI in the rhEPOβ-treated group in our study is unknown but may be attributed to the increased platelet reactivity and the prothrombotic effects which have been described with rhEPO therapy in healthy subjects and a number of different disease states.14 15 Interestingly, high-dose rhEPO (intravenous 400 IU/kg given daily for 3 days) significantly blunted the aspirin-mediated increase in bleeding time when compared with placebo in healthy volunteers, although no effect was observed on the clopidogrel-mediated increase in bleeding time.16
The explanation for the significantly increased myocardial mass (calculated from the myocardial volume) observed on the initial CMR scan in patients treated with rhEPOβ is unknown. It may have been due to enhanced myocardial oedema associated with more severe myocardial reperfusion injury, as suggested by the greater incidence of MVO in the rhEPOβ-treated patients. In this respect, an increased indexed myocardial mass has been noted by CMR 1 week following an acute myocardial infarction in a previous study.17 The acute LV dilatation noted in patients treated with rhEPOβ may well be a compensatory response to greater myocardial injury, where an increase in preload provokes LV dilatation in an attempt to maintain the LV stroke volume.
Initial pilot investigations of rhEPO in human settings of stroke,3 non-STEMI18 and STEMI4 have demonstrated safety and a potential trend to benefit in terms of reduction in IS. These pilot studies were initiated following a considerable number of preclinical studies demonstrating a range of beneficial effects in small animal infarct models (reviewed by Riksen et al2), with protective actions thought to be mediated via the EPO receptor which has been demonstrated in human cardiomyocytes.19 Interestingly, the infarct-limiting effects of EPO as reperfusion therapy in larger animal studies of ischaemia–reperfusion injury such as sheep20 and porcine21 have been negative.
Subsequently, several studies have investigated high-dose rhEPO as a novel cytoprotective agent in STEMI. The administration of rhEPOβ (30 000 IU) prior to tenecteplase thrombolysis in STEMI patients failed to find any difference in cardiac enzyme release or any difference in major adverse cardiac events.22 A pilot study of 30 PPCI patients has reported that the administration of rhEPOα (33 000 IU daily for 3 days) reduced CK-MB release but failed to limit MI size on a CMR scan performed within 3 days of PPCI.23 In that study, the effect of rhEPOα on CMR-detected MVO was not reported. A lower dosing regimen of 12 000 U rhEPOβ following PPCI for STEMI in 36 patients24 was unable to demonstrate a difference in the primary endpoint of LVEF by radionucleotide scintigraphy between groups.
Regenerate Vital Myocardium by Vigorous Activation of Bone Marrow Stem Cells (REVIVAL-3) reported that treatment with rhEPOβ (33 333 IU daily for 3 days) starting immediately after successful PPCI in 138 patients made no difference to LVEF measured at 6 months by CMR and that there was a trend to adverse cardiovascular outcomes (death, recurrent myocardial infarction, infarct-related artery revascularisation and stroke).25 The HEBE-3 study26 recruited 529 patients undergoing PPCI and randomised to 60 000 IU of rhEPOα or placebo within 3 h following reperfusion. There was no significant difference in the primary endpoint of LVEF at 6 weeks by radionucleotide ventriculography. The authors reported secondary endpoints of a favourable safety profile and a statistically significant reduction in adverse events, although total numbers of events were small.
Further studies in other clinical settings of ischaemia–reperfusion injury including coronary artery bypass graft surgery27 and stroke15 have also been negative, with significantly increased adverse events reported in patients with stroke treated with rhEPOα within 6 h of stroke onset.
In our study and those above, the failure of rhEPO to reduce MI size in PPCI patients is in conflict with the preclinical data reporting 50% reductions in MI size in rat, rabbit and dog models of ischaemia–reperfusion injury, with EPO administered at time of reperfusion.2 We administered the rhEPOβ prior to any device crossing the occluded coronary artery in order to ensure that high serum levels of EPO were present at the moment of reperfusion, aiming to prevent myocyte injury caused at this time. The dose was the same total dose as that in a promising pilot study in stroke and has been shown to generate high serum EPO levels3; a study of a lower dose of rhEPO is also negative,24 and the majority of successful animal studies have been performed with very high doses of between 350 and 5000 IU/kg.2 Discordant findings between preclinical animal studies and the clinical translation of novel cardioprotective strategies has been a recurring issue, the causes of which have been highlighted in several recent articles.1 28 Specifically, the proinflammatory and prothrombotic conditions associated with an acute myocardial infarction in a middle-aged patient with comorbidities such as diabetes, dyslipidaemia and hypertension are not reproduced by experimental coronary artery occlusion in disease-free juvenile small- to medium-size animal models.
Furthermore, there has been a recent challenge to the pleiotropic abilities of EPO and doubt cast over the presence of biologically active EPO receptor in tissues not involved in erythropoeisis29; however, this paper has been criticised by a large body of researchers for overstating its conclusions30 and not providing enough evidence for which to discount the work of a large body of other investigators. Thus, the debate as to the exact abilities of EPO continues; however, our study and others have been unable to demonstrate a benefit of acute high-dose EPO in the setting of STEMI, and a number of studies have raised concerns about adverse events. Further studies should be performed with caution, given the current uncertainty about the potential mechanism for an increase in associated adverse events. Further work continues in elucidating the protective pathways of EPO in the preclinical setting and exploring EPO analogues (such as carbamylated EPO), which may provide protective benefits without the apparent associated side effects.
In summary, we have demonstrated that the administration of high-dose rhEPOβ as an adjunct to PPCI failed to reduce MI size or improve cardiac function. In fact, its use may actually be detrimental in that it was associated with a doubling in the incidence of MVO, acute LV dilatation and increased myocardial mass. This study highlights the importance of CMR as a technique for assessing the safety and efficacy of novel reperfusion therapies. The findings from the current study should be considered, alongside those of other recently published studies, in the design of future studies investigating the use of high-dose rhEPO in patients with acute myocardial infarction.
Acknowledgments
We thank the British Heart Foundation (Program Grant RG/03/007) for their ongoing funding and support. We offer our grateful thanks to all the patients and staff, particularly Drs Clare Dollery, Dominic Rogers, Alamgir Kabir, Anoop Shetty, Paul Kotwinski, Vanessa Cobb, Vineet Wadhera, A.B. Gopalamurugan and Costas O'Mahoney at The Heart Hospital for their assistance during this study.
References
Footnotes
See Editorial, p 1537
Funding The work was supported by Roche Ltd. which kindly supplied the rhEPOβ (NeoRecormon), but it played no role in conception, conduct or analysis of this study. This work was undertaken at University College London Hospital/University College London which received a proportion of funding from the Department of Health's National Institute of Health Research Biomedical Research Centres funding scheme.
Competing interests None declared.
Patient consent Obtained.
Ethics approval This study was conducted with the approval of the University College London R&D department.
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- Editorial
- PostScript