Article Text

Abstract
Introduction Early inward motion and thickening/thinning of the ventricular septum associated with left bundle branch block (LBBB) is known as the septal flash (SF). Correction of SF corresponds with CRT response. We hypothesise that electromechanical interactions induced by SF are associated with functional changes in conductivity and a “U-shaped” activation pattern. Characterising the spatio-temporal relationship between electrical and mechanical events may explain why patients with a SF respond to CRT. Methods 13 patients (63±10 years, 10 men) with severe heart failure (EF 22.8±5.8%) undergoing CRT underwent echocardiography and non-contact mapping (NCM) pre-implant. Presence and extent of a SF was defined visually and with M-mode and fused with NCM bull′s eye plots of endocardial activation patterns. LV dP/dtmax was measured during different pacing modes.
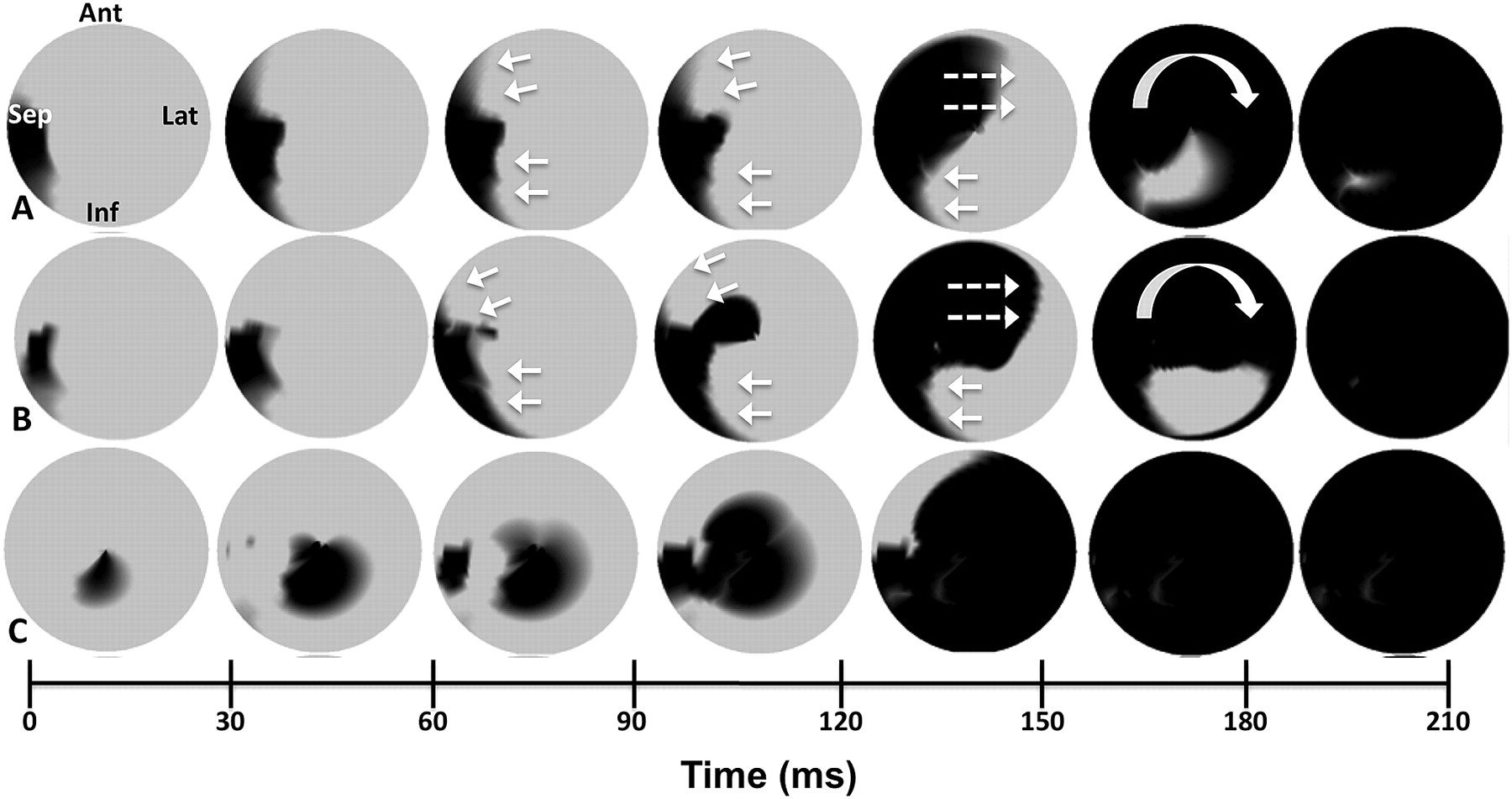
Results Five patients had a large SF, four small SF and four no SF. Patients with large SF had areas of conduction block in non-infarcted regions whereas those with small or no SF did not (Abstract 89 figure 1). Patients with large SF had greater acute response to left ventricular (LV) and biventricular (BIV) pacing vs those with small/no SF (% increase dP/dt 28±14% vs 11±19% for LV pacing and 42±28% vs 22±21% for BIV pacing). The lines of conduction block disappeared after LV and BIV pacing, while remaining present with RV pacing (Abstract 89 figure 2). Abstract 89 figure 1 Patient with a large SF. Unipolar isochronal map with NCM electrograms showing fragmented signals (development of split potentials) indicating a reduction of conduction and inability to cross throughout the inferior region. The NCM mapping electrograms show the criteria used by Auricchio et al to define block, with the emergence of R-wave, smallest and earliest at the superior part of the block (where area of block begins) with largest negative peak. Bold white arrows on the electrogram indicate how the electrical activation spreads superiorly in a U-shape pattern leading to the development of split potentials. Abstract 89 figure 2 Activation maps of patient with a large SF. Row A, baseline with area of block and late anterior breakthrough. Row B, RV pacing showing the area of anterior block remains. Row C, BIV pacing. Functional conduction block has disappeared.

{kind=link}
{kind=link}
Conclusion A strong interaction exists between electrical activation and mechanical deformation of the septum. Correction of both mechanical synchrony and the functional conduction block by CRT may explain the large positive response in patients with a SF.
- Cardiac resynchronisation therapy
- septal flash
- heart failure