Article Text

Abstract
Background The diagnosis of acute myocarditis can be challenging. Cardiovascular magnetic resonance imaging (CMR) can be a useful tool in this setting but often requires multiple modalities for tissue characterisation, including T2-weighted (T2w), early and late gadolinium imaging. Cardiac T1-mapping is a novel technique that is, quantitative and is also sensitive to acute changes in free water content without the need for exogenous contrast agents. We hypothesised that non-contrast T1-mapping can serve as a new diagnostic criterion for acute myocarditis.
Methods We studied 23 patients with suspected acute myocarditis and 17 healthy controls. All patients presented with chest pain and troponin I >0.04 ug/l and non-obstructive coronary arteries (either on coronary angiogram or ruled out by clinical criteria such as young age or no cardiac risk factors). CMR (at 1.5 T) within 10 days included (1) T2-weighted imaging (using the STIR sequence) for oedema; (2) T1-mapping (using the ShMOLLI sequence); and (3) late gadolinium enhancement (LGE) imaging for patterns of cell necrosis (Abstract 091 figure 1). Myocardial T2 signal intensity (SI) relative to skeletal muscle (T2 SI ratio) for detection of oedema and absolute T1 values per-subject were analysed.

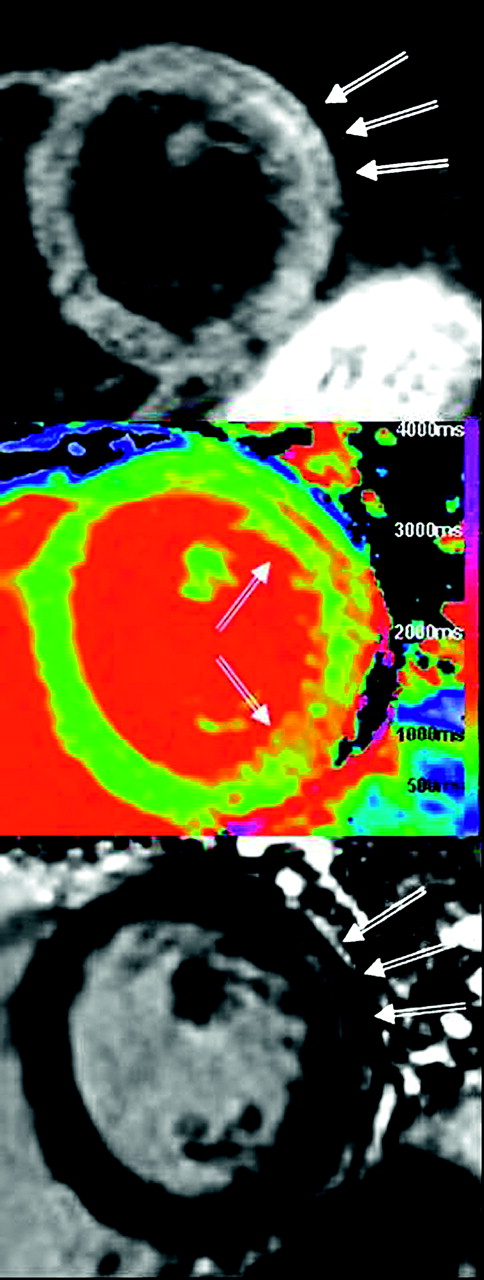
Acute myocarditis. (Top) STIR demonstrating increased signal intensity in the mid lateral wall. (Middle) ShMOLLI T1-map demonstrating increased T1 values (1100–1200 ms) in the lateral wall. (Bottom) LGE imaging demonstrating mid-wall enhancement in the lateral wall.
Results All patients had a CMR diagnosis of acute myocarditis based on both positive T2-weighted imaging and typical non-ischaemic type LGE pattern. Compared to controls, both mean myocardial T1 and T2 SI ratio in patients were significantly higher (T1=1036±71 ms vs T1=938±19; T2 SI ratio=1.77±0.24 vs 1.52±0.10, p<0.0002 for both). Receiver operator characteristics analysis showed excellent diagnostic performance for both methods: the area-under-the-curve for T1-mapping=0.96 and T2-weighted imaging=0.93 (p=0.3, Abstract 091 figure 2). At a T1 value of 958 ms, the sensitivity and specificity were 87%.

{kind=link}
{kind=link}
ROC curves for ShMOLLI T1-mapping and T2-STIR in acute myocarditis.
Conclusions Non-contrast T1-mapping has a high diagnostic performance for acute myocarditis and may be used as a novel additional CMR diagnostic criterion.
- T1-mapping
- cardiovascular magnetic resonance
- myocarditis