Article Text

Statistics from Altmetric.com
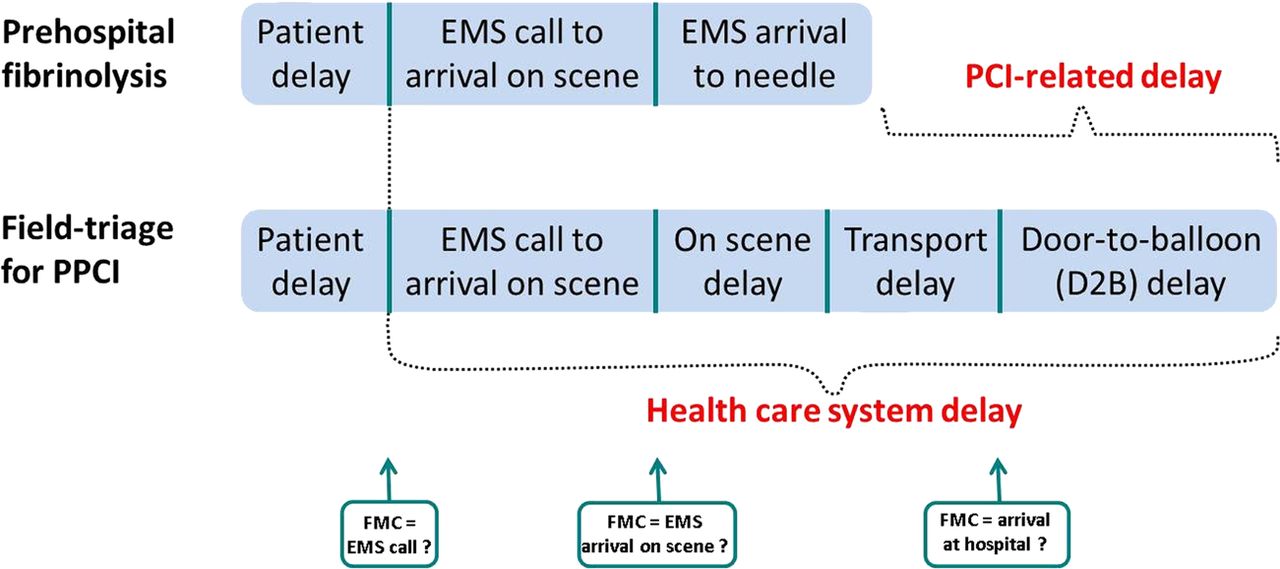
The 2012 European Society of Cardiology (ESC) ST-Elevation Myocardial Infarction (STEMI) guideline acknowledges that STEMI patients should receive reperfusion therapy as soon as possible, and that prehospital fibrinolysis or field-triage directly to Primary Percutaneous Coronary Intervention (PPCI) centres is the preferred reperfusion strategy.1 However, when recommending fibrinolytic therapy (FT) within 30 min from First Medical Contact (FMC), if PPCI cannot be performed ‘within 60 min of FMC in patients presenting early, with a large amount of myocardium at risk’, the guidelines imply that only 30 min extra may be expended to perform PPCI instead of administering FT (‘PCI-related delay’) (figure 1).
{kind=link}
Various delays when treating patients with ST-Elevation Myocardial Infarction (STEMI) with fibrinolysis or primary percutaneous coronary intervention (PPCI). ‘Healthcare system delay’ is the total delay from emergency medical service (EMS) call to PPCI. ‘PCI-related delay’ is the extra delay that one may use to perform PPCI instead of administering fibrinolysis and still achieve a mortality benefit from PPCI. First Medical Contact (either EMS call, EMS arrival on scene, or arrival at hospital according to regional STEMI system of care).
Throughout the years, successive guidelines have mistakenly equated ‘PCI-related delay’ and ‘FMC to PPCI’ (the total delay from FMC to PPCI) (figure 1). This error persists in the recently updated ESC guideline.1 Clarification of this distinction is of paramount importance because of the suggested reduction in the ‘window of opportunity for PPCI’, a suggestion not clearly supported by evidence, which has significant public health implications. In paragraph 3.5.2, the ESC STEMI guideline references a registry analysis from the National Registry of Myocardial Infarction (NRMI),2 concluding: ‘primary PCI (wire passage) should be performed within 90 min after FMC in all cases. In patients presenting early, with a large amount of myocardium at risk, the delay should be shorter (<60 min).’ The NRMI reference is also listed in paragraph 3.4.1 in the ESC STEMI guideline when recommending the acceptable ‘FMC-to-PCI’ delay of only 60 min in early incomers with anterior infarction. However, this study describes ‘PCI-related delay’, that is, the theoretical extra delay that may be spent to perform PPCI over FT (figure 1). The NRMI manuscript by Pinto et al. does not describe ‘FMC-to-PCI’ delay in the cohorts evaluated since timing of Emergency Medical Service (EMS) evaluation was imprecise. The only delay data available were the interval ‘Door-to-balloon (D2B)’ delay, which was 116 min when calculated as a weighted mean (table 1). Given the fact that ‘FMC-to-PCI’ is considerably longer than D2B delay among patients transported by EMS (figure 1), the ‘FMC-to-PCI’ delay is likely to have been considerably longer than 120 min (table 1). Consequently, these data cannot be applied recommendations regarding the optimal time to ‘FMC to PCI’ or to support a recommendation ‘of a systems goal of FMC to PCI of 60 min.’ It would appear that the 2012 STEMI guideline authors,1 when compiling the overwhelming amount of scientific data, have either intended to use a different reference or misinterpreted the findings from Pinto et al’s original work.2 We are not aware of supportive data that would justify the current STEMI guideline recommendations to consider fibrinolysis within 30 min of FMC when PPCI cannot be performed within 60 min of FMC.
Delays to PPCI observed in the references used for recommendation of a First Medical Contact (FMC) to PPCI delay below 60 min in the recent European Society of Cardiology 2012 STEMI-guidelines
There have been several other studies addressing the optimal ‘PCI-related delay’. The initial study by Pinto and colleagues was limited by the fact that optimal FT (fibrin-specific drugs) was compared with a less-than-optimal PPCI strategy (PPCI centres performing only a mean of 20 PPCI procedures a year).2 A later analysis by Pinto and colleagues found an acceptable ‘PCI-related delay’ of approximately 120 min without any excessive mortality in PPCI-treated patients with anterior infarction or short symptom duration, even at a PCI-related delay of approximately 120 min.3 While the magnitude of survival difference between PPCI and FT decreased as delay to PCI increased, at no point did mortality for PPCI exceed that with FT. These findings are concordant with the previous findings by Boersma and colleagues that were based on individual data from studies comparing FT with PPCI.4 Swedish registry data indicate a comparable outcome from PPCI and FT, even with a PCI-related delay of 240 min, and observations from both the French FAST-MI registry and the Vienna registry report comparable outcomes for patients treated with FT and PPCI with a PCI-related delay of 90 min.5–7
The ESC STEMI guideline also relies upon analysis of the Comparison of Angioplasty and Pre-hospital Thrombolysis in Acute Myocardial Infarction (CAPTIM) trial when recommending a ‘FMC-to-PPCI’ delay of 60 min.8 This non-prespecified subgroup analysis, based on 460 patients, claimed a lower mortality in patients randomised to FT versus PPCI among subjects presenting early. However, this finding did not reach statistical significance. A much larger meta-analysis including individual data from 6763 patients demonstrated superiority of PPCI over FT, in early as well as late incomers.4 This finding was also confirmed in the Swedish registry data.5 It seems that the aforementioned subgroup analysis from CAPTIM was weighted too heavily. Furthermore, findings from the CAPTIM substudy offer little value in substantiating a recommendation of ‘FMC to PPCI’ of <60 min, when the ‘FMC to PPCI’ delay must have been at least 100 min in the trial. The time from symptom onset to randomisation was 108 min in the CAPTIM trial, and the time to PPCI was 190 min, indicating that time from randomisation to PPCI was 82 min. The response time (EMS call to arrival on scene) is typically about 10 min, and the ambulance physicians must have used at least 10 min on scene before randomisation. A conservative estimate, thus, is a ‘FMC to PPCI’ delay of at least 102 min in this study. Consequently, neither the CAPTIM trial nor the NRMI analyses support a ‘FMC to PPCI’ delay of <60 min.
Creation of a clinical guideline is an immense task, and we commend the writing group for their efforts in creating a comprehensive and useful document summarising the available scientific data informing management of STEMI patients. The guidelines serve as a valuable resource, but the flow charts and suggestions may be more applicable for new STEMI networks in regions without previously established systems of care. For well-functioning STEMI networks, we believe that the best available evidence supports a PCI-related delay <120 min. If existing STEMI networks were to implement the shorter metrics introduced in the current guidelines, there is a risk of FT administration to patients where outcomes would be better with PPCI.
Finally, in regions with an ideal STEMI systems of care, with prehospital diagnosis and field-triage directly to large-volume PPCI centres, FMC is variably defined as time of EMS call9 or EMS arrival on scene. In regions that do not use prehospital diagnosis, FMC is simply the time of ambulance arrival at the hospital. In self-presenters, FMC is also time of arrival at the hospital (figure 1). It is necessary to standardise and differentiate recommendations of ‘FMC to PPCI’ depending upon whether FMC is EMS call or arrival at hospital because after all, the most important factor is rapid reperfusion with the most optimal strategy for the patient. When comparing regions based on observed ‘FMC to PPCI’ delays, it may erroneously seem that regions rightfully focusing upon prehospital diagnosis are performing inferiorly compared with regions that are not implementing prehospital diagnosis, while the opposite is likely the case. In fact, if one were to incorporate current ESC guideline recommendations of ‘FMC to PPCI delay below 60 min’, in regions using prehospital diagnosis for field-triage to PCI centres with rapid treatment times, FT would be administered to more patients compared with regions without prehospital diagnosis even though total ischaemic times would have been shorter for the patients, or even more absurdly, regions could eliminate prehospital diagnosis, increasing the ‘window of opportunity’ for PPCI.
We recommend that for future guidelines, professional societies on both sides of the Atlantic acknowledge the current confusion about the terminologies on treatment delays in STEMI and uncertainties in utilising available data for information regarding the proper treatment for various patient subsets, and avoid recommendations that may have deleterious consequences. It is uncertain whether a pharmacoinvasive strategy in the future will qualify as an alternative reperfusion strategy. However, the Strategic Reperfusion Early After Myocardial Infarction trial found no mortality benefit but an increased risk of stroke in patients randomised to a pharmacoinvasive strategy compared to patients randomised to a PPCI strategy.10
References
Footnotes
-
Contributors CJT, EB and DSP made the first draft of the viewpoint. All coauthors critically revised the viewpoint, agreed on its content and accepted it for publication.
-
Competing interests None.
-
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- Point-Counterpoint