Article Text

Abstract
Objective To expand the limited information on the prognostic impact of quantitatively obtained collateral function in patients with coronary artery disease (CAD) and to estimate causality of such a relation.
Design Prospective cohort study with long-term observation of clinical outcome.
Setting University Hospital.
Patients One thousand one hundred and eighty-one patients with chronic stable CAD undergoing 1771 quantitative, coronary pressure-derived collateral flow index measurements, as obtained during a 1-min coronary balloon occlusion (CFI is the ratio between mean distal coronary occlusive pressure and mean aortic pressure both subtracted by central venous pressure). Subgroup of 152 patients included in randomised trials on the longitudinal effect of different arteriogenic protocols on CFI.
Interventions Collection of long-term follow-up information on clinical outcome.
Main outcome measures All-cause mortality and major adverse cardiac events.
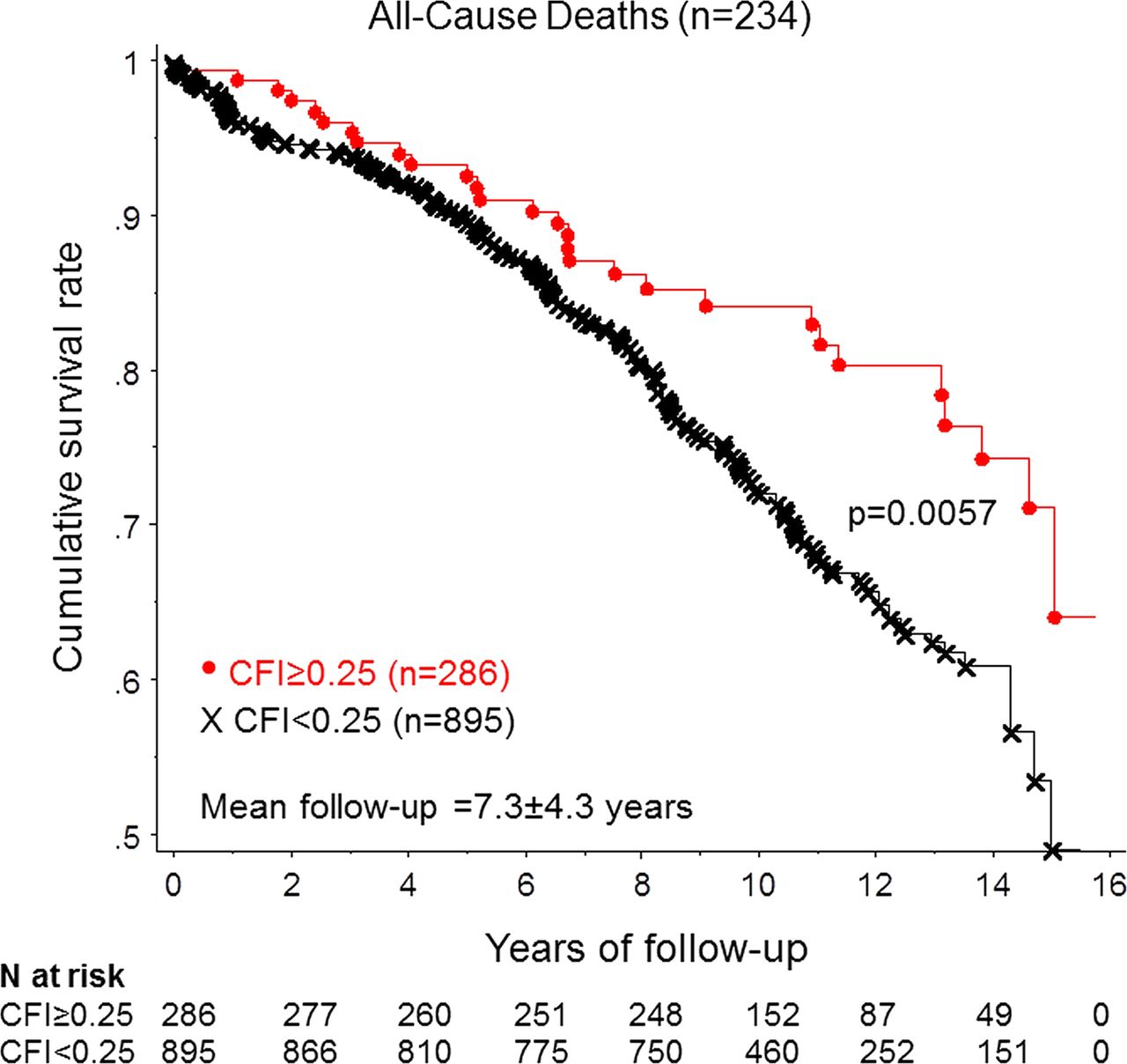
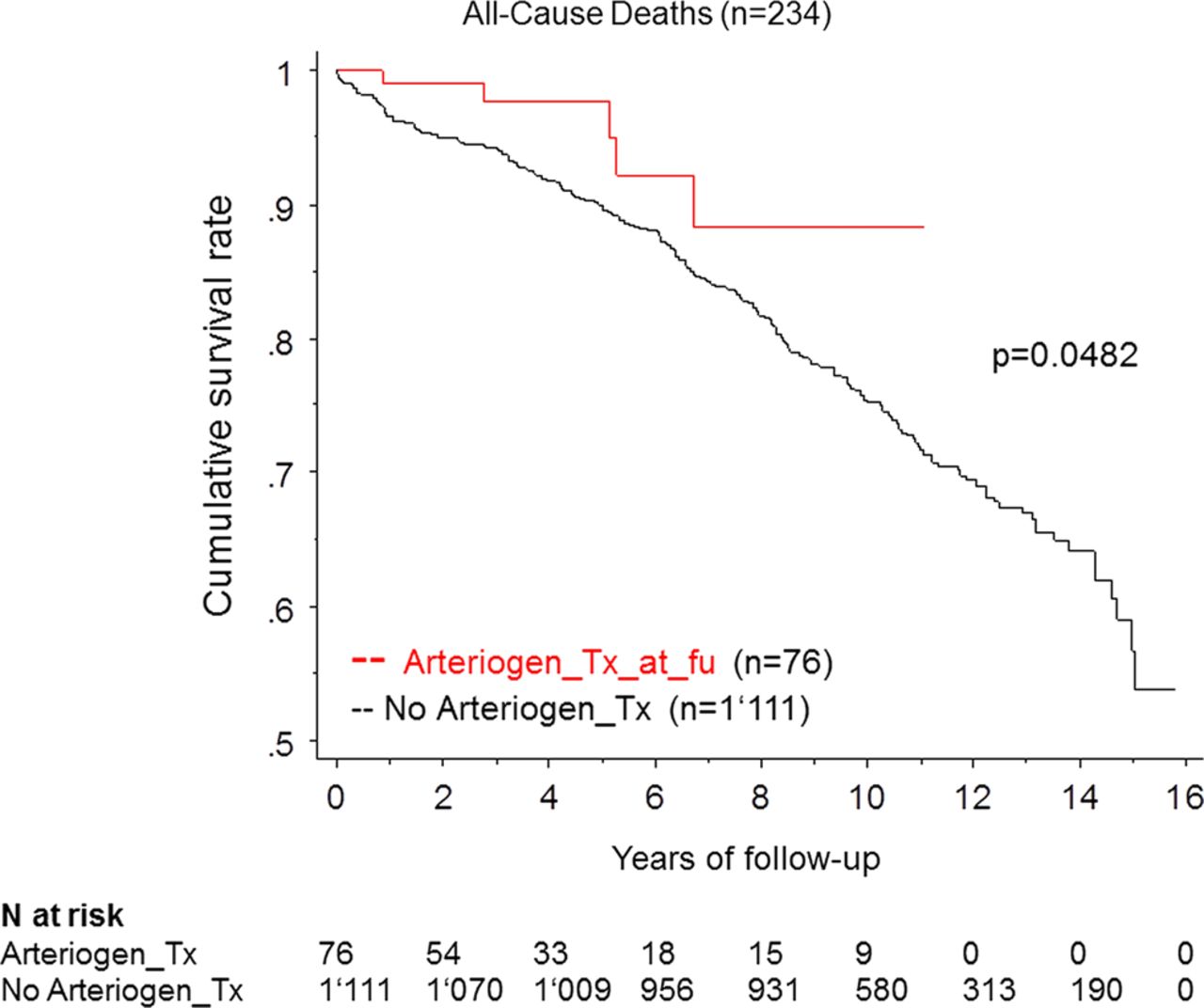
Results Cumulative 15-year survival rate was 48% in patients with CFI<0.25 and 65% in the group with CFI≥0.25 (p=0.0057). Cumulative 10-year survival rate was 75% in patients without arteriogenic therapy and 88% (p=0.0482) in the group with arteriogenic therapy and showing a significant increase in CFI at follow-up. By proportional hazard analysis, the following variables predicted increased all-cause mortality: age, low CFI, left ventricular end-diastolic pressure and number of vessels with CAD.
Conclusions A well-functioning coronary collateral circulation independently predicts lowered mortality in patients with chronic CAD. This relation appears to be causal, because augmented collateral function by arteriogenic therapy is associated with prolonged survival.
Statistics from Altmetric.com
Introduction
The debate on the structural presence of the human coronary collateral network starting in the mid 17th century was ‘overruled’ in 1881 by Cohnheim who—based on canine (!) studies—declared the coronary arteries to be end-arteries.1 It was not until the 1960s that the existence of structural coronary anastomoses was unambiguously verified by William Fulton, who had developed a pathoanatomic imaging technique that enabled differentiation between vascular overlay and true connections between adjacent parts of the circulation.2 ,3 The end of the end-artery dispute incited rather than inhibited the following argument on the ability of structural anastomoses to provide blood flow to a myocardial region in need, that is, to function properly.4 ,5 Wiggers was unable to document functional collateral vessels in the dog heart and thought it unlikely that sufficient blood supply could result from the collateral circulation in the human heart.4 Feldman and Pepine were the first to show functional coronary collaterals in patients during left anterior descending angioplasty with less ECG and haemodynamic signs of myocardial ischaemia in the presence versus the absence of angiographic collaterals.5 The term ‘functional’ in the context of coronary collaterals can not only be used in the haemodynamic but also in the prognostic sense: is the human coronary collateral circulation functional as a determinant of clinical outcome? In this context, the status of the coronary collateral circulation should be assessed functionally during occlusion rather than structurally during vessel patency by angiography in order to obtain an accurate quantitative rather than qualitative measure of the prognosticator in question.6 A recent meta-analysis including 6529 patients with chronic stable coronary artery disease (CAD) or subacute and acute myocardial infarction has found an overall 36% reduction in all-cause mortality in patients with ‘high’ versus ‘low coronary collateral circulation’, as mostly defined by angiography.7 Mortality in the presence of well-developed collateral vessels among patients who had very recently suffered a myocardial infarction has been shown to be reduced, but not independently predictive;8 the fact makes sense considering that more than 60% of the patients have angiographically poor or absent collaterals during acute myocardial infarction.9
The studies of the cited meta-analysis, including our own data using quantitative collateral flow index (CFI) measurements,10 have documented a direct association between well-developed coronary collateral function and long-term survival in chronic stable CAD. Notwithstanding even the statistical independence of coronary collateral function as a beneficial determinant of outcome, no causality of such a relation could be shown so far. The aim of the present study was to assess the impact on survival of quantitatively obtained, recruitable coronary collateral flow in a large patient population with stable CAD during 16 years of follow-up and to assess the prognostic effect of arteriogenic promotion.
Methods
Patients and study design
One thousand one hundred and eighty-one patients followed up between March 1996 and April 2012 (8573 patient years) including 150 patients without CAD, and 1031 patients with one-vessel to three-vessel chronic stable CAD underwent a total of 1771 quantitative, coronary pressure-derived CFI measurements (for calculation see below). In patients with >1 CFI measurement, a single, namely, the lowest CFI value was selected for survival data analysis. Coronary angiography was performed for diagnostic purposes in the context of chest pain. All patients and measurements were prospectively included in our CFI database, which contains approximately 56 demographic, clinical and hemodynamic variables aside from the information on recruitable collateral flow parameters obtained during a 1-min angioplasty balloon coronary occlusion (1st occlusion if >1 were performed during the same invasive procedure). Criteria for measuring collateral flow parameters were as follows: (1) no previous Q-wave myocardial infarction in the area of collateral assessment, (2) no baseline ECG ST segment abnormalities and (3) absence of acute myocardial infarction or unstable angina pectoris. For data presentation, the study population was divided into a group with low collateral flow (CFI<0.25) and one with high collateral flow (CFI≥0.25). The selected CFI cut-off between the groups has been shown to distinguish between patients with and without ST segment shift >0.1 mv on intracoronary ECG during a 1-min coronary occlusion,11 that is, between insufficient and sufficient collateral vessels. Part of the database has been previously described elsewhere.10 ,12–14
Among the 1181 patients, 152 with a total of 575 baseline and follow-up CFI measurements (76 with placebo, 76 with verum arteriogenic treatment) had been included in seven trials on the effect of different arteriogenic protocols on CFI: six of the trials (four of them published) were randomised, placebo-controlled investigations using as arteriogenic treatments granulocyte-macrophage colony stimulating factor,15 ,16 granulocyte colony stimulating factor17 and external counter-pulsation18; one trial was a non-randomised study on the effect of physical exercise training versus sedentary lifestyle on CFI.19
Follow-up information on the occurrence of all-cause mortality and major adverse cardiac events (MACE) after study inclusion was obtained by telephone interview of the patients, their relatives or their family physicians or by examination of hospital charts. MACE was defined as death due to cardiac cause, myocardial infarction, unstable angina pectoris, unplanned recurring percutaneous coronary intervention (PCI), unplanned coronary artery bypass grafting, cerebrovascular stroke and rehospitalisation for cardiac reasons. Cardiac death was defined as any death due to immediate cardiac cause (myocardial infarction, low cardiac output failure, fatal arrhythmia). Myocardial infarction was diagnosed as either one of the following criteria: typical rise and fall of cardiac biochemical markers (troponin, CK-MB) with at least one of the items being ischaemic symptoms, development of new Q-waves on ECG, ECG changes indicative of ischaemia and new Q-waves on ECG without biomarker assessment during the acute event.20
The primary study endpoint was all-cause mortality (secondary endpoints: cardiac mortality and MACE), and it was related to CFI (primarily as a continuous variable) and to the occurrence of arteriogenic therapy at the follow-up examination of the particular study. In addition to CFI, intracoronary ECG ST segment shift and chest pain, both obtained during coronary occlusion, were analysed in relation to the primary endpoint.
The present investigation was approved by the ethics committee of the Kanton of Bern, Switzerland, and the patients gave informed consent to participate in the study.
Cardiac catheterisation and coronary angiography
Patients underwent left heart catheterisation and coronary angiography for diagnostic purposes from the right femoral artery approach. Biplane left ventriculography was performed followed by coronary angiography. Coronary artery stenoses were determined quantitatively as per cent diameter reduction using the guiding catheter for calibration. Aortic pressure was obtained via a 6F coronary artery guiding catheter. Central venous pressure (CVP) was measured via the femoral vein.
Coronary collateral assessment
Coronary pressure-derived CFI (no unit; figure 1): In all patients, recruitable coronary collateral flow during a 1-min (in rare cases 2-min) vascular balloon occlusion relative to normal antegrade flow through the non-occluded coronary artery was determined using coronary pressure measurements. A 0.014-inch fiberoptic pressure monitoring wire (RadiWire, Radi, Upsala, Sweden) was set at zero, calibrated, advanced through the guiding catheter and positioned distal to the site of CFI assessment. CFI was determined by simultaneous measurements of mean aortic pressure (Pao, mm Hg, via the angioplasty guiding catheter), distal coronary occlusive pressure (Poccl, mm Hg) and (CVP=right atrial pressure): CFI=(Poccl − CVP)/(Pao − CVP) (figure 1; CFI calculation at the end of the 1st 1-min balloon occlusion). Sensor-derived CFI measurements have been previously validated21–23 and are regarded as the gold-standard for collateral assessment in humans.6

Collateral flow index (CFI) is calculated at the end of the coronary balloon occlusion by dividing mean distal coronary occlusive pressure (Poccl, mm Hg; scale 0–200 mm Hg) minus central venous pressure (CVP, mm Hg; scale 0–50 mm Hg) by mean aortic pressure (Pao, mm Hg; scale 0–200 mm Hg) minus CVP. CFI=0.049 is insufficient to prevent myocardial ischaemia during a 1-min coronary balloon occlusion as indicated by ST-segment elevations on the intracoronary (i.c.) ECG.
As the first dichotomic method for collateral assessment, a unipolar intracoronary ECG was obtained during coronary occlusion in all patients from the angioplasty guidewire (figure 1). For that purpose, an alligator clamp was attached close to the end of the wire and connected to ECG lead V1.24 Thus, coronary collaterals with or without intracoronary ECG signs of ischaemia (ie, ST-segment shift of >0.1 mV) at the end of the 1-min coronary occlusion were determined. As the second dichotomic method for collateral assessment, the patient was asked immediately after the end of the coronary occlusion whether he or she had experienced chest pain or had been free of angina pectoris.
Study protocol
Following diagnostic coronary angiography, an interval of at least 10 min was allowed for dissipation of the effect of the contrast medium on coronary vasomotion. Before CFI measurement, 5000 units of heparin were given. Two puffs of oral nitroglycerine spray were applied shortly before coronary pressure measurements. The pressure guidewire was positioned distal to the site of the imminent angioplasty balloon occlusion. During the entire protocol, the intracoronary ECG obtained from the pressure guidewire was recorded. Simultaneous recording of Pao, Poccl, CVP and the ECG was started before and continued throughout the coronary balloon occlusion (figure 1). Occlusion was performed using an appropriately sized angioplasty balloon. If indicated, PCI for treatment of a stenotic lesion was performed following CFI measurement. If the CFI measurement was performed in a normal coronary artery, an adequately sized balloon was inflated at a low pressure around 1 atm just sufficient to occlude the vessel. The safety of such an occlusion in a normal vessel segment has been documented previously.25
Statistical analysis
The study population was divided into a group with poorly developed collateral vessels (CFI<0.25) and one with well-grown collateral vessels (CFI≥0.25). Between-group comparisons of continuous demographic, clinical, angiographic, hemodynamic and collateral flow data were performed by a two-sided unpaired Student's t test. A χ2 test (2×2 table) was used for comparison of categorical variables among the study groups. The calculation of cumulative survival and event rates was performed using Kaplan–Meier analysis, whereby statistical comparison between the groups was done by a log rank test (Mantel-Cox). Cox proportional hazards analysis was carried out to determine independent predictors for all-cause mortality. The following variables selected on the basis of a univariate Kaplan–Meier analysis (p<0.10) were entered in the Cox proportional hazard analysis: age, female gender, number of vessels with CAD, percent diameter narrowing of the stenosis undergoing PCI and CFI measurement, CFI, left ventricular (LV) end-diastolic pressure, systolic blood pressure during the invasive examination (but not during CFI measurement) and the tag ‘arteriogenic therapy at follow-up’.
Results
Patient characteristics and clinical data
There were no statistically significant differences between the two groups regarding age, gender, duration of chest pain prior to CFI measurement, prior remote myocardial infarction, body mass index and frequency of most of the cardiovascular risk factors as well as the use of the majority of cardiovascular drugs (table 1). Systemic arterial hypertension was more prevalent in the group with low CFI than high CFI.
Patient characteristics and clinical data
Coronary angiographic data
The coronary arteries undergoing CFI measurement and the number of vessels with CAD were similarly distributed among the groups (table 2). CFI measurements with proximal vessel occlusion were performed more often in the low CFI group than in the high CFI group. Percent diameter stenosis at the site of CFI measurement was lower and fractional flow reserve of this vessel was higher in the group with low CFI than with high CFI (table 2).
Coronary angiographic data
Hemodynamic and collateral circulation data
Heart rate (70±13 in both groups), diastolic arterial blood pressure (71±12 mm Hg in both groups), LV ejection fraction (62±11% in both groups) and CVP (6±3 mm Hg in both groups) were similar between the groups. Systolic arterial blood pressure was 130±24 mm Hg in the group with low CFI and 128±23 mm Hg in the group with high CFI (p=0.31). LV end-diastolic pressure was 12±7 mm Hg in the group with low CFI and 13±6 mm Hg in the group with high CFI (p=0.0282). ECG ST-segment shift >0.1 mV on intracoronary ECG and angina pectoris during coronary occlusion was observed more often in the group with low CFI than with high CFI (figure 2). By group definition, CFI was lower in the group with CFI<0.25 than in the group with CFI≥0.25: 0.129±0.067 vs 0.366±0.127 (p<0.0001).
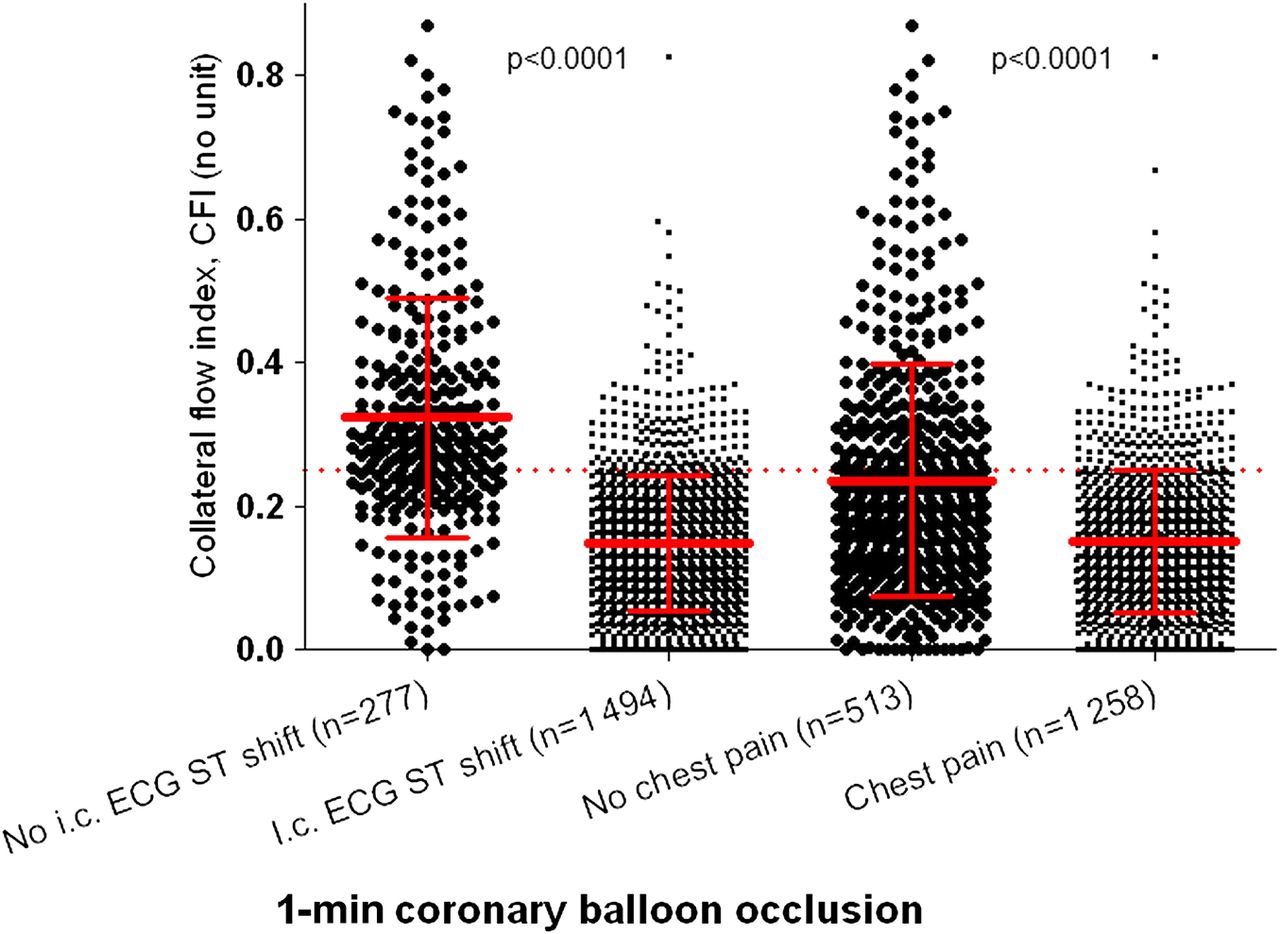
Plot of all the collateral flow index (CFI) measurements (vertical axis) without and with simultaneously obtained intracoronary (i.c.) ECG ST-segment shift >0.1 mV, and without and with chest pain during the coronary balloon occlusion. The red broken line indicates a CFI value of 0.25. Error bars: mean plus minus SD.
CFI in patients under arteriorgenic treatment: CFI in patients undergoing arteriogenic treatment increased from 0.151±0.120 at baseline to 0.191±0.125 at follow-up (p=0.0002).
CFI measurement variability: Three hundred serial CFI measurements in the absence of altering hemodynamic conditions between the measurements (ie, no change of stenosis severity), and with placebo treatment during follow-up, were performed in 76 patients (follow-up duration: 2 weeks and 3 months). CFI was 0.157±0.096 at baseline and it was 0.150±0.093 at follow-up (p=0.25).
Clinical outcomes
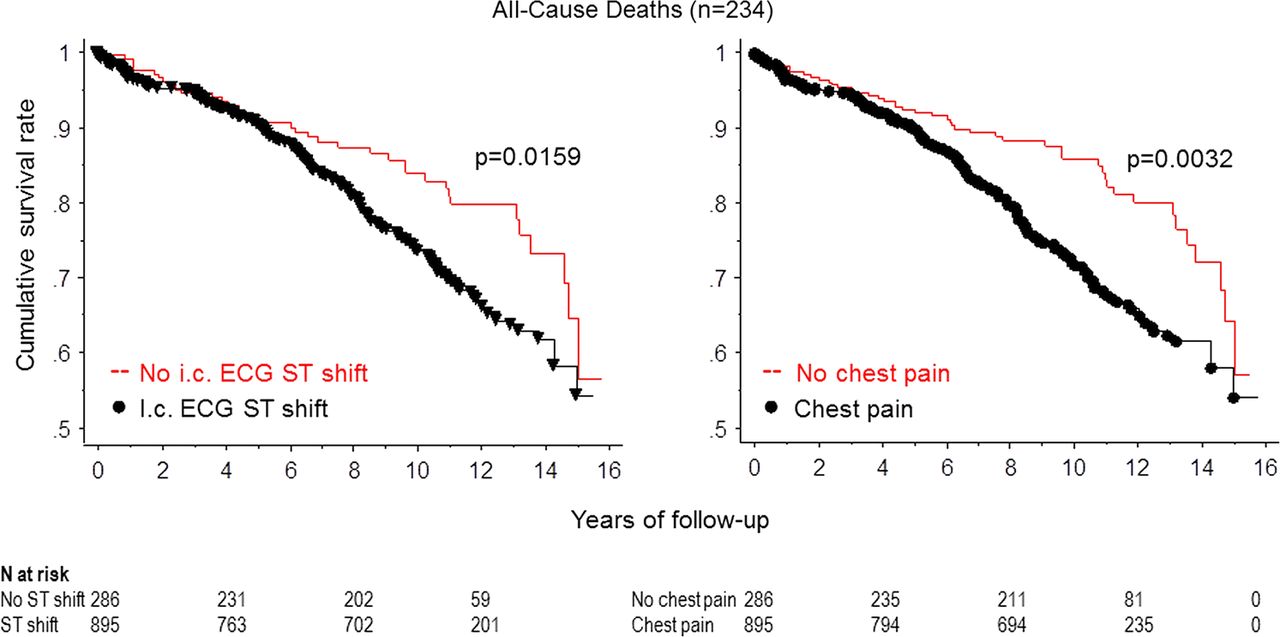
Follow-up duration ranged from 2 weeks to 15.8 years (average: 7.3±4.3 years). Follow-up duration was significantly shorter in patients with low CFI than in those with high CFI (table 3). Median follow-up duration (inter-quartile range) was 6.8 years (7.0) in the group with CFI<0.25 and 9.1 years (6.6) in the group with CFI≥0.25. Follow-up was complete in 1142 patients (97%). The raw event rate of deaths due to all causes irrespective of follow-up duration (n=234) was similar between the groups, and the number of cardiovascular deaths (n=90) tended to be higher in the group with low CFI versus high CFI (table 3). The raw event rate of other MACEs did not differ between the groups. The cumulative event-free rate of all-cause death was lower in patients with low CFI versus high CFI (figure 3). The cumulative event-free rates of cardiac death and MACE, respectively, were significantly lower in the group with low CFI versus high CFI (figure 4). The cumulative event rate free of all-cause death was lower in patients with intracoronary ECG ST shift >0.1 mV than in those without, and it was also lower in those with angina pectoris during coronary occlusion than in those without (figure 5). Patients having completed a course of arteriogenic therapy (tagged ‘arteriogenic therapy at follow-up’) revealed a higher cumulative survival rate than those without arteriogenic therapy (figure 6). Proportional hazard analysis showed the following independent predictors of all-cause mortality (table 4): age, number of vessels with CAD, CFI and LV end-diastolic pressure.
All-cause and cardiovascular events during follow-up
Proportional hazard analysis for all cause mortality
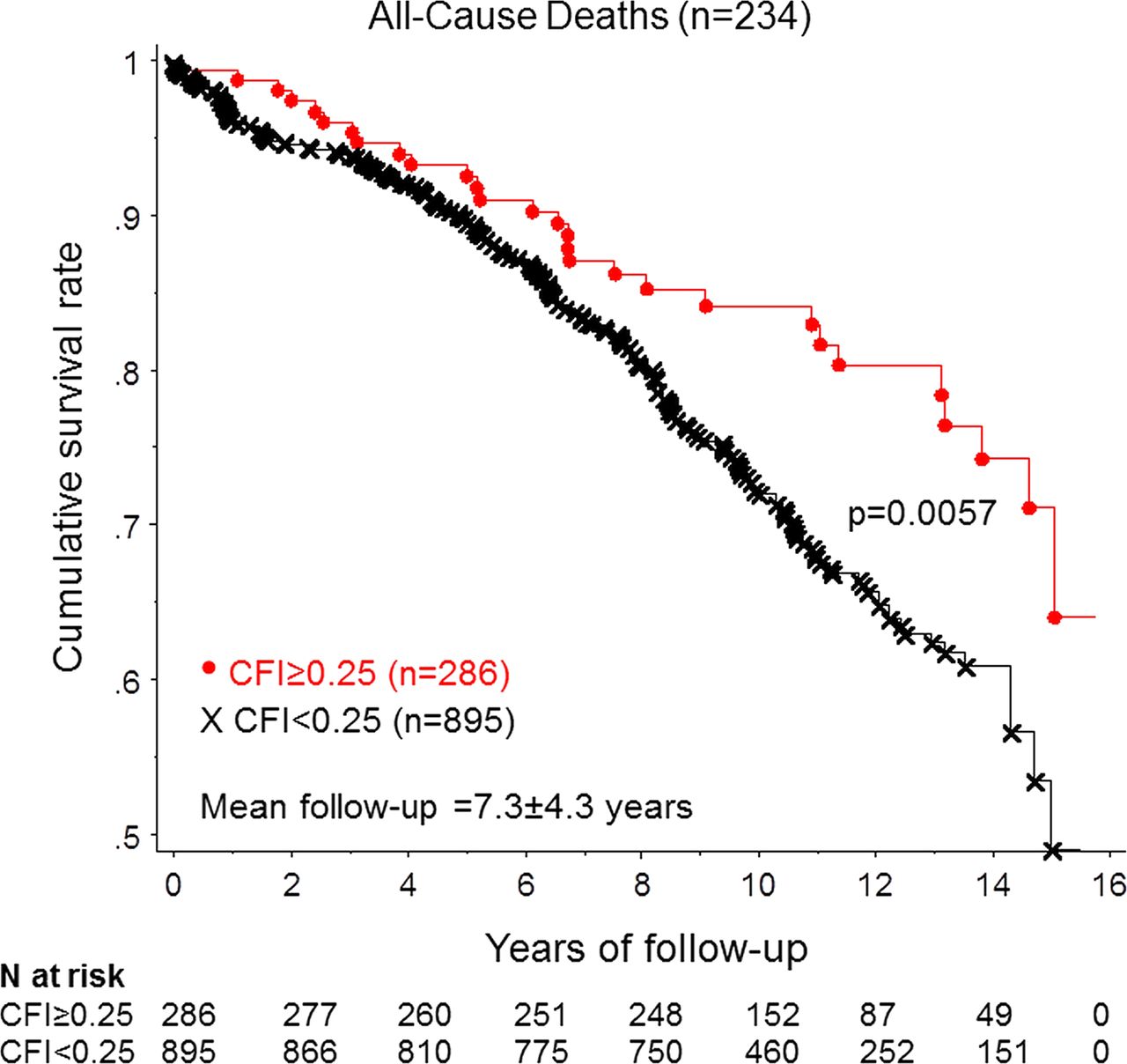
Cumulative survival rates related to all-cause mortality in patients with low and with high collateral flow index (CFI).

Cumulative survival rates related to cardiac mortality (left panel) and to major adverse cardiac events (right panel) in patients with low and with high collateral flow index (CFI).

Cumulative survival rates related to all-cause mortality in patients without and in those with intracoronary ECG ST-segment shift >0.1 mV during a 1-min coronary balloon occlusion (left panel). Cumulative survival rates related to all-cause mortality in patients without and in those with chest pain during the same 1-min coronary balloon occlusion (right panel).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Cumulative survival rates related to all-cause mortality in patients with arteriogenic therapy at follow-up (Arteriogen_Tx_at_fu) versus those without arteriogenic therapy (No arteriogen_Tx).
Discussion
The present 8500 patient-year study found the coronary collateral circulation related to diminished all-cause mortality as well as to reduced MACE, and this was independent of the method used for collateral assessment. Therapeutic promotion of the collateral circulation conveyed lowered all-cause mortality. It is likely that an improved coronary collateral function, as gained during stable CAD, conveys its survival benefit through myocardial salvage in case of sudden coronary occlusion.
The coronary collateral circulation and adverse events
In the clinical context of chronic CAD, the association between the angiographic presence of collaterals connecting different coronary territories and medium-term outcome has been investigated as early as 1971.26 The risk of dying from any cause during a follow-up of almost 2 years in that study by Helfant et al was reduced to almost half in the presence versus the absence of angiographic collaterals. However, the 95% CI of the relative risk (0.22 to 1.47) found in that study rendered the survival benefit of patients with good collateral supply uncertain, and exemplified the triple limitation of many subsequent studies on the same topic: low number of recruited patients with a brief observation time and use of a blunt method for collateral assessment (coronary angiography). The range of patients included in 13 studies on the prognostic effect of the coronary collateral circulation is equal to 22–2173 (mean 866), the range of follow-up duration is between 30 days (or in-hospital) and 16 years (the present study; mean 19 months), and all except for two studies from our laboratory have employed angiographic grading of spontaneously visible collaterals as the method for assessment.7 The investigation of Antoniucci et al and of Steg and co-workers illustrate that the use of a vague method for collateral assessment can be compensated for by including more patients in a setting in which mortality is genuinely higher than in the population with chronic stable CAD: acute, respectively subacute myocardial infarction.8 ,27 The relative risk for mortality from any cause in these studies among patients with spontaneously visible collateral arteries has been reduced to 0.47 (95% CI 0.25 to 0.87) in the former investigation and to 0.72 (95% CI 0.49 to 1.06) in the latter investigation.8 ,27 Similarly, employing two dichotomic methods for collateral assessment independent of quantitative CFI measurement, the present study found that absence of intracoronary ECG ST segment shift >0.1 mV and of angina pectoris during the 1-min coronary occlusion was related to lowered all-cause mortality. This finding augments the reliability of this study's main result that a growing collateral function, as quantitatively assessed by CFI, is an independent beneficial prognostic determinant. In turn, this is consistent with the principal finding of a recent meta-analysis documenting a relative risk reduction for all-cause mortality of 0.64 (95% CI 0.45 to 0.91) among patients with a well-developed coronary collateral circulation.7
Aside from the mentioned quality features of a high internal and external validity of our main study finding, there is also an indicator for a good quality multivariate analysis, leading to the result of CFI as a statistically independent beneficial prognosticator: the findings aside from the just mentioned were biologically plausible. The strongest predictor for mortality was the age of the patient at study inclusion. The second strongest determinant of mortality was LV end-diastolic pressure as obtained during the diagnostic part of the invasive exam prior to the study measurements, which sensitively reflects LV function as a whole. Importantly, LV end-diastolic pressure was directly related to mortality, whereas CFI was related inversely to mortality. This is a strong argument in favour of the quality of CFI measurements, which in the numerator of the equation, carry the coronary occlusive pressure (Poccl). Poccl measurements in this study did not reflect LV end-diastolic pressure, which could be theoretically conceivable considering the vicinity of both measurement sites, because a high CFI was beneficial and the latter a detrimental prognosticator for survival. The number of vessels with haemodynamically relevant stenoses was related to increased mortality.
Coronary collateral supply as a beneficial prognosticator: confounded or causal relation?
In the context just described, collateral function as obtained by the quantitative parameter of CFI is a reliable, statistically independent prognosticator of survival. However, this does not imply a causal relationship between the two parameters, because it may be confounded by an association between CFI and the ‘real’ causal determinant of prolonged survival, that is, CFI may be just its indicator. For example, and considering the tight relation between collateral function and severity of a stenotic lesion, CFI could be regarded just a marker of stenosis severity, the latter of which would be the causal link to increased mortality. As our data show, a more severe stenotic lesion does not independently predict a higher risk of death from any cause. This finding cannot rule out a causal relation between stenosis severity and prognosis, and the finding of Steg et al8 that angiographically visible collaterals predicted prolonged survival by univariate but not multivariate statistical analysis ought not preclude a causal relation between the two parameters.
A causal relation between augmented CFI and improved survival can only be established on the basis of an experimental study design in patients randomly allocated to a pro-arteriogenic treatment or to placebo. Therefore, the present study performed a specific survival analysis for all the patients tagged ‘arteriogenic therapy at follow-up examination’ in comparison to all the patients without such a treatment. CFI in that group increased from 0.151±0.120 at baseline to 0.191±0.125 at follow-up (p=0.0002). Hence, in association with this therapeutically induced augmentation in coronary collateral function, patients showed a lower mortality rate than patients without such a treatment (see figure 6). That is, the most original finding of the present study was to demonstrate a survival benefit for patients receiving a treatment with one of the following arteriogenic therapies: granulocyte-macrophage colony stimulating factor, granulocyte colony stimulating factor, external counter-pulsation and physical exercise training. In the context of the limited size of the respective trials, each of the arteriogenic therapies have been shown to be effective in regard to the endpoint CFI, but not to the clinical endpoint survival rate or rate of MACE.
Study limitations
An important study limitation aside from those alluded to above is that the subgroup of patients with arteriogenic therapy had received different treatments, thus precluding the conclusion, which one was actually prognostically beneficial. Though the absolute majority of the respective trials were randomised controlled studies, none was designed to analyse efficacy of the treatment in regard to clinical outcome. Also, the number of patients included in the arteriogenesis trials was quite small relative to the entire study population. LV functional parameters beyond LV end-diastolic pressure such as ejection fraction were not shown due to spatial constraints, but they were normal and not statistically different between the groups at baseline or at follow-up exam.
Conclusion
A well-functioning coronary collateral circulation independently predicts lowered mortality in patients with CAD. This relation appears to be causal, because improvement of collateral function by arteriogenic therapy is associated with prolonged survival.
References
Footnotes
RE and LB contributed equally to this study.
-
Contributors CS: concept and design of the study, data acquisition and analysis and writing the manuscript. RE and LB: data acquisition and analysis. MS and TT: data acquisition and analysis and critical review of the manuscript. PM: critical review of the manuscript. HS: data acquisition.
-
Funding Supported by a grant from the Swiss National Science Foundation, grant-#32003B-141030/1.
-
Competing interests None.
-
Ethics approval Kantonale Ethikkommission Bern, Switzerland.
-
Provenance and peer review Not commissioned; externally peer reviewed.