Article Text

Abstract
Background The prognostic value of admission heart rate (HR) on long-term mortality in ST-elevation myocardial infarction (STEMI) remains uncertain in the era of primary percutaneous coronary intervention (PPCI).
Methods Retrospective analysis of prospectively collected data of 2571 consecutive STEMI patients undergoing PPCI at a regional tertiary centre. Only patients in sinus rhythm on admission (n=2310) were included in this study, which aimed to assess the predictive value of admission HR on long-term mortality following PPCI and the influence of β-blockers on post-discharge survival.
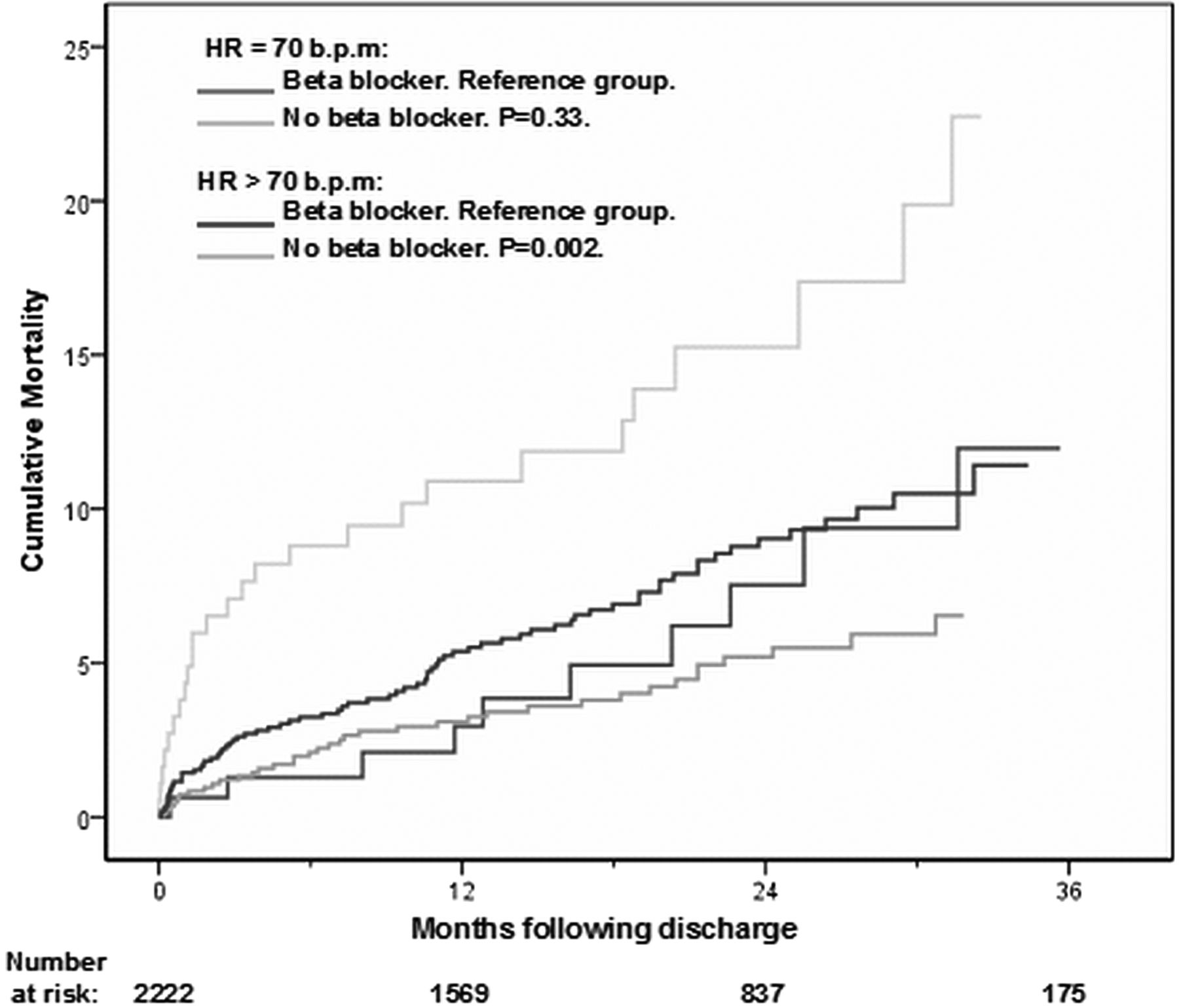
Results Patients were classified according to admission heart rate: either low (≤70 beat per minute (bpm), n=1015) or high HR group (>70 bpm, n=1295). At a median follow-up of 559 days, all-cause mortality was 7.0% in the low HR group compared to 12.7% in the high HR group. In the Cox proportional hazard model corrected for several confounders, the adjusted HR for all-cause mortality in the high HR group was 1.59 (95% CI 1.15 to 2.20; p=0.005). Furthermore, every 10 bpm increase in admission heart rate was associated with 17% increase in all-cause mortality. Pharmacological intervention with β-blockers on discharge was associated with a reduction in post-discharge mortality only in the high HR group (adjusted HR, 0.49; 95% CI 0.31 to 0.77; p=0.002) versus 0.74 (95% CI 0.37 to 1.49; p=0.40) in the low HR group.


{kind=link}
{kind=link}