Article Text

Abstract
Background: Ischaemic preconditioning results in a reduction in ischaemic-reperfusion injury to the heart. This beneficial effect is seen both with direct local preconditioning of the myocardium and with remote preconditioning of easily accessible distant non-vital limb tissue. Ischaemic postconditioning with a comparable sequence of brief periods of local ischaemia, when applied immediately after the ischaemic insult, confers benefits similar to preconditioning.
Objective: To test the hypothesis that limb ischaemia induces remote postconditioning and hence reduces experimental myocardial infarct size in a validated swine model of acute myocardial infarction.
Methods: Acute myocardial infarction was induced in 24 pigs with 90 min balloon inflations of the left anterior descending coronary artery. Remote ischaemic postconditioning was induced in 12 of the pigs by four 5 min cycles of blood pressure cuff inflation applied to the lower limb immediately after the balloon deflation. Infarct size was assessed by measuring 72 h creatinine kinase release, MRI scan and immunohistochemical analysis.
Results: Area under the curve of creatinine kinase release was significantly reduced in the postconditioning group compared with the control group with a 26% reduction in the infarct size (p<0.05). This was confirmed by MRI scanning and immunohistochemical analysis that revealed a 22% (p<0.05) and a 47.52% (p<0.01) relative reduction in the infarct size, respectively.
Conclusion: Remote ischaemic postconditioning is a simple technique to reduce infarct size without the hazards and logistics of multiple coronary artery balloon inflations. This type of conditioning promises clear clinical potential.
- LAD, left anterior descending artery
- LE, late enhancement
- LV, left ventricule
- PTCA, percutaneous transluminal coronary angioplasty
- STEMI, ST elevation myocardial infarction
Statistics from Altmetric.com
- LAD, left anterior descending artery
- LE, late enhancement
- LV, left ventricule
- PTCA, percutaneous transluminal coronary angioplasty
- STEMI, ST elevation myocardial infarction
Although primary angioplasty has reduced the risk of mortality as compared with fibrinolysis in ST elevation myocardial infarction (STEMI; 7% vs 9%), left ventricular (LV) dysfunction still occurs in many patients.1 The degree of LV dysfunction, the strongest determinant of mortality after STEMI,2 has been related to the duration of ischaemia, the number of diseased vessels, the completeness of epicardial coronary artery patency and the restoration of microcirculatory flow, which fails in up to 30% of patients (no reflow).3 However, there is broad consensus that reperfusion in itself also mediates myocardial reperfusion injury.4
Warning hearts of impending ischaemia through the delivery of brief tolerating cycles of local ischaemia or ischaemia in remote non-vital organs can reduce infarct size between 40% and 90% in various species.5 However, the widespread applicability of this preconditioning is limited by the implicit proviso that preconditioning must be instituted before unanticipated ischaemic events.6 More recently, the ability to mitigate reperfusion injury through the application of several brief cycles of infarct-associated coronary artery occlusion after a sustained ischaemic insult has been achieved by postconditioning.7 Although this controlled reperfusion is successful in animal and even in human studies,8 significant methodological hurdles may limit the broad clinical applicability and potential safety of postconditioning.9 The objectives of the present study were to investigate whether episodes of ischaemia applied to non-vital remote tissues, immediately after reperfusion in a validated swine model of STEMI, can safely limit infarct size through remote postconditioning.
METHODS
Experimental animals
All experiments performed in this report conformed to the standards in the Guiding Principles in the Use and Care of Laboratory Animals published by the National Institute of Health (NIH Publication No 85–23, revised in 1996). Twenty four Yorkshire pigs of both sexes, weighing 18–22 kg and free of clinically evident disease, were randomised to remote postconditioning (n = 12) or not (n = 12).
Interventional cardiology procedure
Pigs were anesthetised by ketamine (0.2 ml/kg), intubated orotracheally, and ventilated mechanically with O2 and 1.5% isofluorane. The animals were placed on a homeothermic blanket control unit to maintain a core body temperature of at least 37°C. A 6F sheath was inserted into the right femoral artery, heparin was given as an anticoagulant and the left coronary artery was intubated with a 6F JR3.5 guiding catheter. A standard guide wire was introduced into the left anterior descending artery (LAD). Acute myocardial infarction was induced with percutaneous transluminal coronary angioplasty (PTCA) balloon inflation (2.5×10 mm Maverick balloon at 6 atm) for 90 min in the LAD distal to the second diagonal branch. Complete LAD occlusion was confirmed by contrast injection. Myocardial infarction was confirmed by ST segment elevation on the ECG, total creatine kinase release, gadolinium-enhanced contrast MRI scan and histological examination.
Postconditioning procedure
Immediately after PTCA balloon deflation, reversible lower limb ischaemia was induced with repeated inflation of a blood pressure cuff above the systolic blood pressure of the animals for 5 min followed by lower limb reperfusion by cuff deflation for 5 min. Four cycles of ischaemia-reperfusion were performed.
Enzymatic infarct size
Blood samples were taken at anaesthetic induction, every 4 h after deflating the PTCA balloon during day 1 and every 6 h on days 2 and 3. To avoid stress on the animals, they were kept under constant sedation with midazolam. Area under the curve of total serum creatine kinase release (Creatine Kinase Kit, Beckman Coulter, Fullerton, California, USA) was calculated in each animal and used as a surrogate marker of enzymatic infarct size.
Infarct size by MRI scan
After 72 h, cardiac MRI (1.5-T system, Magnetom Sonata, Siemens Medical Solutions, Malvern, Pennsylvania, USA) was performed using ECG gating under the same general anaesthetic regimen as above. All images were acquired during suspension of the ventilation. After intravenous infusion of gadopentate dimeglumine (Magnevist, Berlex Laboratories, Wayne, New Jersey USA; 0.2 mmol/kg bolus), late enhancement (LE) imaging was performed with a delay time of 15 min. Volumes of the regions revealing LE were calculated using the ARGUS software (Siemens Medical, Erlangen, Germany).
Infarct size by immunohistochemistry
After 72 h of reperfusion, animals were killed by using sodium pentobarbital (160 mg/kg intravenous) and the heart was excised. The LAD, circumflex artery and right coronary artery were catheterised. LAD was reversibly re-occluded in the original position distal to the second diagonal branch. Evans blue (0.4%) was infused into the LAD, circumflex artery and right coronary artery to stain the non-ischaemic myocardium in blue, and thereby outline the area at risk (not blue). The occluded LAD was reopened, a catheter was placed distal to the second diagonal branch and a ligation bend was tightened around the tip of the catheter to occlude the LAD again. 2,3,5-triphenyltetrazolium chloride (0.1%) at 37°C was infused into the occluded part of LAD, which stained the viable myocardium in red to measure the extent of necrosis. The atria and right ventricle were removed and the LV was weighed and then immersed in formaldehyde (10%) solution for 24 h. The left ventricle was cut into slices of about 10 mm. Individual slices were weighed and digitally photographed in colour. The extent of myocardial necrosis and the area at risk was quantified in each slice by using image analysis software (Adobe Photoshop V.7.0).
Calculations and statistical analysis
Data are presented as mean (SEM). Area under the curve for total creatine kinase release was calculated with the following equation:
Area = A1+A2+A3+ … +A14 = (((y0+y1)x1)/2))+(((y1+y2)x2)/2) +(((y2+y3)x3)/2)+ … (((y13+y14)x14)/2)
The area at risk was expressed as a percentage of the LV mass, and the infarct size as a percentage of the area at risk. Significance was assumed if p<0.05 (analysis of variance). All analyses were conducted blinded to the randomisation status (postconditioning or control).
RESULTS
Enzymatic measurement of infarct size
The area under the curve (fig 1) of total serum creatine kinase release during the first 72 h of reperfusion was significantly reduced in the postconditioned group than in the control group; this represents 26% reduction in the infarct size (p<0.01; fig 2). The peak total serum creatine kinase release was also significantly lower in the postconditioned group than in the control group (2659 (113) IU/ml vs 3599 (99) IU/ml; p<0.01). Even at 36 h, a significant difference in total serum creatine kinase release persisted between the postconditioned and the control groups.
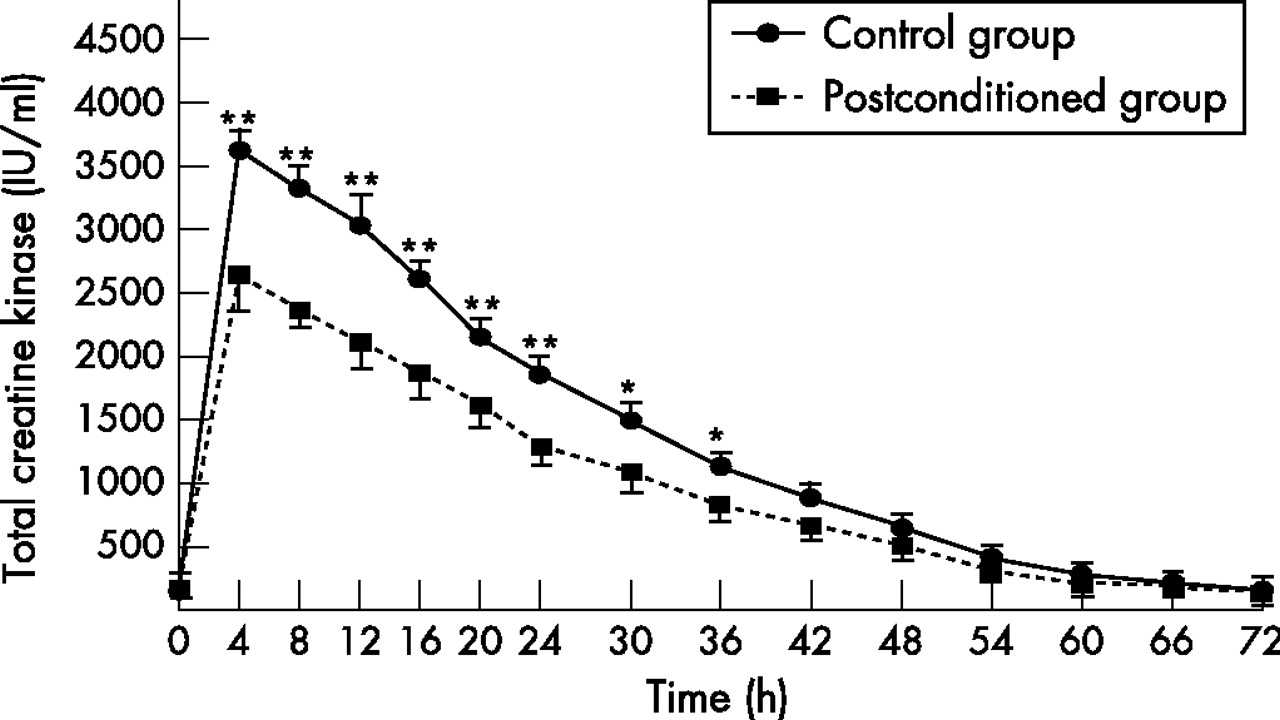
Total serum creatine kinase release. Serum creatine kinase was measured over the first 72 h of reperfusion (IU/ml) in the control (solid line) and the postconditioned (dotted line) animals. Values are expressed in IU/ml as mean (SEM). *p<0.05, **p<0.01.

Enzymatic measurement of the reduction in the infarct size. Area under the curve of total serum creatine kinase release was calculated in each animal and used as a surrogate marker of enzymatic infarct size. Values are expressed in arbitrary units as mean (SEM). There was a significant 26% reduction in the infarct size for postconditioned animals than in control animals (**p<0.01).
Measurement of the infarct size by MRI scan
Infarct size was measured by the volume of gadolinium LE, which was 22% lower in the postconditioned group (29 (9) ml vs 38 (11) ml, p<0.05).
Measurement of the infarct size by histological examination
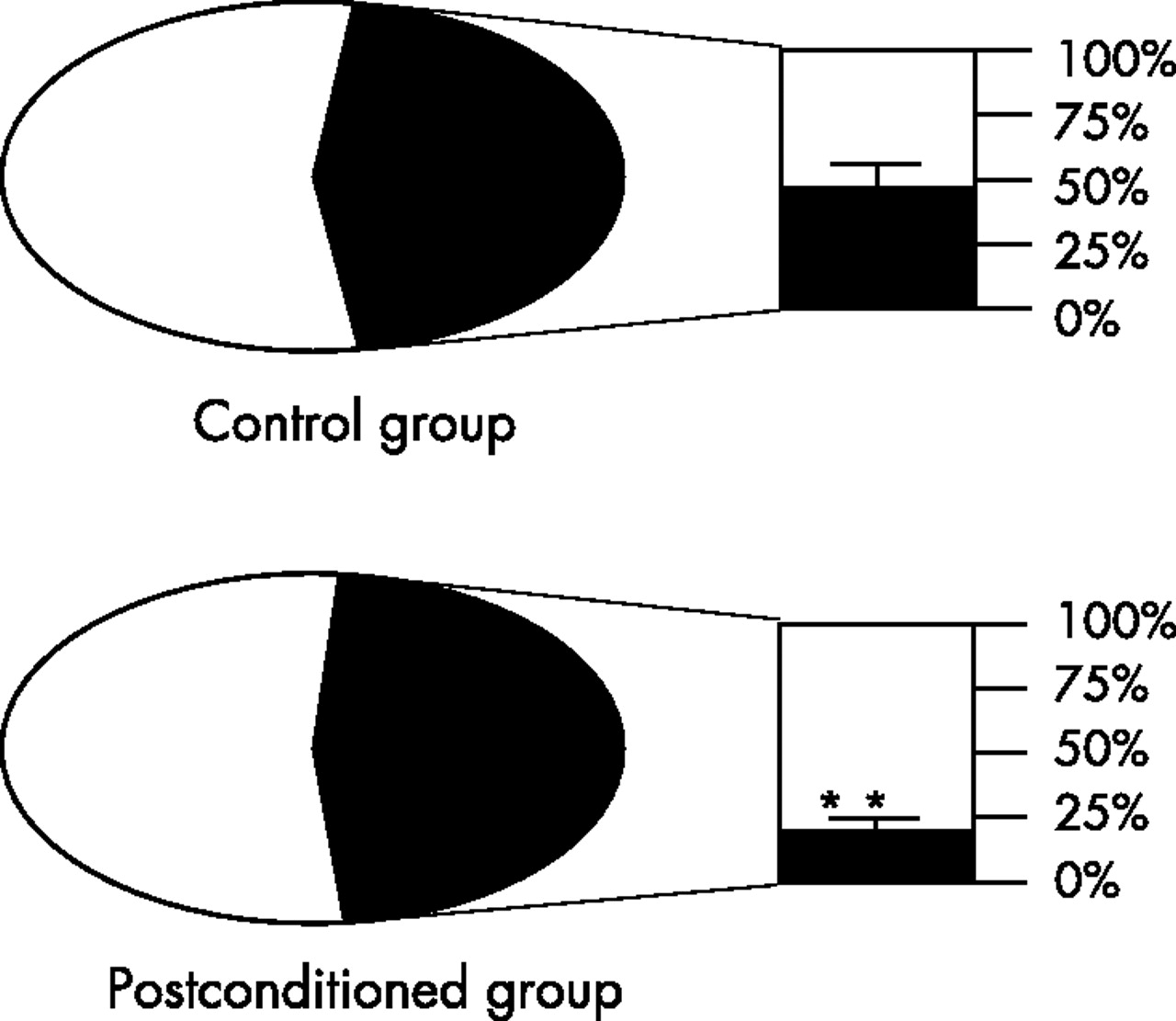
The proportion of area at risk of the LV was similar between the control and the postconditioned groups (41.3% (3.4%) vs 44% (4.1%), non-significant). In the control animals, the infarct size represented 48.4% (5.2%) of the area at risk, whereas in the postconditioned animals, the infarct size represented 23% (2.4%) of the area at risk. This represented a significant decrease in the infarct size (47.5% (5%), p<0.01; fig 3).

{kind=link}
{kind=link}
{kind=link}
Measurement of the infarct size by histological examination. The π graphs show the proportion of area at risk (black)/left ventricle (white) in both the control and the postconditioned animals. The proportion of area at risk did not differ significantly between the control and the postconditioned animals. The bar graphs show the proportion of infarct size (black)/area at risk (white) in both the control and the postconditioned animals. In the control animals, the infarct size represented 48.4% (5.2%) of the area at risk, whereas in the postconditioned animals, the infarct size represented 23% (2.4%) of the area at risk. This represented a significant decrease in infarct size (47.5 (5)%, p<0.01). Values are expressed in percentage as mean (SEM). *p<0.01.
DISCUSSION
The present study confirms the hypothesis that brief cycles of hindlimb ischaemia inducing remote postconditioning applied immediately at the time of reperfusion can reduce the myocardial infarct size by ∼48%. This finding is compelling as all the multiple modalities used to assess infarct size consistently shown statistically and clinically significant reductions in the infarct size, one of the key determinants of STEMI prognosis.10
In some ways, the findings of this and similar studies represent the logical culmination of two decades of research on conditioning.5 Although rapid reperfusion is the best strategy to reduce the complications of myocardial ischaemia, reperfusion itself also confers myocardial dysfunction.4 Reperfusion injury involves several mechanisms driven putatively by an overload of calcium and free-radical, including aberrations in myocardial energetics and metabolism, endothelial dysfunction, inflammation, hypercontracture and necrosis/apoptosis.7 Although preconditioning has been a source of scientific inspiration, its clinical applicability has been limited by the inability to predict acute myocardial events. The subsequent recognition that activation of reperfusion injury-signalling kinases may reduce the extensive damage of reperfusion and salvage the myocardium11 has reinvigorated interest in controlled or mitigated reperfusion—a symptom known in surgical literature for decades.12 Although local postconditioning may ultimately prove to be successful,8 local coronary balloon inflation may be limited by logistical considerations.9 Accordingly, postconditioning has also been recently shown to be effective remotely in rodent models of acute myocardial infarction by potentially invasive renal manipulation13 and by limb manipulation in a lapine model.14 The latter and present studies show that remote postconditioning (rather than conditioning before reperfusion)13,15 by ischaemic hindlimb manipulation is safe and effective.
The magnitude of infarct size as determined by the standard measure of myocardial infarction relative to the area at risk as compared with controls was reduced by ∼48%. This was confirmed by other validated measures of the infarct size (eg, MRI).16 The efficacy of postconditioning in our model is certainly consistent with other studies assessing preconditioning and postconditioning in animals as diverse as rats, rabbits and dogs.17 Although preconditioning has both intuitively and empirically been more effective, a direct comparison with a similar pig model of Kharbanda et al18 suggests that the reduction in the infarct size is potentially comparable (26 (9)% vs 53 (8)%, p<0.05, hence ∼50%).18 Any difference in the absolute infarct size may be explained by methodological differences; Kharbanda et al inflated PTCA balloons in smaller (∼15 kg) Danish Landrace pigs for only 40 min at the first diagonal. We used larger (∼20 kg) Yorkshire pigs for only 90 min but at the second diagonal, hence the infarct subtended a smaller area at risk. Moreover, we studied our animals at 72 h rather than immediately.
The most enduring concepts traditionally associated with the conditioning irrespective of the animal model used (rat, rabbit, canine or human) are the duration and number of cycles of ischaemia (single vs multiple cycles) and the organ of index ischaemia (local vs remote; eg, renal ischaemia) is conditioning in general,19 and postconditioning in particular,7,13 which must be applied within 1 min of the reperfusion event. The present study successfully uses a genuine postconditoning regimen in the human-pertinent closed-chest pig model, rather than a small animal model, that has proven to be somewhat resistant to postconditioning,20,21 and can be inferred that postconditioning is more than just a local hydrodynamic executor, inducing controlled reperfusion.22 Instead, remote postconditioning putatively rapidly activates multiple layers of signalling moieties that potently mitigate the ravages of reperfusion injury.
Although it is likely that the precise mediators and their time course of action will vary (depending on the organ rendered ischaemic and the temporal aspects of the ischaemia) and the mechanisms underlying remote conditioning (preconditioning or postconditioning) remain elusive, it is likely that some similarities exist between the two. It is generally accepted that adenosine release and, hence, activation of the A2A and A3 receptors have a critical role in the reduction in the infarct size.7 As in the case of humoral factors, a neurogenic arc could be one of the triggers easing the release of adenosine in the myocardium in some forms of preconditioning. This reflex can be abolished in some cases by the ganglion blocker, hexamethonium.19 Moreover, blocking the subsequent effect of adenosine by non-selective adenosine receptor blocker 8-ρ-sulphophenyl theophylline abolishes the infarct-sparing effect of postconditioning.13 Other potential triggers include reaction-elaborated reactive oxygen species, endogenous opioids operating through the κ and δ receptors and nitric oxide. Downstream effectors include protein kinase C, reperfusion injury-signalling kinases, KATP channels and the mitochondrial permeability transition pore. It is noteworthy, that unlike humans, pigs do not exhibit an extensive coronary collateral network, hence any putative mediator must be operative through mechanisms other than direct myocardial amelioration, or must be active rapidly after the onset of reperfusion. Clearly, a great deal of mechanistic work remains to be done to elucidate these pathways and how they interact with other conditioning drugs such as inhalational anaesthetics.
Although this observational study is limited by the absence of a definitive mechanistic explanation for genuine remote postconditioning and elucidation of the downstream signalling pathways, the main aim of this study was to establish that remote postconditioning could occur. Indeed, at its inception, postconditioning was considered illogical by some, as the traditional conditioning doctrine required a distinct period of pre-ischaemia and reperfusion for the signalling events to become effective.19 Accordingly, this is the first study in a closed-chest large mammal analogous to humans to confirm the ability for this safe and easy form of remote postconditioning to be applied to fields as diverse as paediatric cardiac transplantation and primary angioplasty. The present study confirms recent observations in two small animal models of remote postconditioning, an adenosine-mediated model described by Vinten-Johansen’s group in rats exposed to a single 5-minute episode of renal ischaemia initiated before reperfusion,13 and a lapine model of postconditioning subject to limb ischaemia.14 This study highlights the capacity of early remote postconditioning to be of benefit to humans and mandates replication, mechanistic and clinical studies to be performed in order to usher in the decade old paradigm of mechanical conditioning to the bedside.
REFERENCES
Footnotes
-
↵* MPF and PA have contributed equally as the principal investigators of this study and are joint senior authors.
-
Published Online First 19 April 2007
-
Funding: This work was supported by grants from the OTKA (Grant F43380 to P A), the ETT (Grant 302/2003 to P A), the Gottsegen Hungarian Institute of Cardiology (to P A) and the Semmelweis University (to P A). PA is the recipient of the Hungarian Academy of Sciences Bolyai Postdoctoral Fellowship. G Sz is the recipient of the Research Fellowship of the European Society of Cardiology.
-
Competing interests: None.