Article Text

Abstract
Objective To explore whether trimetazidine could improve symptoms, cardiac functions and clinical outcomes in patients with heart failure (HF).
Methods A systematic literature search was conducted to identify randomised controlled trials (RCT) of trimetazidine for HF between 1966 and May 2010 in Pubmed, the Cochrane Central Registry of Clinical Trials and EMBASE. Reports of trials were sought that compared trimetazidine with placebo control for chronic HF in adults, with outcomes including all-cause mortality, hospitalisation, cardiovascular events, changes in cardiac function parameters and exercise capacity.
Results 17 trials with data for 955 patients were identified by the literature search. Trimetazidine therapy was associated with a significant improvement in left ventricular ejection fraction in patients with both ischaemic (weighted mean difference (WMD) with placebo 7.37%; 95% CI 6.05 to 8.70; p<0.01) and non-ischaemic HF (WMD 8.72%; 95% CI 5.51 to 11.92; p<0.01). With trimetazidine therapy, left ventricular end-systolic volume was significantly reduced (WMD 10.37 ml; 95% CI 15.46 to 5.29; p<0.01) and New York Heart Association classification was improved (WMD 0.41; 95% CI 0.51 to 0.31; p<0.01) as was exercise duration (WMD, 30.26 s; 95% CI 8.77 to 51.75; p<0.01). More importantly, trimetazidine had a significant protective effect for all-cause mortality (RR 0.29; 95% CI 0.17 to 0.49; p<0.00001) and cardiovascular events and hospitalisation (RR 0.42; 95% CI 0.30 to 0.58; p<0.00001).
Conclusion Trimetazidine might be an effective strategy for treating HF. More studies, especially larger multicentre RCT, are warranted to clarify the effect of trimetazidine on HF.
Statistics from Altmetric.com
With more than 5 million prevalent cases and nearly 1 million hospital discharges yearly, heart failure (HF) represents a rapidly growing therapeutic challenge for healthcare providers.1 Continual knowledge of the pathophysiological background of HF is fundamental in the management of this complex disease. The past 20 years have seen considerable progress in the treatment of HF, with ACE inhibitors, aldosterone antagonists, β-receptor blockers and resynchronisation therapy.2 However, HF remains a leading cause of morbidity and mortality throughout the world.3
Myocardial energy metabolism may be normal in the early stages of HF, but as failure progresses, mitochondrial oxidative metabolism is reduced, and glycolysis is increased with the downregulation of glucose and fatty acid oxidation.4 In particular, evidence suggests that with HF, a shift of metabolism away from a preference for fatty acid towards more carbohydrate oxidation can improve contractile function, thus slowing the progression of HF and improving prognosis in patients with HF.5
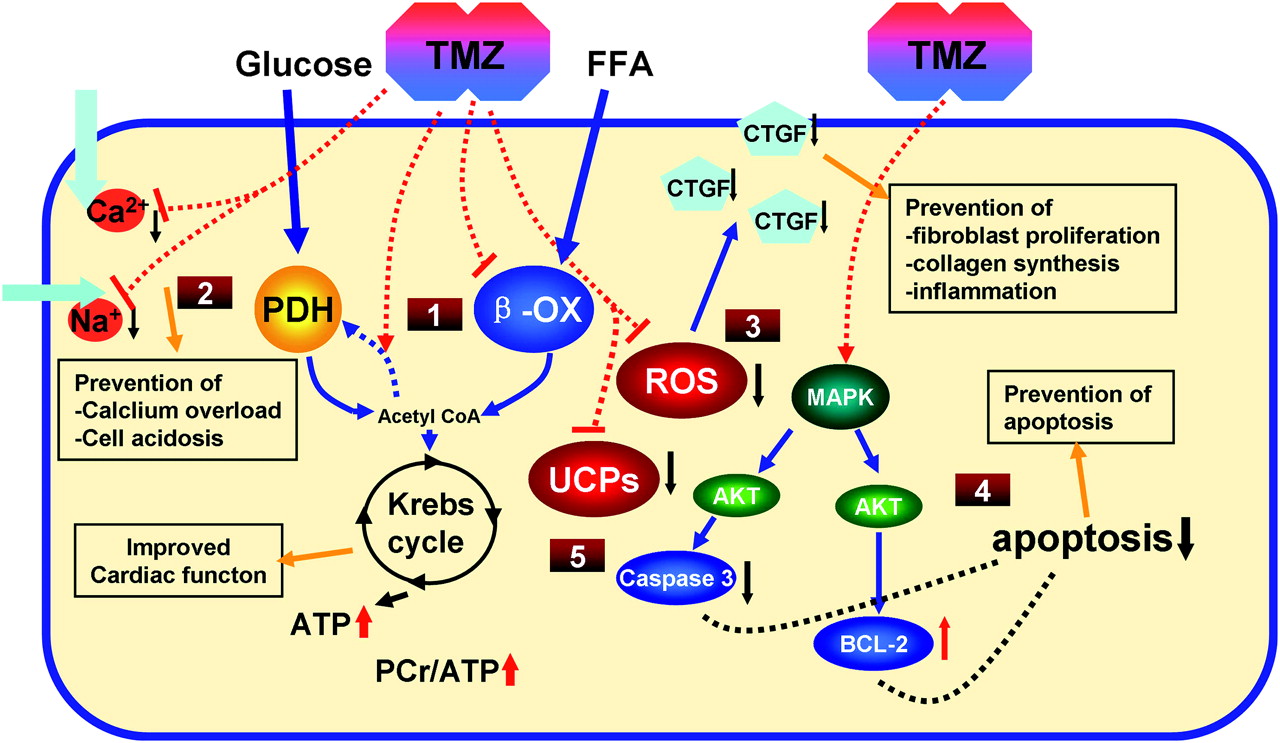
Trimetazidine, a piperazine derivative used as an anti-anginal agent, selectively inhibits long-chain 3-ketoacyl coenzyme A thiolase (the last enzyme involved in β-oxidation) activity. Trimetazidine has been reported to have a potential benefit in HF.6 Trimetazidine may affect myocardial substrate use by inhibiting oxidative phosphorylation and shifting energy production from free fatty acids (FFA) to glucose oxidation.7 It may also contribute to the preservation of intracellular levels of phosphocreatine and ATP,8 reduce calcium overload and free radical-induced injury,9 inhibit cell apoptosis10–12 and improve endothelial function.13 More recently, trimetazidine has been suggested to inhibit cardiac fibrosis through an NADPH oxidase-reactive oxygen species–connective tissue growth factor pathway14 (see figure 1).

Possible mechanisms of the benefit effects of trimetazidine (TMZ) in heart failure (HF): from metabolism to myocardial protection. Administration of trimetazidine induces the partial inhibition of fatty acid β-oxidation (β-ox) and increases pyruvate dehydrogenase (PDH) (1) and determines the increase in glucose oxidation, energetically useful in HF. (2) Limitation of accumulation of sodium and calcium and intracellular acidosis. (3) Reduces reactive oxygen species (ROS)-induced cell damage, and inhibits cardiac fibrosis and inflammation through the ROS/CTGF pathway. (4) Prevention of cell apoptosis through the mitogen-activated protein kinase (MAPK)/AKT pathway. (5) Reduces uncoupling proteins (UCP) and increases PCr/ATP ratio. The final effect is a reduction in cellular damage and an improvement in HF. FFA, free fatty acid. PCr, creatine phosphate; CTGF, connective tissue growth factor.
Over the past few decades, several small randomised controlled trials (RCT) have been conducted using trimetazidine in the HF population. These trials investigated symptoms, cardiac function parameters, various quality of life aspects and adverse events, comparing trimetazidine with placebo. Some studies have shown a benefit with trimetazidine in HF. However, the studies showed limited benefits, and the small sample sizes produced underpowered results, and until now metabolic therapy was not recommended by guidelines.1 We therefore performed a meta-analysis to explore the potential therapeutic effects of trimetazidine in the management of chronic HF.
Methods
Literature search
Two authors (DG and NN) independently conducted a search for reports of RCT in Medline via PubMED (studies published from 1966 to June 2010), EMBASE (studies published from 1980 to June 2010) and the Cochrane Central Register of Controlled Trials (using the OVID interface for studies published before the second quarter of 2010). The search terms were ‘Trimetazidin*’, ‘VASTAREL*’ or ‘IDAPTAN*’ plus ‘heart failure’, ‘cardiac failure’ or ‘cardiomyopathy’. Sensitive filters identified clinical research or RCT in the Medline database15 and the EMBASE database.16 The search was limited to human subjects, with no restriction for language. Conference proceedings from the American College of Cardiology (2005–10), American Heart Association (2005–10), and European Society of Cardiology Congress (2005–10) were also searched. The search was finalised on 18 June 2010. The Clinical Trials database (http://clinicaltrials.gov/) was searched with the search term ‘Trimetazidin*’ for articles in other archived registries. We also contacted the manufacturers of trimetazidine (no additional studies were identified) and reviewed the bibliographies of reports of RCT and review articles for possible missed reports of RCT.17
Inclusion criteria
Two authors (DG and NN) reviewed all retrieved abstracts to identify potential reports of RCT. The full texts of potential articles were retrieved and reviewed by the same authors to determine eligible articles. Disagreements were resolved by consensus, and if necessary a third author (XN) was consulted. Reports of RCT of trimetazidine compared with placebo control for chronic HF in adults and reporting at least one of the outcomes of interest were considered eligible. These outcomes included mortality, hospitalisation, cardiovascular events, changes in cardiac function parameters (ie, left ventricular ejection fraction (LVEF), left ventricular end-diastolic volume (LVEDV), left ventricular end-systolic volume (LVESV)), New York Heart Association (NYHA) classification and exercise capacity (ie, exercise duration).
Validity assessment and data abstraction
All included articles were assessed for validity by two authors (DG and NN) independently, with disputes resolved by discussion. The quality of the included RCT was also assessed by the Jadad scale.18 If a study did not clearly mention one of these key points, we considered that the point was not covered in the study, and the results may have underestimated the reported characteristics.
Data were abstracted by the use of specific data collection forms by the two authors (DG and NN) and checked for accuracy (by XN). Data were collected on study characteristics (publication data, first author's last name, year of publication, sample size, intervention, comparator therapy, follow-up interval,inclusion criteria and endpoints) and patient characteristics (number of patients, age, gender, cause of the HF, LVEF at baseline, NYHA classification at baseline, other concurrent therapies and the presence of diabetes). When the report did not contain sufficient details to evaluate the validity of the study or outcome data were missing, we attempted to contact the authors by email and in writing. The study complied with the recently reported Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISRMA) statement.19
Statistical analysis
We referred to the guidelines of the Cochrane handbook for systematic reviews of interventions20 for this meta-analysis. For reports of crossover studies in which the authors did not report the data as mean differences between treatment and control but separately as data for two groups, data were analysed as two separate parallel trials, labelled (a) and (b). For dichotomous outcomes, results were expressed as RR with 95% CI. For continuous outcomes, pooled data were described with the weighted mean difference (WMD) and 95% CI. The heterogeneity of results across trials was assessed with a standard χ2 test with significance set at p<0.10 and an I2 statistic with significance set at I2 greater than 50%. A random effects model was used for statistical analysis due to wide clinical and methodological variability across the trials. Publication bias was evaluated by the funnel plot. All analyses involved use of review manager version 5.0 (Revman; The Cochrane Collaboration, Oxford, UK). A value of p<0.01 was considered statistically significant. To evaluate the effect of methodological characteristics of studies on the results of this meta-analysis, the impact of the components of such characteristics on our meta-analysis was assessed by sensitivity analysis.
Results
Study characteristics
The search revealed 159 reports of RCT of trimetazidine for HF; 38 full-text articles and six abstracts were retrieved for in-depth review. The reports for 17 studies,21–37 enrolling 955 participants fulfilled all eligibility criteria, were analysed. Figure 2 shows the flow of studies through the selection process. The validity assessments are shown in table 1. The trial and patient characteristics are shown in tables 2 and 3, respectively. Reports of 16 trials21 23–37 described an evaluation of LVEF (n=866), 1021 23–25 27 28 30 33 34 37 LVESV and LVEDV (n=491), six23 27 28 33 35 37 exercise capacity (exercise duration) (n=381), seven21 22 26 27 29 30 37 NYHA classification (n=426), four26 27 29 35 all-cause mortality (n=376) and four24 26 27 30 cardiovascular events and hospitalisation (n=189) during the study periods. Trimetazidine dosage ranged from 60 to 70 mg/day and treatment periods from 4 weeks to 24 months.
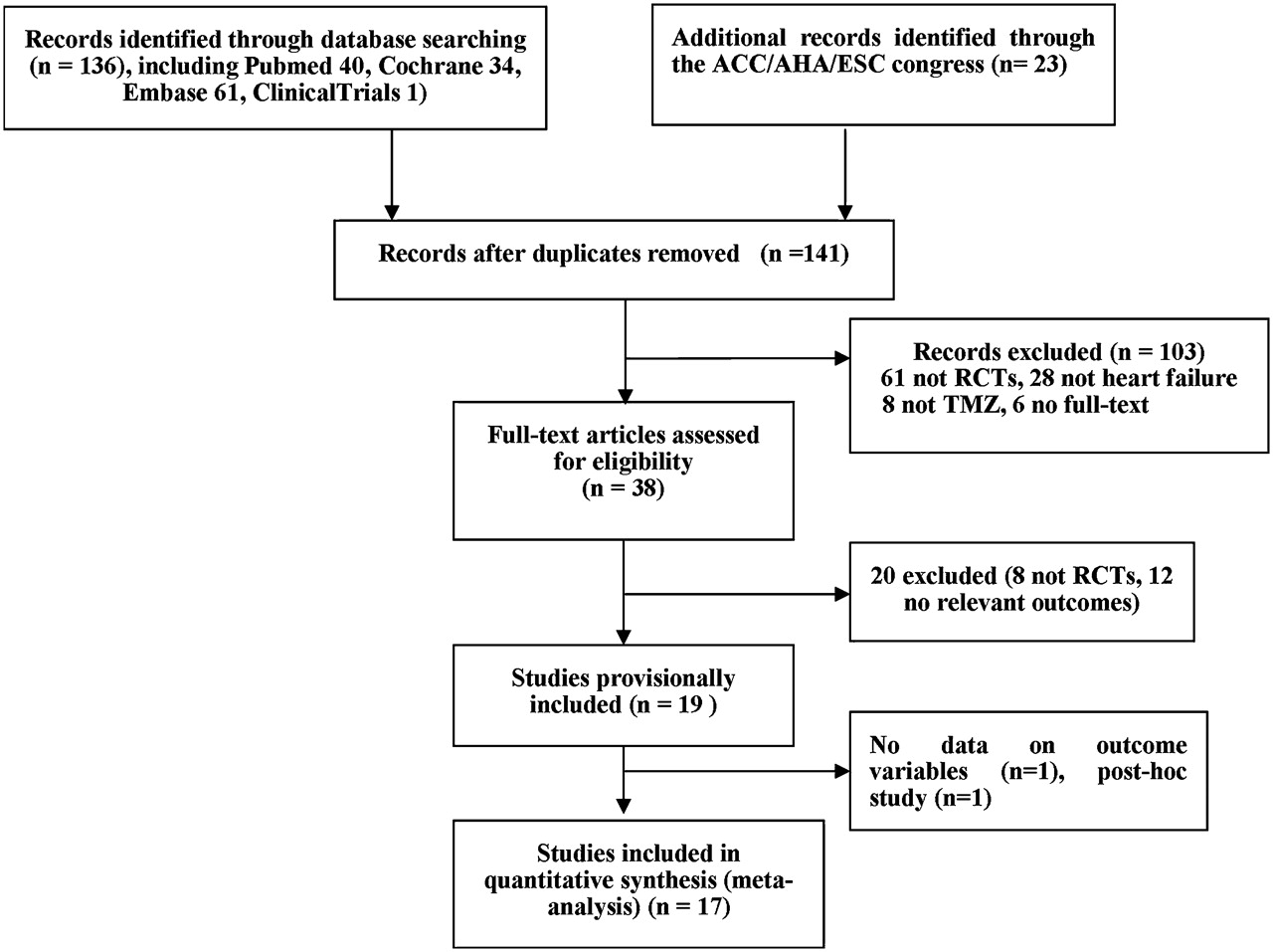
Flow diagram of the trial selection process. ACC, American College of Cardiology; AHA, American Heart Association; ESC, European Society of Cardiology; RCT, randomised controlled trial; TMZ, trimetazidine.
Quality features of 17 reports of RCT assessed in the meta-analysis
Study characteristics
Patient characteristics
Cardiac function
Left ventricular ejection fraction
Among the 16 reports providing data on LVEF, LVEF was significantly higher for patients who received trimetazidine therapy (WMD 7.49%; 95% CI 6.26 to 8.71; p<0.01). Subgroup analysis revealed trimetazidine associated with a significant improvement in LVEF for patients with both ischaemic (WMD 7.37%; 95% CI 6.05 to 8.70; p<0.01) and non-ischaemic HF (WMD 8.72%; 95% CI 5.51 to 11.92; p<0.01) (figure 3A). For the subgroup of patients with diabetes with ischaemic HF, LVEF was similarly elevated in response to trimetazidine treatment (WMD 6.19%; 95% CI 4.16 to 8.23; p<0.01) (figure 3B). The results of the subgroup and sensitivity analyses are displayed in table 4. As shown in table 4, the LVEF response to trimetazidine was still pronounced in studies of which standard therapies for HF (concomitant use of ACE inhibitors/angiotensin receptor blockers (ARB) and β-blockers) were used (WMD 7.14%; 95% CI 5.99 to 8.30; p<0.01). In trials that included patients of NYHA classification IV, a more profound improvement in LVEF was found (WMD 10.87%; 95% CI 9.39 to 12,35; p<0.01). The effect of the follow-up interval on the result was also analysed. After excluding the trials that lasted less than 3 months, a profound improvement in LVEF was observed (WMD 8.12%; 95% CI 6.68 to 9.55; p<0.01). In addition, we renewed the analysis according to methodological quality (excluding scores less than three). There was still a significant improvement in LVEF with trimetazidine compared with placebo control (WMD 7.52%; 95% CI 6.22 to 8.82; p<0.01). A funnel plot of all studies evaluating LVEF appeared symmetrical, thus indicating the low likelihood of publication bias (figure 4).
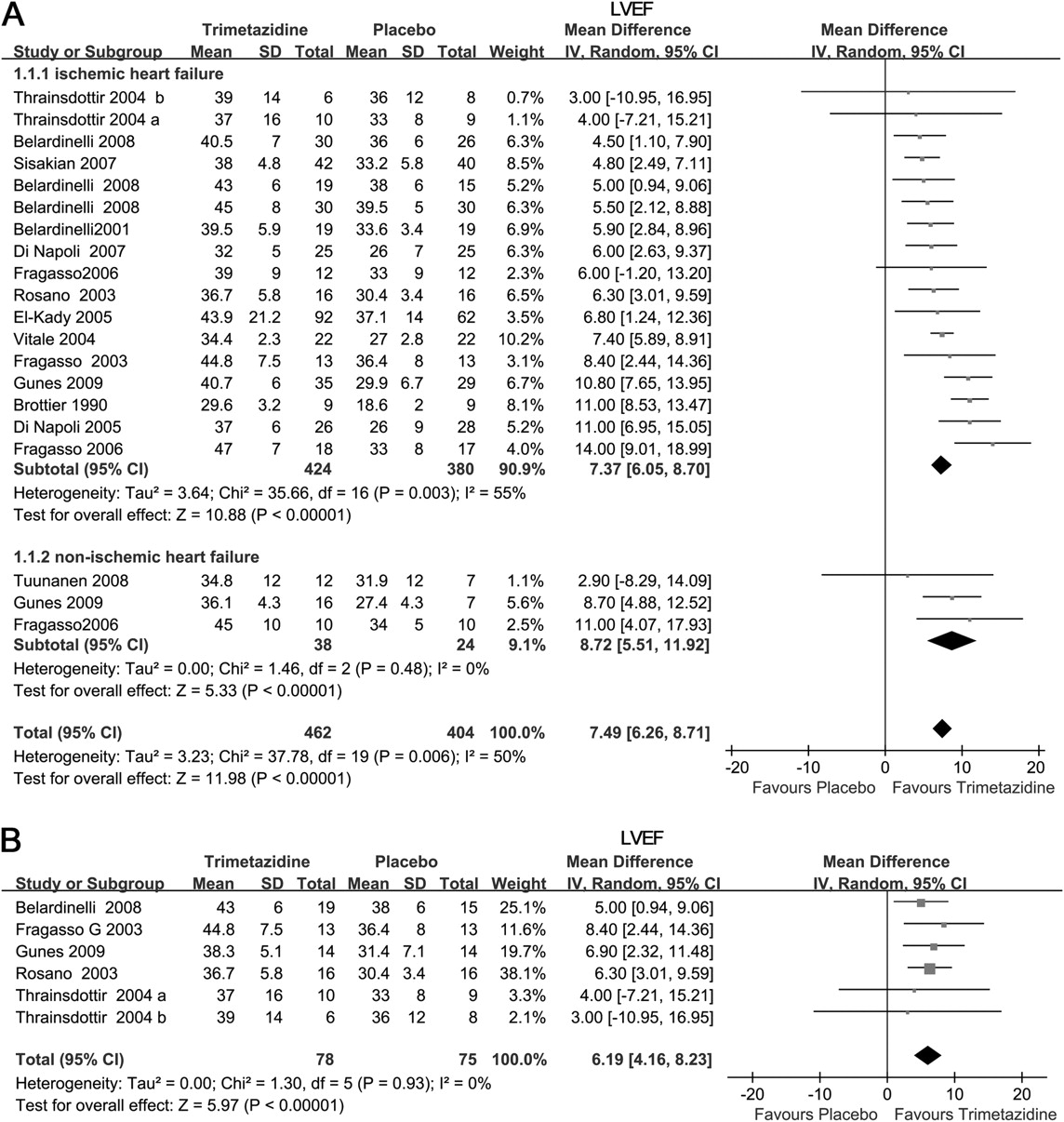
Forest plot from meta-analysis of weighted mean differences in left ventricular ejection fraction (LVEF) for patients with heart failure (HF) receiving trimetazidine (TMZ) or placebo. Subgroup analysis of the effect in patients with ischaemic HF, non-ischaemic HF (A) and patients with diabetes with HF (B). IV, inverse variance.
Sensitivity and subgroup analyses
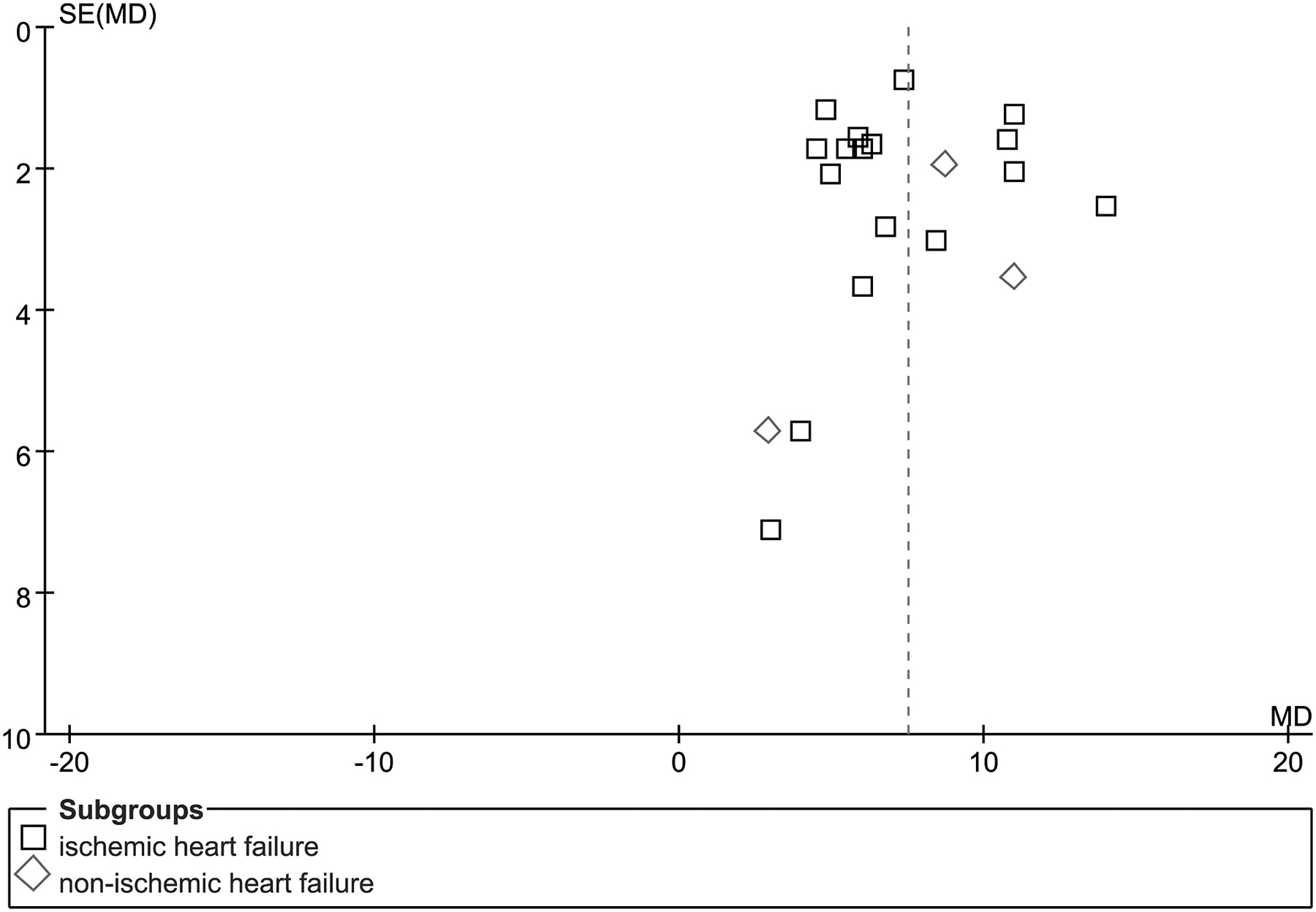
Funnel plot assessing evidence of publication bias from 16 trials.
Left ventricular end-systolic volume and left ventricular end-diastolic volume
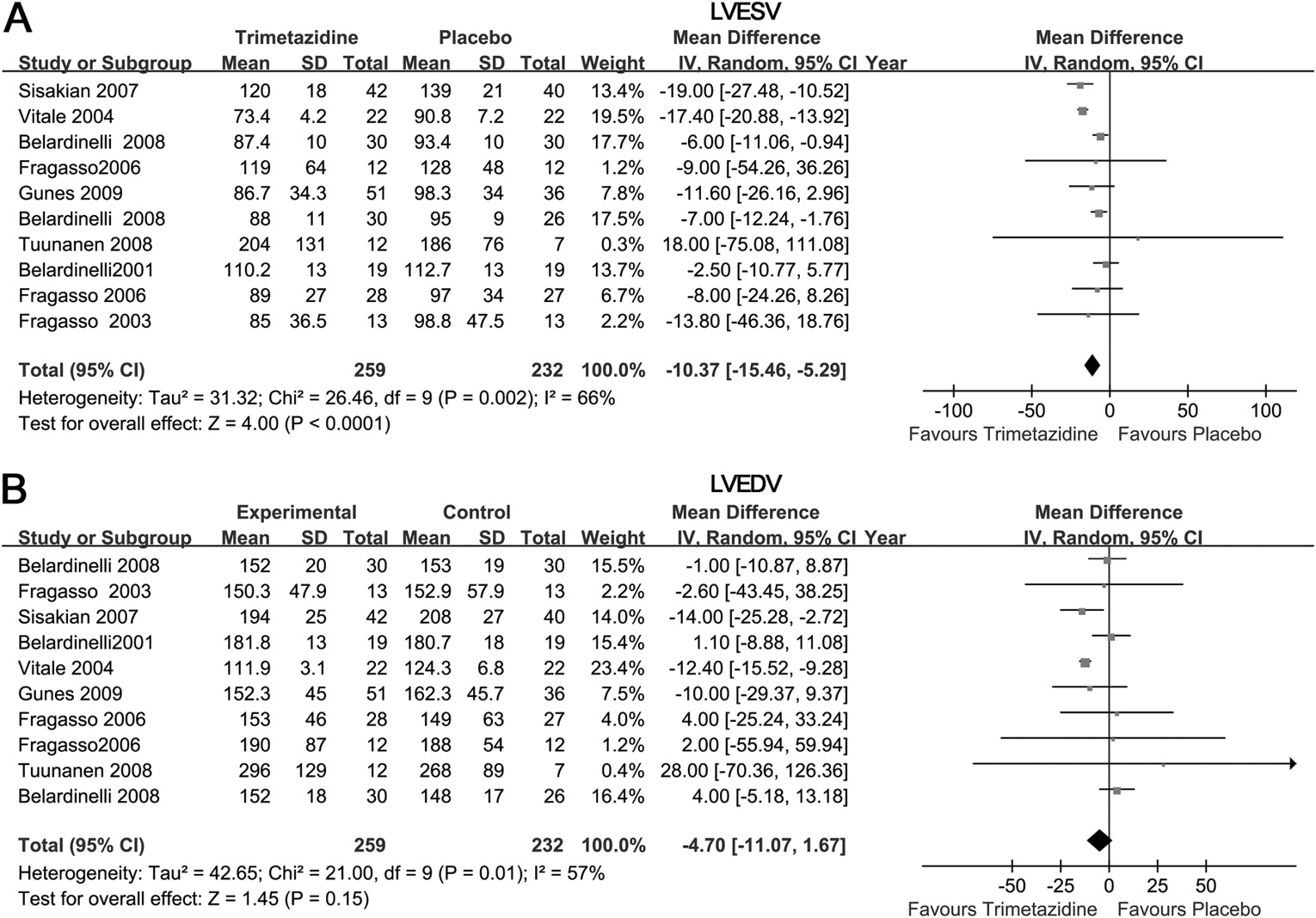
LVESV was significantly lower in patients who received trimetazidine therapy than placebo treatment (WMD −10.37 ml; 95% CI −15.46 to −5.29; p<0.01) (figure 5). LVEDV was not significantly decreased in response to trimetazidine treatment (WMD −4.70 ml; 95% CI −11.07 to 1.67; p=0.15).

Forest plot of weighted mean differences for left ventricular end-systolic volume (LVESV) (A) and left ventricular end-diastolic volume (LVEDV) (B) for patients with heart failure receiving trimetazidine or placebo. IV, inverse variance.
Clinical symptoms
NYHA classification
For the seven reports containing data on NYHA classification, trimetazidine therapy resulted in a significant improvement in NYHA classification compared with placebo (WMD −0.41; 95% CI −0.51 to −0.31; p<0.01) (figure 6A).
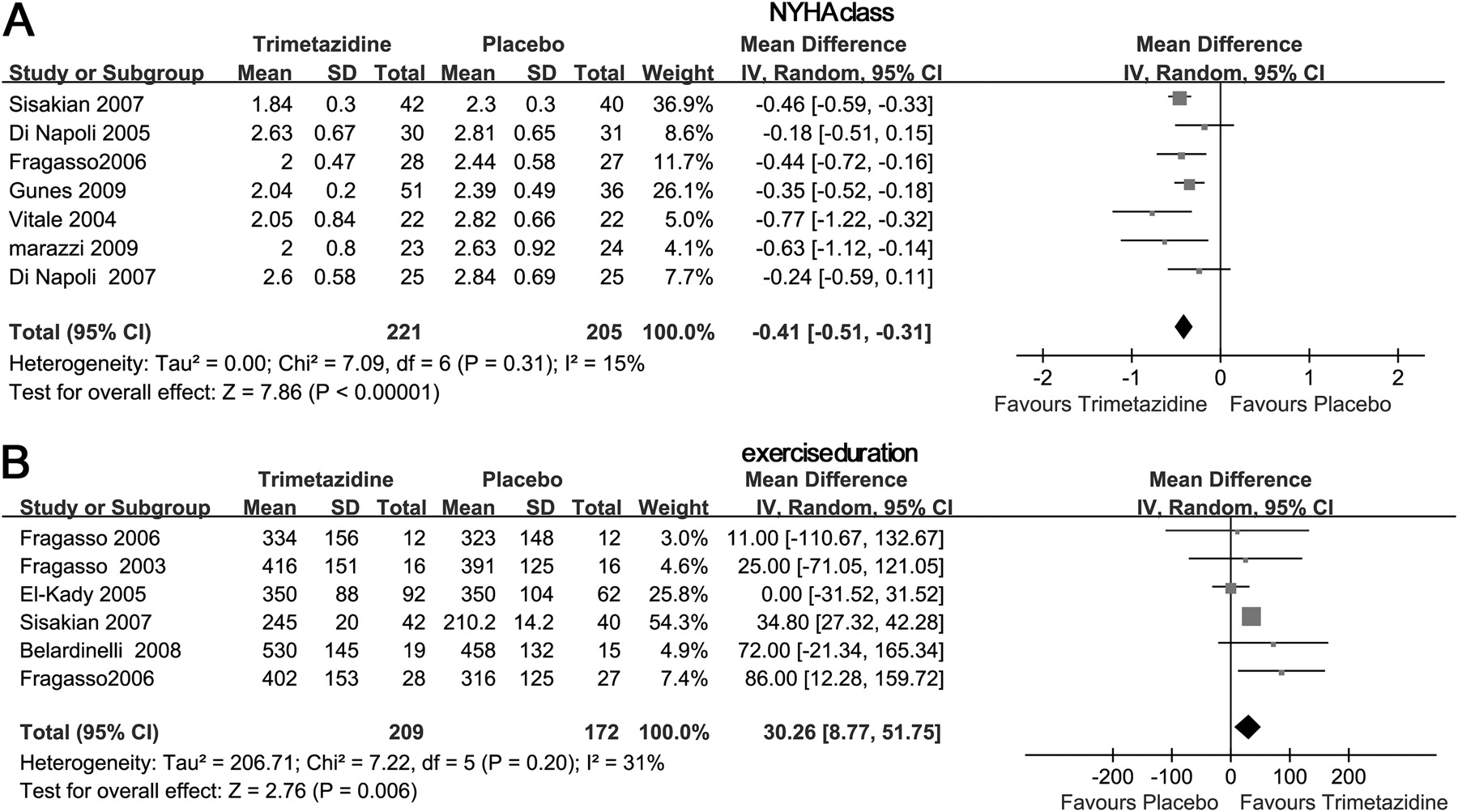
Forest plot of weighted mean differences for New York Heart Association classification (NYHA) (A) and exercise duration (B) for patients with heart failure receiving trimetazidine or placebo. IV, inverse variance.
Exercise capacity
For the six reports containing data for exercise capacity, trimetazidine significantly increased exercise duration compared with placebo control (WMD 30.26 s; 95% CI 8.77 to 51.75; p=0.01) (figure 6B).
Major adverse events
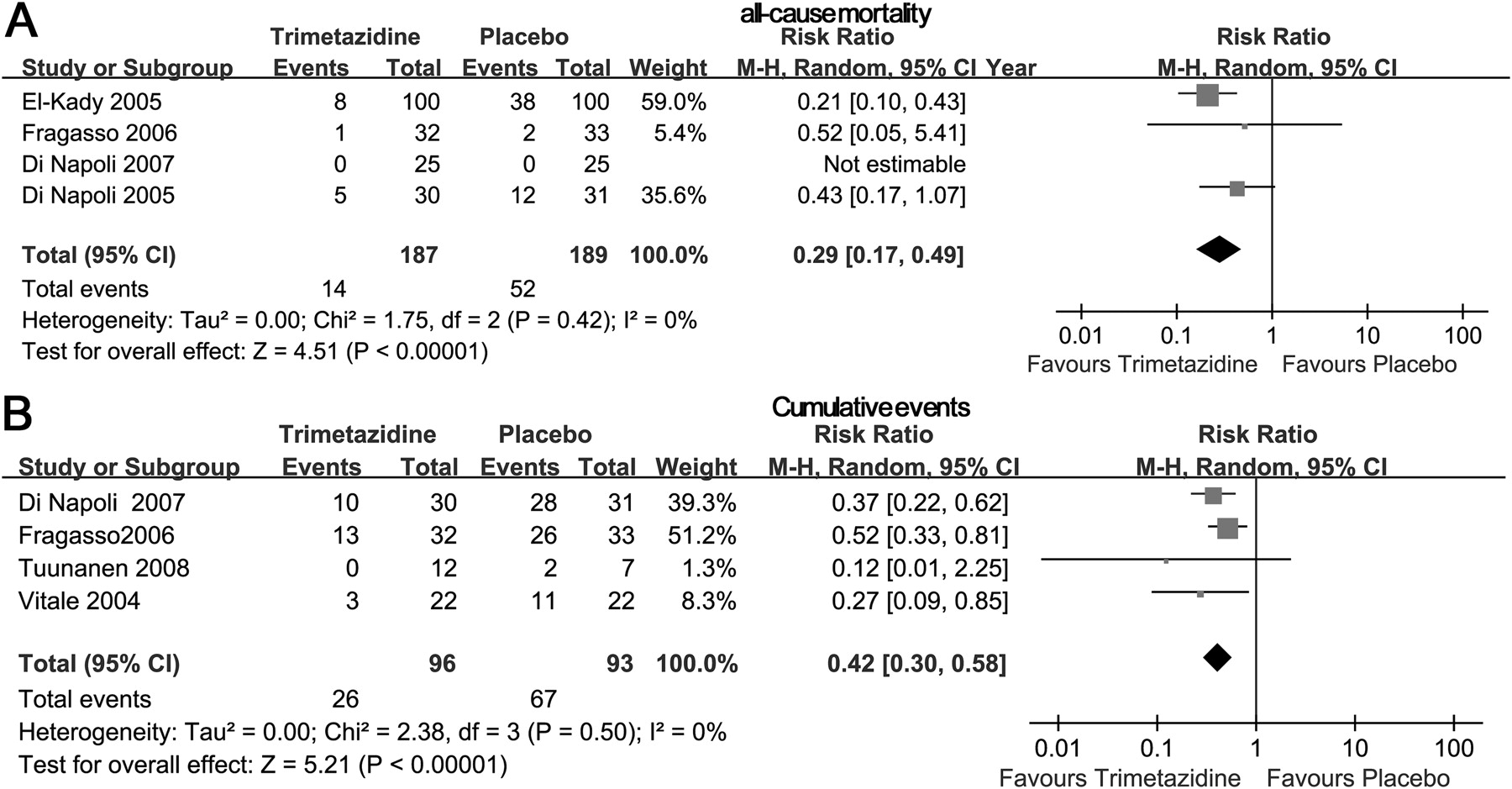
For the four reports containing data on mortality, with trimetazidine treatment mortality was lower than that with placebo (7.5%; 14/187 patients vs 27.5%; 52/189 patients), for a significant protective effect of trimetazidine treatment on mortality with HF (RR 0.29; 95% CI 0.17 to 0.49; p<0.01) (figure 7A).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Comparison of clinical outcomes of patients with heart failure receiving trimetazidine or placebo for (A) all-cause mortality and (B) cumulative events. M–H, Mantel–Haenzel.
Cardiovascular events and hospitalisation data reported for four trials revealed a significant decrease in these conditions with trimetazidine treatment (RR 0.42; 95% CI 0.30–0.58; p<0.01) (figure 7B).
Discussion
We performed a meta-analysis of RCT evaluating the effect of trimetazidine compared with placebo control on cardiac function variables, clinical symptoms and major adverse events in patients with chronic HF. We found trimetazidine treatment resulted in better cardiac function for ischaemic and non-ischaemic HF, and improved clinical symptoms. More importantly, trimetazidine was associated with a significant reduction in the RR for mortality, cardiovascular events and hospitalisation.
Trimetazidine is initially used as an anti-ischaemic or ‘cytoprotective’ agent through a metabolic pathway: switching cardiac metabolism from FFA to glucose oxidation, which is efficient in terms of oxygen consumption and energy production. Because FFA inhibitors can act as metabolic modulators in protecting the ischaemic myocardium, the effects of trimetazidine on HF have previously been assessed mainly in patients with ischaemic HF. The results of several small RCT have revealed improved cardiac function with trimetazidine. By pooling these results, our meta-analysis confirms increased LVEF in response to trimetazidine treatment in ischaemic HF. Because we included studies that were published over a long period (1990–2010), changes in practice over time could have an effect on the results. We observed a more profound effect of trimetazidine on LVEF (11%) in the study by Brottier et al36 in which ACE inhibitors/ARB or β-blockers were not used. Sensitivity analysis of the trials that ACE inhibitors/ARB and β-blockers were concomitantly used resulted in a WMD for LVEF of 7.49% to 7.14% (p<0.01), with reduced heterogeneity (I2 from 50% to 38%). This indicates that trimetazidine may improve cardiac function even with the concomitant use of current standard therapies. Trimetazidine was recently found to have cardioprotective effects in patients with HF of different aetiologies other than ischaemic HF.21 24 27 We pooled the results for LVEF from three trials of non-ischaemic HF in response to trimetazidine treatment and showed a significant improvement (8.72%) of LVEF with trimetazidine. Several lines of evidence suggest that high plasma levels of FFA and high rates of fatty acid oxidation in the myocardium results in impaired contractile function and a higher incidence of ventricular arrhythmias during and after myocardial ischaemia in the diabetic heart.38 Therefore, trimetazidine might have more benefit in patients with diabetes with HF. However, our pooled results showed a similar improvement in LVEF in this subgroup (WMD 6.19%; 95% CI 4.16 to 8.23). A mechanism other than an energy modulator, which positively redirects the neurohormonal pathway39 or inhibits cardiac fibrosis through an NADPH oxidase-reactive oxygen species connective tissue growth factor pathway,14 may contribute to this effect.
Improving clinical symptoms is an important treatment goal in HF. Our pooled results revealed an improvement in NYHA classification and exercise capacity (exercise duration) with trimetazidine. As a result of a lack of these outcomes, we cannot estimate the differential changes in NYHA classification and exercise capacity by different aetiologies. We found significant heterogeneity in our meta-analysis of exercise capacity (I2=85%). Differences in baseline exercise capacity and cardiac function may contribute to this heterogeneity.
In patients with HF, the effect of trimetazidine on mortality and other main outcomes is still controversial. Only four reports of RCT with small samples26 27 29 35 described all-cause mortality, and four described24 26 27 30 cardiovascular events and hospitalisation. The pooled results from our study indicate that trimetazidine provided a significant protective effect on decreasing the risk of all-cause mortality, cardiovascular events and hospitalisation. Given the relatively small sample sizes of the studies, we cannot estimate the effect of trimetazidine by different aetiologies, and more importantly the overall effect of trimetazidine on mortality in chronic HF should be tested in large-scale, randomised controlled clinical trials.
Some limitations of our meta-analysis need to be acknowledged. First, the methodological quality of the studies included in this analysis was less than optimal, with only five studies meeting all the validity criteria. Four studies were limited by their single-blind design. Three studies were open label, and three studies did not report blinding. We were not able to exclude the potential risk of bias in these trials. Second, the number of patients included in this meta-analysis was small, so some estimates such as for all-cause mortality, cardiovascular events and hospitalisation are based on relatively small numbers of measurements. However, we tried to include all available trials, and we did observe some benefits (including cardiac function, clinical symptoms and hard endpoints) associated with trimetazidine use. As a result of the small sample size, there is a probability of overestimating the clinical benefit if one does not exist (type I error). Results from our meta-anlaysis should be interpreted with caution. Third, we did not have access to individual patient data. Subgroups of HF patients might show a difference with trimetazidine treatment, but we could not perform these analyses given the limited number of patients for the currently available reports, especially for major adverse events. Finally, the follow-up times varied widely, from 4 weeks to 48 months.
In conclusion, our meta-analysis shows that trimetazidine improves systolic function and clinical symptoms for patients with chronic HF, as shown by a significant change in systolic function, NYHA classification and exercise duration. Moreover, these improvements associated with trimetazidine may result in reduced all-cause mortality, cardiovascular events and hospitalisation after long-term treatment. Given these results, large-scale, prospectively designed, randomised, double-blinded trials are still required to clarify some of these questions. Trimetazidine might be a choice for patients with chronic HF, especially those with ischaemic HF, even for whom current standard therapies are used. However, until now, we cannot recommend the routine use of trimetazidine for the treatment of HF.
References
Footnotes
See Editorial, p 267
Linked articles 214932.
Funding This study was supported by a grant from the National Natural Science Foundation of China (no 30900617 to DG), Research Fund for the Doctoral Program of Higher Education of China (no 2008.6981036 to DG), and Major Basic Research Development Program of China from the Ministry of Science and Technology (no 2006CB503802 to XN).
Competing interests None to declare.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.