Article Text

Abstract
Objective There is a paucity of data on the impact of complete revascularisation (CR) following percutaneous coronary intervention (PCI) among patients with diabetes with multivessel coronary disease. In this study, we assess the impact of CR, using a relatively simple anatomical definition, on long-term outcomes (median follow-up 7.9 years) in patients with diabetes, and compare with patients without diabetes.
Methods 5350 patients with multivessel disease (coronary stenoses ≥70% in ≥2 major epicardial arteries) who underwent PCI between January 1997 and June 2011 were included. Patients were divided into 4 groups according to diabetes and CR status (absence of residual coronary stenosis in major, predominantly proximal, epicardial segments according to Coronary Artery Surgery Study (CASS) classification).
Results Patients with diabetes and patients with incomplete revascularisation (IR) had more adverse clinical and angiographic characteristics. IR was frequent in patients with diabetes, and was marginally more common than in patients without diabetes (47% vs 44%, p<0.001). Patients with diabetes and patients without diabetes had higher mortality rates after IR than after CR (HR 1.56 (95% CI (1.39 to 1.85), p<0.001 for patients with diabetes and 1.70 (95% CI (1.50 to 1.92), p<0.001) in patients without diabetes). However, the absolute risk was higher for patients with diabetes (5-year mortality: IR 35.8%, CR 21.2%) than in patients without diabetes (5-year mortality: IR 22.2%, CR 14.1%). In a multivariable model, IR and diabetes mellitus were independent predictors of total mortality. This effect was present in the bare metal stent and drug-eluting stent eras and in patients with stable disease and acute coronary syndromes.
Conclusions CR is associated with lower long-term mortality in patients with diabetes and patients without diabetes. However the difference was significantly greater in patients with diabetes compared with patients without diabetes.
Statistics from Altmetric.com
Introduction
The prevalence of diabetes mellitus (DM) and associated morbidity and mortality due to cardiovascular disease is on the rise in the USA and around the world.1 This fact represents a major threat to the recent progress made in the prevention and treatment of coronary artery disease. Therefore, improved understanding of the mechanisms implicated in development and prognosis of coronary artery disease in patients with diabetes is essential. Currently, there is a paucity of data on the impact of incomplete revascularisation (IR) following percutaneous coronary intervention (PCI) among patients with diabetes with multivessel disease.2
Moreover, the data on IR in general are controversial and inconclusive due to the use of inconsistent definitions,3 variable thresholds for defining significant obstructive atherosclerosis,4 combination of percutaneous or surgical revascularisation,5 evolution in PCI techniques over time,6 and analyses being restricted to selective patient populations.4 ,7 ,8 The published studies are post hoc analyses from clinical trial4 ,6 ,7 or administrative databases8 ,9 and do not provide long-term outcomes among an all-comers diabetic population undergoing PCI. We hypothesised that IR is associated with adverse outcomes following PCI in patients with diabetes. The aim of this study was to evaluate the frequency and impact of IR on long-term mortality and revascularisation from a large consecutive series of patients with diabetes with multivessel disease undergoing PCI for stable angina and acute coronary syndromes (ACS) using a simple, intuitive definition of IR, and comparing their outcomes with patients without diabetes.
Methods
All patients undergoing PCI at the Mayo Clinic in Rochester, Minnesota, are prospectively enrolled in a registry which includes demographic, clinical, angiographic and procedural data. Follow-up of all patients is standardised with recording of immediate postprocedural and inhospital events and phone surveys using a standardised questionnaire at 6 months, 1 year and then annually after the procedure by trained data technicians. Routinely, 10% of all records are randomly audited by the supervisor for data integrity. All adverse events are confirmed by reviewing the medical records of the patients followed up at our institution and by contacting the patients’ physicians and reviewing the hospital records of patients treated elsewhere.
Study population
The study included patients from January 1997 to June 2011. Subjects with multivessel disease, defined as coronary stenoses ≥70% in two or more of the three major epicardial arteries and their branches were included in this analysis. Lesions of interest for revascularisation had to involve the following segment Coronary Artery Surgery Study (CASS) classification10 (segments 1,2,3 for right coronary; segment 11 for left main; segments 12 and 13 for left anterior descending; and finally segment 18 for circumflex (and 19 if left dominant/balanced are present)). Exclusion criteria were cardiogenic shock prior to PCI, prior coronary artery bypass graft (CABG) surgery, unsuccessful PCI in any lesion, and refusal of research authorisation. The earliest complete qualifying PCI per patient was considered the index event. The primary group of interest was those with DM but data on patients without diabetes is also provided for comparison.
To assess the impact of PCI technique, patients were divided into two groups according to the date of their intervention: (1) the bare-metal stent (BMS) era (January 1997 through March 2003) included patients from a time period during which routine stenting with such stents was the preferred strategy in conjunction with dual oral antiplatelet therapy; and (2) the drug-eluting stent (DES) era (April 2003 through June 2011) consisted of patients whose PCI reflects contemporary practice.
In accordance with a State of Minnesota statute, patients who did not grant authorisation for medical records research were also excluded from the analysis (205 patients between 1 January 1990 and 30 June 2011).
Definitions
DM was defined as a documented history of diabetes treated with medication or diet. Complete revascularisation (CR) was defined as successful PCI to all significant lesions in the segments of interest during the index hospitalisation. Conversely, IR was defined if there was successful PCI to one more lesion but there was at least one significant lesion in the segments of interest that was not treated. Procedural success was defined as a reduction of residual luminal diameter stenosis to no more than 20% without inhospital death, Q-wave myocardial infarction (MI) or need for emergency CABG. Acute coronary syndrome was defined as either (1) MI within the previous 7 days or (2) unstable angina requiring non-elective PCI.
Primary end point of interest was all-cause mortality following discharge. Secondary end point was any target lesion revascularisation.
Statistical analysis
Continuous data are summarised as mean (SD) unless otherwise stated. Categorical data are summarised as frequency (group percentage). Group comparisons were made between patients with and without diabetes and between completely revascularised and incompletely revascularised patients within diabetes status. One-way analysis of variance and Pearson's χ2 tests are used for continuous and categorical data, respectively. Ordinal variables are tested using the Kruskal-Wallis test. Kaplan-Meier methods are used to estimate follow-up event rates, with follow-up beginning at time of discharge (unsuccessful PCIs and patients who died in hospital were excluded); group tests were conducted with the log-rank test. Survival plots demonstrate the absolute risk reduction over time. Multiple Cox regression models for mortality were constructed with risk-adjustment through the Mayo Clinic Risk Score for long-term mortality.11 Models for repeat revascularisation also adjusted for age, gender, current smoker, history of MI, history of peripheral vascular disease, cerebrovascular accident/transient ischaemic attack, calcium in stenosis, device size and use of DES. Also included in the models were indicator variables for diabetes, CR and the interaction between those two factors. HRs from the models reflect the relative risk of patients with diabetes versus those without and for IR versus CR. Interaction effects were retained regardless of the significance of the interaction to demonstrate effect sizes within subgroups of DM and CR. The proportional hazards assumption was assessed by means of plotting scaled Schoenfeld residuals over time and overlaying a scatter plot smoother with 95% CIs. There was no evidence of a violation of the assumptions.
Results
Five thousand three hundred and fifty patients with multivessel disease undergoing PCI met the inclusion criteria for this study. Of these, 1425 (26.6%) had, and 3925 (73.4%) did not have DM. IR was present in 2377 (44.4%) patients, and it was marginally more frequent in patients with diabetes 668/1425 (46.9%) compared with patients without diabetes 1709/3925 (43.5%), p<0.001.
Baseline clinical characteristics
Main differences between groups are described; Comparison patients with diabetes versus patients without diabetes; patients with diabetes with IR versus CR (table 1).
Baseline clinical characteristics
Angiographic and procedural characteristics
Compared with patients without diabetes, patients with DM presented unfavourable characteristics and use of DES was higher (table 2).
Angiographic and procedural characteristics
Patients with diabetes with IR, compared with those with CR, had more severe disease. Patients with IR also received fewer stents and were less likely to have DES.
Long-term outcomes
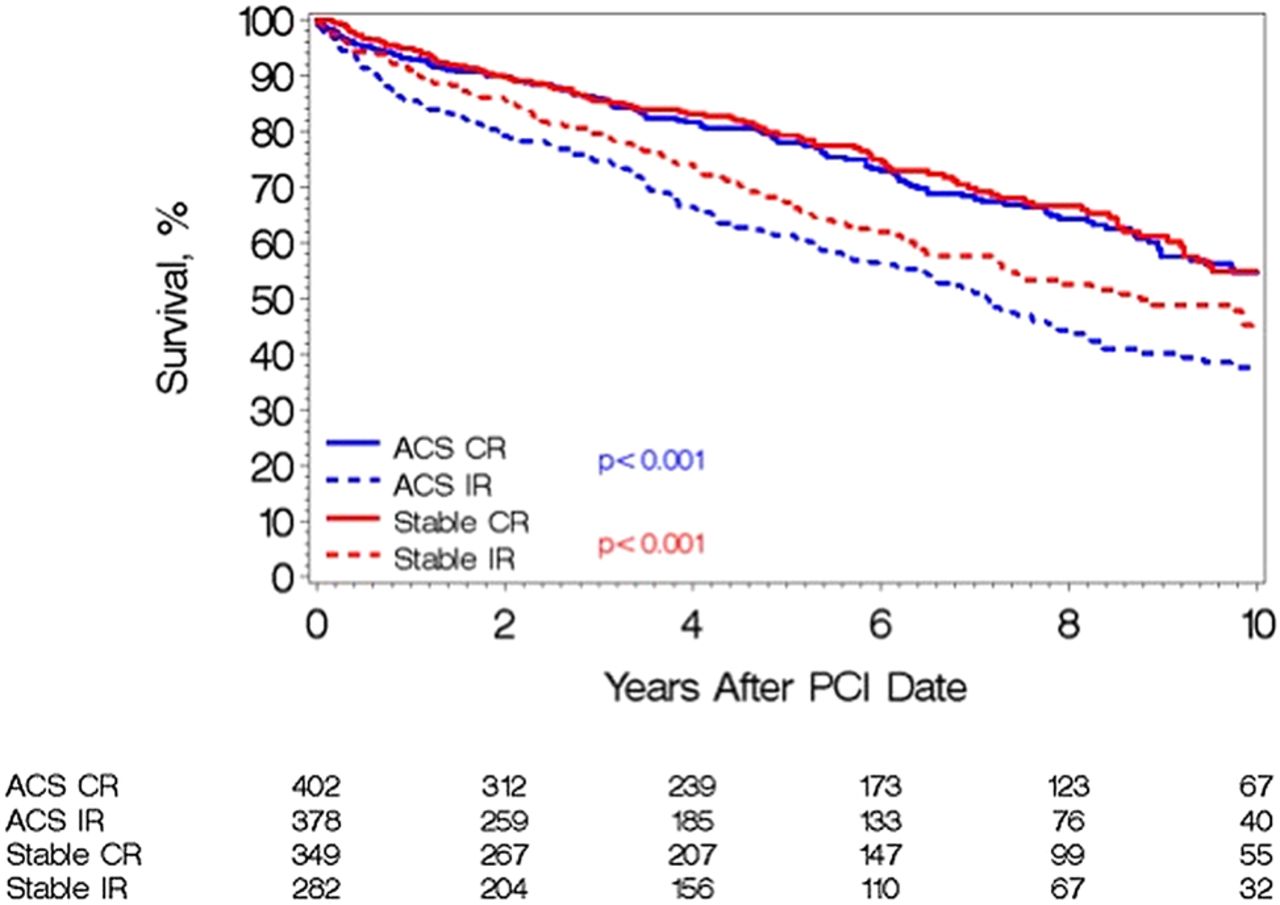
The median duration of follow-up was 7.9 (IQR 4.2, 10.8) years. Fifty-nine per cent of patients had follow-up available within 1 year of freezing the data for analysis, and 79% had follow-up available in the prior 2 years. Patients with DM had a higher mortality, and those with IR had significantly greater mortality compared with those with CR (figure 1, p<0.001). In subgroup analyses among patients with diabetes, the differential outcome between IR and CR was present during the BMS and DES eras (figure 2); and when PCI was performed for stable disease versus ACS (figure 3).

Unadjusted mortality curves during follow-up for patients with diabetes and patients without diabetes according to complete (CR) or incomplete revascularisation (IR). PCI, percutaneous coronary intervention.

Unadjusted mortality curves during follow-up for bare-metal stent (BMS) and drug-eluting stent (DES) eras. CR, complete revascularisation; IR, incomplete revascularisation; PCI, percutaneous coronary intervention.

{kind=link}
{kind=link}
{kind=link}
Unadjusted mortality curves during follow-up for stable disease versus acute coronary syndrome (ACS). CR, complete revascularisation; IR, incomplete revascularisation; PCI, percutaneous coronary intervention.
In univariate analysis, patients with diabetes and patients without diabetes with IR had higher mortality rates compared with those with CR (HR 1.56 (95% CI (1.39 to 1.85), p<0.001), and was 1.70 (95% CI (1.50 to 1.92), p<0.001), respectively. Though the relative risk was similar, the absolute risk was higher for patients with diabetes (5-year mortality: IR 35.8%, CR 21.2%) than in patients without diabetes (5-year mortality: IR 22.2%, CR 14.1%). In a multivariable model that included the Mayo Clinic risk score, which was by far the most powerful independent predictor, IR and DM were also independent predictors (table 3). There was no significant evidence that the effect of CR was different between patients with and without diabetes.
Multivariable Cox model for long-term mortality
By univariate analysis, the HR for repeat revascularisation with respect to IR in patients with diabetes was 1.10 (0.92 to 1.33); p=0.28, while it was 1.23 (1.09 to 1.38); p<0.001 in patients without diabetes. In a multivariable model that included Mayo Clinic risk scores for death and death/MI as well as risk factors for restenosis, IR and DM were also independent predictors of repeat revascularisation (table 4). There was no significant evidence that the effect of CR was different between patients with and without diabetes.
Multivariable Cox model for long-term repeat revascularisation
Discussion
The main findings of our study are the following. First, we observed that IR is common (47%) following PCI in our population of patients with diabetes with multivessel coronary artery disease without prior CABG, and is marginally more frequent than in patients without diabetes (43%). Second, CR is associated with lower long-term mortality in patients with diabetes and patients without diabetes. The lower relative risk with CR versus IR was similar in both groups (41% vs 36%), however, the absolute risk was significantly higher in patients with diabetes (14.6% at 5 years) compared with patients without diabetes (8.1%). Third, this effect was present in the BMS and DES eras. Finally, the relationship between CR and mortality was present regardless of whether revascularisation was for stable disease or ACS.
Prior studies have reported a variable frequency (41–67%) and prognostic impact of IR following PCI. There are many reasons for these inconsistencies. First, there is no uniformly accepted definition of IR, and it has been generally limited to angiographic criteria.3 ,5 ,12 The commonly used anatomical definitions have used the presence of an untreated ≥50% stenosis in any coronary artery that is >1.5 mm in diameter, but others have been more stringent with >70% stenosis as the cut-off, and some limiting assessment to vessels >2.5 mm in diameter.12 However, there is a need for a practical, simple, intuitive definition of IR for clinical studies and practice. The pragmatic definition of IR used in the present study avoids the need to integrate vessel diameter, a measure that is generally neither recorded in large databases nor routinely measured in practice. Rather, we focused on the proximal coronary segments of the three major epicardial arteries as surrogates for large areas of myocardium at jeopardy from significant (>70% diameter stenosis) atherosclerotic lesions, and hence ischaemic burden.
Our study is unique in that it provides very long-term follow-up among a large ‘all-comers’ cohort of patients with diabetes who were evaluated to address the impact of the completeness of percutaneous revascularisation. It demonstrates that non-diabetic status and CR are independently associated with a lower risk of death. This risk is independent of the many adverse baseline characteristics that cluster in patients with diabetes and known to influence survival (table 3). While the relative impact of CR was similar in patients with diabetes and patients without diabetes, CR resulted in a significantly greater absolute risk reduction in patients with diabetes. Thus, survival of patients without diabetes with IR was identical to that of patients with diabetes with CR (figure 1). The improved outcomes associated with CR were present in the BMS and DES eras suggesting that changes in stent technology and adjunctive pharmacological therapies have not significantly altered this relationship. Moreover, the association hold true regardless of the acuity of presentation at the time of PCI, a fact that to the best of our knowledge has not been previously reported. Our data is consistent with that published by Schwartz et al,7 Garcia et al13 and Head et al14 from post hoc analyses of clinical trials who described the impact of completeness of revascularisation on long-term (5 years) cardiovascular outcomes. To date, the only published observational ‘all-comers’ study reporting on patients with diabetes has a small (n=191) sample size15 in which CR was associated with better composite outcomes, but it was underpowered to show a statistically significant relationship with hard end points such as death.
Patients with diabetes represent a large proportion of patients requiring consideration for revasularisation.2 The FREEDOM trial16 and substudies from the SYNTAX trials17 have confirmed the superiority of CABG over PCI for patients with diabetes with advanced multivessel disease. Therefore the present guidelines-based approach in patients with diabetes with multivessel disease is the calculation of the SYNTAX score and a review by the ‘heart team’. CABG is a class 1 indication in patients with three vessel and/or left main disease and a SYNTAX score of >22.18 ,19 However, PCI remains a consideration for a significant proportion of patients with diabetes either because they are not suitable for CABG (eg, diffuse distal vessels, comorbidities) or because the patient does not wish to have surgery.4 ,20 Thus, our findings remain pertinent to contemporary practice and the significance of CR merits further investigation.
Intuitively, the rate of single vessel PCI would have been expected to be low in those with CR. However, despite, the presence of multivessel disease, the majority (72%) of patients in our study underwent single vessel PCI, regardless of the diabetes status. Among those achieving CR, the frequency of single vessel PCI was marginally lower at 66–68%. This compares with single vessel PCI rates of 85% and multivessel disease frequency of approximately 50% in our practice, figures that have remained unchanged over a 25-year period.21 Thus, the high frequency of single vessel PCI reflects the overall practice of PCI and also the inclusion criterion which limited the segments of interest to the proximal coronary tree.
The present study has several limitations. First, we did not perform systematic assessment of ischaemic burden (eg, fractional flow reserve measurement or stress testing) or viability to ascertain the full clinical significance of the stenoses. However, we believe that the cohort selected for the study would have included patients with clinically meaningful and significant lesions. Moreover, perfusion scintigraphy and other stress tests are not without their own limitations in multivessel coronary disease.22 ,23 Second, our study is retrospective and subject to the limitations of such analyses. Thus, we did not prospectively collect the reasons for CR versus IR, nor the reason for unsuccessful PCI among those excluded from the study. This raises the possibility of unmeasured confounders; for example, the success or ease of the PCI procedure may itself be associated with the decision to proceed with CR versus IR and may be associated with the likelihood of adverse events. Patients with IR had more advanced disease, which may have contributed to the relationship with adverse outcomes. However, we performed multivariate analysis including a large number of variables to adjust for these differences between the groups.
In conclusion, our all-comers study, among the largest cohort of patients with diabetes undergoing percutaneous coronary revascularisation, confirms the adverse prognostic association of IR and long-term mortality. While our retrospective study cannot establish a causal link, it is hypothesis generating and highlights the potentially important clinical significance of achieving CR and assessing the optimal strategy for patients with diabetes with multivessel coronary disease. This needs to be considered in the context of other variables24–27 such as age, LV function, severity of symptoms, myocardial viability,28 antiplatelet therapy29 and coronary anatomy (presence of chronic total occlusion, suitability of the left anterior descending artery for grafting and quality of the distal vessels).
Key messages
What is already known on this subject?
It is well known that patients with diabetes have a worse prognosis than patients without diabetes after percutaneous coronary revascularisation. Moreover, there is debate about impact of complete revascularisation among patients with diabetes and patients without diabetes with multivessel disease. In this study, we assess the impact of complete revascularisation, using a relatively simple anatomical definition, in a large (>5000 patients) cohort, on long-term outcomes (median follow-up 8 years).
What might this study add?
Complete revascularisation is associated with lower long-term mortality in patients with diabetes and patients without diabetes. However absolute risk reduction was significantly higher in patients with diabetes compared with patients without diabetes. This was present in patients with stable disease and acute coronary syndromes.
How might this impact on clinical practice?
The study is significant because it highlights the potential importance of complete revascularisation in patients with diabetes as well as patients without diabetes across the spectrum of coronary artery disease presentations.
References
Footnotes
Contributors All authors have substantial contributions to this paper.
Funding MFJ-N received a grant from Institute of Health Carlos III, ISCIII (Ministry of Economy and Competitiveness) (Spain) (Beca BAE) and from Sociedad Andaluza de Cardiología (Beca Estancia Extranjero).
Competing interests None.
Patient consent Obtained.
Ethics approval The Institutional Review Board at Mayo Clinic.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Limited.