Article Text

Abstract
Objective To determine whether provision of web-based lifestyle advice and coronary heart disease risk information either based on phenotypic characteristics or phenotypic plus genetic characteristics affects changes in objectively measured health behaviours.
Methods A parallel-group, open randomised trial including 956 male and female blood donors with no history of cardiovascular disease (mean [SD] age=56.7 [8.8] years) randomised to four study groups: control group (no information provided); web-based lifestyle advice only (lifestyle group); lifestyle advice plus information on estimated 10-year coronary heart disease risk based on phenotypic characteristics (phenotypic risk estimate) (phenotypic group) and lifestyle advice plus information on estimated 10-year coronary heart disease risk based on phenotypic (phenotypic risk estimate) and genetic characteristics (genetic risk estimate) (genetic group). The primary outcome was change in physical activity from baseline to 12 weeks assessed by wrist-worn accelerometer.
Results 928 (97.1%) participants completed the trial. There was no evidence of intervention effects on physical activity (difference in adjusted mean change from baseline): lifestyle group vs control group 0.09 milligravity (mg) (95% CI −1.15 to 1.33); genetic group vs phenotypic group −0.33 mg (95% CI −1.55 to 0.90); phenotypic group and genetic group vs control group −0.52 mg (95% CI −1.59 to 0.55) and vs lifestyle group −0.61 mg (95% CI −1.67 to 0.46). There was no evidence of intervention effects on secondary biological, emotional and health-related behavioural outcomes except self-reported fruit and vegetable intake.
Conclusions Provision of risk information, whether based on phenotypic or genotypic characteristics, alongside web-based lifestyle advice did not importantly affect objectively measured levels of physical activity, other health-related behaviours, biological risk factors or emotional well-being.
Trial registration number ISRCTN17721237; Pre-results.
- heart disease
- coronary artery disease
- cardiac risk factors and prevention
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Many cardiovascular disease (CVD) primary prevention strategies involve identification of individuals at high risk using scores incorporating information on phenotypic factors such as age, sex, smoking, blood pressure and serum lipids.1 Several randomised controlled trials have investigated the impact of providing phenotypic risk information to individuals and practitioners.2 3 However, those trials are limited by modest power, use of imprecise measures or reliance on participants’ self-reported measures of behaviours.2 3
As understanding of the genetic determination of CVD has advanced,4 it has been suggested that genetic information could augment risk prediction.5 Again, however, although a previous systematic review reported no strong effects, little is reliably known about the potential benefits and harms of provision of CVD genetic risk information due to limitations of existing studies.6 Similar limitations apply to previous randomised evidence about the potential benefits and harms of providing web-based lifestyle advice, which could be an effective7 and scalable8 communication approach.
To address these uncertainties, we conducted the Information and Risk Modification (INFORM) trial. We aimed to quantify the short-term (12 weeks) effects of provision of phenotypic and genetic coronary heart disease (CHD) risk information, alongside a web-based lifestyle intervention, on changes in objectively measured physical activity and dietary behaviour, cardiovascular risk factors, perceived risk and psychological outcomes.
Methods
Trial design
We have previously reported full details of the trial design and methods.9 Briefly, INFORM is a parallel-group, open randomised trial. We allocated participants in a 1:1:1:1 ratio to either a no intervention control group (group 1, control group) or to one of three active intervention groups: web-based lifestyle advice only (group 2, lifestyle group); lifestyle advice plus information on estimated 10-year CHD risk based on phenotypic characteristics (group 3, phenotypic group) and lifestyle advice plus information on estimated 10-year CHD risk based on phenotypic and genetic characteristics (genetic risk estimate) (group 4, genetic group). All participants provided electronic informed consent. We did not provide any incentives for participation in this study.
Participants
INFORM participants were a convenience sample of those recruited into the INTERVAL study, a trial of blood donors throughout England randomised to different frequencies of blood donation.10 We invited INTERVAL participants to take part in the INFORM trial if they had completed the 2-year follow-up questionnaire for the INTERVAL study, provided a blood sample for genotyping and indicated an interest in wearing a physical activity monitor. The most important eligibility criteria for the INFORM trial were: aged 40–84 years at the time of recruitment and no history of CVD.9 The INFORM trial was administered by the University of Cambridge. We recruited participants between March and June 2015 and completed follow-up on 31 December 2015.
Randomisation and blinding
Randomisation of the INFORM participants was undertaken centrally at the trial coordinating centre at the Department of Public Health and Primary Care, University of Cambridge. We randomised participants at the individual level using a computer program built into the study database. A data manager (MW), working independently from the trial coordinators, designed and implemented this computer program. We stratified randomisation by age (≤60 years) and sex in order to balance baseline phenotypic CHD risk across study groups. Participants were randomised into intervention arms on a daily basis based on an assigned random number. Given the nature of the trial, it was not possible to blind participants to which intervention they received. However, researchers assessing the trial outcomes and processing data remained blinded to study group allocation.9
Interventions
The intervention in the INFORM trial was web-based, informed by evidence available at the time of designing the study and piloted before the trial. The phenotypic and the genetic CHD risk estimates consisted of three pieces of information: the absolute risk of having CHD in the next 10 years; ‘Heart Age’ and a comparative risk estimate (see online supplement S1 and S2). We have previously reported the methods for calculating phenotypic and genetic risk estimates in detail (for examples of calculating phenotypic and genetic CHD risk estimate, refer to the study bySilarovaet al (this needs to be reference 9) 11: additional file 1B and 1E, respectively). We presented both phenotypic and genetic CHD risk estimates in exactly the same format to ensure that the only experimental difference was the addition of information on the risk of CHD based on genetic variants.
Supplementary file 1
The web-based lifestyle advice was adapted for the UK population from an intervention developed for the US Heart to Health study12 (following permission from the corresponding author), which has been shown to be effective at reducing modelled CHD risk and improving health-related behaviours at both 4 and 12 months.7 In the INFORM trial, the web-based lifestyle advice consisted of three interactive sessions (a library of over 250 web pages) tailored to participants’ individual characteristics. Participants could, for example, set their own goals and first steps on how they were going to achieve their goals. Separate modules were available for physical activity, diet and smoking cessation using behaviour change techniques such as goal setting, feedback and tips on overcoming barriers.12 Sessions were delivered at monthly intervals.
Outcomes
Primary outcome
The primary outcome was objectively measured physical activity, defined as daily average activity-related acceleration (expressed in relative gravity, milligravity (mg)) assessed using the wrist-worn Axivity AX3 3-Axis Logging Accelerometer. Participants were instructed to wear the accelerometer for seven consecutive days and nights. If INFORM participants took part in physical activity monitoring as part of a substudy within the INTERVAL trial prior to the randomisation, their existing physical activity data were used as a baseline measurement for INFORM. All other participants undertook physical activity monitoring within INFORM prior to randomisation as a baseline assessment. Follow-up assessment of physical activity occurred 12 weeks postrandomisation. Identical procedures were used for physical activity monitoring in INFORM and INTERVAL. We cleaned and processed raw acceleration data in line with previous studies reporting activity-related acceleration (mg).11 13 14
Secondary outcomes
All prespecified secondary outcomes except CHD-related worry were recorded at baseline and at 12 weeks postrandomisation. More details on these measures are reported elsewhere9 and in online supplement S3 and S4. We also conducted individual interviews and focus groups with participants who were allocated to the active intervention groups to gain further insight into the effectiveness and feasibility of our interventions. This qualitative substudy is reported separately.15
Patient involvement
Patient involvement representatives (CG and KL) were recruited from the Patient and Public Involvement Panel at Cambridge University Hospitals NHS Foundation Trust to the Trial Steering Committee, and were involved in study concept, design and overseeing the study. They also assisted with reviewing study documentation, the intervention, newsletters and this manuscript. Results of this study will be disseminated to study participants via email with the link to the publication.
Statistical methods
The statistical analysis plan was finalised prior to any analysis, and is available online16 and in online supplement S5. All trial analyses were based on the intention-to-treat principle.
We tested for any differences between the four randomised groups in mean change from baseline in objectively measured physical activity using an F-test of the relevant parameters from an analysis of covariance (ANCOVA) model, with adjustment for baseline. We also used this model to derive estimates of the baseline-adjusted differences in mean change and 95% CI for each of the four pairwise comparisons (group 2 vs group 1; group 4 vs group 3; group 3+4 vs group 1 and group 3+4 vs group 2).
For each continuous secondary outcome, we estimated the four pairwise differences using the method described above, except for CHD-related worry, which was only assessed at follow-up, and hence was analysed using linear regression. For binary secondary outcomes, we performed similar analyses using logistic regression.
We excluded those with missing follow-up data. Participants with missing baseline values of the outcome being analysed were included using the missing indicator method.17
For the primary outcome, we extended the ANCOVA model to include an interaction between randomised group and (1) age (below/above median of 56.7 years), (2) baseline phenotypic CHD risk (below/above median of 4%), (3) sex (men/women), (4) perceived phenotypic risk below/above absolute risk and (5) perceived genetic risk below/above absolute risk.
We performed all analyses using Stata Release V.14.
Sample size
Full details of the sample size calculation have been reported9; the calculation was performed using ‘sampsi’ in Stata.18 As in other studies,19 we defined a 10% increase in the primary outcome as important. We set the significance level to 1.25% to allow for four pairwise comparisons in the primary analysis. We calculated that 186 participants per group would be needed to detect this effect with 80% power and 95% confidence, assuming the estimated SD of change in physical activity from baseline to follow-up was 0.05 and the correlation between physical activity at baseline and follow-up was 0.6.20 Allowing for an attrition rate of 20%, we aimed to randomise a total of 932 participants (233 per group).
Results
Participant characteristics
The flow of participants through the INFORM trial is shown in figure 1. Following assessment of eligibility, we randomised 956 (32.9%) to the four study groups. Of those randomised, three participants (one from the phenotypic group and two from the genetic group) withdrew from the trial after randomisation and did not allow their data to be used. Hence, baseline characteristics are shown in table 1 for 953 participants. Of these 953 participants, four were randomised despite one not returning the baseline questionnaire and three not returning a baseline physical activity monitor. Three of those were randomised to the control group and one to the phenotypic risk estimate and lifestyle advice group. We included data in the analyses for these participants.
Baseline demographic and clinical characteristics for each group—intention-to-treat population
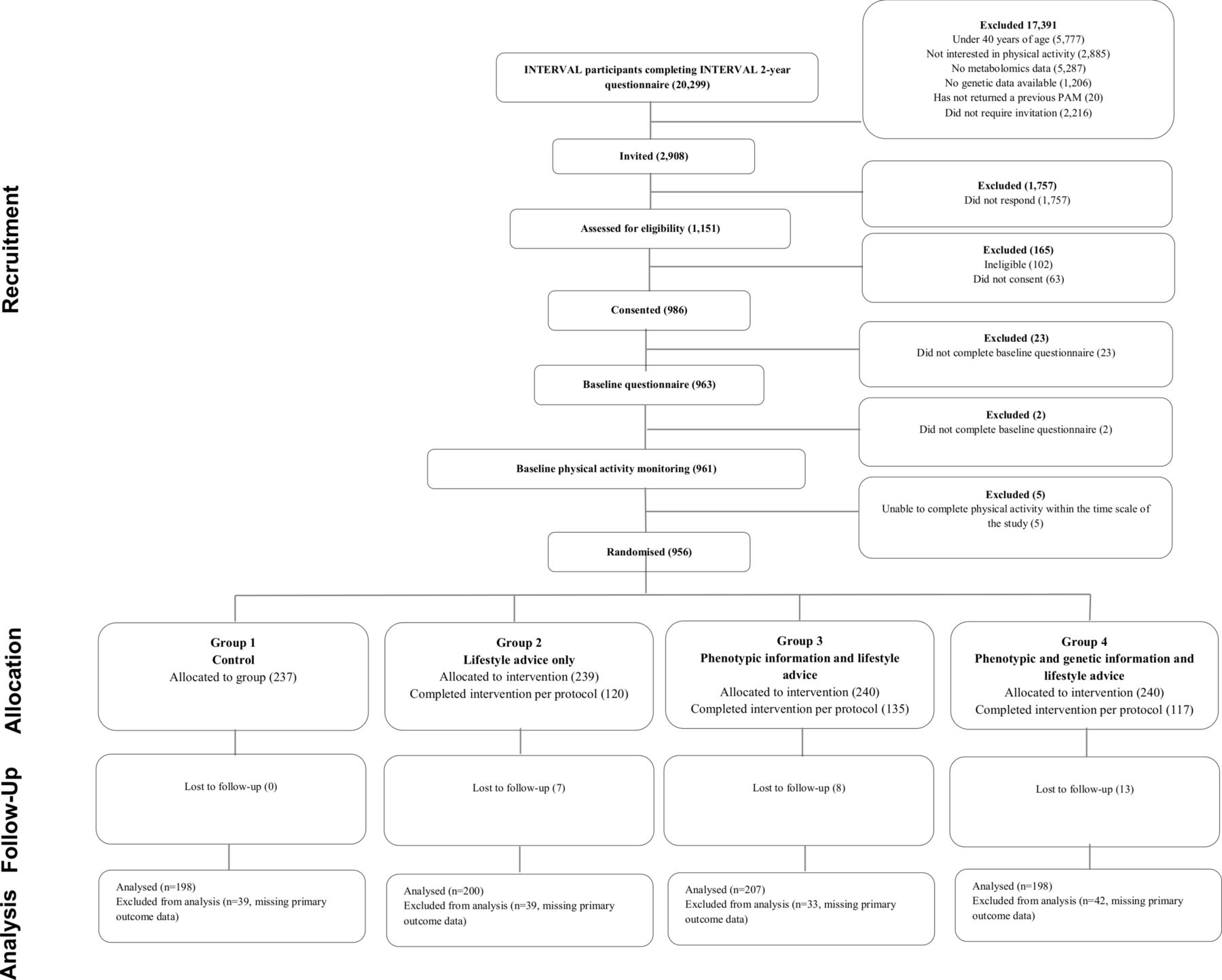
Flow of participants through Information and Risk Modification trial.
Primary outcome
The primary outcome was analysed for 803 (84%, figure 1) participants. There were no significant baseline differences between those with and without information on the primary outcome with regard to age, sex, education, ethnicity and family history of CHD and baseline phenotypic risk estimate (see online supplementary table S1). For each pairwise comparison of primary and secondary outcomes, the estimated effect sizes and 95% CI are presented in figure 2 and in online supplementary table S2. In addition, table 2 shows means and SDs for primary and secondary outcomes for each study group at baseline and change from baseline. There were no between-group differences in physical activity defined as an average acceleration (mg) over the observation period (difference in adjusted mean change from baseline). In addition, we analysed the data by risk level. Based on our statistical analysis plan,16 that was finalised prior to any analyses, we performed a test for interaction (group allocation×baseline phenotypic CHD risk score) for our primary outcome (change in objectively measured physical activity). There was no evidence of an interaction (p=0.89) and so we did not present the results stratified by baseline risk. Prespecified analyses showed that the interventions also had no effect on physical activity within subgroups defined by age (below/above median; p=0.30), sex (men/women; p=0.51), perceived phenotypic risk below/above absolute risk; p=0.563 and perceived genetic risk below/above absolute risk; p=0.283.

{kind=link}
{kind=link}
Pairwise comparisons for primary and secondary outcomes—intention-to-treat population (data are reported in natural units). Full details are reported in online supplementary table S2 (some values in the figure were inverted to fit with the favoured group). *CHD-related worry only measured at 12-week follow-up; difference, 95% CI and p value estimated from a linear regression model. Group 1: control; group 2: lifestyle advice only; group 3: phenotypic risk estimate and lifestyle advice; group 4: phenotypic and genetic risk estimates and lifestyle advice. Primary outcome and secondary continuous outcomes: difference and 95% CI estimated from analysis of covariance model with adjustment for baseline. Participants with missing values of the outcome at baseline included using the missing indicator method.
Means and SDs of baseline and change from baseline to follow-up values—intention-to-treat population
Secondary outcomes
There were no between-group differences in change in levels of serum carotenoids, lipid panel, fructosamine, self-reported whole grain, fish or alcohol intake, weight, perceived risk, overall stress, mood or smoking status (p≥0.02 for all) (figure 2; table 2 and online supplementary table S2).
Use (intervention adherence, exposure)
Of those who were allocated to any intervention group, 578 (80.7%) and 491 (68.6%) completed the first session on diet and physical activity, respectively, 406 (56.7%) and 298 (41.6%) the second session and 325 (45.4%) and 215 (30.0%) all three sessions. There were 21 (2.9%) smokers allocated to any of the intervention groups and 11 (52.4%) completed the first session concerning smoking, 4 (19.0%) the second session and 4 (19.0%) all three sessions on smoking.
Acceptability
Among those who received lifestyle advice, 460 (64.3%) participants considered it understandable, 417 (58.2%) trustworthy, 424 (59.3%) helpful, 340 (47.5%) motivating and 352 (49.2%) important in making decisions about decreasing their risk of CHD. The proportion of participants who believed that their risk was fair or very accurate and talked to a healthcare professional, family member or friend about it was 299 (62.7%) and 131 (27.6%), respectively, among those who received a phenotypic CHD risk estimate, and 134 (56.3%) and 51 (21.5%), respectively, among those who received a genetic CHD risk estimate. There were no statistically significant differences in responses to the question ‘How accurate do you believe your CHD risk is’ between those allocated to phenotypic CHD risk group and those allocated to genetic CHD risk group.
Discussion
Our results indicate that provision of risk information to individuals, whether based on phenotypic or genotypic characteristics, alongside web-based lifestyle advice, has limited potential to improve behavioural and biological risk factors for CVD in the population we studied (ie, middle-aged and older adults between 40 and 77 years without manifest CVD living in a Western industrialised country). Our data also indicate that communication of CHD risk information has no adverse effects on overall stress, or mood and was associated with only small changes in worry.
These results are consistent with those from previous literature-based reviews6 21 and most recent trials.22 However, INFORM should be considerably more robust than previous studies because this trial uniquely combined several key strengths, notably: strict randomisation; isolation of different elements (lifestyle advice, phenotypic risk information and genetic risk information); adequate power to detect clinically relevant effects on behavioural outcomes; concealment of group allocation from those assessing outcomes; objective assessment of behavioural outcomes as well as consideration of biological and psychological outcomes and low attrition rates. Furthermore, as there is evidence that different formats of risk communication can have a different impact on risk perception and risk accuracy, potential bias was avoided by presenting both the phenotypic and genetic risk information in the same format.
Previous systematic reviews have suggested that provision of risk information to practitioners may influence prescribing decisions and patients’ CVD risk factors.3 However, risk information needs to be accompanied by other tools in order to influence patients’ health-related behaviours.2 23 The INFORM trial accompanied the provision of risk information with web-based lifestyle advice, adapting an approach used in the Heart to Health trial.12 However, in contrast to the Heart to Health trial (which reported increases in objectively measured physical activity and self-reported diet at 4 months of follow-up7), the INFORM trial did not observe improvements in physical activity with lifestyle advice, either alone or in combination with risk estimates. In the INFORM trial, participants allocated to lifestyle advice reported increases in fruit and vegetable intake compared with those not allocated such advice, but the interpretation of these results remains uncertain, especially given the absence of concomitant changes in levels of serum carotenoids. The Heart to Health trial involved interventions (eg, a counsellor available to assist with the web-based programme during the first visit, use of a cookbook, pedometers and physical activity logs) not used in the INFORM trial and included only participants at moderate or high risk for CHD (≥10% 10-year risk for CHD)12, such differences might have accounted for the two trials’ differing results.
The INFORM trial adds importantly to the evidence that providing individuals with CHD risk information is unlikely to produce emotional harm.3 6 22 24 In particular, our data suggest that provision of either phenotypic or genetic CHD risk information did not influence overall stress or mood. We did find small increases in CHD-related worry between those who received either genetic or phenotypic risk estimates and control, with those receiving risk estimates having higher values at follow-up. However, this was not seen between those who received genetic or phenotypic risk estimates compared with those who received the lifestyle advice and given the effect size and its 95% CI we consider these results not to be important from a clinical point of view.
The most important potential limitation of our trial relates to its generalisability, since the participants were blood donors. It could be that the scope for lifestyle improvement was somewhat limited because blood donors in England are likely to have healthier lifestyles than the general population.25 We also do not have access to information about the characteristics of participants who did not respond to the study invitation. Next, we used plasma carotenoids as an objective measure of fruit and vegetable intake but other aspects of diet (eg, whole grain intake) were assessed using a self-report one item instrument. The average 10-year CHD risk, either based on phenotypic or genetic characteristics, was additionally relatively low in this sample, and therefore the received risk estimate may have been a disincentive to make lifestyle changes. However, we did not find an interaction between the baseline CHD risk and intervention group on our primary outcome. More importantly, on average there was no evidence of adoption of unhealthy behaviours among our participants receiving a potentially reassuringly low-risk estimate. Another potential limitation was the relatively short (12-week) duration of follow-up in our trial. However, a 12-week period is sufficient time for participants to initiate changes in health-related behaviours but does not reflect an immediate and unsustained reaction to the information. As EPIC-CVD (the study we used to estimate the coefficient for our genetic risk estimate) had only CHD end points available at the time of trial design, we used CHD (rather than a combination of CHD and stroke) as the outcome for modelling. However, the majority of genetic loci known to be associated with CVD are CHD loci. Next, although we included web-based lifestyle advice that has been shown to be effective in improving objectively measured physical activity and other CHD risk factors,7 we delivered the entire intervention via a website and did not include assistance from a counsellor as in this previous trial. Other studies reporting reductions in LDL cholesterol levels22 have also delivered face-to-face interventions and it is possible that an individual’s perception and understanding of their estimated risk is different when presented face-to-face. Future studies may consider comparing interventions that are clinic-based with practice support versus entirely web-based formats to compare their effect on health-related behaviours and other CHD risk factors. Additionally, the acceptability scores measured as part of INFORM trial were modest. These may be improved in future studies by greater engagement with end-users in the design and development of the intervention.26 Finally, even though participants who took part in qualitative interviews,15 viewed the lifestyle intervention as important in motivating them to adopt healthy behaviours, the adherence to the intervention ranged from, for example, 80.7% participants completing the first session on diet to 45.4% participants completing all three sessions. Challenges around engaging participants with online interventions are well described.27
Conclusion
We conclude that provision of risk information, whether based on phenotypic or genotypic characteristics, alongside web-based lifestyle advice had limited potential to improve behavioural and biological risk factors for CVD in the population we studied. However, we did not find evidence that communication of CHD risk information had clinically important adverse psychological consequences.
Key messages
What is already known on this subject?
Impact on behaviour of provision of cardiovascular disease risk information to individuals remains unclear as previous randomised studies have been constrained by modest power and/or use of imprecise measures that rely on participants’ self-report.
What might this study add?
Overcoming methodological limitations of previous studies, we have shown that providing phenotypic and genetic coronary heart disease risk information, alongside lifestyle advice, does not affect objectively measured levels of physical activity or fruit and vegetable intake, intermediate causal risk factors for cardiovascular disease or psychological outcomes.
How might this impact on clinical practice?
Based on our results, it is unlikely that simply informing individuals of their risk of developing coronary heart disease will motivate them to adapt recommended behaviours.
Achieving change in behaviour requires additional approaches.
Acknowledgments
Acknowledgments are reported in Online supplement (S6. Acknowledgments).
References
Footnotes
Contributors Study concept and design: BS, JAU-S, JL, RAP, GS, ZT, CM, AB, EDA, JD, SJG. Acquisition, analysis or interpretation of data: BS, SS, RAP, MW, SJG. Drafting of the manuscript: BS, SS, SJG. Critical revision of the manuscript for important intellectual content: BS, SS, JAU-S, JL, RAP, GS, SJG, KL, ZT, CM, MW, AB, EDA, JD, SJG. Obtained funding: JD, SJG. Administrative, technical or material support: BS, JL, RAP, GM, MW, JD, SJG. Study supervision: BS, JAU-S, JL, RAP, GS, ZT, CM, AB, EDA, SJG. SJG (principal investigator) and BS had full access to all the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis.
Funding This work was supported by a European Commission Framework 7 EPIC-CVD Grant agreement no: 279233. NHS Blood and Transplant funded the INTERVAL trial. DNA extraction and genotyping in INTERVAL/INFORM was funded by the National Institute for Health Research. The coordinating team for INTERVAL/INFORM at the Cardiovascular Epidemiology Unit of the University of Cambridge was supported by core funding from: UK Medical Research Council (G0800270), British Heart Foundation (SP/09/002), British Heart Foundation Cambridge Cardiovascular Centre of Excellence and UK National Institute for Health Research Cambridge Biomedical Research Centre. BS was supported by the Medical Research Council (MC_UU_12015/4). JD is a British Heart Foundation Professor, European Research Council Senior Investigator and National Institute of Health Research Senior Investigator. SJG is a National Institute of Health Research Senior Investigator and member of the NIHR School for Primary Care Research. The University of Cambridge has received salary support in respect of SJG from the NHS in the East of England through the Clinical Academic Reserve.
Disclaimer All authors declare no support from any organisation for the submitted work; no financial relationships with any organisations that might have an interest in the submitted work in the previous 3 years; no other relationships or activities that could appear to have influenced the submitted work.
Competing interests None declared.
Ethics approval Ethical approval was received from the National Research Ethics Service Committee East of England—Cambridge Central (14/EE/1164) on 3 December 2014.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Patient level data and statistical code are available from the corresponding author at ProfGP@medschl.cam.ac.uk.
Patient consent for publication Obtained.