Article Text

Abstract
Background The prevalence of obesity is increasing globally and this could partly explain the worldwide increase in the prevalence of atrial fibrillation (AF), as both overweight and obesity are established risk factors. However, the relationship between weight change and risk of incident AF, independent of starting weight, remains uncertain.
Methods MEDLINE, Embase, Pubmed, Web of Science, Cochrane Central Register of Controlled Trials, Database of Abstracts of Reviews of Effects, Trials Register—clinicaltrials.gov, CINAHL and the WHO ICTRP were searched from inception to July 2018.
We included randomised controlled trials and cohort studies across all healthcare settings but excluded studies of bariatric surgery. A random effects model was used to calculate pooled hazard ratios. The primary outcome was the risk of incident AF in relation to weight change.
Results Ten studies, including 108 996 people, met our inclusion criteria. For a 5% gain in weight, the incidence of AF increased by 13% (HR 1.13, 95% CI 1.04 to 1.23, I2=70%, n>20 411 in five studies; study size was unknown for one study). A 5% loss in body weight was not associated with a significant change in the incidence of AF (HR 1.04, 95% CI 0.94 to 1.16, I2=73%, n=40 704 in five studies).
Conclusions Weight gain may increase the risk of AF, but there was no clear evidence that non-surgical weight loss altered AF incidence. Strategies to prevent weight gain in the population may reduce the global burden of AF. Given the lack of studies and methodological limitations, further research is needed.
- Atrial Fibrillation
- Systemic Review
- Meta-analysis
- Obesity
- Global Disease Patterns
This is an open access article distributed in accordance with the Creative Commons Attribution 4.0 Unported (CC BY 4.0) license, which permits others to copy, redistribute, remix, transform and build upon this work for any purpose, provided the original work is properly cited, a link to the licence is given, and indication of whether changes were made. See: https://creativecommons.org/licenses/by/4.0/.
Statistics from Altmetric.com
Background
Atrial fibrillation (AF) is the most common sustained cardiac arrhythmia, affecting 33.5 million people worldwide.1 It is associated with a fivefold increased risk of embolic stroke, 50% increased risk of death in the 3 years following diagnosis and reduced quality of life.2–4 AF is also costly, accounting for 2% of healthcare expenditure in high-income countries.5
The prevalence of AF is rising and anticipated to double in Europe before 2060 due to an ageing population and increased prevalence of established risk factors including obesity, hypertension, diabetes and obstructive sleep apnoea.6 Three systematic reviews have demonstrated that obesity is associated with an increased risk of incident AF.7–9 The pathological mechanisms linking excess weight and AF are not fully understood but may be mediated by the metabolic syndrome and direct damage to the heart from excess adipose tissue. Overweight leads to an increase in epicardial adipose tissue, atrial enlargement and diastolic dysfunction, which can lead to atrial electrical remodelling and an increased risk of AF.10
In people diagnosed with AF, increasing body mass index (BMI) and pericardial fat volumes are associated with a higher symptom burden.11 12 Weight reduction and effective risk factor management in overweight individuals can reduce the frequency and duration of AF episodes and increase arrhythmia-free survival postablation.13 However, whether weight change alters the risk of developing AF is uncertain. The aim of this study was to assess the association between weight change and AF incidence and, if possible, determine whether the association was modified by baseline weight status.
Methods
The review was conducted following the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) guidelines (eAppendix 1). Our methods were prespecified in our study protocol, which is included in the online supplementary file (eMethods 1).
Supplementary file 1
Supplementary file 8
Search strategy
We searched nine electronic databases from inception to July 2018 (eMethods 2). One author (NJ) screened all the abstracts and titles, and two authors screened the full texts (NJ, PA and KT (in pairs)). We manually checked the references of the full-text papers to ensure literature saturation.
Supplementary file 2
Eligibility criteria
We included randomised controlled trials (RCTs) and cohort studies of weight change (measured by kg, BMI or percentage weight change) in adults who reported the incidence of paroxysmal, persistent or permanent AF as an outcome. There was no restriction by language or setting.
We excluded case–control studies, case reports and case series, as they could not assess the incidence of AF, and conference abstracts as they provided insufficient information to appraise the study. We excluded studies of bariatric surgery, as the rapid, large volume of weight loss along with nutritional and physiological differences induced by the surgery may not reflect the association between weight change and AF in the general population.
For each study, two authors (NJ and KT) independently extracted data, contacting authors as necessary.
Assessment of risk of bias and quality of the evidence
Two authors (NJ and KT) independently assessed the risk of bias using the Newcastle-Ottawa Scale (NOS) for non-randomised studies.14 Two authors (NJ and PA) independently assessed the risk of bias and strength of evidence across the studies, using the Grading of Recommendations Assessment, Development and Evaluation (GRADE) framework headings.15 A full GRADE assessment was precluded because not all studies reported the absolute number of people with incident AF in each weight change category. For each assessment, disagreements were discussed and resolved.
Data analysis and synthesis
We log-transformed the reported HRs across the weight change categories and calculated study-specific slopes (linear trends) using the method of Greenland and Longnecker and the Stata glst command of Orsini et al.16 17 Where possible, we undertook random effects meta-analysis based on the DerSimonian and Laird method to compute the summary HRs with 95% CIs of incident AF.18 We assessed statistical heterogeneity using the I-squared statistic and calculated approximate 95% prediction intervals to estimate the likely effect in an individual setting using the methods of Higgins et al.19 20 Where there were insufficient data to pool, we report results descriptively.
We could not carry out our prespecified subgroup analyses (by intentionality of weight loss, initial weight, comorbidity and gender) and instead, we subgrouped by population type and duration of follow-up in a post hoc analysis. We assessed whether the results were sensitive to the choice of model, quality of the studies, whether data were estimated from the presented results and the heterogeneity of the patient populations. To do so, with separate analyses, we carried out fixed-effects analysis and excluded individual studies, studies with poor quality data and those for which we estimated data. There were insufficient data to carry out meta-regression or assess publication bias (exploratory contour plots are included in the online supplementary file (eMethods 3). All analyses were carried out using Stata V.14.2.
Results
Study characteristics
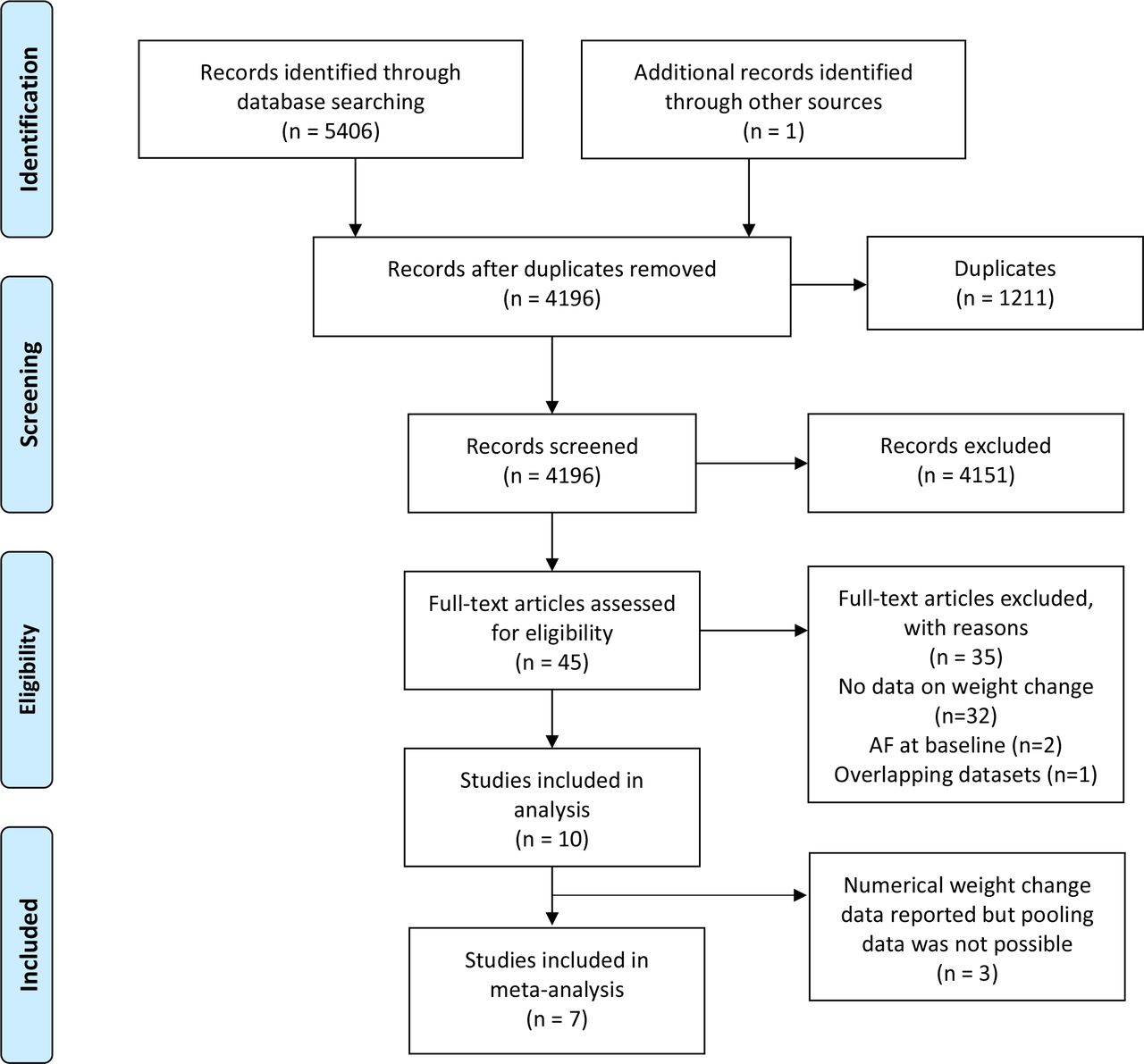
From 5407 records, we screened 45 full texts, of which 10 met the eligibility criteria (figure 1). Nine were cohort studies (table 1). In the single RCT, Alonso et al randomised participants with type 2 diabetes (T2DM) to an intensive weight loss intervention or a diabetes support and education programme.21 We included the combined data for these two groups, reported in a multivariate analysis adjusted for a range of important covariates including age, blood pressure and intervention arm (eTable 1).
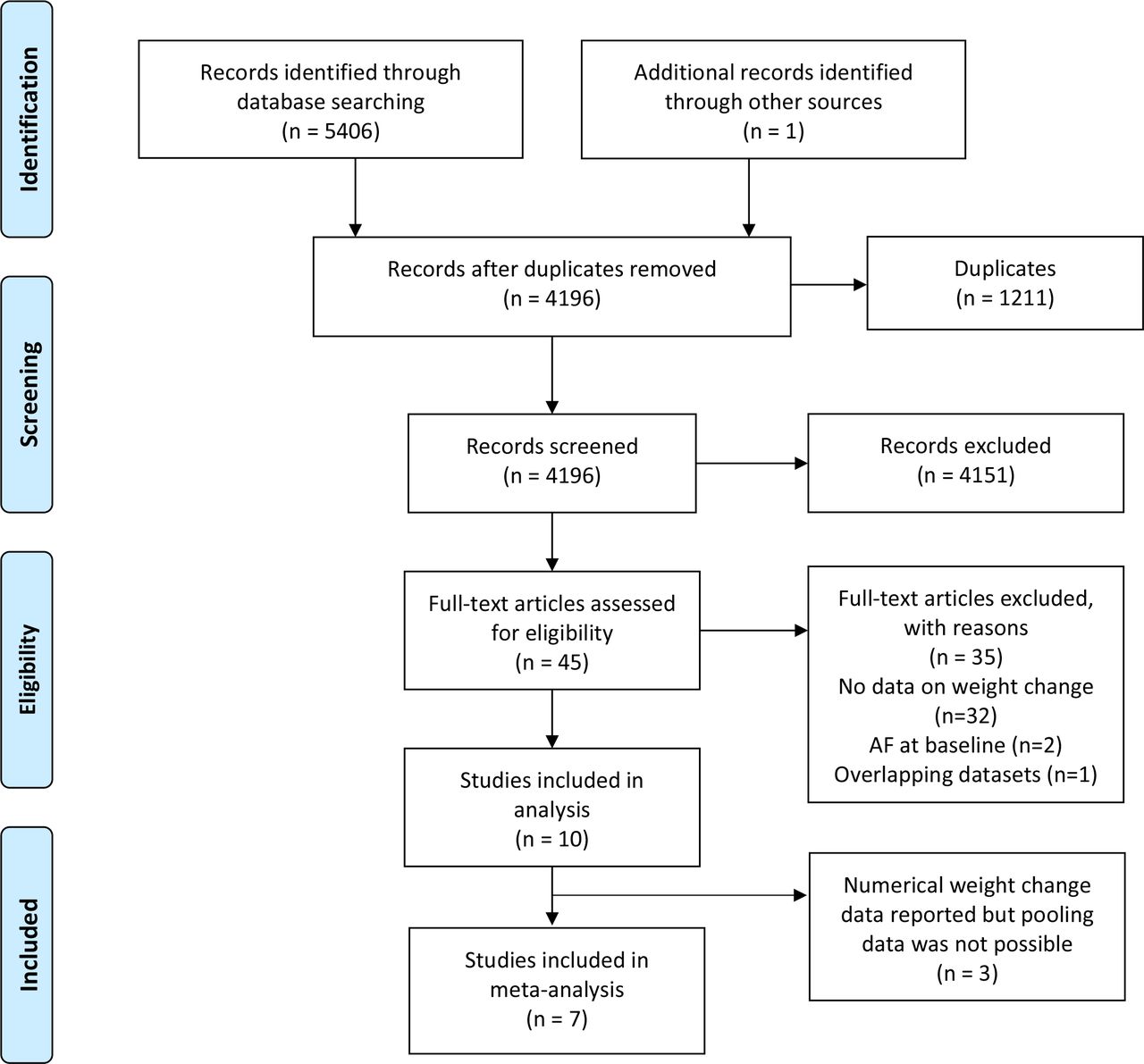
Preferred Reporting Items for Systematic Reviews and Meta-analyses flow diagram of study selection. AF, atrial fibrillation.
Characteristics of participants in the included studies
In general, participants were middle-aged people attending routine health checks, but in two studies all participants had T2DM.21 22 AF incidence rates were higher in studies of people with diabetes or cardiovascular risk factors compared with population surveys of healthy people (table 1). In four studies, most participants had a healthy weight at baseline,23–26 whereas in six most were overweight or obese. Only the RCT of the weight loss programme assessed whether participants intended to lose weight.21 Follow-up varied between 4.6 and 35 years. Six studies reported the incidence of AF during follow-up after the period of measured weight change, whereas four reported the association between weight change and AF incidence across the same period (table 2). Nine studies used linked electronic health records to capture incident cases of AF (table 1). In four studies, this was triangulated with ECGs at study follow-up visits. One study relied on a single follow-up visit ECG to capture incident cases.27 In one study, AF was detected by 7 day Holter monitoring.28
Follow-up methods, including weight assessments and AF case definition
Weight gain and risk of incident AF
Percentage weight gain
Pooled analysis from six populations (five studies) showed that for a 5% gain in weight, the incidence of AF increased by 13% (HR 1.13, 95% CI 1.04 to 1.23, with 95% prediction interval 0.88 to 1.44) (figure 2), with moderately high statistical heterogeneity. Excluding the study by Rosengren et al reduced the I2 statistic from 70% to 33%.29 Most participants were overweight or obese at the outset in five of the six populations.

Risk of 5% weight gain on incidence of atrial fibrillation.
Sensitivity analysis generally produced consistent results (eTable 2). Outcome data were converted to percentage weight gain for two studies included in the pooled analysis.22 23 Excluding these studies did not change the point estimate for incident AF but the result was no longer statistically significant (eTable 2). In both studies of general populations and in the single study of a population with T2DM,22 a 5% gain in weight was associated with a significant risk of AF, and the same result applied for both studies with follow-up less than and greater than 10 years (eTable 2).
Other measures of weight gain
Several studies reported weight gain in continuous or categorical terms by kg or BMI gained. Where possible, these results were converted and pooled.22 23 We were unable to pool data from three studies.24–26 Johnson et al reported the association between an annual increase in weight measured by kg in the first 6 years of follow-up and incidence of AF in the subsequent years of follow-up (mean 22.3 years).25 In this study the incidence of AF increased by 14% (HR 1.14, 95% CI 1.05 to 1.24) for a 1 kg gain per annum. Ball et al reported the association between weight gain and risk of AF by change in BMI category.26 A 4 kg/m2 increase in BMI was associated with a 35% increased risk of AF in men (HR 1.35, 95% CI 1.18 to 1.54) and 23% in women (HR 1.23, 95% CI 1.07 to 1.41).26 Tedrow et al reported a 41% higher risk for women who became obese compared with those who did not (HR 1.41, 95% CI 1.05 to 1.90).24
Weight gain by baseline weight
Two studies presented subgroup analyses by baseline weight. Grundvold et al reported weight gain in those who were obese at baseline was associated with a similar increase in risk of AF compared with the whole population (obese subgroup HR 1.59, 95% CI 1.02 to 2.47, whole population HR 1.53, 95% CI 1.10 to 2.12).22 Johnson et al reported weight gain of 1 kg per annum resulted in a similar increased risk of AF in people with healthy weight (BMI<25 kg/m2) compared with the whole study population (healthy BMI subgroup HR 1.13, 95% CI 0.99 to 1.30, whole population HR 1.12, 95% CI 1.03 to 1.23).25
Weight loss and risk of incident AF
Percentage weight loss
In the RCT, the intervention group achieved a mean percentage weight loss of 6.0%, compared with 3.5% in the control group, and the HR for the onset of AF was 0.99 (95%CI 0.77 to 1.28).21 As results were reported by trial arm, those who did not lose weight were included in the analysis and therefore the results may underestimate any association between weight loss and AF.
In a pooled analysis from seven populations (five studies), there was no statistically significant association between 5% weight loss and incidence of AF (HR 1.04, 95% CI 0.94 to 1.30 with a prediction interval 0.77 to 1.42) (figure 3). In all the studies, most participants were overweight or obese at baseline. Grundvold et al reported no significant difference in risk of AF between those who were obese at baseline and lost weight compared with the whole population in the only such subgroup analysis.22

{kind=link}
{kind=link}
{kind=link}
Risk of 5% weight loss on incidence of atrial fibrillation.
There was high statistical heterogeneity (I2=73%). Excluding the study by Huxley et al 30 dropped the I2 to 0% and resulted in a minor but significant reduction in incidence of AF (HR 0.95, 95% CI 0.90 to 0.99) (eTable 3). In both studies of general populations and in the single study of a population with T2DM, there was no significant association between weight loss and AF. In studies with follow-up less than 10 years, there was a significant reduction in risk of AF and in the study populations with follow-up more than 10 years, there was a significant increase in risk (eTable 3).
Rosengren et al found no evidence that losing more than 4% body weight from age 20 years to midlife was associated with a significant change in the incidence of AF compared with individuals whose weight only changed by between −4% and 4% in the same period (HR 1.00, 95% CI 0.72 to 1.27).29 These results could not be pooled.
Other measures of weight loss
Ball et al reported a reduction in BMI of 2 kg/m2 was associated with a 18% decrease in risk of AF in men (HR 0.82, 95% CI 0.75 to 0.90) and 19% in women (HR 0.81, 95% CI 0.71 to 0.94), compared with people whose BMI increased by 1 kg/m2.26 Tedrow et al reported that women who were obese at baseline but lost weight to reduce their BMI below 30 kg/m2 no longer had an elevated risk of AF compared with people who were never obese (HR 1.01, 95% CI 0.58 to 1.79).24
Amount of weight loss and risk of AF
Four studies reported the impact of degrees of weight loss on the risk of AF, but the results were inconclusive.21 27 30 Alonso et al and Diouf et al both reported no significant association between weight loss and AF across all reported ranges of weight loss.21 27 Ball et al reported a non-significant trend towards a decrease in the risk of incident AF for people whose BMI decreased by up to 2 kg/m2 compared with those who gained 1 kg/m2.26 Huxley et al reported a significant increase in incident AF in those who lost more than 5% of their weight and suggested that conditions associated with muscle wasting, which will lead to unintentional weight loss, may explain their finding.30
Quality assessment
The NOS scores ranged from 5 to 7 reflecting a moderate to low risk of bias (table 3). Based on the GRADE framework, there was moderate certainty in the 5% weight gain summary finding and very low certainty in the summary estimate of 5% weight loss. Further details of the quality assessments are included online (eResults).
Risk of bias measured by the Newcastle-Ottawa Scale
Discussion
Main findings
Weight gain was associated with an increased risk of AF in our pooled and unpooled analyses. Weight loss was not associated with an altered risk of incident AF in our pooled analysis. One unpooled study reported a significant association between weight loss and reduced AF incidence, another showed no association, and a third showed that those who dropped weight below the obesity threshold were no longer at an elevated risk of AF.24 26 29 In both pooled analyses, the majority of people were overweight or obese at baseline, although there were significant numbers of people with a normal BMI in most studies. Both results had high heterogeneity. There was moderate certainty in the weight gain summary finding, but only very low certainty in the weight loss finding.
Comparison with other studies
Our results suggest that weight gain itself in addition to BMI status may be linked to future risk of AF. Three systematic reviews have showed that obesity increases the risk of incident AF.7–9 One also analysed weight gain and AF, reporting no significant association between a 5% increase in bodyweight and AF incidence, based on two studies (relative risk of AF 1.08, 95% CI 0.97 to 1.19).7 Our review expands on this result, adding three further studies in the pooled analysis.
Strengths
This is the first systematic review to assess the risk of incident AF in relation to weight loss and extends our understanding of the association between weight gain and AF risk. We analysed data from 108 996 people across 10 individual studies, including seven in the pooled analyses. Most studies were conducted within the past 10 years across a range of economically developed countries and recruited middle-aged participants with a relatively low burden of comorbidity, providing contemporary, generalisable results.
Limitations
Pooling data from people who were healthy weight with those who were obese or overweight at baseline may have diluted the summary estimates and thus underestimate the effect of weight loss on the subsequent risk of AF. Most studies had significant numbers of people who had a normal BMI at baseline and there were insufficient data to perform the planned subgroup analysis by baseline weight. The weight gain studies which did split by baseline weight status reported very similar estimates of AF risk across groups. Some studies reported AF incidence during follow-up after the period when weight change was measured and it is possible that further weight change may have occurred that altered the subsequent risk of AF. There was inconsistency in the results of our analysis of weight loss measured by percentage change and change in BMI, and we were unable to summarise the overall effect as it was not possible to pool all these data. Studies presented data differently, which we sought to overcome by making conservative approximations to convert data into a common form to enable pooling from more studies.
Some studies relied on periodic ECG assessments, which may miss cases of paroxysmal AF and so underestimate true incidence, but this is unlikely to have biased differences by weight change status. Many studies attempted to triangulate their case detection with other electronic health records. Two studies calculated weight change using a recalled weight as the baseline measure, but these results were consistent with other studies.29
Nine of our 10 studies were observational. We included results from multivariate analyses but relevant covariates such as physical activity and history of cardiovascular disease were sometimes excluded.
Policy implications
Weight gain of 5% was associated with an increase in the risk of AF of 13% (95% CI 4% to 23%), with the likely effect in an individual setting varying between 18% reduction and a 44% increase in risk. Our results suggest that the risk of incident AF continues to rise in relation to weight gain across all categories of weight status. This evidence supports public health interventions that promote maintaining a healthy weight and preventing weight gain to reduce the burden of AF. Given the paucity of data and high heterogeneity, our conclusions are only tentative.
Whether intentional weight loss can reduce the risk of developing AF remains uncertain and may be related to the amount of weight people lose.31 Large amounts of weight loss achieved through bariatric surgery has been reported to reduce the risk of AF by 29% compared with no weight change (HR 0.71, 95% CI 0.60 to 0.83) over long-term follow-up.32
Unintentional weight loss may occur as a result of diseases that are independent risk factors for AF, such as cancer, hyperthyroidism or muscle wasting conditions as suggested by one of the included studies, which reported weight loss being associated with a significant increased risk of developing AF.30
Future research
Obesity is the second highest population attributable risk factor for incident AF behind hypertension, accounting for over 10% of all cases.33 The link between obesity and incident AF has been established, but more research is needed to understand the degree of increased risk associated with weight gain, whether non-surgical weight loss can reduce the risk of incident AF and if this depends on baseline weight status, intentionality and amount of weight loss.
Conclusion
Gaining weight increases the risk of incident AF, but the evidence is uncertain whether relatively small amounts of non-surgical weight loss reduces that risk. Interventions that help prevent weight gain in both individuals and populations, even in those already overweight, may reduce the growing global burden of AF and related healthcare costs.
Key messages
What is already known on this subject?
While there is an established association between obesity and an increase in the incidence of atrial fibrillation (AF), the relationship between weight change and the risk of AF is unclear.
What might this study add?
In this systematic review and meta-analysis of over 100 000 people, we found weight gain was associated with an increase in the incidence of AF, but no consistent association between non-surgical weight loss and altered incidence of AF.
How might this impact on clinical practice?
Preventing weight gain could be an important strategy in reducing the global burden of AF.
Acknowledgments
We thank Nia Roberts for her help with setting the search strategy.
References
Footnotes
Contributors NJ and PA conceived the original idea for the study. NJ created the search strategy. NJ, PA and KT screened and selected the studies. KT and NJ extracted all data in duplicate and KT led on the data analysis. CT provided input on the background literature and was involved in the critical revision of the manuscript. All authors were involved in drafting the final manuscript.
Funding NJ is a general practitioner and Wellcome Trust Doctoral Research Fellow in Primary Care (grant number 203921/Z/16/Z). KT is a medical statistician who receives funding from the NIHR Programme for Applied Research (RP-PG-1210-12003). CT is an academic clinical lecturer, funded by the National Institute for Health Research (NIHR). PA is an NIHR senior investigator and is funded by the NIHR Oxford Biomedical Research Centre (BRC) and Collaboration for Leadership in Health Research Care (CLAHRC). The project was supported by the NIHR CLAHRC Oxford. The views expressed are those of the authors and do not necessarily reflect those of the NIHR, NHS or Department of Health.
Competing interests CT reports speaker fees from Vifor and Novartis and non-financial support from Roche outside the submitted work. The other authors declare that they have no competing interests.
Provenance and peer review Not commissioned; externally peer reviewed.