Article Text

Abstract
Objective Contemporary data on patients with previously undiagnosed severe aortic stenosis (AS) are scarce. We aimed to address this gap by gathering data from consecutive patients diagnosed with severe AS on echocardiography.
Methods This was a prospective, multicentre, multinational, registry in 23 tertiary care hospitals across 9 European countries. Patients with a diagnosis of severe AS were included using echocardiography (aortic valve area (AVA) <1 cm2, indexed AVA <0.6 cm2/m2, maximum jet-velocity (Vmax) >4 m/s and/or mean transvalvular gradient >40 mm Hg).
Results The 2171 participants had a mean age of 77.9 years and 48.0% were female. The mean AVA was 0.73 cm2, Vmax4.3 m/s and mean gradient 47.1 mm Hg; 62.1% had left ventricular hypertrophy and 27.3% an ejection fraction (EF) <50%. 1743 patients (80.3%) were symptomatic (shortness-of-breath 91.0%; dizziness 30.2%, chest pain 28.9%). Patients had a EuroSCORE II of 4.0; 25.3% had a creatinine clearance <50 mL/min, and 3.2% had an EF <30%. Symptomatic patients were older and had more comorbidities than asymptomatic patients. Despite European Society of Cardiology 2017 valvular heart disease guideline class I recommendation, in only 76.2% a decision was made for an intervention (transcatheter 50.4%, surgical aortic valve replacement 25.8%). In asymptomatic patients, 57.7% with a class I/IIa indication were scheduled for a procedure, while 36.3% patients without an indication had their valve replaced.
Conclusions The majority of patients with severe AS presented at an advanced disease stage. Management of severe AS remained suboptimal in a significant proportion of contemporary patients with severe AS.
Trial registration number NCT02241447;Results.
- aortic stenosis
- transcatheter aortic valve replacement
- surgical aortic valve replacement
- symptoms
Statistics from Altmetric.com
Introduction
Aortic stenosis (AS) is a progressive disease that is increasing in prevalence as the global population ages.1 The rate at which the condition progresses varies widely between patients,2 with many remaining symptom-free for several years. Once symptoms develop, the prognosis is poor, and timely treatment is essential for improving survival.3 4
There are now several options for treating patients with severe symptomatic AS, namely surgical aortic valve replacement (SAVR) and transcatheter aortic valve replacement (TAVR). The latter was developed as an alternative treatment for patients with multiple comorbidities or a level of frailty that puts them at too high a risk for SAVR.5 6 Thus, most patients with severe symptomatic AS now have, at least theoretically, one option involving valve replacement.
Patient and disease characteristics of patients with severe AS have been recorded as part of the Euro Heart Survey (EHS; 2001), the Dutch Aortic VAlve RIJNmond (AVARIJN) study (2006–2009), and the Japanese Contemporary outcomes after sURgery and medical tREatmeNT in patients with severe Aortic Stenosis (CURRENT) AS (2003–2011).7–10 In the years since these studies were performed, however, there have been significant changes in the approach to diagnosis and management of AS, with the introduction of TAVR the most noteworthy. Therefore, there is a need for contemporary data regarding this patient population.
The aim of the Study to Improve Outcomes in Aortic Stenosis (IMPULSE) registry was to collect data from consecutive patients diagnosed with severe AS on echocardiography with or without being symptomatic in tertiary hospitals throughout Europe. The present article describes the characteristics of these patients, including their comorbidities, the functional and morphological details of their AS, and their subsequent treatment decisions, discusses these on the background of recent guideline recommendations and compares them to the prior data evidence available.
Methods
Study design and site selection
IMPULSE is a prospective, multinational registry of patients with AS in Europe, the rationale and design of which has been described.11 In short, a total of 23 centres from 9 countries (Austria, Czech Republic, France, Germany, Italy, the Netherlands, Spain, Switzerland and the UK) were involved in the present study. All study sites offered the full range of treatment options for AS, including surgical and transcatheter procedures. The study was carried out in accordance with the Declaration of Helsinki and was approved by the independent ethics review boards at each participating institution.
Patients
Patients over 18 years of age who had an echocardiogram at one of the participating centres that diagnosed severe AS, either symptomatic or asymptomatic, were consecutively included in the registry. A diagnosis of severe AS was defined as one or more of the following findings: an aortic valve area (AVA) of <1 cm2, an indexed AVA of <0.6 cm2/m2, a maximum jet velocity (Vmax) of >4 m/s or a mean transvalvular gradient of >40 mm Hg.4 11 Patients were excluded if they had previously undergone an aortic valve replacement procedure. Enrolment took place between March 2015 and April 2017.
Documentation
Data were collected by a dedicated study nurse using a standardised electronic case report form. Demographic characteristics were documented for each patient, along with a full medical history. Symptoms that could be attributed to AS were recorded, including chest pain, shortness of breath and dizziness on exertion/syncope. Patients were defined as ‘symptomatic’ if they presented with either chest pain, shortness of breath and/or dizziness on exertion/syncope. Severe symptoms were defined as Canadian Cardiovascular Society (CCS) class III or IV angina, New York Heart Association (NYHA) functional class III or IV and/or dizziness on exertion/syncope. The logistic EuroSCORE I and the EuroSCORE II were calculated based on comorbidities and other characteristics of the patient. Frailty was assessed according to the ability of the patient to walk 5 m in <6 s and to perform activities of daily living (ADL).12 ADL and life expectancy were assessed by the dedicated nurses or physicians. The results of echocardiographic assessment were also recorded, including the presence of coexisting aortic regurgitation, mitral or tricuspid valve disease, transvalvular gradient, left ventricle dimensions and left ventricular ejection fraction (LVEF). Finally, treatment decisions (TAVR, SAVR, medical management, watchful waiting) within 3 months were documented. Treatment decision relied on standard operating procedures in place at each centre.
For the appropriateness of the intervention, we referred to the 2017 ESC guidelines on valvular heart disease although they became into effect after completion of the study. This is because we aimed to reflect the appropriateness based on current knowledge. Principal differences compared with the 2012 guidelines are the class II recommendation being assigned to symptomatic patients with low-flow, low-gradient AS, a reduced LVEF and no flow reserve, and those with a paradoxical low-flow, low-gradient AS. Asymptomatic patients have an indication for AVR if Vmax >5.5 m/s and/or LVEF <50% in the 2012 guidelines with pulmonary artery pressure systolic (PASP) >60 mm Hg being added in the 2017 guidelines.
Statistics
Data are given as means with SD, medians with IQR, or absolute values with percentages. Comparisons between symptomatic and asymptomatic patient groups were made using a Pearson’s χ2 or Fisher’s exact test for categorical variables, and a t-test or Mann-Whitney-Wilcoxon rank sum test for continuous variables.
A p value of <0.05 was considered statistically significant. Statistical analysis was performed using SPSS V.23.0.
Results
Centre and patient characteristics
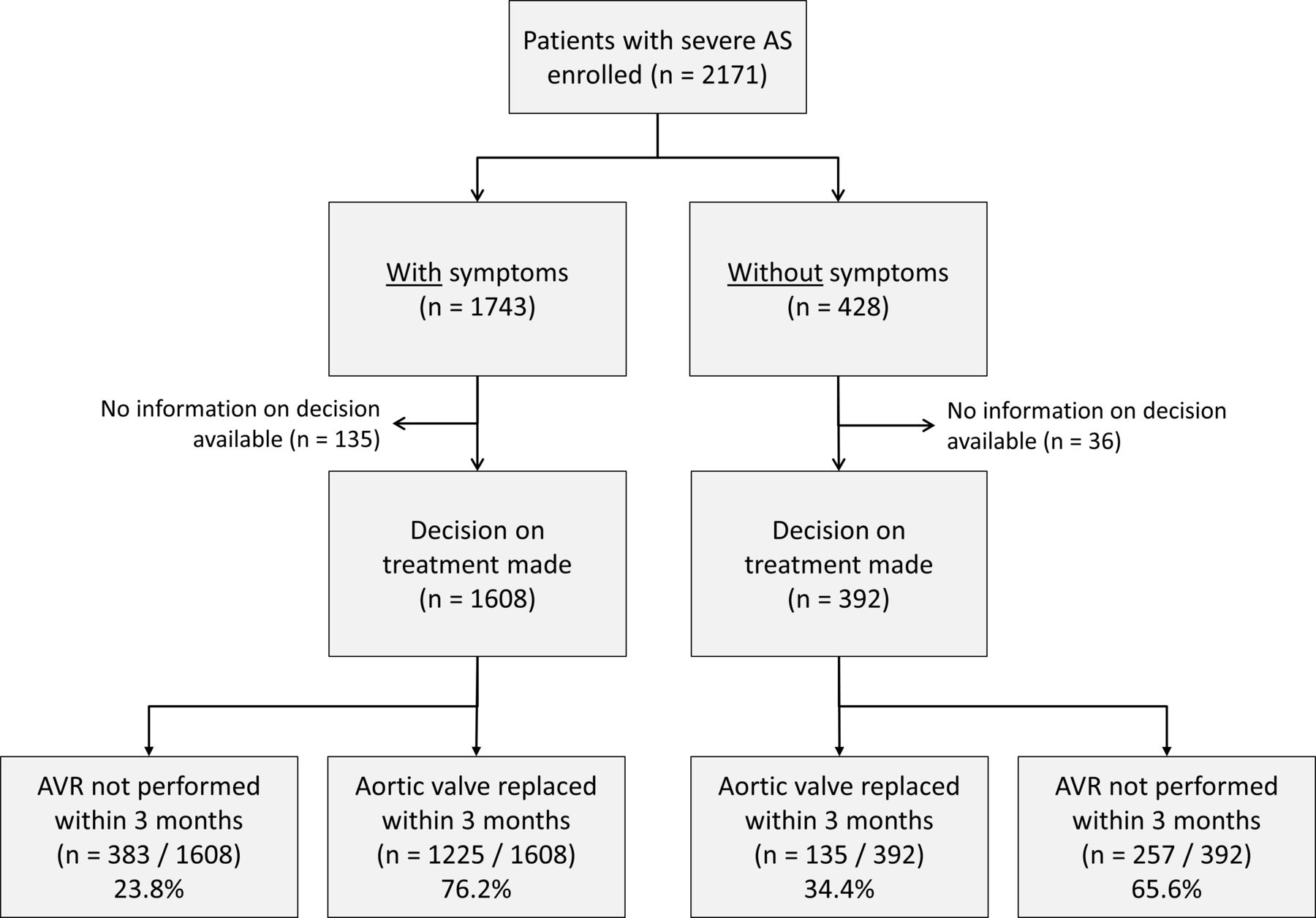
A total of 2171 patients were enrolled from 23 centres across Europe (figure 1). The centres varied in terms of their size and numbers of AS patients treated per year (online supplementary table 1). Overall, the median number of beds per hospital was 1000 (IQR: 553; 1200) and the median number of severe AS patients treated was 225 (IQR: 130; 418) per year. All centres performed both TAVR and SAVR, at median rates of 76 (IQR: 59; 176) and 136 (IQR: 62; 249) procedures per year, respectively. The cardiology departments had a median of 68 (IQR: 37; 112) beds, 20 (IQR: 15; 32) cardiologists and the hospitals 9 (IQR: 6; 15) cardiac surgeons. The mean age of the 2171 patients with severe AS that were enrolled in the IMPULSE registry was 77.9±10.0 years and 48.0% were female (table 1).
Supplemental material
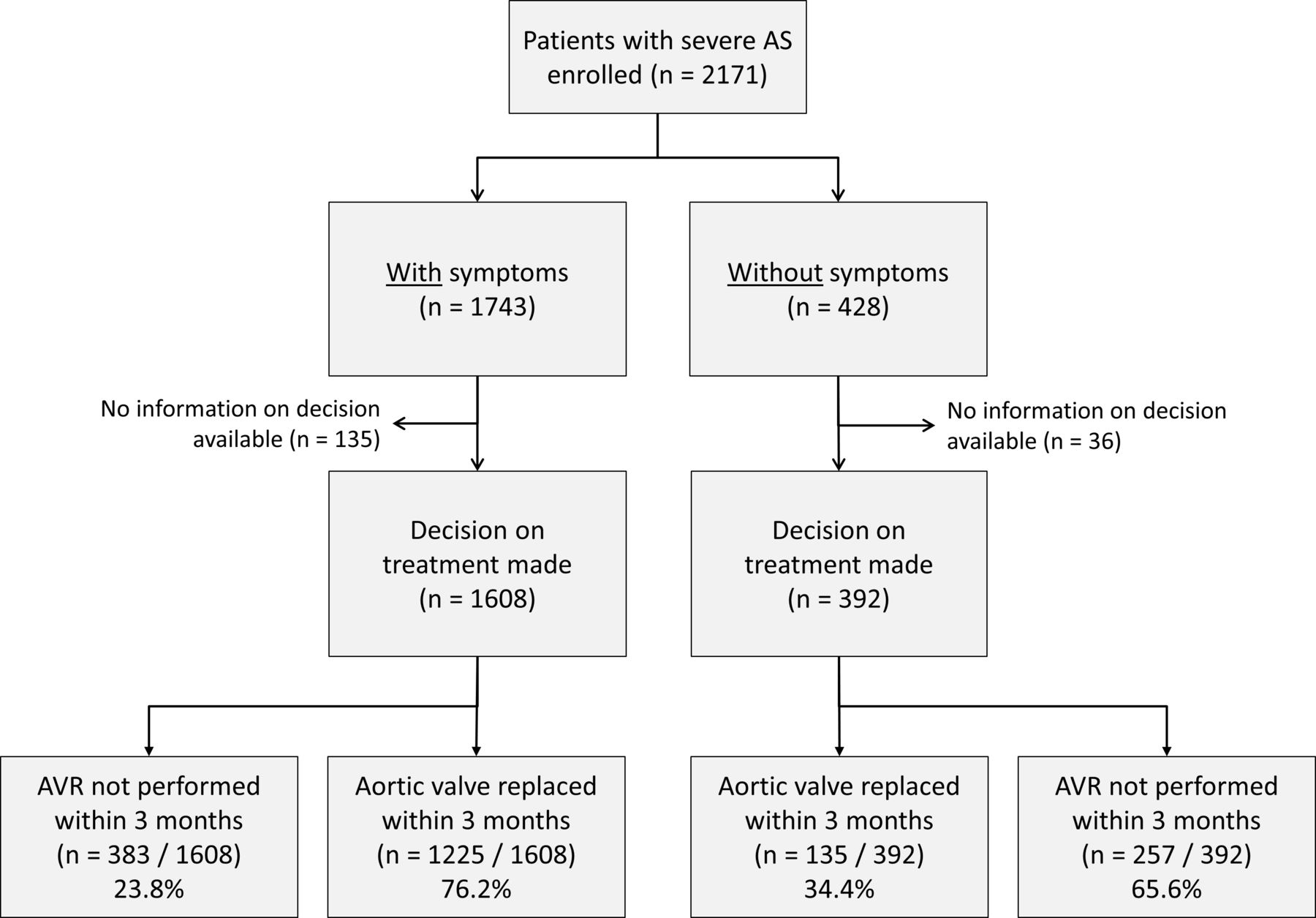
Flowchart of the population and management according to functional status. AS, aortic stenosis; AVR, aortic valve replacement.
Patient characteristics and echocardiography findings
Echocardiography findings
The mean AVA was calculated to be 0.73±0.19 cm2, with a value of 0.40±0.11 cm2/m2 when indexed to body surface area (table 1). The mean values for Vmax and mean aortic gradient were 4.3±0.7 m/s and 47.1±14.7 mm Hg, respectively. Grade III or IV aortic regurgitation was found in 8.1% of patients, grade III or IV mitral regurgitation in 10.7% and grade III or IV tricuspid regurgitation in 7.9%. While the mean values for left ventricle diameter were not elevated (47.0 and 31.6 mm for end-diastole and end-systole, respectively), a high proportion of patients were diagnosed with left ventricular hypertrophy (LVH; 62.1%). LV systolic dysfunction was common with 27.3% of the population presenting with a LVEF <50% including 3.2% displaying a value of <30%.
Clinical symptoms
Overall, 1743 (80.3%) of the 2171 patients with severe AS were classified as being symptomatic (figure 1). The most common AS-related symptoms displayed by these patients was shortness of breath (91.0%); 40.1% of the 1743 patients were being classified as being NYHA class III or IV by the physician. Dizziness on exertion or syncope was reported by 30.2% of patients; dizziness as the sole symptoms was very rare (2.1%). Chest pain was reported by 28.9% with a subset being considered CCS class III or IV (6.0% of all symptomatic patients).
Comorbidities
A total of 15.9% of the population had atrial fibrillation, while 7.2% had previously undergone cardiac surgery. Chronic lung disease and pulmonary hypertension (pulmonary artery pressure (PAP) systolic >55 mm Hg) were also commonly found, at rates of 11.4% and 10.8%, respectively. Approximately a quarter (25.3%) of patients suffered from severe renal impairment, while 2.0% were on dialysis. 32.3% presented with one comorbidity and 20.7% with two or more. In terms of frailty, 32.0% of patients were considered mildly frail and 5.1% severely frail. Mean EuroSCOREs I and II were calculated to be 15.6%±13.9% and 4.0%±5.0%, respectively.
Patients who were symptomatic were, on average, older and more often had atrial fibrillation, previous cardiac surgery, pulmonary hypertension, chronic lung disease or severe renal impairment (table 1). More of the symptomatic patients were frail (41.2%) than of the asymptomatic (20.2%) (p<0.001). The EuroSCORE II also differed significantly, with much higher values found for the symptomatic than for the asymptomatic patients (4.5±5.4 vs 2.1±2.1; p<0.001). Symptom status was not related to differences in measures of AS severity, ventricular size or function, except for a slightly smaller mean AVA for the symptomatic patients compared with the asymptomatic (0.72 vs 0.78 cm2; p<0.001) (table 1). Both significant mitral and tricuspid regurgitation were more common in the symptomatic group than in the asymptomatic. Although there was a statistical difference in the numbers with severe LV dysfunction according to symptom status, the numbers overall with an LVEF <30% were small—found only in 3.6% of the symptomatic patients and 1.5% of the asymptomatic patients.
Treatment decisions
All the 1743 symptomatic patients had an indication for valve replacement based on the 2017 European Society of Cardiology/European Association for Cardio-Thoracic Surgery (ESC/EACTS) guideline; in 135 of those no treatment decision was made. Of the remaining 1608 patients, 383 (23.8%) were denied such an intervention. TAVR was considered in 810 (50.4%) and SAVR in 415 patients (25.8%). Symptomatic patients who were denied any intervention were older (p<0.001) and presented more often with comorbidities such as chronic lung disease or renal insufficiency and overall high surgical risk scores (table 2). Excluding patients with a life expectancy <2 years and/or severe frailty (74 patients), and/or with discordant grading (valve area <1 cm2 and mean pressure gradient <40 mm Hg, 88 patients) further reduced this number to 221 or 12.7% of patients which were left untreated despite a clear indication.
Patient with unusual treatment decisions for whom decision was collected (171 missing patients)
Of 428 patients without symptoms, in 36 no decision on treatment decision was made. Of those with a decision (n=392), 88 patients were scheduled for TAVR (22.4%), while 65 patients were scheduled for SAVR (16.6%) (table 2). A total of 52/391 patients (13.3%) either had a class I (LVEF <50%) or a class IIa indication (Vmax >5.5 m/s, PAPsys >60 mm Hg) for valve replacement based on the 2017 ESC/EACTS guideline (figure 2). On the one hand, out of 52 patients with class I or class IIa indication, 30 (57.7%) were considered for TAVR (22 patients) or SAVR (8 patients), with the remaining (22 patients) not being intervened. On the other hand, 339/391 patients had no class I or class II indication, but 123 patients were scheduled for an intervention with TAVR chosen in 66 patients and SAVR in 57 patients.

{kind=link}
{kind=link}
Treatment decisions in asymptomatic patients based on the 2017 ESC/EACTS guidelines. *Class I/class II indication: LVEF <50% (other causes of LV dysfunction could not be excluded), Vmax >5.5 m/s or PAPsys >60 mm Hg based on the 2017 ESC/EACTS guidelines.4 Green colour indicates a guideline compliant decision while red colour indicates a non-compliant treatment decision. AV, aortic stenosis; LV, left ventricular; LVEF, l eft ventricular ejection fraction; SAVR, surgical aortic valve replacement; TAVR, transcatheter aortic valve replacement.
Discussion
In this large prospective multicentre registry (IMPULSE) based on 2171 patients with severe AS, we observed that symptomatic patients are still referred late in the course of the disease with severe symptoms and or LV dysfunction already present. Despite the availability of TAVR and clear guideline recommendations for the treatment of these patients, >20% of symptomatic patients are denied an intervention and conservative treatment pursued instead. On the other hand, more than a third of asymptomatic patients are referred for an intervention in the absence of class I or class IIa indications and TAVR was preferred over SAVR in these cases. Taken together, despite significant improvements, management of severe AS remained suboptimal in a significant proportion of contemporary patients with severe AS.
Contemporary patients
The average age of the patients enrolled in IMPULSE (77.9 years) (table 3) was much higher than that of the EHS cohort (69 years),7 and slightly higher than that of the AS patients in the Dutch AVARIJN study (72.6 years), which was conducted from 2006 to 2009.10 This may indicate that European patients are developing severe AS at an older age than they were 15 years ago and/or that with the availability of TAVR more patients are referred to tertiary centre, although we cannot exclude that the different setting with only tertiary hospitals in IMPULSE versus inclusion of single practice/private practices in the EHS cohort may explain some of the observed differences. Nevertheless, these findings may have major public policy implications. Although a direct comparison cannot be made with the published data from the EHS, the left ventricle dimensions, AVA and transvalvular gradient values did not vary greatly from those in the present study.13 The mean values for LVEF for the two studies were also similar, as were the proportions of patients with an LVEF of <30%. While different comorbidities were recorded in the EHS and IMPULSE registry, current patients present with multiple comorbidities in addition to AS. Severe renal impairment and atrial fibrillation were particularly common in the IMPULSE cohort. A similar finding was reported for the Japanese CURRENT AS study, which was performed between 2003 and 2011.9
Comparison of characteristics of patients with severe aortic stenosis in prior research projects
Delayed diagnosis
As found in the EHS over 15 years ago,13 the IMPULSE registry demonstrates that a substantial part of patients in Europe are currently referred late in the course of the disease. Given that well over a third have advanced symptoms by the time they present, consideration should be given to improve screening and increase awareness to diagnose the condition before patients reach a critical stage. The data collected for the IMPULSE registry show that symptomatic patients were older than those without symptoms, which was also found in the EHS and the AVARIJN study.10 13 It is not known whether this older age reflects reluctance on the part of the patient to complain or on the part of the primary care physician to refer the patient. Higher proportions of the symptomatic patients also displayed both greater comorbidity and frailty, which increase the risk of a poor outcome from intervention. Therefore, strategies for achieving earlier diagnosis of AS need to be investigated, especially in the context of ongoing clinical trials that assess ‘prophylactic’ TAVR in asymptomatic patients with severe AS (EARLY TAVR; clinicaltrials.gov NCT03042104).
Treatment decisions and guideline recommendations
Almost a quarter of symptomatic AS patients were still denied any intervention, even though all the patients in this study were diagnosed at tertiary hospitals capable of delivering all forms of intervention for severe AS, including TAVR and SAVR. It is not known whether the rate of non-intervention would be even higher in smaller hospitals without such access, but it is highly plausible. Although part of symptomatic patients with low flow AS do not present a true severe AS and thus do not have a class I indication for valve replacement, our findings remained unchanged excluding patients with discordant grading (valve area <1 cm2 and pressure gradient <40 mm Hg) which includes those with low flow. For the symptomatic patients who were referred for an intervention, TAVR was considered in almost double the number of patients compared with SAVR, which reflects the older age and high comorbidity burden of this population. Nevertheless, it is surprising that the fraction of symptomatic patients denied therapy remains high, even in the era of TAVR. Thus, despite the development of TAVR and the fact that this registry was carried out in centres with ‘full capabilities’ our data suggest that a relevant degree of undertreatment persists >15 years since publication of the EHS. The number of asymptomatic patients with no indication for valve replacement, but who were referred for either TAVR or SAVR, is also intriguing. Current guidelines state that TAVR is not recommended for asymptomatic patients4; yet, TAVR was the treatment decision more often than SAVR. This unusual management does not seem to be explained by baseline characteristics as differences were modest suggesting that other factors may have influenced the decision. Although we could not exclude that some patients may have been falsely classified as asymptomatic and that an exercise test may had unveil a functional impairment, this seems marginal as an exercise test is seldom performed in routine practice in the octogenarian population. Discrepancies observed between guidelines and real-world practice reflects the lack of data regarding valve replacement in asymptomatic patients and highlights a need for further research. It is also worth noting that despite surgical risk scores were relatively low, TAVR was the main type of intervention proposed. Our findings are fully aligned with the progressive shift towards intermediate and even low-risk patients in Western countries.14 15
Limitations
IMPULSE is the largest prospective registry to date documenting clinical characteristics and management decisions in contemporary patients with severe AS with or without symptoms. In addition, we were able to capture the complete spectrum of AS patients including those who did not undergo aortic valve replacement and as such not being part of recent surgical and transcatheter registries. As an observational, cross-sectional registry though, IMPULSE is associated with some inherent limitations: (1) although treatment decisions were documented, the actual treatment that each patient underwent may have differed; (2) outcomes after valve intervention were not recorded; (3) some variables were not 100% complete, leaving room for a degree of uncertainty; (4) the performance of an exercise test and the aortic stroke volume were not collected to judge the appropriateness of the intervention in a subset of patients; (5) finally, it is difficult to definitively assign symptomatic status in AS as some of the symptoms may have been unspecific.
Conclusions
Symptomatic patients were older and had multiple comorbidities, suggesting that the initial presentation of AS patients has shifted towards older patients compared with previous decades. Despite significant improvements, management of severe AS remained suboptimal in a significant proportion of contemporary patients with severe AS.
Key messages
What is already known on this subject?
Most of the data on characteristics of and treatment strategies in patients with aortic stenosis (AS) are based on clinical trials and registries that describe patients scheduled for an intervention, but there is no contemporary population based data on patients with a new diagnosis of severe AS, and the course of their subsequent clinical management.
What might this study add?
In this registry based on patients with severe AS, we observed that symptomatic patients are still referred late in the course of the disease with severe symptoms and or left ventricle dysfunction already present. Despite the availability of transcatheter aortic valve replacement (TAVR) and clear guideline recommendations for the treatment of these patients, >20% of symptomatic patients are denied an intervention and conservative treatment pursued instead. More than a third of asymptomatic patients are referred for an intervention in the absence of class I or class IIa indications and TAVR was preferred over surgical aortic valve replacement in these cases.
How might this impact on clinical practice?
Despite significant improvements, management of severe AS remained suboptimal in a significant proportion of contemporary patients with severe AS.
Acknowledgments
Data were captured using the s4trials software provided by Software for Trials Europe GmbH, Berlin, Germany. The authors would like to thank Cornelia Deutsch (IPPMed) for performing the statistical analysis. The study was funded by Edwards Lifesciences, Nyon, Switzerland.
References
Footnotes
Contributors NF, RPS, DM-Z, JK, MT and PB were involved in the conception and design of the study. NF, PB and DM-Z drafted the manuscript and all other authors revised the article for important intellectual content. All authors gave final approval of the version to be published.
Funding This work was supported by a research grant provided by Edwards Lifesciences (Nyon, Switzerland) to the Sponsor, the Institute for Pharmacology and Preventive Medicine (IPPMed, Cloppenburg, Germany).
Competing interests PB is the representative of the IPPMed. NF, RPS, TKR and DM-Z have received speakers’ honoraria from Edwards Lifesciences. The institutions of these three and those of the remaining authors representing study centers have received funding from the sponsor for employing a study nurse for the duration of the study. IPPMed designed and executed the study, collected and analysed the data and drafted/revised the manuscript in collaboration with the other authors.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Data are available upon reasonable request.
Patient consent for publication Not required.