Article Text

Abstract
Objective The optimal timing for transplantation is unclear in patients with Eisenmenger syndrome (ES). We investigated post-transplantation survival and transplantation-specific morbidity after heart–lung transplantation (HLTx) or lung transplantation (LTx) in a cohort of Nordic patients with ES to aid decision-making for scheduling transplantation.
Methods We performed a retrospective, descriptive, population-based study of patients with ES who underwent transplantation from 1985 to 2012.
Results Among 714 patients with ES in the Nordic region, 63 (9%) underwent transplantation. The median age at transplantation was 31.9 (IQR 21.1–42.3) years. Within 30 days after transplantation, seven patients (11%) died. The median survival was 12.0 (95% CI 7.6 to 16.4) years and the overall 1-year, 5-year, 10-year and 15-year survival rates were 84.1%, 69.7%, 55.8% and 40.6%, respectively. For patients alive 1 year post-transplantation, the median conditional survival was 14.8 years (95% CI 8.0 to 21.8), with 5-year, 10-year and 15-year survival rates of 83.3%, 67.2% and 50.0%, respectively. There was no difference in median survival after HLTx (n=57) and LTx (n=6) (14.9 vs 10.6 years, p=0.718). Median cardiac allograft vasculopathy, bronchiolitis obliterans syndrome and dialysis/kidney transplantation-free survival rates were 11.2 (95% CI 7.8 to 14.6), 6.9 (95% CI 2.6 to 11.1) and 11.2 (95% CI 8.8 to 13.7) years, respectively. The leading causes of death after the perioperative period were infection (36.7%), bronchiolitis obliterans syndrome (23.3%) and heart failure (13.3%).
Conclusions This study shows that satisfactory post-transplantation survival, comparable with contemporary HTx and LTx data, without severe comorbidities such as cardiac allograft vasculopathy, bronchiolitis obliterans syndrome and dialysis, is achievable in patients with ES, with a conditional survival of nearly 15 years.
- Eisenmenger syndrome
- lung transplantation
- heart-lung transplantation
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Eisenmenger syndrome (ES) is the most severe expression of any unrepaired congenital cardiac defect with a systemic-to-pulmonary shunt. The initial left-to-right shunt may result in elevated pulmonary vascular resistance and right-to-left/bidirectional shunt causing cyanosis.1 Development of ES represents a point at which the pulmonary vascular disease is irreversible with contraindication against closure of the shunt lesion.
Medical therapy with pulmonary vasodilators such as endothelin receptor antagonists, phosphodiesterase-5 inhibitors or prostacyclins may result in decreased pulmonary vascular resistance with improved exercise capacity and possibly improved survival.2–6 However, despite this advance in medical treatment in the last decade, transplantation, either combined heart–lung transplantation (HLTx) or lung transplantation (LTx) with concomitant cardiac repair, remain the only definitive treatment options available for severely symptomatic patients.
Since the 1980s, congenital heart disease including ES has been the indication for approximately 40% of HLTx.7–10 The high rate of HLTx in the 1980s peaked in 1989, when almost 300 adult and paediatric HLTx procedures were reported to the registry of the International Society of Heart and Lung Transplantation (ISHLT). The number of HLTx procedures has subsequently declined to an annual rate of 38–94 for the latest decade, with 58 HLTx procedures reported in 2016.10 11
Transplantation is usually reserved for increasingly symptomatic patients with ES, as the overall survival rate for stable patients managed medically has been considered comparable to that of HLTx.12 13 The optimal timing for transplantation is difficult to determine, given that patients who survive to adulthood are often well adapted to their restricted exercise capacity and may present with acute deterioration before considering transplantation.14 15 And although a risk stratification model for these patients are available, the optimal timing for transplantation is still debateable.14 The aims of the present study were to evaluate Nordic patients with ES who underwent transplantation from 1985 to 2012 in order to describe their overall survival and major morbidity-free survival, to aid decision-making regarding when to list patients for HLTx.
Methods
This was a retrospective, descriptive, multicentre study of patients transplanted because of ES. From the population-based Nordic Eisenmenger database, data on all transplantations in patients with ES were available.16 ES was defined as pulmonary vascular disease in the presence of a large non-restrictive shunt accompanied by cyanosis.1 16–19 The patients were divided into simple pre-tricuspid (atrial septal defects (ASD)), simple post-tricuspid (ventricular septal defects (VSD), patent ductus arteriosus (PDA) and aortopulmonary window) and complex lesions including ASD, univentricular hearts, transposition of the great arteries and truncus arteriosus. The patients’ records (each with a unique personal identification number) were cross-checked with the national death registries providing vital status, date of death and cause of death. Follow-up data regarding survival and transplantation-specific morbidity were available for all patients. Renal insufficiency was defined as decreased estimated glomerular filtration rate (<60 mL/min/1.73 m2) and/or increased serum creatinine (above the limit of the normal range according to local guidelines) over a period of >90 days and/or the diagnosis given in the medical chart (retrospective patients). End-stage renal insufficiency was defined as the need for dialysis or kidney transplantation (RTx). Systemic hypertension was defined as elevated blood pressure requiring medical treatment. Follow-up of surviving patients was censored at 31 December 2015. For the analysis of cause-specific mortality, the term ‘perioperative death’ was defined as death occurring within 30 days of transplantation. Supplementary donor data was obtained from the Scandia transplant database.20
Ethics
The present study and the Nordic Eisenmenger database were registered and approved by appropriate health, ethics and data authorities in all participating countries from the Nordic region and were registered at clinicaltrials.gov (INCT01976533). All data were anonymised when shared across borders. As this was a retrospective study evaluating existing data from national registries and medical records, individual informed consent was not required.
Statistics
Continuous variables are presented as mean±SD if normally distributed or as median and IQR otherwise. Categorical variables are presented as frequencies and percentages. Associations between categories were evaluated by the χ2 test or Fisher’s exact test, where appropriate. Student’s t-test or the Mann-Whitney U-test was used for continuous variables.
For assessing time-to-event rates, Kaplan-Meier analysis was used. For survival analysis, all-cause mortality was included. The Kaplan-Meier analysis conditioned by surviving the first year post-transplantation accounted for left truncation. Survival curves were assessed and compared with the log-rank test. All statistical analyses were performed with SPSS V.22 (IBM, Armonk, New York, USA) and the null hypothesis was rejected based on a two-sided p value of <0.05.
Results
Patients
We identified 714 patients with ES in the Nordic countries. In the period from 1985 to 2012, 63 of these patients underwent HLTx (57 patients, 90.5%) or LTx with concomitant repair of the cardiac defect (six patients, 9.5%). All LTx patients underwent double-lung transplantation. The procedures were performed in five centres throughout the Nordic region, and two transplants were performed in other European countries prior to an established HLTx programmed in the region. The corrected defects were mainly of the simple type (two ASD, two and one) and one complex (pulmonary atresia with VSD and major aortopulmonary collateral arteries) (table 1). During the same time period, a total of 125 HLTx and 1886 LTx procedures were performed in the region.20 Thus, ES was the indication for 3% of all LTx and 46% of the HLTx procedures performed during this period.
Demographic data and patient characteristics
The median age at transplantation was 31.9 (IQR 21.1–42.3) years. Paediatric transplantations (<18 years) accounted for 13% of the transplantations. The median donor age was 26.5 (IQR 18.3–39.8) years. Most transplants (n=55, 87%) were performed prior to 2006. Of the eight patients transplanted in 2006 or later, six (75%) received medical pulmonary vasodilator therapy prior to transplantation. The median duration of pretransplantation advanced therapy was 5.0 (IQR 1.1–7.1) years.
The median proportion of patients with ES who underwent transplantation during the period was 0.37% (IQR 0.19%–0.73%), with the highest annual proportion of 2.1% in 1994 (figure 1). Demographic data, patient characteristics and pretransplant evaluation are presented in table 1.

Transplantations in patients with ES in the Nordic region. ES, Eisenmenger syndrome; HLTx, heart–lung transplantation; LTx, lung transplantation.
No patients were transplanted urgently from mechanical circulatory support. Waiting time to transplantation was less than a year in 30 patients (48%). Ischaemic time was below 4 hours in 65% of patients (table 2). Information about induction therapy with antithymocyte globulin and maintenance immunosuppression are available in table 2.
Transplantation and treatment
Survival
A total of 39 deaths (62%) occurred during the study of which seven (11%) were perioperative deaths within 30 days of transplantation; 55 patients (87%) were discharged from hospital alive. The crude 1-year survival rate was 86%. Median survival post-transplantation was 12.0 (95% CI 7.6 to 16.4) years, with 1-year, 5-year, 10-year and 15-year survival rates of 84.1%, 69.7%, 55.8% and 40.6%, respectively (figure 2). The median survival conditioned by surviving the first year after transplantation was 14.8 (95% CI 8.0 to 21.8) years, with 5-year, 10-year and 15-year survival rates of 83.3%, 67.2% and 50.0%, respectively (figure 2).
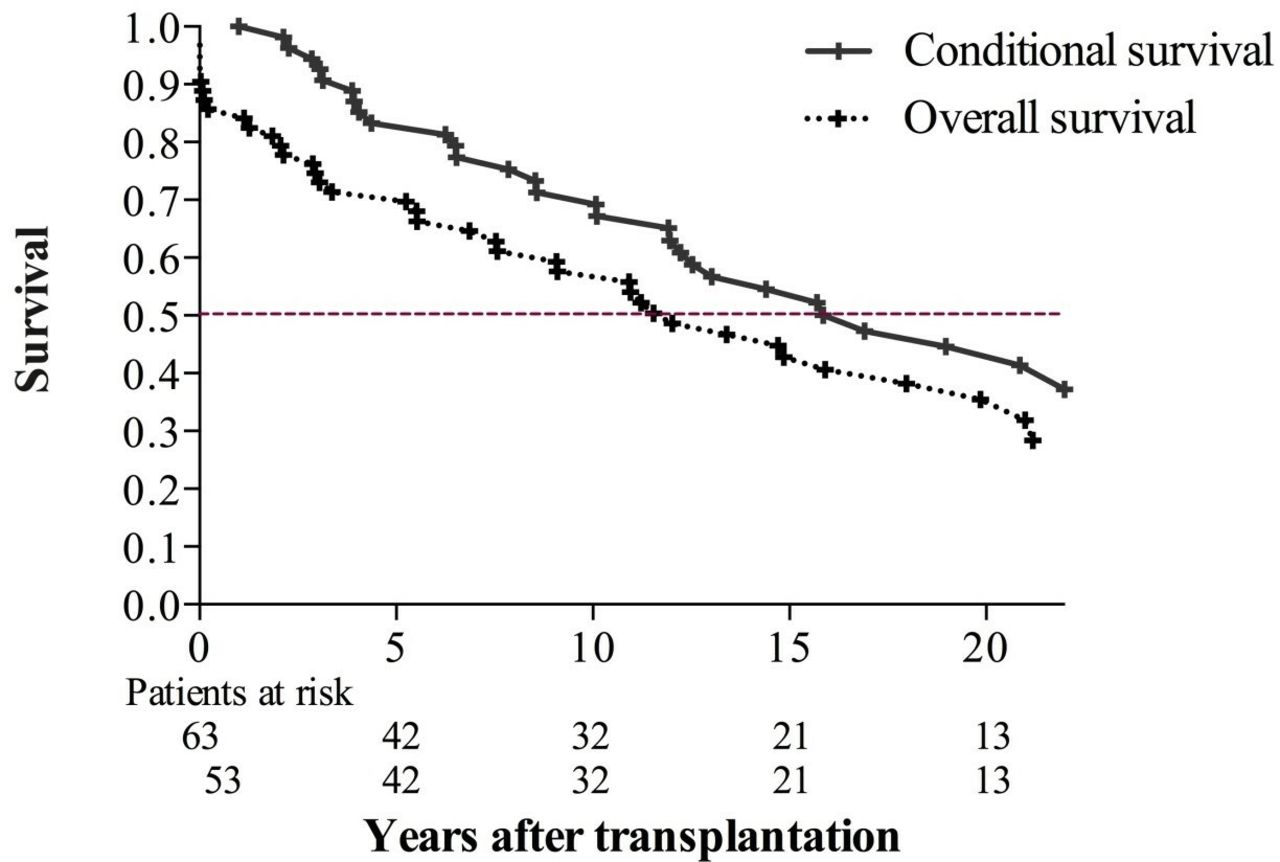
Kaplan-Meier curve illustrating post-transplantation survival.
There was no difference in median survival after HLTx and LTx (12.0 vs 10.9 years, log-rank p=0.718). Likewise, there was no difference in survival between complex (median survival 14.7 years) and simple defects (median 11.5 years, p=0.845), between paediatric and adult transplantations (7.6 vs 13.4 years, p=0.59), or between centres (median 5.5–18.5 years, p=0.128). No data were available on the number of patients that died while waiting for transplantation. None of the patients underwent retransplantation.
Transplantation-related morbidity
Typical transplantation-related morbidity was observed both short and long term (table 3). Almost one-third of the patients underwent reoperation within the first week, almost all due to haemorrhage (95%), and nearly half were treated for allograft rejection within the first year. More than one in five persons were diagnosed with cancer, of which 60% were non-skin cancers. Nine patients (14%) developed end-stage renal insufficiency and required dialysis; four patients (6%) later received RTx. Over 10% developed cardiac allograft vasculopathy (CAV) and 37% developed bronchiolitis obliterans syndrome (BOS). More than half of the patients were treated for systemic hypertension (table 3).
Transplantation-related morbidity and complications
Median CAV, BOS, dialysis/RTx and non-skin malignancy-free survival rates were 11.2 (95% CI 7.8 to 14.6) years, 6.9 (95% CI 2.6 to 11.1) years, 11.2 (95% CI 8.8 to 13.7) years and 11.2 (95% CI 8.1 to 14.4) years, respectively. Survival with freedom from the composite of all of the endpoints above was 5.5 (95% CI 2.3 to 8.8) years. For patients surviving 1 year after transplantation, the conditional CAV, BOS, renal dialysis/RTx and non-skin malignancy-free survival rates are shown in figure 3. Conditional survival with freedom from the composite of all the endpoints above was 6.8 (95% CI 3.0 to 10.5) years.

{kind=link}
{kind=link}
{kind=link}
Conditional cardiac allograft vasculopathy, bronchiolitis obliterans syndrome, renal dialysis and kidney transplantation and non-skin malignancy-free survival rates.
Cause-specific mortality
Cause-specific mortality could be identified from death certificates or medical records in 37 (94.9%) patients, and 18.9% of the deaths were perioperative (table 4). Among the remaining deaths, the leading cause of death was infection (36.6%), followed by BOS (23.3%). Infections were largely dominated by pneumonia (63.3%). Death due to heart failure ranked fourth (10%), whereas other causes such as haemorrhage (6.7%), rejection (6.7%), organ failure (6.7%), trauma (6.7%) and malignancy (3.3%) accounted for the remaining nine deaths (30.1%) (table 4).
Cause-specific mortality
Discussion
The main finding of this multicentre study was a median survival of 12 years after transplantation in patients transplanted due to ES, which is very similar to contemporary heart transplantation (HTx) data.10 Second, it indicated that good post-transplantation survival without severe complications is achievable in this multimorbid group of patients.
Survival
Survival after HLTx in various patients with congenital heart disease differs according to pretransplantation diagnosis, with patients with ES having the best overall and conditional survival compared with patients with congenital heart disease without ES and patients with idiopathic pulmonary arterial hypertension.8 Within the group of patients with ES, the present study found no variation in survival based on underlying congenital defect in accordance with an earlier study.21
A small number of reports on overall survival rates post-transplantation in patients with ES are available in the literature.7–9 21–24 For HLTx, 30 days and 1 year survival was 80.7% and 70.1% compared with 68% and 55.2% for LTx using United Network for Organ Sharing/ISHLT Joint Thoracic Registry,22 and in another study from Cambridge, 1-year, 5-year and 10-year survival rates for ES were 72.6%, 51.3% and 27.6%, respectively,21 which is also considerably lower than observed in this Nordic cohort. In comparison, the observed survival rates in the present study are similar to recent ISHLT data on survival after adult HTx25 as well as HTx reported from Scandinavian centres within a similar period.26 In contrast, survival after LTx ranges from 4.3 to 6.5 years.9 25 However, it should be noted that patients in the present cohort were transplanted at a median age of 31.9 years, at a somewhat younger age than patients with ES from other studies.26–28 This difference could likely have had an impact on survival.
In the present study, a difference in survival between HLTx and LTx was not confirmed, although only six LTx procedures were performed. However, an earlier multicentre study from 2002, based on data from the ISHLT, including 576 patients with ES over a 10-year period, reported a 1-year survival after HLTx of 70% as compared with 55% after LTx.22
In recent years, however, and despite findings in the ISHLT study,22 bilateral and single LTx procedures with repair of the cardiac defect have been advocated for patients with ES in order to maximise the use of the scarce donor organ supply. The reality is that single-organ transplantation offers much shorter waiting times and thus a better chance of transplantation.11 21 23 24
All LTx procedures for ES in the Nordic cohort were performed within the latter 15 years of the study period, mirroring the international trend.8
However, the notable survival rates after HLTx reported in the present study and the procedural difference as suggested by the ISLHT data22 merits further multicentre investigations to define the best use of organs in patients with ES.
In the current cohort, only few transplantations were performed after 2006 when treatment with oral pulmonary vasodilators became more widely available.2 However, whether this observation is due to fewer patients suffering from ES,16 improved condition of patients with ES resulting in fewer listings for transplantation or merely the result of the prioritised organ expenditure or a coincidental finding cannot be distinguished from the present study. Recent reports have also indicated that treatment with pulmonary vasodilators in ES may substantially delay the need for HLTx and may also have a positive effect on survival.6 13 The current data indicate that survival after transplantation in patients with ES are better than previously reported; however, this post-transplantation survival is similar to the reported survival of patients with ES treated with pulmonary vasodilators.15 And even though one may argue that the patients with ES on pulmonary vasodilator therapy and the transplanted patients with ES are from two different eras, any treatment option without the severe morbidities following transplantation, ought to be exploded prior to transplantation. Still, only 75% of the patients in the present cohort transplanted after 2006 received pulmonary vasodilators prior to transplantation. Furthermore, approximately 75% of the current cohort had relative anaemia according to the suggested optimal relationship29 prior to transplantation, which is an acknowledged cause of poor functional level.
Although the present data do not elucidate these findings, it could be hypothesised that the increased awareness of the pitfalls of routine phlebotomy, including iron deficiency and thrombogenicity, alongside an increasing focus on iron supplement and the use of pulmonary vasodilators, may be contributory to the fading rate of transplantation for ES.
Transplantation-related morbidity
Although data exists on long-term complications and complication-free survival after HLTx due to congenital heart disease, idiopathic pulmonary arterial hypertension and cystic fibrosis,7–10 the present study is the first study devoted solely to patients with ES. Confirming data after LTx for all diagnoses,7 9 10 BOS was the major factor determining long-term graft outcome. BOS was diagnosed in more than one-third of the patients and the cause of death in almost one-fifth, suggesting failure of the pulmonary graft rather than the cardiac graft.
Dialysis/RTx was much more frequent in the present study than in previous reports (23% vs 0%–4%), although the proportion of patients with renal dysfunction (22%–42%) was quite similar between the studies.7–10 Given that most transplantations were performed more than a decade ago, calcineurin inhibitor-free regimens, typically based on everolimus, were not used in this cohort. Contrarily, CAV and non-skin cancer had little impact on comorbidity-free survival in the present study as well as in previous studies. Non-severe comorbidities such as hypertension were less frequent in the present study despite a longer follow-up compared with other studies.7–10
Cause-specific mortality
After the perioperative period, more than one-third of the deaths were due to infections and more than half the deaths were due to either infections or BOS. Susceptibility to infections after any solid organ transplant is usually attributed to immunosuppression and the infection is typically caused by bacteria or viruses common in the community. However, infections are also a frequent cause of death in non-transplanted patients with ES,29 accounting for almost 30% of the deaths in these patients. Although CAV was diagnosed in almost 10% of the patients, it was not the primary cause of death in any patient, corroborating data from an earlier study on transplantation in patients with ES.21
Strengths and limitations
The present study was based on data from the Nordic Eisenmenger cohort with a large population-based design.16 In the Nordic countries, the implementation of a system with individual unique personal identification numbers and a social structure allowing general access to free, qualified healthcare and population-based validated registries creates a unique opportunity for the long-term follow-up of large numbers of patients. In addition, the extensive Nordic registries provide reliable outcome data on all citizens, thus, minimising ‘informative censoring’ and strengthening survival analysis. In addition, the Nordic registries diminish the risk of reporting bias where only good results are reported, as all procedures regardless of outcome are registered.
This study, however, has obvious limitations due to the nature of its design as retrospective data were collected from several centres in the Nordic countries over a long period with different strategies for treatment and follow-up. Further on, although the study is population based and include all patients from the Nordic region, larger registry-based studies on the outcome after transplantation in this patient group are available in the literature.7–9 21–24
As in all retrospective studies reporting on cause-specific mortality, the validity of the cause of death was dependent on the reporting physician at the time of death. During the study period of 25 years, the classification and investigations of the cause of death may have changed and the autopsy frequency could have decreased, which may have introduced a bias.
Conclusion
This study shows that post-transplantation survival with a low incidence of severe transplant-related morbidities such as CAV, BOS, dialysis and non-skin cancer is achievable in patients with ES, with a conditional survival of nearly 15 years. In carefully selected patients with ES, HLTx and LTx with cardiac repair remain viable treatment options with acceptable outcomes.
Key messages
What is already known about this subject?
The number of heart–lung transplantations (HLTx) has decreased during recent decades. In patients with Eisenmenger syndrome, transplantation is usually reserved for increasingly symptomatic patients, as the overall survival rate for stable patients managed medically has been considered comparable with that of HLTx.
What might this study add?
This is the first population-based study in patients with Eisenmenger syndrome who underwent transplantation over almost three decades. This study enables us to describe overall survival and major morbidity-free survival, to aid decision-making regarding listing patients for HLTx. The main finding of the study was a median survival of 12 years after transplantation, which is very similar to contemporary heart transplantation (HTx) data. Second, it indicated that good post-transplantation survival without severe complications is achievable in this multimorbid group of patients.
How might this impact on clinical practice?
These findings illustrate that satisfactory post-transplantation survival, comparable with contemporary HTx and lung transplantation data, without severe comorbidities such as cardiac allograft vasculopathy, bronchiolitis obliterans syndrome and dialysis, is achievable in patients with Eisenmenger syndrome. This may be of interest and use to cardiologists and researchers within congenital heart disease and transplantation in order to plan future clinical service as well as research areas.
Acknowledgments
The following persons are acknowledged for their contribution with data acquisition and overall support of the study: Mikael Dellborg (Department of Cardiology at Sahlgrenska Academy, University of Gothenburg, Gothenburg) and Henrik Holmstrøm (Department of Paediatric Cardiology, Rikshospitalet, Oslo, Norway).
References
Footnotes
Contributors CSH, TG, MOP, TM, MT, UT and FG made substantial contributions to the conception or design of the work or the acquisition, analysis or interpretation of data. CSH drafted the work. TG, GD, MOP, ASJ, TM, MT, UT, FG and LS revised the work critically for important intellectual content. All authors contributed to the final approval of the version published.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests CSH received an educational grant from Actelion Pharmaceuticals. ASJ received a research grant and speaker’s fees from Actelion Pharmaceuticals. UT received fees for lectures and being member of advisory board from Actelion Pharmaceuticals. LS received research grant, as well as fee for lectures and being member of advisory board from Actelion Pharmaceuticals. TG, GD, MOP, TM, MT and FG reports no relationships that could be construed as a conflict of interest.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.