Article Text

Abstract
Objective We assessed the diagnostic and prognostic implications of early cardiac magnetic resonance (CMR), CMR-based deformation imaging and conventional risk factors in patients with troponin-positive acute chest pain and non-obstructed coronary arteries.
Methods In total, 255 patients presenting between 2009 and 2019 with troponin-positive acute chest pain and non-obstructed coronary arteries who underwent CMR in ≤7 days were followed for a clinical endpoint of all-cause mortality. Cine movies, T2-weighted and late gadolinium-enhanced images were evaluated to establish a diagnosis of the underlying heart disease. Further CMR analysis, including left ventricular strain, was carried out.
Results CMR (performed at a mean of 2.7 days) provided the diagnosis in 86% of patients (54% myocarditis, 22% myocardial infarction (MI) and 10% Takotsubo syndrome and myocardial contusion (n=1)). The 4-year mortality for a diagnosis of MI, myocarditis, Takotsubo and normal CMR patients was 10.2%, 1.6%, 27.3% and 0%, respectively. We found a strong association between CMR diagnosis and mortality (log-rank: 24, p<0.0001). Takotsubo and MI as the diagnosis, age, hypertension, diabetes, female sex, ejection fraction, stroke volume index and most of the investigated strain parameters were univariate predictors of mortality; however, in the multivariate analysis, only hypertension and circumferential mechanical dispersion measured by strain analysis were independent predictors of mortality.
Conclusions CMR performed in the early phase establishes the proper diagnosis in patients with troponin-positive acute chest pain and non-obstructed coronary arteries and provides additional prognostic factors. This may indicate that CMR could play an additional role in risk stratification in this patient population.
- cardiac magnetic resonance (CMR) imaging
- acute myocardial infarction
- myocarditis
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
A growing number of studies have confirmed that myocardial infarction (MI) with non-obstructed coronary arteries (MINOCA) is an important working diagnosis subgroup among patients with signs and symptoms of acute coronary syndrome (ACS). The prevalence of patients with a working diagnosis of MINOCA is up to 10% among patients with ACS.1 2 The inclusion and exclusion criteria and diagnostic methods of studies assessing these patients have varied greatly.3–7
To facilitate clinical decision making, the European Society of Cardiology (ESC) published a position paper on MINOCA. This paper, among others, suggests that CMR imaging should be used in patients with a working diagnosis of MINOCA due to its unique capability to non-invasively assess cardiac function, structure and tissue characteristics, including oedema and necrosis/fibrosis.2
Myocardial deformation imaging modalities, especially CMR-based feature-tracking analysis in recent years, are gaining recognition for their unique value in more accurately approximating myocyte metabolism and contractility than the widely used left ventricular ejection fraction (LVEF).8 Although limited data are available regarding whether CMR-based strain parameters have incremental prognostic roles in addition to other readily available imaging modalities, some studies have already demonstrated the prognostic value of LV strain in patients with acute MI.9 10
According to the current ESC guidelines on patients with acute MI presenting with ST-segment elevation, in the subgroup of patients with non-obstructed coronary arteries, performing a CMR examination within 2 weeks after the onset of symptoms should increase the diagnostic accuracy of this method.11 However, little is known about the systematic application of early CMR in both the differential diagnosis of patients with a working diagnosis of MINOCA and their subsequent prognosis. Thus, we conducted a study with the following two aims. First, we evaluated the diagnostic implications of early CMR (≤7 days). Second, we sought to assess the prognostic impact of conventional risk factors and CMR examination, including diagnosis, standard parameters and strain analysis, in patients with a working diagnosis of MINOCA.
Methods
Study population
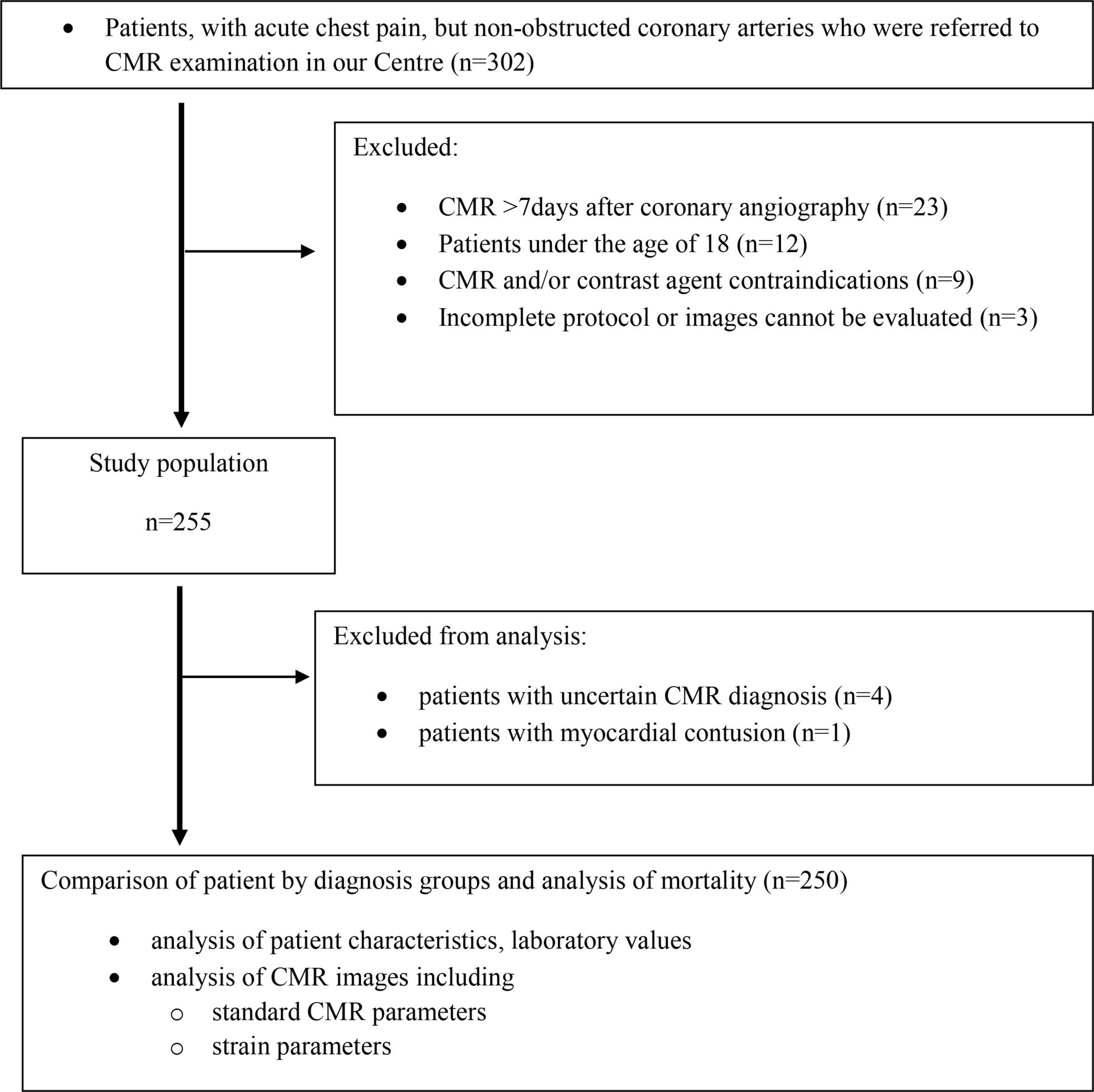
Consecutive patients presenting between April 2009 and April 2019 with a working diagnosis of MINOCA (troponin-positive acute chest pain and non-obstructed coronary arteries) who underwent CMR in our tertiary referral centre were identified in our CMR database and followed up in this retrospective longitudinal observational study. The inclusion criteria for enrolment into the study were: (1) acute chest pain; (2) a significant increase in the high-sensitive troponin T value (>14 ng/L); (3) ECG changes, such as at least 1 mm of ST-segment elevation or ST-segment depression or negative T-waves in at least two related leads; and (4) normal coronary arteries or coronary arteries with signs of atherosclerosis with stenosis <50% in a luminal diameter as demonstrated by invasive coronary angiography. The exclusion criteria were: (1) a CMR examination performed more than 7 days after invasive coronary angiography; (2) malignant ventricular arrhythmias at presentation or having known dilated cardiomyopathy with signs of severe heart failure as a primary complaint; (3) acute renal failure or chronic disease with a glomerular filtration rate <30 mL/min/1.73 m2; and (4) age <18 years (figure 1). Patients’ referral diagnoses were based on a physical examination, 12-lead ECG, laboratory values, comorbidities, and coronary angiography and echocardiography, and these results were provided to us by the referring physician. All patients gave their written informed consent for data collection and research purposes.

Study flow chart. CMR, cardiovascular magnetic resonance.
Cardiovascular magnetic resonance (CMR) protocol
CMR examinations were performed on a 1.5 Tesla MRI scanner (Achieva, Philips Medical Systems). The CMR protocol contained the following sequences: cine movie images, T2-weighted spectral inversion recovery (SPIR) images for myocardial oedema and late gadolinium enhancement (LGE) images for necrosis/fibrosis. Functional imaging was performed using balanced steady-state free precession cine sequences in four-chamber, two-chamber and three-chamber long axis (LA) views and a short axis (SA) stack from the cardiac base to apex, with full coverage of the left and right ventricle. Wall motion abnormalities (WMAs) were assessed. LGE images were acquired using a segmented inversion recovery sequence 10–15 min after the administration of an intravenous bolus of 0.15 mmol/kg of the gadolinium-based contrast agent gadobutrol (Gadovist, Bayer-Schering Pharma) at a rate of 2–3 mL/s through an antecubital intravenous line. The inversion time was adjusted to provide optimal suppression of normal myocardium.
Image analysis
For all participating patients, the CMR studies were analysed and reported under the supervision and with the final approval of at least one of two consultants with >10 years of experience in performing CMR with a European Association of Cardiovascular Imaging CMR level 3 certification. The visual and parametric information obtained from cine movies was combined with T2-weighted and LGE images to establish the final diagnosis. Based on the CMR findings, patients received one of the following diagnoses: acute MI, acute myocarditis, Takotsubo syndrome (Takotsubo) or normal CMR. A diagnosis of MI was based on an increased or decreased T2 signal, perfusion defect, microvascular obstruction and an ischaemic LGE pattern (subendocardial to transmural).2 12 Acute myocarditis was defined as an increased T2 signal showing myocardial oedema on SPIR images and the presence of LGE in a patchy non-ischaemic pattern with a subepicardial and/or midmyocardial extent.13 The diagnosis of Takotsubo was established based on regional WMAs extending beyond a single coronary territory with no extensive LGE and potential myocardial oedema.14 If we did not find any abnormalities, including myocardial oedema, necrosis/fibrosis or WMA, the patient was characterised as having normal CMR. Patients with an LGE pattern not specific to any disease were defied as inconclusive. LV functional and morphological parameters were calculated from the SA stack using MedisSuite/QMass Software (Medis Medical Imaging Software, The Netherlands). The CMR-based diagnosis was recorded and subsequently compared with the referring diagnosis to investigate the diagnostic impact of CMR. Quantitative deformation assessment was obtained using cine images and analysed with the feature-tracking application of Medis QStrain software by an experienced reader. Endocardial contour detection was performed manually on LA and SA cine images in end-systolic and end-diastolic phases as described by Pedrizzetti et al.15 Global strain values, including longitudinal (GLS), circumferential (GCS) and radial (GRS) LV strain parameters, were measured. For global dyssynchrony measurement, mechanical dispersion (MD) was assessed, defined as the SD of the time-to-peak circumferential (MDC) and longitudinal (MDL) strain of the LV segments and expressed as a per cent of the cardiac cycle. No patient was excluded from the analysis because strain measurements could not be performed. Interobserver variability in strain parameters was compared in a subgroup of randomly selected patients (n=100) that included 25 patients from each diagnosis group. Only strain parameters with an inter-rater agreement (kappa) higher than 0.6 were accepted for analysis; therefore, all strain parameters concerning myocardial rotation and MD derived from radial strain were excluded.
Study endpoint
The endpoint of our study was all-cause mortality, which was ascertained based on both available medical records and the National Health Insurance Fund of Hungary (Hungarian acronym: NEAK) database, which includes up-to-date information on deaths. The NEAK, as a central agency, performs functions specified by legislation, maintains records and financial accounts and fulfils reporting obligations. As part of the core activity of the NEAK, the institute provides information on health insurance and its current status.
Data management and statistical analysis
Patient data, including risk factors, laboratory values, standard CMR and CMR-based strain parameters, are described by the CMR-based diagnostic groups. Continuous variables that had a normal distribution based on Shapiro-Wilk’s test are presented as the mean and SD, and those with a non-normal distribution are presented as the median and 95% CI. Categorical variables are presented as frequencies and percentages. Comparisons of the means of continuous variables with normal distribution were performed using one-way analysis of variance and the Scheffe test for post hoc pairwise comparisons. The distributions of non-normal continuous variables were compared by Kruskal-Wallis tests. The χ2 test was applied to compare the distributions of categorical data. Univariate associations of time variables with mortality were visualised using Kaplan-Meier curves and compared by the log-rank test. Univariate and multivariate associations of risk factors and covariates with mortality were assessed using Cox proportional hazard regression analyses. Variables with values of p<0.05 in univariate analyses were candidates for multivariate analysis. Probability values were two sided, and values of p<0.05 were considered significant. MedCalc software and R Studio were used for the statistical analysis and graph generation.
Patient and public involvement in the study
It was not possible to involve patients or the public in the design, conduct, reporting or dissemination plans of our research.
Results
The diagnostic impact of CMR
During the 11-year study period, we analysed the data of 255 patients (42±16 years, 165 men) with troponin-positive acute chest pain who underwent CMR examination within 7 days following coronary angiography with non-obstructed coronary arteries (figure 1). The mean time delay between the coronary angiography and CMR examination was 2.7 days. CMR provided a final diagnosis in 86% of the cases: MI (n=55), acute myocarditis (n=136), Takotsubo (n=26) and myocardial contusion (n=1).16 CMR demonstrated a structurally normal heart in 33 patients. The diagnosis of four patients remained inconclusive after CMR. In these four patients, the examination raised the suspicion of sarcoidosis, atypical myocarditis or amyloidosis. Further examinations revealed Churg-Strauss syndrome, Amyloid light-chain amyloidosis, autoimmune disease affecting multiple organs or remaining inconclusive. Given the combined small number of patients with myocardial contusion and uncertain diagnosis (n=5), these patients were excluded from the statistical analysis. The distributions of CMR diagnoses in patients with normal arteries and those with signs of atherosclerosis are shown in table 1.
Description of the sample
In 61% of the MI (or MINOCA) patients, coronary angiography was normal. Figure 2 shows the distributions of the referral diagnoses as they relate to the CMR-based diagnosis. Overall, CMR confirmed the referral diagnosis in 48% and overrode it in 16% of the patients. CMR identified a diagnosis in 79% of those with an uncertain referral diagnosis (n=71). The most common referral diagnosis was myocarditis (n=155); however, CMR revealed MI in 21% of these patients. A comparison was performed between patients with a referral diagnosis of myocarditis in whom the CMR confirmed this suspicion (n=106) and those who were diagnosed with MI (n=32). The results showed that, compared with patients with myocarditis, patients with MI were slightly older (44±15 vs 33±9; p<0.001) and a higher percentage had hypertension (41% vs 14%; p=0.002). Takotsubo patients were referred to CMR as Takotsubo (n=13), myocarditis (n=3) or uncertain (n=10). Overall, CMR influenced patient management in 46% of the cases. Most importantly, in newly diagnosed patients with MI, the medication was changed. Based on an unexpected diagnosis of MI in 51, Takotsubo in 13 and myocarditis in 30 patients, CMR led to lifestyle changes and/or closer surveillance.

The diagnostic impact of early CMR. Among patients with troponin-positive acute chest pain and non-obstructed coronary arteries, an early CMR (≤7 days) established a diagnosis in 86% of the patients. CMR confirmed the referral diagnosis in 48% and overrode it in 16%, identified the aetiology in 22%, revealed a structurally normal heart in 13% and remained Inconclusive in 1% of the patients. CMR, cardiovascular magnetic resonance.
Patient characteristics, laboratory values, CMR parameters and strain analysis
While the prevalence of traditional cardiovascular risk factors was relatively low, certain significant differences in patient characteristics were observed (table 1). Overall, the mean LVEF remained preserved with normal LV volumes (table 1). Takotsubo patients showed lower LVEF and higher left ventricular end-systolic volume index than was found in any other group. Among strain parameters, the following differences were observed: Takotsubo patients had significantly higher (ie, less negative) GLS and GCS and lower GRS values than were found in the other groups (table 1, online supplementary figure 1). A comparison of MI and myocarditis patients showed there was no significant difference regarding their GLS, GCS and GRS values; however, global dyssynchrony parameters, especially MDC, were significantly higher in the MI group. Figure 3 demonstrates the strain analysis and the patterns of LGE in MI, myocarditis and Takotsubo patients.
Supplemental material

CMR images of patients with myocardial infarction (A and D), myocarditis (B and E) and Takotsubo syndrome (C and F). CMR cine movie images depict endocardial contours during strain analysis (A–C). Late gadolinium-enhanced images showing transmural necrosis (white arrow) and microvascular obstruction (red arrow) in patients with acute myocardial infarction (D); patchy, midmyocardial necrosis in myocarditis (white arrows) (E); and the lack of LGE in Takotsubo syndrome (F). CMR, cardiovascular magnetic resonance; LGE, late gadolinium enhancement.
Follow-up and mortality
Overall, the 30-day, 1-year and 4-year mortality rates were 0.4%, 1.8% and 5.9%, respectively (table 2).
Follow-up and mortality
The 4-year all-cause mortality rates by the diagnosis of MI, myocarditis, Takotsubo or normal CMR in these patients were 10.2%, 1.6%, 27.3% and 0%, respectively. Figure 4 shows Kaplan-Meier survival analysis figures and the corresponding log-rank tests. There was a strong association between a CMR diagnosis and mortality (log-rank test: 24, p<0.0001). Takotsubo and MI as the diagnosis, age, history of hypertension or diabetes, female sex, LVEF, left ventricular stroke volume index (LVSVi) and most of the investigated strain parameters, including GLS, GCS, GRS and MDC, were significant univariate predictors of mortality (table 3).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Kaplan-Meier curves showing the risk of mortality by CMR diagnosis. CMR, cardiovascular magnetic resonance.
Univariable and multivariable association for mortality
In the multivariate model, hypertension and a strain-derived dyssynchrony parameter, MDC, were independent predictors of mortality.
Correlations of the variables are shown in online supplementary 2a-c.
Supplemental material
Discussion
In our study of a large single-centre cohort of the systematic application of CMR (≤7 days) in patients with troponin-positive acute chest pain and non-obstructed coronary arteries, we found the following:
Performing CMR within a suitably narrow time window can provide a diagnosis in up to 86% of this patient population.
The aetiologies in these patients differ considerably, and the prognosis of the diagnosis groups may vary.
Takotsubo and MI as a diagnosis, age, hypertension, diabetes, female sex, LVEF, LVSVi and most of the investigated strain parameters were univariate predictors of mortality; however, in the multivariate analysis, only hypertension and MDC remained independent predictors of mortality.
Studies with a longer delay between coronary angiography and CMR have demonstrated variable success rates (27%–74%) in identifying the diagnosis in patients with a working diagnosis of MINOCA. Due to the temporary nature of certain alterations, this may lead to the misclassification of cases.7 17 All patients in our study underwent CMR within 7 days (mean of 2.6 days) after coronary angiography, and we were able to provide a definite diagnosis in almost 90% of these cases, akin to what Bhatia et al 18 found in their study with a similar cohort size (215 patients) and mean time delay to CMR (3.68 days). Our study therefore corroborates the finding that early CMR has an excellent diagnostic yield in these patients and leads to the reclassification of a high proportion of cases.3 4 18–20 The proportion of MI (or MINOCA) patients in our study (22%) was slightly higher than that reported by Kawecki et al (9%) and some other studies that reported MI diagnosed by CMR in patients with a working diagnosis of MINOCA but similar to those found by Bhatia et al (22%) and Dastidar et al (25%).7 18 19 21 22 Notably, our patient population is slightly younger than those in previous studies. This may be related to the high proportion of patients with a clinical suspicion of acute myocarditis; however, among these patients, CMR indicated MI in 21% of the patients, which is not a negligible portion.
As reported previously, MINOCA patients have slightly better prognoses than those with obstructive coronary artery disease; however, recent studies based on the SWEDEHEART registry showed that these patients have unfavourable outcomes.5 6 23 Most studies that have assessed the prognosis of MINOCA treat this group as homogenous, and this confounding factor may account for the wide variation observed in 1-year mortality, which ranges from 0.6% to 12.3%.5 24–26 First, patient groups are heterogeneous concerning their ages—the low mortality (0.6%) found by Safdar was observed in a younger (aged 18–55 years) patient population, while the high mortality (12.3%) observed by Dreyer et al 24 was found among patients aged >65 years. Second, the group of patients with a working diagnosis of MINOCA is not homogenous. Indeed, Ferreira and Sechtem et al emphasised the heterogeneity of the diagnoses obtained in patients with a working diagnosis of MINOCA in their recent editorials. They concluded that the use of CMR may refine the diagnostic labelling of such patients, thereby influencing treatment strategies and patient prognosis.3 4 Our results are comparable with those presented in a recent study by Dastidar et al,7 who used CMR systematically at a median of 37 days. Their findings reinforced the diagnostic and prognostic value of CMR in these patients. However, we found that mortality was higher in the MI (or MINOCA) group (10% vs 4%) over a slightly longer follow-up (3.5 vs 4 years). Additionally, they found a heterogeneous group of cardiomyopathies. We found that the mortality rate was slightly higher per patient-year among our Takotsubo patients than was reported in Templin et al,27 who described the long-term outcomes of the Takotsubo patients included in the InterTAK registry (6.4% vs 5.6%).
In our univariate analysis, Takotsubo and MI as a diagnosis, many risk factors and CMR parameters, notably LVEF, LVSVi and most of the investigated strain parameters, were predictors of mortality. However, in our multivariate analysis, only hypertension and a strain-derived dyssynchrony parameter were significant predictors of all-cause mortality. The reason for this might be confounding among the candidate predictor variables. For example, in the bivariate correlations, hypertension showed only a marginal correlation with any other risk factors or CMR parameters. This might explain why hypertension was both a univariate and a multivariate predictor, consistent with the previous findings of large national registries that reported prognoses of MINOCA patients.5 28 Other parameters, including older age and female sex, were significant predictors of mortality in univariate but not multivariate analysis. However, MDC was correlated with patient age, sex, Takotsubo or MI as the CMR diagnosis, and many CMR parameters, including LVEF and all of the strain parameters, all of which were significant univariate predictors. Our findings indicate that CMR has an important role in the diagnosis of patients with a working diagnosis of MINOCA and may provide useful additional parameters in the risk stratification of these patients.
Conclusions
Among patients with troponin-positive acute chest pain and non-obstructed coronary arteries, CMR performed within 7 days established a diagnosis in 86% of the patients. The aetiology in these patients varies considerably, and the prognosis of different diagnosis groups may differ. Furthermore, with the implementation of strain analysis, CMR may provide additional prognostic factors. As such, CMR may have an important role in the risk stratification of these patients.
Limitations
One limitation is that this was a single-centre study with a relatively limited sample size by diagnosis group, which might limit the generalisability of our prognostic conclusions. Although our study was designed to represent a real-world population, we excluded patients with contraindications to CMR, which might have resulted in an underestimation of our HRs. Approximately one-third of patients were referred from other hospitals; therefore, their clinical data were provided by the referring clinicians. During the data collection (2009–2019), all patients referred for CMR had one of the mentioned ECG alterations; therefore, our results are only applicable to patients with ECG changes. Due to the retrospective nature of the study, blinded interpretation of the CMR images was not performed. Moreover, although coronary vascular imaging modalities, intravascular ultrasound and optical coherence tomography can provide insight into plaque disruption or spontaneous coronary artery dissection,2 these modalities were not included in our study.
Key messages
What is already known on this subject?
The position paper by the European Society of Cardiology on myocardial infarction with non-obstructive coronary arteries (MINOCA) suggested the use of cardiac magnetic resonance (CMR) imaging in patients with a working diagnosis of MINOCA.
What might this study add?
Among patients with troponin-positive acute chest pain and non-obstructed coronary arteries, CMR performed within 7 days established a diagnosis in 86% of the patients. Their aetiologies differed considerably, and the prognosis of different diagnosis groups may vary.
How might this impact on clinical practice?
CMR may enable clinicians to establish the proper diagnosis and provide additional prognostic factors, which could enhance the personalised assessment of prognosis in patients with troponin-positive acute chest pain and non-obstructed coronary arteries.
References
Footnotes
HV and LS are joint first authors.
DB and BM are joint senior authors.
Twitter @liliana_e_szabo
HV and LS contributed equally.
DB and BM contributed equally.
Contributors HV and LS: involved in data collection, study design, manuscript preparation and statistical analysis. ZD, CC, AT, FIS and GB: involved in data collection and manuscript review. VAG: involved in statistical support and manuscript preparation. DB and BM: involved in study design and manuscript review.
Funding This study was supported by the National Research, Development and Innovation Office of Hungary (NKFIA; NVKP_16-1-2016-0017 National Heart Programme). This research was financed by the Higher Education Institutional Excellence Programme of the Ministry for Innovation and Technology in Hungary within the framework of the Therapeutic Development Thematic Programme of Semmelweis University.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Patient consent for publication Not required.
Ethics approval Ethical approval was obtained from the Hungarian National Institute of Pharmacy and Nutrition (OGYEI/29206-4/2019) in correspondence with the ethical standards laid down in the 1964 Declaration of Helsinki and its later amendments
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available on reasonable request. Please contact the corresponding author.