Article Text

Abstract
Background Lipoprotein-associated phospholipase A2 (Lp-PLA2) activity has been shown to predict calcific aortic valve stenosis (CAVS) outcomes. Our objective was to test the association between plasma Lp-PLA2 activity and genetically elevated Lp-PLA2 mass/activity with CAVS in humans.
Methods and results Lp-PLA2 activity was measured in 890 patients undergoing cardiac surgery, including 476 patients undergoing aortic valve replacement for CAVS and 414 control patients undergoing coronary artery bypass grafting. After multivariable adjustment, Lp-PLA2 activity was positively associated with the presence of CAVS (OR=1.21 (95% CI 1.04 to 1.41) per SD increment). We selected four single nucleotide polymorphisms (SNPs) at the PLA2G7 locus associated with either Lp-PLA2 mass or activity (rs7756935, rs1421368, rs1805017 and rs4498351). Genetic association studies were performed in eight cohorts: Quebec-CAVS (1009 cases/1017 controls), UK Biobank (1350 cases/349 043 controls), European Prospective Investigation into Cancer and Nutrition-Norfolk (504 cases/20 307 controls), Genetic Epidemiology Research on Aging (3469 cases/51 723 controls), Malmö Diet and Cancer Study (682 cases/5963 controls) and three French cohorts (3123 cases/6532 controls), totalling 10 137 CAVS cases and 434 585 controls. A fixed-effect meta-analysis using the inverse-variance weighted method revealed that none of the four SNPs was associated with CAVS (OR=0.99 (95% CI 0.96 to 1.02, p=0.55) for rs7756935, 0.97 (95% CI 0.93 to 1.01, p=0.11) for rs1421368, 1.00 (95% CI 1.00 to 1.01, p=0.29) for rs1805017, and 1.00 (95% CI 0.97 to 1.04, p=0.87) for rs4498351).
Conclusions Higher Lp-PLA2 activity is significantly associated with the presence of CAVS and might represent a biomarker of CAVS in patients with heart disease. Results of our genetic association study suggest that Lp-PLA2 is however unlikely to represent a causal risk factor or therapeutic target for CAVS.
- aortic stenosis
- coronary artery disease
Statistics from Altmetric.com
Introduction
Calcific aortic valve stenosis (CAVS) is the most common form of heart valve disease and currently affects almost 3% of the population older than 65.1 2 Replacement of the aortic valve is the only effective treatment for CAVS. Similar to atherosclerosis or coronary artery disease (CAD), the molecular mechanisms that initiate CAVS include infiltration of oxidised lipids, lipoproteins and inflammatory cells, as well as extracellular matrix remodelling, degradation and calcification. CAD and CAVS also share similar clinical risk factors. In a large population-based study, we showed that risk factors associated with poor cardiovascular health (an unhealthy diet, physical inactivity, smoking, obesity, type 2 diabetes, hypertension and hypercholesterolaemia, often referred to as Life’s Simple 7) are associated with CAVS incidence.3 Despite the important overlap between the pathobiological mechanisms and clinical risk factors between CAD and CAVS, traditional CAD treatments have so far been ineffective in treating CAVS. Low-density lipoprotein (LDL) cholesterol-lowering therapies such as statins and ezetimibe had no effect on the prevention and treatment of CAVS in previous studies.4–6 Whether other cardiovascular drugs under development could be effective for the treatment of CAVS is unknown.
Lipoprotein-associated phospholipase A2 (Lp-PLA2) was suggested as a driver of aortic valve calcification.7 In a prospective observational study of patients with mild to moderate CAVS, Lp-PLA2 activity was shown to be a predictor of CAVS progression.8 An important proportion of Lp-PLA2 in the bloodstream can be found on LDL and lipoprotein(a) (Lp(a)) particles, and both elevated LDL cholesterol and Lp(a) levels are potentially causal risk factors for the development of CAVS.9–12 However, the causality of Lp-PLA2 in the aetiology of CAVS has not been established, and whether Lp-PLA2 inhibitors such as darapladib could be used for the prevention and/or treatment of CAVS is unknown. On the other hand, the causality of Lp-PLA2 in cardiovascular disease (CVD) prevention was severely questioned following the publication of two large trials showing no effect of darapladib treatment on cardiovascular events and by the lack of association between genetic variants influencing Lp-PLA2 mass/activity and CVD.13
The objective of this study was to assess the relationship between Lp-PLA2 activity and the presence of CAVS in patients with documented heart disease undergoing cardiac surgery. We also sought to determine whether the relationship between Lp-PLA2 and CAVS risk was potentially causal by examining genetic variants at the PLA2G7 locus associated with circulating Lp-PLA2 mass or activity in patients undergoing cardiac surgery as well as in the general population.
Methods
Laboratory analyses and study population (biomarker study)
Lp-PLA2 activity was measured by a commercial colorimetric activity method (platelet-activating factor acetylhydrolase (PAF-AH) assay kit, Cayman Chemical, Ann Arbor, Michigan) in patients undergoing heart surgery at the Institut universitaire de cardiologie et de pneumologie de Québec (IUCPQ), Québec, Canada. Briefly, the assay uses 2-thio PAF, which serves as a substrate for all PAF-AHs. On hydrolysis of the acetyl thioester bond at the sn-2 position by PAF-AH, free thiols are detected using 5,5’dithio-bis-(2-nitrobenzoic acid), which absorbs 412 nm wavelength light. The intra-assay and interassay coefficients of variation were both below 10%. Only patients with a tricuspid aortic valve were selected in order to study a homogeneous population. These patients were compared with controls scheduled for a coronary artery bypass grafting who had no valvular heart disease (including no aortic sclerosis) at preoperative echocardiography. Patients with moderate to severe aortic and/or mitral valve regurgitation (grade >2) were excluded. Patients with a history of rheumatic disease, endocarditis and inflammatory diseases were also excluded. All patients signed a written informed consent.
Study populations and single nucleotide polymorphism selection (genetic association study)
Genetic association studies were performed in eight cohorts: Quebec-CAVS (1009 CAVS cases and 1017 controls), UK Biobank (1350 CAVS cases and 349 043 controls), European Prospective Investigation into Cancer and Nutrition-Norfolk (504 CAVS cases and 20 307 controls), Genetic Epidemiology Research on Aging (GERA) (3469 CAVS cases and 51 723 controls), Malmö Diet and Cancer Study (682 CAVS cases and 5963 controls) and three French cohorts (3123 CAVS cases and 6532 controls), totalling 10 137 CAVS cases and 434 585 controls. The cohorts are described in detail in the online supplementary file. Single nucleotide polymorphisms (SNPs) were selected based on their association with Lp-PLA2 mass or activity levels in the study of Grallert et al.14 This meta-analysis included data from five community-based cohorts from the USA and Europe as part of the Cohorts for Heart and Aging Research in Genetic Epidemiology (CHARGE) consortium, including 13 664 subjects. Lp-PLA2 activity was assessed in the Cardiovascular Health Study (CHD), Framingham Heart Study (FHS) and Rotterdam Study using a colorimetric method (diaDexus CAM Kit, diaDexus, San Francisco, California, USA) or a radioactive method (Perkin Elmer Life Sciences, Waltham, Massachusetts, USA). Lp-PLA2 mass concentration was measured in the Atherosclerosis Risk in Communities, CHD, FHS and Cooperative Health Research in the Region of Augsburg studies using a commercial sandwich enzyme immunoassay (PLAC Test, diaDexus). Genotyping was performed using high-throughput assays and genetic imputation was performed to obtain results on >2.5 million SNPs. The SNP–phenotype association (Lp-PLA2 mass/activity) was performed using linear regression on log-transformed values in an additive model adjusted for age, sex and, if applicable, recruitment site. There was no sample overlap between the cohorts used to derive the exposure and the outcomes. We selected genome-wide significant and independent SNPs (r2 <0.40) at the PLA2G7 locus to increase the probability of true effects (table 1). We investigated the association between the four selected SNPs (two associated with Lp-PLA2 mass and two associated with Lp-PLA2 activity) at the PLA2G7 locus and CAVS in eight cohorts (described in the online supplementary data file). All patients provided informed consent.
Supplemental material
SNPs included in the genetic association study
Statistical analyses
Differences between biomarker levels in patients with versus without CAVS were tested using one-way analyses of variance and unpaired t-tests. The association between measured Lp-PLA2 activity and the presence of CAVS was determined using logistic regression and OR for an increment of 1 SD unit before and after adjusting for cardiovascular risk factors (age, sex, body mass index, diabetes, smoking, lipid-lowering therapy use and creatinine levels). Lp-PLA2 activity was transformed into a z score (z=(x-mean(x))/SD(x)) to fit the logistic model. For each of the four selected SNPs, we used logistic regression models to verify their association with CAVS per allele in each cohort. Models were adjusted for age, sex and the first 10 ancestry-based principal components when available. In the GERA cohort, genetic variants were modelled using PLINK2 in logistic regression models adjusted for age, age squared and sex. In the French cohorts, models were not adjusted for age. We performed a fixed-effect meta-analysis using the inverse-variance weighted method as implemented in the rmeta package (V.3.0) in R (V.3.3.1). Genetic study power was calculated using QUANTO V.1.2.4 with a log-additive mode of inheritance using allele frequencies provided in table 1, with the unmatched case–control ratio of our study cohorts and a two-tailed p value threshold of 0.05. Statistical analyses were performed with R.
Results
Lp-PLA2 activity and CAVS
The clinical characteristics of the study participants included in the biomarker study are presented in table 2. By design, the proportion of patients with CAD was higher in controls compared with cases. The mean Lp-PLA2 activity was higher in patients with CAVS compared with controls (figure 1).

Lp-PLA2 activity in patients with versus without calcific aortic valve stenosis. *P=4.3×10−5. Lp-PLA2, lipoprotein-associated phospholipase A2.
Clinical characteristics of study participants
Table 3 presents the positive association between higher Lp-PLA2 activity and the presence of CAVS. The association between Lp-PLA2 activity and CAVS remained significant after adjusting for potential confounders (age, sex, body mass index, diabetes, smoking, lipid-lowering therapy use and creatinine levels).
Association between Lp-PLA2 activity and CAVS risk
Genetic variants at the PLA2G7 locus, CAVS and aortic valve calcium
The association between each SNP at the PLA2G7 locus and CAVS is presented in figure 2. None of the Lp-PLA2 mass/activity raising SNPs was significantly associated with CAVS in the individual cohorts or in the meta-analysis. We found no evidence of heterogeneity across these meta-analyses (p value for heterogeneity >0.05 for all). In addition, none of the selected SNPs showed a significant association with aortic valve calcification assessed by CT and defined by an Agatston score >0 in 6942 participants from the CHARGE consortium: p values for rs7756935, rs1421368, rs1805017 and rs4498351 were 0.15, 0.71, 0.99 and 0.052, respectively. To determine whether SNPs included in this analysis showed pleiotropic associations, we used the PhenoScanner,15 16 an online tool that provides the phenotypic spectrum of these SNPs. The results presented in online supplementary table 1 suggest no association between these SNPs and traits (other than Lp-PLA2 mass/activity) at p<1.05E−5, with the exception of rs1421368 associated with viral infections of unspecified site in the UK Biobank.

Meta-analysis of the per-allele association between four single nucleotide polymorphisms associated with Lp-PLA2 mass and/or activity and CAVS risk. CAVS, calcific aortic valve stenosis; EPIC, European Prospective Investigation into Cancer and Nutrition; GERA, Genetic Epidemiology Research on Aging; Lp-PLA2, lipoprotein-associated phospholipase A2; MDCS, Malmö Diet and Cancer Study.
Discussion
Lp-PLA2 is an enzyme that hydrolyses oxidised phospholipids (Ox-PL) into lysophosphatidylcholine (lyso-PC), which is an important chemoattractant and proinflammatory mediator. Lp-PLA2 is secreted by inflammatory cells and is transported into the bloodstream by atherogenic lipoprotein particles such as LDL and Lp(a). Lp(a) is an important likely causal risk factor for CAVS. On top of Lp-PLA2, Lp(a) transports Ox-PL in the blood. Given the lack of a causal association between genetically elevated Lp-PLA2 mass/activity and CAVS, we believe that Lp(a) might drive the initiation and progression of CAVS via mechanisms that are independent of Lp-PLA2, such as Ox-PL-mediated inflammation and calcification.
Prospective observational studies have shown that circulating Lp-PLA2 mass and/or activity is associated with CAD risk.17 18 For instance, in a meta-analysis that included more than 79 000 participants in 32 prospective studies, a continuous association between Lp-PLA2 activity and risk of coronary heart disease was observed. In that study a relative increase in risk of 1.10 (95% CI 1.05 to 1.16) for each 1 SD increase in Lp-PLA2 activity was observed after adjustment for conventional risk factors.19 The possibility that Lp-PLA2 might be causally related to atherosclerosis was further supported by treatment with the Lp-PLA2 inhibitor darapladib in a porcine model.20 In that study, in diabetic pigs fed a hyperlipidaemic diet, treatment with darapladib (n=20) reduced the development of coronary atherosclerosis and inhibited the subsequent progression to advanced lesions, resulting in a more stable plaque phenotype compared with control pigs treated with placebo (n=17). A marked reduction in necrotic core development and a change in arterial lesion composition were observed following Lp-PLA2 inhibition. Following these promising observations, two large-scale cardiovascular outcomes trials that documented the impact of the Lp-PLA2 inhibitor darapladib on health outcomes were launched. In both studies, however, treatment of patients with stable coronary heart disease (STABILITY trial)21 or acute coronary syndrome (SOLID-TIMI 52 trial)22 did not lead to reductions in cardiovascular outcomes, which has left many to suggest that Lp-PLA2 might simply represent a biomarker of, rather than a causal risk factor of, CAD. This observation was further supported by the results of Mendelian randomisation studies. Mendelian randomisation relies on the random assortment of alleles during meiosis to divide a population into groups with and without an elevation in a risk factor. The random distribution of inherited variants affecting the risk factor minimises the possibility that reverse causation or confounding is responsible for the association between the risk factor and the outcome. Mendelian randomisation had ‘predicted the failure’ of Lp-PLA2 inhibition for atherosclerotic cardiovascular diseases (ACVD) risk reduction by providing evidence that variants at the PLA2G7 locus associated with lifelong reductions in Lp-PLA2 mass or activity were not associated with cardioprotection.23 24
Lp-PLA2 is involved in aortic valve mineralisation. A recent transcriptomic study by Mahmut et al 7 revealed that the expression of Lp-PLA2 was increased more than fourfold in calcified aortic valves compared with normal aortic valves in humans. In the same report, it was documented that lyso-PC induced mineralisation and apoptosis of the human valvular interstitial cells in vitro. A small study showed that Lp-PLA2 levels were higher in patients with CAVS compared with participants without CAVS.25 Our group also showed that higher Lp-PLA2 activity was associated with the progression of CAVS8 and the structural degeneration of bioprostheses.26
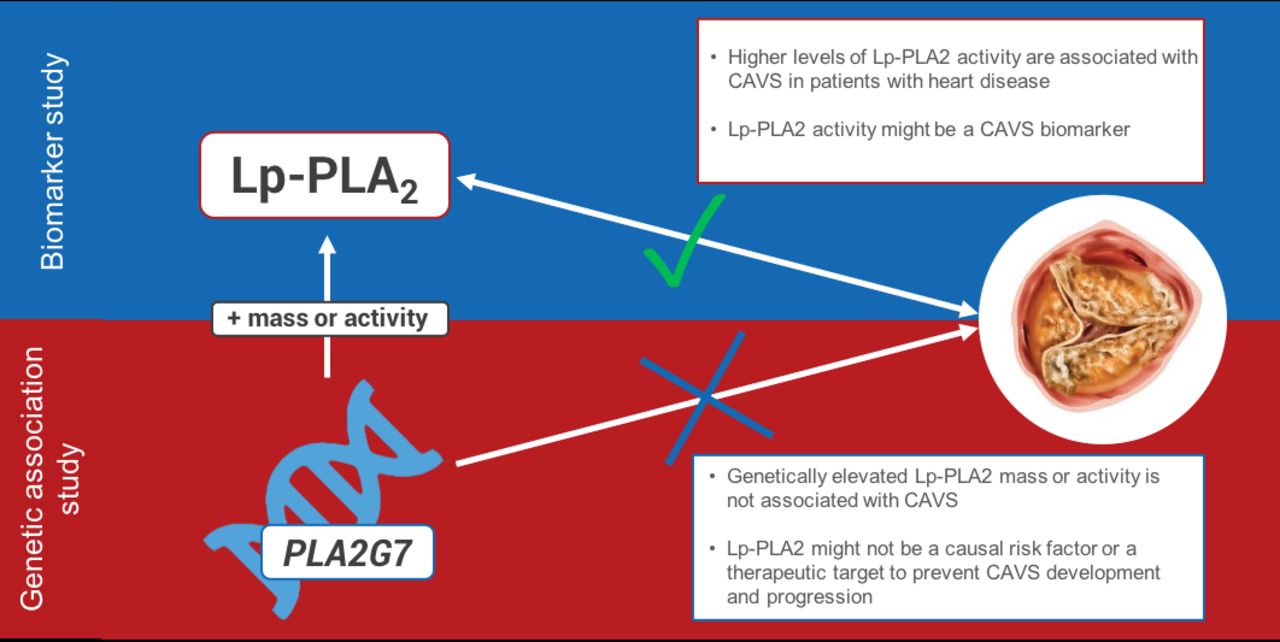
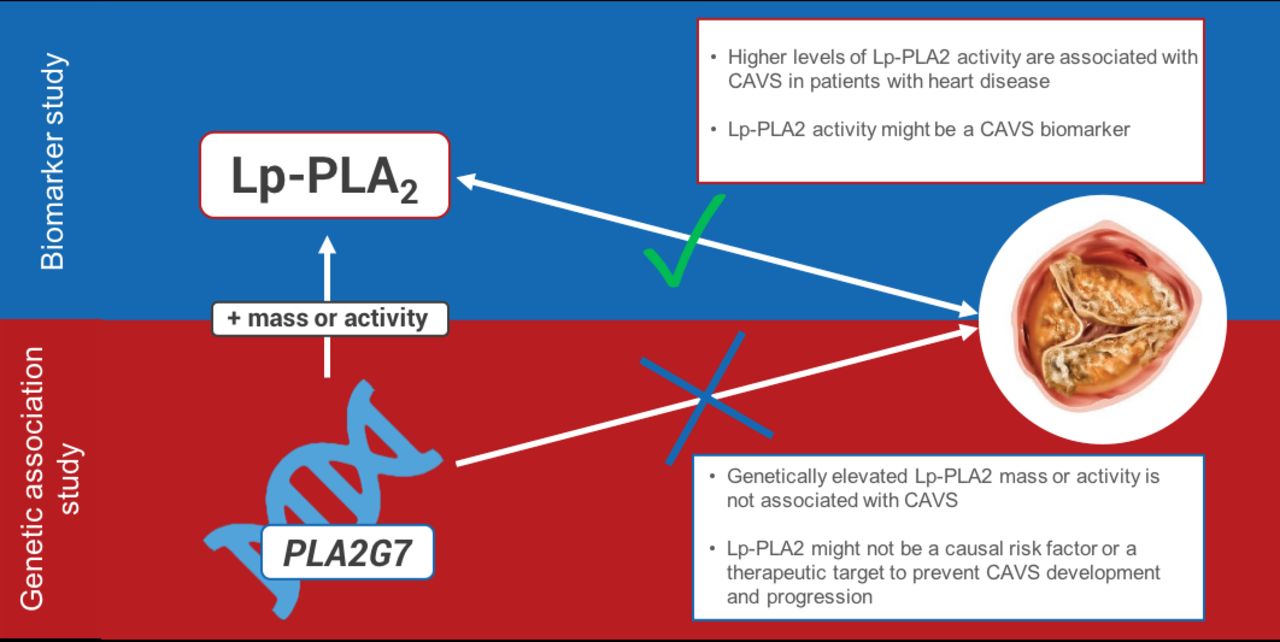
The present study shows that elevated Lp-PLA2 activity is associated with CAVS, even when compared with patients with documented CAD, thereby suggesting that Lp-PLA2 activity might be a stronger marker of the presence of CAVS compared with CAD. However, we found no association between genetic variants at the PLA2G7 locus that are associated with Lp-PLA2 mass or activity and CAVS in eight cohorts. Consequently, Lp-PLA2 mass or activity is unlikely to represent a causal risk factor or therapeutic target for CAVS (figure 3).
{kind=link}
{kind=link}
{kind=link}
Higher Lp-PLA2 activity is significantly associated with the presence of CAVS in patients with heart disease, but variants influencing Lp-PLA2 mass or activity are not associated with CAVS in this large genetic association study. CAVS, calcific aortic valve stenosis; Lp-PLA2, lipoprotein-associated phospholipase A2.
Previous Mendelian randomisation studies on CAD have used rare loss-of-function mutations with large effect on Lp-PLA2 activity (up to 94%) and/or common variants with modest impact on the risk factor. Limitations of our study include the low absolute effects on Lp-PLA2 activity/mass of our selected SNPs. However, the per-allele effects of the two SNPs, rs7756935 and rs1421368, associated with Lp-PLA2 activity used in the genetic study correspond, respectively, to 34% and 43% of the difference of Lp-PLA2 activity observed between cases and controls in our biomarker study. It is also worth mentioning that the effects of these variants on Lp-PLA2 mass or activity are lifelong effects. As CAVS is a less prevalent medical condition than ACVD, and mutations with large effects on Lp-PLA2 are extremely rare, we could not use genetic instruments with a large effect on the biomarker. To our knowledge, our present study has the largest number of CAVS cases collected in a genetic association study. Our sample size had 80% power to detect per-allele OR for CAVS of 1.05, 1.07, 1.05 and 1.04, respectively, for rs7756935, rs1421368, rs1805017 and rs4498351. It must also be mentioned, however, that individuals included in this study were all of European ancestry. Therefore, caution is warranted prior to generalising these findings to populations from other ethnic backgrounds. This limitation also applies to our observational study. Additional limitations of our observational study include the presence of a control group of patients with CAD and the fact that Lp-PLA2 activity but not mass was measured. Although the inclusion of our control of patients with CAD enabled us to study the association of Lp-PLA2 activity with CAVS possibly independently of the presence/absence of CAD, we believe that additional studies including healthy controls and measuring both Lp-PLA2 mass and activity would be required to confirm and extend our findings.
The present study further consolidates the strong association between elevated Lp-PLA2 activity and CAVS by reporting this association in a population with a high prevalence of ACVD. However, the lack of association between variants influencing Lp-PLA2 mass or activity and CAVS suggests that, as shown for CAD, elevated Lp-PLA2 is more likely to represent a biomarker for CAVS rather than a causal risk factor.
Key messages
What is already known on this subject?
Lipoprotein-associated phospholipase A2 (Lp-PLA2) activity has been shown to predict calcific aortic valve stenosis (CAVS) outcomes.
What might this study add?
The results of our observational study suggest that Lp-PLA2 activity could represent an independent biomarker for CAVS.
However, we show for the first time that genetic variants influencing Lp-PLA2 mass or activity are not associated with CAVS in this large genetic association study.
How might this impact on clinical practice?
Lp-PLA2 might represent a biomarker for the presence of CAVS.
The results of our genetic association study suggest that inhibition of Lp-PLA2 activity might not be beneficial for CAVS prevention and/or treatment.
References
Footnotes
Twitter @none, @PPibarot, @ArsenaultBenoit
Contributors All authors have contributed to the manuscript with either substantial contributions to the conception or design of the work, or acquisition, analysis or interpretation of data. All authors have contributed to the first draft of the work or revising it critically for important intellectual content. They all gave final approval of the version published.
Funding This study was supported by grants from the Fondation de l’IUCPQ and the Canadian Institutes of Health Research (CIHR) (awarded to BA (FRN149068 and FRN155226) and YB (MOP102481 and MOP137058)) and by the Heart and Stroke Foundation of Canada (awarded to YB (PJT153396)). The COFRASA (NCT00338676) and GENERAC (NCT00647088) studies are supported by grants from the Assistance Publique - Hôpitaux de Paris (PHRC National 2005 and 2010 and PHRC Régional 2007). BA, ST and M-AC hold junior scholar awards from the Fonds de recherche du Québec: Santé (FRQS). PM holds an FRQS Research Chair on the Pathobiology of Calcific Aortic Valve Disease. His research programme is supported by the Canadian Institutes of Health Research grants (FRN148778, FRN159697). PP holds the Canada Research Chair in Valvular Heart Disease, and his research programme is supported by a Foundation Scheme Grant from CIHR. YB holds a Canada Research Chair in Genomics of Heart and Lung Diseases. JJS is supported by an ANR and FRM grant (13-BSV6-0011, DCV20070409278). TLT is supported by the Fédération Française de Cardiologie, a Fondation Coeur et Recherche and an Inserm Translational Research grant. RC is supported by a 'Connect Talent' research chair from Région Pays de la Loire and Nantes Métropole. JGS was supported by grants from the Swedish Heart-Lung Foundation (2016-0134 and 2016-0315), the Swedish Research Council (2017-02554), the European Research Council (ERC-STG-2015-679242), the Crafoord Foundation, Skåne University Hospital, the Scania County, governmental funding of clinical research within the Swedish National Health Service, a generous donation from the Knut and Alice Wallenberg Foundation to the Wallenberg Centre for Molecular Medicine in Lund, and funding from the Swedish Research Council (Linnaeus grant Dnr 349-2006-237, Strategic Research Area Exodiab Dnr 2009-1039) and the Swedish Foundation for Strategic Research (Dnr IRC15-0067) to the Lund University Diabetes Centre. GT is supported by R01 HL128550 from the NIH/NHLBI.
Competing interests BA has received research funding from Pfizer, Merck and Ionis Pharmaceuticals and is a consultant for Novartis. PM is a consultant for Casebia Therapeutics.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Patient consent for publication Not required.
Ethics approval For the biomarker study, the study protocol was approved by the Ethics Committee of the IUCPQ. For the genetic association study, all study protocols were approved by the local ethics committees.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement No data are available.