Article Text

Abstract
Objective To evaluate whether the use of dipeptidyl peptidase-4 (DPP-4) inhibitors and their cardiac tissue distribution profile and anticalcification abilities are associated with risk of aortic stenosis (AS) progression.
Methods Out of the five different classes of DPP-4 inhibitors, two had relatively favourable heart to plasma concentration ratios and anticalcification ability in murine and in vitro experiments and were thus categorised as ‘favourable’. We reviewed the medical records of 212 patients (72±8 years, 111 men) with diabetes and mild-to-moderate AS who underwent echocardiographic follow-up and classified them into those who received favourable DPP-4 inhibitors (n=28, 13%), unfavourable DPP-4 inhibitors (n=69, 33%) and those who did not receive DPP-4 inhibitors (n=115, 54%).
Results Maximal transaortic velocity (Vmax) increased from 2.9±0.3 to 3.5±0.7 m/s during follow-up (median, 3.7 years), and the changes were not different between DPP-4 users as a whole and non-users (p=0.143). However, the favourable group showed significantly lower Vmax increase than the unfavourable or non-user group (p=0.018). Severe AS progression was less frequent in the favourable group (7.1%) than in the unfavourable (29.0%; p=0.03) or the non-user (29.6%; p=0.01) group. In Cox regression analysis after adjusting for age, baseline renal function and AS severity, the favourable group showed a significantly lower risk of severe AS progression (HR 0.116, 95% CI 0.024 to 0.551, p=0.007).
Conclusions DPP-4 inhibitors with favourable pharmacokinetic and pharmacodynamic properties were associated with lower risk of AS progression. These results should be considered in the preparation of randomised clinical trials on the repositioning of DPP-4 inhibitors.
- aortic stenosis
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Calcific aortic stenosis (AS) is the most common valvular heart disease in developed countries, but there are currently no effective medical treatments that can stop or delay AS progression.1 The only available treatment option is replacing the aortic valve by open heart surgery or transcatheter valve implantation in patients with severe AS, which routinely allows the development of an end-stage, irreversible disease. The aortic valve had been traditionally regarded as a metabolically inactive tissue, and clinicians thus believed that AS is a typical example of a degenerative disease associated with ageing. However, the identification of valvular interstitial cells (VICs) with potential to differentiate into osteoblast-like cells in human aortic valves resulted in a major paradigm shift, and AS is now regarded as a metabolically active disease.2
Our group recently reported that endothelial dysfunction in aortic valve leads to increased expression of dipeptidyl peptidase-4 (DPP-4), which induces the degradation of insulin-like growth factor-1 (IGF-1) and subsequent osteogenic differentiation of VICs.3 As DPP-4 inhibitors are currently used for management of type 2 diabetes, researchers have suggested that DPP-4 inhibitors may be repositioned to manage other diseases including AS.3 4 Analysing clinical data from patients with diabetes who received DPP-4 inhibitors may provide valuable information on whether DPP-4 inhibitors may be useful for preventing AS progression. We thus evaluated the factors that are potentially associated with the therapeutic efficacy of DPP-4 inhibitors for AS. Specifically, we tested whether the cardiac tissue distribution profile of DPP-4 inhibitors and their direct anticalcification effect on VICs are associated with efficacy.
Methods
Experimental animals
The animal (Sprague-Dawley rat) was a standard species routinely used in pharmacokinetic evaluations, and the number of animals used in the study was the minimum necessary to properly perform plasma pharmacokinetic evaluation.
We tested the cardiac tissue distribution of eight different DPP-4 inhibitors using male Sprague-Dawley rats (7–9 weeks old), which were equally divided according to each inhibitor (online supplementary table 1). The DPP-4 inhibitors were weighed and mixed with appropriate volume (1 mL/kg) of vehicle to obtain uniform clear solutions. Two 20 µL aliquots of each formulation were used for dose validation by either liquid chromatography with ultraviolet detection (LC/UV) or liquid chromatography with tandem mass spectrometry (LC-MS/MS). The solutions were prepared on the day of dosing and were administered via the tail vein within 4 hours after preparation (online supplementary data). We also tested in vitro the anticalcifying efficacy of eight DPP-4 inhibitors (five of which were used in the retrospective patient study) using human aortic VICs (online supplementary table 1).
Supplemental material
We assumed that the concentration of DPP-4 inhibitors within the heart would have to be higher than the half-maximal anticalcifying effective concentration (EC50) in order to exert a significant effect on aortic VICs. Thus, using both pharmacokinetic and pharmacodynamic data,5 we calculated the adjusted H:P ratio (heart to plasma concentration ratio at 4 hours × [heart concentration at 4 hours/EC50]) for each DPP-4 inhibitor to compare their theoretical efficacy on VICs to prevent AS progression.
Patient data
Electronic medical records and echocardiographic database of three tertiary referral hospitals in South Korea (Asan Medical Center, Seoul; Samsung Medical Center, Seoul; Seoul National University Bundang Hospital, Gyeonggi-do) from 2009 and 2016 were retrospectively screened to identify patients with type 2 diabetes with mild-to-moderate AS. Mild-to-moderate AS was defined as initial maximal transaortic velocity (Vmax) between 2.5 and 3.5 m/s and normal left ventricular systolic function (left ventricular ejection fraction >50%). We further screened for patients who underwent follow-up echocardiographic examination at intervals of more than 2 years. Exclusion criteria included the presence of other haemodynamically significant valvular lesions that may affect the Vmax, decreased left ventricular systolic function by more than 10% during the follow-up and end-stage renal disease. Patients who did not receive specific diabetes medication during echocardiographic follow-up duration were also excluded. The flow diagram for patient selection is shown in figure 1. The need for informed consent was waived due to the retrospective nature of the study.

Patient flow diagram. AS, aortic stenosis; DM, diabetes mellitus; DPP-4, dipeptidyl peptidase-4.
From the electronic medical records, we extracted the demographic information, blood test results and diabetes medications of the patients. We also extracted echocardiographic data regarding AS severity; Vmax and peak transaortic pressure gradient were, respectively, defined as the highest velocity and pressure gradient obtained from multiple windows. The mean pressure gradient was determined by tracing the contour of the aortic jet obtained by continuous-wave Doppler imaging. Progressions of AS severity—annual changes in Vmax as well as peak and mean pressure gradients—were calculated using the final echocardiographic data from baseline assessments. Systematic case report forms were filled by dedicated research nurses and physicians. Clinical follow-up data were included in the case report forms. Development of clinical events included progression to severe AS (defined as follow-up Vmax ≥4 m/s) and aortic valve intervention by either surgical or transcatheter replacement.
Patient and public involvement
Patients were not involved in the study design.
Statistical analysis
Patient characteristics were compared using the χ2 test or the Student’s t-test between the non-user and user of DPP-4 inhibitors. Discrete variables were reported as numbers with percentages and continuous variables were expressed as mean and SD. For comparison of annual progression of AS severity, analysis of variance test was performed among the three groups of study population (non-user group, favourable DPP-4 inhibitor group and unfavourable DPP-4 inhibitor group). To minimise the baseline differences between patients who received favourable DPP-4 inhibitors and those without, a propensity score matching was used using a logistic model including age, sex, dyslipidaemia, coronary artery disease, baseline glomerular filtration rate, baseline aortic valve mean pressure gradient, follow-up duration, and use of statin and antidiabetic drugs (sulfonylurea, metformin or insulin) as covariates. After calculating the predicted probabilities, we matched each favourable DPP-4 inhibitor user (n=25) to two non-user groups (n=50) using the Greedy algorithm (online supplementary table 2). Model discrimination was assessed with C statistics (0.776), and model calibration was assessed with Hosmer-Lemeshow statistics (χ2=7.2941, df=8, p=0.5053). Multivariate analysis was performed with adjustment of covariance; covariates of p<0.1 and considered to be clinically significant were included in the model. The Tukey-Kramer method was applied to the post-hoc analysis for pairwise comparisons between the groups. Cox regression models were constructed to determine the factors associated with progression to severe AS. In the multivariate model, the covariates considered to be clinically significant were added. The final model included age, use of favourable or non-favourable DPP-4 inhibitors, baseline AS severity, and renal function. The probability of significance was judged based on p<0.05. All statistical analyses were performed using the SAS V.9.4 software.
Results
Anticalcification effect and cardiac tissue distribution profiles of DPP-4 inhibitors
Online supplementary table 1 shows the pharmacokinetic and pharmacodynamic profiles of each DPP-4 inhibitor, including the EC50 of anticalcification and the absolute heart and plasma concentrations at 1 and 4 hours after intravenous injection in rats. We selected five DPP-4 inhibitors used in our patient cohort, and their pharmacokinetic and pharmacodynamic properties are illustrated in figure 2. Most of the DPP-4 inhibitors significantly attenuated the osteogenic changes in human VICs from patients with AS (figure 2A). The H:P ratios of linagliptin and gemigliptin were significantly higher than those of alogliptin, sitagliptin and vildagliptin (figure 2B). When the ratio was adjusted by weighing on the absolute tissue concentration relative to the EC50 for anticalcification, the difference became greater (figure 2C,D). We thus classified the DPP-4 inhibitors as favourable (linagliptin and gemigliptin) and unfavourable (alogliptin, sitagliptin and vildagliptin) in the subsequent analysis. Of the eight DPP-4 inhibitors, evogliptin had the highest adjusted H:P ratio (online supplementary table 1), although this was not used in any of the patients in the clinical study.
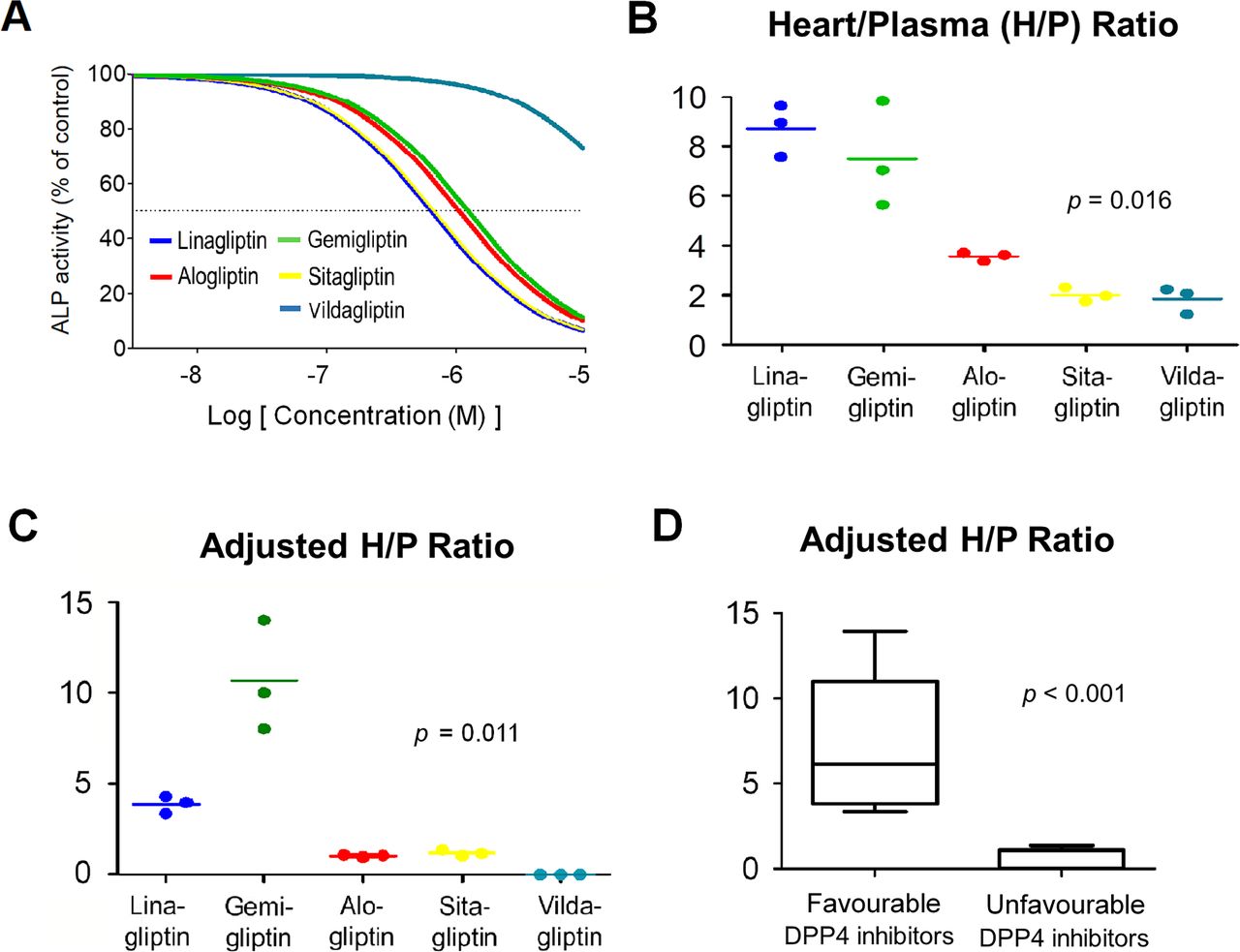
Results of the pharmacokinetic and pharmacodynamic tests. (A) The dose–response curves for alkaline phosphatase (ALP) activity of human valvular interstitial cells (hVICs) after treatment with dipeptidyl peptidase-4 (DPP-4) inhibitors after 1 week of osteogenic stimulation. (B) Heart to plasma concentration (H:P) ratio of the DPP-4 inhibitors at 4 hours after intravenous injection in rats (n=3 for each drug). (C,D) Adjusted H:P ratio of favourable (linagliptin and gemigliptin) and unfavourable (alogliptin, sitagliptin and vildagliptin) DPP-4 inhibitors.
Patients with diabetes and mild-to-moderate AS
A total of 1081 patients with mild-to-moderate AS and normal left ventricular systolic function were initially screened, and after applying the exclusion criteria 212 patients (mean age, 72±8 years; 111 men) were included in the analysis. One hundred and fifteen patients (54%) did not receive DPP-4 inhibitors (non-user group); 28 (13%) and 69 (33%) patients had received favourable and unfavourable DPP-4 inhibitors, respectively (figure 1).
Baseline clinical and echocardiographic characteristics are summarised in table 1. There were no significant differences in clinical risk factors among the three groups, except antidiabetic drugs including insulin. Nonetheless, the baseline and follow-up haemoglobin A1c were not significantly different among the groups. Age, sex, presence of coronary artery disease, use of statin and baseline estimated glomerular filtration rates, as well as use of metformin, sulfonylurea and insulin, were considered potential confounding variables and their effects were adjusted in the following analyses.
Comparison of patient baseline characteristics
AS progression
Baseline Vmax and AS severity were not significantly different among the three groups and the mean baseline Vmax was 2.9±0.3 m/s (table 1). During a median echocardiographic follow-up of 3.7 years (IQR 2.8–5.1 years), Vmax increased to 3.5±0.7 m/s. The annual change in Vmax was not significantly different between the DPP-4 inhibitor user group and the non-user group (14.3±16.0 vs 17.8±17.1 cm/s/year, p=0.143) (online supplementary table 3). However, the favourable group showed significantly lower Vmax increase compared with the unfavourable group or non-user group (overall p=0.018). The annual change of mean (p=0.015) and peak (p=0.027) pressure gradient showed similar trends (table 2 and figure 3). In the post-hoc analysis, the favourable DPP-4 inhibitor group showed significantly lower Vmax change (8.0±13.0 cm/s/year) compared with the non-user group (17.8±17.1 cm/s/year, p=0.014) or the unfavourable group (16.9±15.9 cm/s/year, p=0.039) (online supplementary table 4). The differences were significant after adjustment for age, sex, coronary artery disease, use of statin, baseline estimated glomerular filtration rate level, and use of metformin, sulfonylurea and insulin (table 2 and online supplementary table 4). After propensity matching, use of favourable DPP-4 inhibitor was associated with significantly lower annual change of Vmax and mean and peak pressure gradient (online supplementary table 5).

Changes of maximal transaortic valve velocity (A), mean (B) and peak (C) pressure gradient according to medications. Turkey’s method was used to make box plots. DPP-4, dipeptidyl peptidase-4.
Haemodynamic progression of aortic stenosis according to use of antidiabetic drugs
During a median follow-up of 5.0 years (IQR 3.6–6.7 years), progression to severe AS was confirmed in 56 (26.4%) patients, of whom 27 underwent aortic valve intervention. In the non-user group, 34 (29.6%) had AS progression and 14 (12.2%) underwent aortic valve intervention; in the unfavourable group, 20 (29.0%) had severe AS progression and 11 (15.9%) underwent aortic valve intervention. In contrast, two (7.1%) patients had severe AS progression and underwent intervention in the favourable group. Thus, the favourable group had a significantly lower proportion of patients with severe AS progression than the non-user group (p=0.01) or the unfavourable group (p=0.03). In Cox regression analysis after adjusting for age, baseline renal function and baseline AS severity, use of favourable DPP-4 inhibitor had a significantly lower risk of progression to severe AS (adjusted HR 0.116, 95% CI 0.024 to 0.551, p=0.007) (table 3 and figure 4).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Risk of progression to severe aortic stenosis after adjustment for age, baseline renal function and baseline severity of aortic stenosis according to diabetes medication. DPP-4, dipeptidyl peptidase-4.
Cox proportional regression models for aortic stenosis progression
Discussion
In our study, we categorised five DPP-4 inhibitors into favourable and unfavourable according to anticalcification abilities and cardiac tissue distribution profiles. Importantly, we found that among patients with diabetes and mild-to-moderate AS, those who received favourable DPP-4 inhibitors (ie, inhibitors with high anticalcification ability and high H:P ratios) had significantly lower degree of increase in Vmax as well as lower frequency of AS progression and aortic valve intervention than those who received unfavourable DPP-4 inhibitors or did not receive DPP-4 inhibitors. These results warrant the need for clinical trials on the repositioning of DPP-4 inhibitors for the management of AS.
AS is a progressive condition characterised by long asymptomatic phase; accordingly, AS has been traditionally regarded as a typical disease entity of prolonged ‘wear and tear’. Nevertheless, recent molecular studies showed that aortic valve has VICs with unique homeostatic mechanisms, and that valvular degeneration starts with active inflammation involving biochemical, humoral and genetic factors.6 As lipid-lowering agents failed to show efficacy in preventing AS progression,7–9 researchers have investigated potential therapeutic molecular targets including lipoprotein (a),10 11 apolipoprotein B oxidised phospholipid12 and interleukin 11.13 Similarly, the target of medical interventions has greatly expanded and ranges from the classic calcification (SALTIRE 2 trial using denosumab or bisphosphonate; NCT02132026) to the matrix before calcification (BASIK 2 trial targeting matrix γ-carboxyglutamic acid protein; NCT02917525).
Our group previously reported that degradation of IGF-1 by DPP-4 is linked to progressive aortic valve calcification,3 and that reciprocal interactions between valvular endothelial cells and VICs are critical for the development of AS. In physiological condition, IGF-1 suppresses osteogenic transformation of aortic VICs. Importantly, endothelial dysfunction increased DPP-4 expression and promoter binding in aortic VICs, thereby leading to increased degradation of IGF-1 and subsequent osteogenic differentiation of VICs. Accordingly, treatment with DPP-4 inhibitor hindered the progression of aortic valve calcification in animal models of AS.
Among various molecular targets potentially associated with AS development and progression, the DPP-4–IGF-1 axis is particularly useful for drug repositioning as DPP-4 inhibitors are widely used in patients with diabetes. For successful drug repositioning of DPP-4 inhibitors as disease-modifying agents for AS, the anticalcification effect and the cardiac tissue distribution profile of different DPP-4 inhibitors need to be analysed and compared. The currently available DPP-4 inhibitors have been reported to have a similar degree of inhibition of DPP-4 activity and thus show comparable efficacy for diabetes control; however, we observed that antidiabetes efficacy and anticalcification efficacy were quite different even in the same drug. For example, the anticalcifying EC50 value of sitagliptin acquired from our in vitro study was 699 nM, whereas the half-maximal inhibitory concentration values for diabetes were reported to be in the range of 10–20 nM.14 15 This implies that higher plasma or tissue concentrations may be needed to have a sufficient therapeutic effect in AS than those for diabetes. Moreover, five DPP-4 inhibitors had marked heterogeneity in their in vivo H:P concentration ratios, although most of them were able to attenuate in vitro osteogenic changes significantly. These results suggest that the in vivo anticalcifying efficacy of different DPP-4 inhibitors may also be different, and for this reason pharmacokinetic and pharmacodynamic modelling will be a useful approach to estimate the proper effect of each DPP-4 inhibitor to prevent calcific AS progression. As such, we observed that the frequency of AS progression was the lowest in patients who received favourable DPP-4 inhibitors with favourable anticalcification effect and high H:P concentration ratio.
DPP-4 inhibitors are currently being used for treatment of type 2 diabetes mellitus; the use of DPP-4 inhibitors is not accompanied by weight gain and carries a low risk of hypoglycaemia.16 As the actions of these drugs are based on restoration of physiological incretin effect, absence of inducible hypoglycaemia in normal controls has been well demonstrated,17 which supports successful drug repositioning to prevent AS progression in patients without diabetes. Based on this, a phase II clinical trial for patients without diabetes with mild-to-moderate AS is ongoing with evogliptin (NCT04055883), which is a long-acting DPP-4 inhibitor and has the most favourable effects in our experimental study. One potential issue is possible worsening of heart failure reported in several clinical trials.18 Different results were reported using a different DPP-4 inhibitor,19 and an analysis of big data from large cohorts of patients with diabetes (up to 1 500 000) reported that incretin-based drugs were not associated with an increased risk of hospitalisation for heart failure.20 We believe that this potential safety issue does not preclude from doing a clinical trial for successful drug repositioning of DPP-4 inhibitors.
Our study has several limitations. Although we screened more than several hundred thousand echocardiographic examinations in three large-sized tertiary referral hospitals, the number of patients included in the final analysis was rather small and adherence to medication could not be adequately evaluated in this retrospective study. Thus, our findings should be confirmed in a larger patient cohort. Also, as we only included AS patients with diabetes, our observations may not be directly applicable to AS patients without diabetes; a randomised clinical trial incorporating AS patients without diabetes would be useful to broaden the applicability of our results. Lastly, we used an arbitrary binary classification of DPP-4 inhibitors (favourable vs unfavourable) based on an adjusted H:P ratio. The best cut-off value of the index that we proposed could not be determined. Moreover, as we could not specifically measure valvular concentration of each drug, valvular DPP-4 activity after treatment cannot be evaluated; thus, the clinical implication of the adjusted H:P ratio we calculated needs to be further tested. In addition, we only used alkaline phosphatase activity assessment for comparison of pharmacodynamic properties of different DPP-4 inhibitors, but it can be also evaluated using different experimental models.
Conclusions
The currently available DPP-4 inhibitors used for diabetes control showed heterogeneous cardiac tissue distribution profiles and anticalcifying effects on aortic VICs. Our retrospective study on patients with diabetes and mild-to-moderate AS showed that DPP-4 inhibitors may be effective as disease-modifying agents for AS, as DPP-4 inhibitors with favourable tissue distribution profile and anticalcification effects were associated with smaller frequency of severe AS progression. These results should be considered in the preparation of randomised clinical trials on the repositioning of DPP-4 inhibitors for AS.
Key messages
What is already known on this subject?
A recent translational research revealed that the dipeptidyl peptidase-4 (DPP-4)–insulin-like growth factor-1 axis can be a potential therapeutic target to prevent calcific aortic stenosis (AS) progression, suggesting the possibility of drug repositioning of DPP-4 inhibitors.
What might this study add?
Our retrospective study on patients with diabetes and mild-to-moderate AS showed that DPP-4 inhibitors with favourable tissue distribution profile and anticalcification effects were associated with lower degree of AS progression and lower frequency of severe AS progression.
How might this impact on clinical practice?
We observed that pharmacokinetic–pharmacodynamic modelling using tissue distribution profile and anticalcification efficacy is useful in predicting the effect of DPP-4 inhibitors to prevent AS progression, and these results should be considered in the preparation of randomised clinical trials on the repositioning of DPP-4 inhibitors for AS.
Acknowledgments
The authors thank the Drug Metabolism and Pharmacokinetics (DMPK) core at the Convergence Medicine Research Center, Asan Medical Center for support and instrumentation. The authors also thank Dr Joon Seo Lim from the Scientific Publications Team at Asan Medical Center for his editorial assistance in preparing this manuscript.
References
Footnotes
SL and S-AL contributed equally.
Contributors SL and S-AL participated in the study design and analysis and interpretation of the final data, as well as in the drafting and approval of the final manuscript. BC, Y-JK and SJO were involved in in vivo animal experiments for pharmacokinetic–pharmacodynamic modelling and statistical analysis. H-MC, EKK, D-HK, G-YC, J-MS, SWP and D-HK were involved in the recruitment of participants from clinics. J-KS was responsible for the design and supervision of the study and revision of the manuscript.
Funding This research was supported by the Korea Drug Development Fund, funded by the Ministry of Science and ICT, Ministry of Trade, Industry and Energy, and Ministry of Health and Welfare (KDDF-201609-12, Republic of Korea).
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Patient consent for publication Not required.
Ethics approval The respective institutional review boards of each institution approved the protocols of this study. All animal experiments and protocols were performed in accordance with the Guide for the Care and Use of Laboratory Animals and approved by the Institutional Animal Care and Use Committee of Asan Institute for Life Sciences in Asan Medical Center (Seoul, Republic of Korea).
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available upon reasonable request. Please contact the corresponding author for our data.