Article Text

Statistics from Altmetric.com
Learning objectives
Identify the cardiovascular complications of COVID-19.
Identify the current management of acute coronary syndromes (ACS).
Identify the challenges in delivering treatment of ACS in the context of COVID-19.
Describe the best practice for primary angioplasty for ST-elevation myocardial infarction in the COVID-19 era.
Describe scenarios where thrombolysis should be considered.
Introduction
The coronavirus pandemic (COVID-19) has had unprecedented impact on healthcare systems, including acute cardiology services.1 2 COVID-19 directly leads to cardiac complications in those patients with underlying heart disease or cardiac risk factors. COVID-19 indirectly impacts patients through the required change in healthcare resource allocation and the need for social distancing. A reduction in health-seeking behaviour3 4 reduced attendances for cardiac emergencies,5 6 and reduction in traditional chronic care will have implications that extend beyond the infective reach of the virus. Therefore, cardiovascular care during the pandemic should remain a priority to mitigate the significant morbidity and mortality from both the direct and indirect effects of COVID-19.7 As future coronavirus waves are anticipated, it is prescient to review its impact on the delivery of cardiovascular care, in particular the management of acute coronary syndromes (ACS).
Cardiovascular concerns in COVID-19
Early reports suggested a strong relationship between traditional cardiovascular risk factors and poor outcomes from COVID-19.8 9 COVID-19 related myocardial injury is evident in postmortems.10 Those with critical illness demonstrate elevation of troponin and B-type natriuretic peptide (BNP) levels and rising levels correlate to poorer clinical outcomes.11 12
The mechanisms of myocardial injury remain poorly understood but candidates may involve ACE2 expression within the myocardium and coronary vessels triggering local inflammation, hypercoagulopathy and thrombosis. Coronary thrombosis will cause ACS and localised ischaemia in the form a type I myocardial infarction (MI).11 Ischaemia may also result from respiratory failure and hypoxia; in the context of underlying coronary disease, troponin rise may reflect a type II MI due to supply/demand mismatch.13 Pulmonary emboli may also occur, driving elevated pulmonary pressures with right ventricular strain.14 An immune-mediated inflammatory response appears to drive a secondary myocarditis and contributes to acute heart failure and multiorgan failure.15 The COVID-19 myocarditis generates striking ECG changes with marked and even regional ST elevation (‘STEMI-mimic’). Also, sympathetic drive may drive a Takutsubo-style cardiomyopathy or drive cardiac arrhythmia.
Acute coronary syndromes
In the pre-COVID-19 era, diagnosis of ACS relied on classical symptoms of chest discomfort (often associated autonomic features), characteristic electrocardiographic features and the rise in cardiac biomarkers (typically troponin). Management requires antiplatelets (aspirin with a potent P2Y1₁₂ antagonist such as clopidogrel, prasugrel or ticagrelor), injectable anticoagulants (such as fondaparinux) and modification of cardiac demand (with beta-blockers).12 13 Statins are given early as they may promote plaque stabilisation. While initial reports raised concerns about the use of ACE inhibitor and angiotensin receptor in patients with COVID-19,16 age-corrected models have not supported this, and ARBs may even have a protective role.17
Those with higher risk features such as significant troponin markers, ongoing ECG changes or high GRACE scores are offered invasive angiography as revascularisation reduces poor outcomes including reinfarction.18 19 In ST-elevation myocardial infarction (STEMI), immediate revascularisation with primary percutaneous coronary intervention (PCI) is essential. Untreated, STEMI has high mortality and risks mechanical complications such as mitral regurgitation or ventricular septal defects.18 Door-to-balloon time should be less than 60 min where feasible. Non-ST elevation myocardial infarction (NSTEMI) should have angiography within 72 hours, ideally sooner.
All these factors remain true in the COVID-19 era with the additional assessment of infective status and appropriate protection of staff. COVID-19 treatment algorithms have incorporated the use of anticoagulants given the thrombotic risk.20 Ischaemic events may be reducedby the addition of rivaroxaban 2.5 mg 21twice daily and ongoing studies are assessing this in the COVID-19 era.
While chest pain is common in COVID-19, symptoms of true MI remain distinct and detectable on assessment of history. The principle issue is distinguishing such type I MI events from troponin elevation due to arrhythmia, heart failure, myocarditis, pericarditis or systemic illness (type II MI).13 Clinical assessment, serial ECG and troponin measurement are key to diagnosis. In the context of COVID-19, conservative management may be appropriate for non-true ACS.
Point of care echocardiography can support decision making: the presence of regional wall motion changes would suggest typical ACS. Since echocardiography is an intimate examination with a sustained period of contact between patient and healthcare worker, there is increased risk of viral transmission, and full personal protective equipment (PPE) is advocated. Focused scans with limited views to answer the question are appropriate. Patients should wear masks during scanning and during their assessment and treatment.
Reperfusion for STEMI
In STEMI, rapid mechanical reperfusion through primary percutaneous coronary intervention (PPCI) is the preferred treatment option.22 The National Health Service and the British Cardiovascular Intervention Society have reiterated that PPCI remains the treatment of choice for STEMI in the COVID-19 era.23 In the UK, most cardiac networks have STEMI diagnosed by ambulance services, and patients are taken directly to designated cardiac catheter laboratories. Occasionally, patients may require acute transfer from district general hospitals into hub hospitals if the first hospital cannot offer revascularisation within a timely fashion. Typically, critical care ambulances are required for this.
As there is an asymptomatic period in which infected patients are shedding the virus, those presenting as emergency STEMI could drive viral transmission to first responders and those performing PPCI. COVID-19 diagnostic tools are not sufficiently rapid yet to permit screening prior to emergency PPCI for STEMI, and while screening with CT-thorax is useful in more elective settings, it is unfeasible in a STEMI setting. As PPCI can involve cardiac arrest, a recognised ‘aerosol generating procedure’, it is agreed that full PPE is recommended for all those performing PPCI.23 24 Services should consider shielding members of staff at highest risk from COVID-19: those with lung conditions or those over the age of 65 years have been redeployed to non-patient-facing activities appropriately.
PPCI should be performed with reperfusion within 120 min of symptom onset and within 60 min of arrival at a PPCI capable centre.20 21 Radial access is preferred to facilitate early patient ambulation. Observational data suggest those with COVID-19 have a greater burden of thrombus: multivessel thrombosis and stent thrombosis rates are higher.25 Higher rates of aspiration thrombectomy and greater need for GPIIb/IIIa and higher doses of intraprocedural heparin are all reported.25 Prolonged hospitalisation and greater mortality is seen in those with COVID-19 and STEMI.25 26
A dedicated catheter laboratory is recommended, and all possible equipment should be available within this to limit staff having to fetch equipment and potentially spread the virus. A designated area for donning and doffing PPE is essential; staff should observe each other to provide support in this process. All team members should have sufficient PPE with FF2 or FFP3 mask, gown, goggles and/or visor. As PPE remains scarce, some may choose to limit PPE usage to operators only. However, in the event of a cardiac arrest, team members will need to leave the cardiac catheter lab to don PPE before exposure to Cardiopulmonary resuscitation (CPR) manoeuvres.
Negative pressure facilities have been recommended to minimise spread of the virus, but few have this capability. The alternative is to deep clean after each case. In the event of multiple STEMI patients arriving at once, a risk assessment should be performed and, if delays are inevitable, then thrombolysis should be considered.
In those developing cardiogenic shock in the context of COVID-19 infection, futility should be considered. However, as decision making in the acute setting can be challenging, all available supportive therapies should be used when appropriate.
Thrombolysis for STEMI
While PPCI remains the treatment of choice for STEMI, the number of COVID-19 cases in Wuhan and Lombardy raised sufficient concerns that thrombolysis should be considered in certain circumstances.24 27 28
In normal circumstances, transfer to PPCI centres is effective and safe. However, during the COVID-19 peak, hospital transfers have been affected and, for those unwell COVID-19 patients who are actively shedding virus, are potentially hazardous. Furthermore, critically unwell patients requiring non-invasive ventilation are challenging to transfer safely with aerosolised secretions posing a threat to staff. Intubated patients have closed circuits that lower the risk of transmission, but these patients remain a challenge to transfer in a timely manner. Those patients in intensive care units (ICU) in district generals without acute primary angioplasty services will be disadvantaged as acute transfer to local PPCI centres will be delayed. Those patients who have fulminant COVID-19 may be unable to lie flat and be unable to tolerate an invasive angioplasty.
In these scenarios, thrombolysis should be considered early and administered promptly in the absence of contraindications; the greatest value is within 1 hour of pain onset. Fibrin-specific agents such as alteplase and tenectaplase can be given easily; the latter is preferable as a single bolus reduces the need for close nursing contact.
The use of thrombolysis remains controversial with concerns over bleeding risks in the context of possible COVID-19 myocarditis. Furthermore, a quarter of patients will not reperfuse and still require facilitated PCI.23 However, despite these concerns, thrombolysis is used for STEMI around the world29 and has been used successfully in patients with COVID-19 in China. While PPCI has clear advantage in lower bleeding risk and greater likelihood of reperfusion, the efficacy balance between thrombolysis and PPCI is closer to equipoise when PPCI is delayed. The Strategic Reperfusion Early after Myocardial Infarction (STREAM) study demonstrated even a single hour of delay meant there was no significant difference in major events after randomised to either thrombolysis or PPCI.30
Patients should be urgently discussed with a senior cardiologist and an interventional cardiologist. Rapid communication is essential and may need to be entirely remote to facilitate speed. Documentation should reflect on why thrombolysis is used and the system constraints that mandated it. Upfront decisions should be documented for subsequent treatment for those patients in which ST segments do not sufficiently resolve. A cardiac catheter laboratory should be activated and steps taken for safe transfer. Patients achieving reperfusion should be considered for invasive angiography on stabilisation.
Unique issues regarding ACS in the COVID-19 era
STEMI-mimic
Unwell patients with COVID-19 have manifested severe ST-elevation but have been found to have unobstructed coronary arteries on invasive angiography.12 26 The mechanism remains unclear but is attributed to myocarditis or a Takutsubo-type response to overwhelming inflammation. As COVID-19 case numbers rose in Wuhan and Lombardy, there was concern that PPCI services would be overwhelmed by similar patients and expose patients to the risks of unnecessary invasive procedures.31 32 However, this has been less evident in the UK. Echocardiography can help support a diagnosis of a global myocarditis, but coronary angiography is still advocated to avoid missing a true coronary occlusion.33
Delayed attendance
As the pandemic evolved, a global reduction in ACS admissions has been noted.3 5 This is, perhaps, in response to strong governmental messages to ‘stay at home’. Anecdotally, patients have avoided hospitals despite significant cardiac symptoms. Patients may fear contracting the virus or wish to avoid overloading medical services. Referrers in primary or intermediate care settings may misconstrue chest pain as part of COVID-19. Those in smaller district hospitals may be unable to transfer patients to catheter-lab centres due to saturation of emergency services.34 Globally, a 20%–40% reduction in STEMI presentations has been reported; greater reductions in NSTEMI are noted.35–37 Those attending have experienced significantly longer door-to-balloon times with longer times of assessment in emergency rooms, longer times for staff to prepare PPE and potentially longer procedure times due to clot burden, disease complexity or the need for respiratory support.34 35
Late presentations for STEMI have increased34 and may have a large thrombotic burden with a failure to reperfuse despite PCI. Mechanical complications such as septal defects and ventricular rupture have been reported. It is expected that the incidence of heart failure may rise due to this late presentation with ACS. The national PCI and MI registries in the UK are being used to study the pattern of ACS admissions since the pandemic started.38
Novel pathways & new ways of working
Significant changes in working patterns have meant novel care pathways have been instituted. Some of these may have value beyond the pandemic. Pathways should be modified according to the resources available locally.
Minimised length of stay
Prompt treatment and minimisation of testing unlikely to change near-term clinical decisions should help to minimise the inpatient length of stay. This is important to reduce the likelihood of patients acquiring de novo coronavirus infection from other patients. In efficient healthcare systems with early reperfusion, it should be feasible for uncomplicated MI to discharge within 24 hours of admission. Prompt review in emergency departments with same-day angiography should be considered where feasible. As elective care has been curtailed, catheter laboratories have the capacity for rapid turn around and radial access permits early discharge. Bedside point of care echocardiography can provide LV assessment. A short period of rhythm monitoring is appropriate in low-risk patients with uncomplicated PCI. Tests such as Positron emission tomography (PET), Myocardial Perfusion Imaging (MIBI) and Magnetic Resonance Imaging (MRI) are less readily available in the current pandemic. Unless critical for decision making, it is suggested these tests are deferred to reduce the length of inpatient stay.
Low-risk patients with low Global Registry of Acute Coronary Events (GRACE) scores and small troponin-rises can be stratified, and if appropriate, then early urgent angiography can be considered on an ‘outpatient’ basis without inpatient stays. Some Trusts have kept angiographic facilities in ‘clean zones’ allowing patients to be discharged from emergency departments and attend semielectively the next day for the invasive procedure while minimising hospital stay. Maximal antiplatelet therapy and appropriate counselling is required.
Clustering of patients
In some cases, inpatient stay is inevitable. Hospitals have developed clearly demarcated ‘zones’ to reflect the likelihood of viral cross-contamination. Patients with confirmed COVID-19 should be clustered with others who have the virus. However, delays in viral diagnostics can mean apparently well but infected and shedding patients can enter ostensibly ‘clean’ zones.
Surgical disease
Patients presenting with ACS may be found to have coronary disease best revascularised by coronary artery bypass surgery. Early in the pandemic, all elective surgery was cancelled to reduce the impact on intensive care facilities. This has evolved into allowing urgent surgery once discussed at an Multi-disciplinary Team Meeting (MDT) but in a limited number of centres. MDTs should be performed early and ideally daily to minimise uncertainty and duration of inpatient stay. In patients who have COVID-19, there is concern that surgery will pose undue risk and harm. In these cases, PCI should be preferred where possible. As surgical disease can be complex, additional care and attention will be necessary when performing PCI with consideration of adjunctive technologies.
Areas for research
National registries are working to detect patterns of disease during the pandemic and will offer insights into how patients were treated. The C19-ACS randomises COVID-19 patients with known coronary artery disease or risk factors to standard therapy or the addition of dual antiplatelet therapy with low-dose anticoagulation with rivaroxaban 2.5 mg BD. The concept is that part of the elevated mortality in COVID-19 is driven by cardiac events and localised thrombosis. A pilot study is running before a wider roll-out (https://clinicaltrials.gov/ct2/show/NCT04333407).
ACS phenotypes in COVID-19 era
One can consider a number of different phenotypes of ACS in the current era.
A classical ACS, with undiagnosed COVID-19, found on routine testing on admission
A 55-year-old man with a background history of hypertension and 20-a-day cigarette habit is admitted with 15 min of retrosternal chest pain. He is otherwise well. The ECG demonstrates deep T-wave inversion across the anterior leads, and the troponin is 253 ng/L. Handheld echocardiography reveals anterior hypokinesia. There is no history of fever or dyspnoea, but a nasopharyngeal swab is PCR positive for COVID-19. He undergoes invasive angiography wearing a mask; the treating team is in full PPE. Following PCI to the mid-Left Anterior Descending (LAD) artery with a single drug eluting stent, he is allowed home promptly and given clear instructions for monitoring his temperature and saturations.
Learning points
In this case, near routine care was delivered and an early discharge aimed to minimise viral exposure to other patients.
Asymptomatic patients may be COVID-19 positive, and it is unclear if they are infective or not.
PPE should be mandated while treating patients.
Patients with higher risk NSTEMI (dynamic ECG changes and elevated troponin) are best treated with revascularisation where possible.
Classical COVID-19 features with concomitant true STEMI
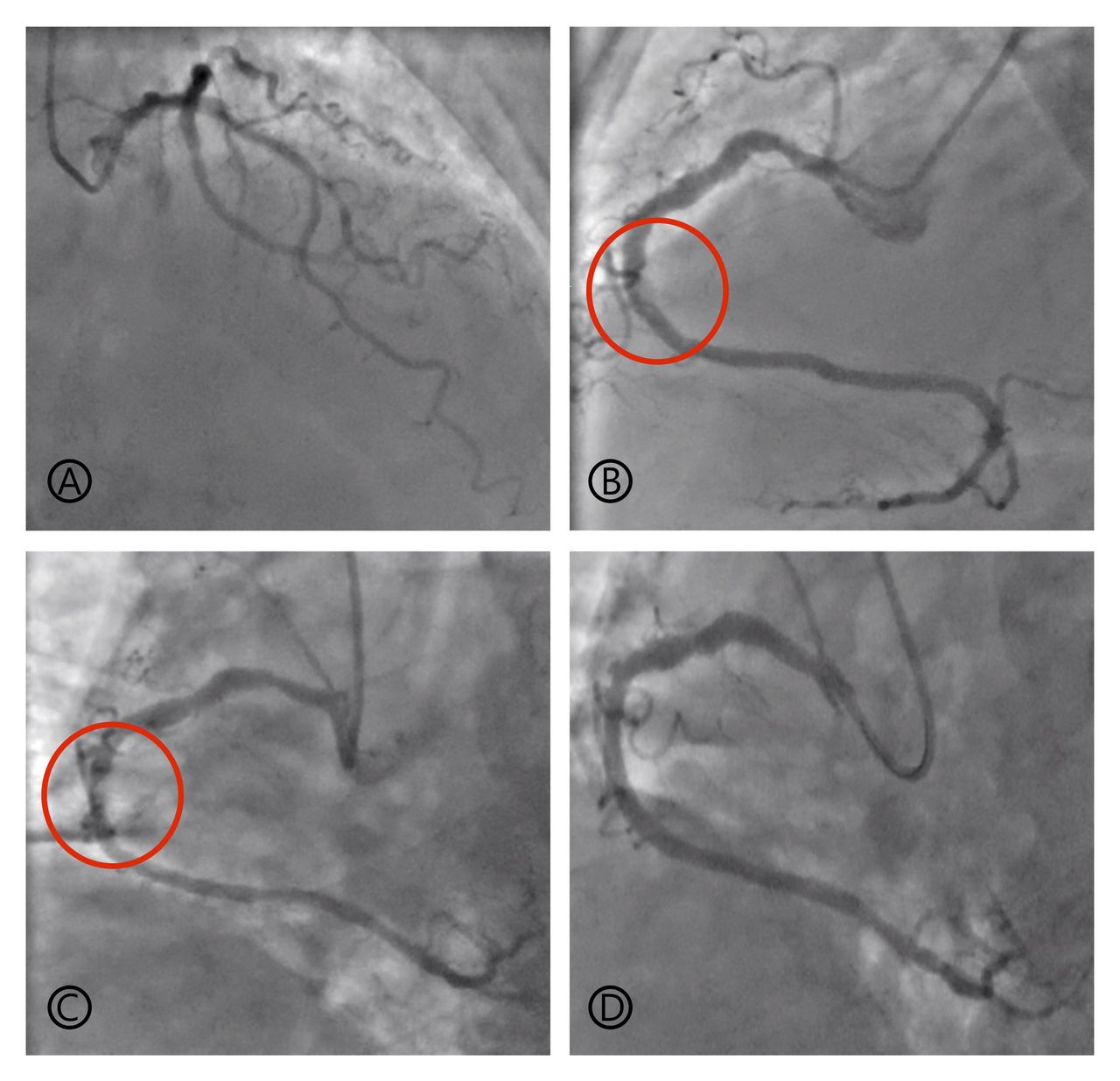
A 66-year-old man with a background history of prior PCI over a decade previously is admitted with a classical presentation of COVID-19. He is breathless with a persistent cough and high fevers. Bilateral infiltrates are seen on chest radiographs. Initial ECGs are within normal limits (figure 1A). He requires continuous positive airways pressure (CPAP) but remains stable. Five days into admission, he develops central crushing chest pain at 06:00. He is markedly breathless and cannot lie flat. Severe inferior ST elevation is noted (figure 1B). Primary PCI requires urgent transfer to the local tertiary centre, but intensivists feel he is unsafe for transfer and prefer not to intubate. His case is urgently discussed between the cardiologist on the ward and interventionalists locally and at the tertiary centre; thrombolysis is agreed. Following alteplase and heparin, ST segments resolve (figure 1C), and the patient is stabilised on aspirin and clopidogrel. The troponin is 1800 ng/L. After a further 5 days, he is well enough for invasive angiography. The left coronary system had a patent stent and minor disease. A thrombotic lesion is noted in the Right Coronary artery (RCA) (figure 2B,C). This is stented, and he is discharged on maximum secondary prevention.

Electrocardiographs of patient with COVID-19 developing ST elevation myocardial infarction. (A) Baseline electrocardiograph on admission. (B) The patient developed severe central crushing chest pain while on continuous positive airways pressure. ST elevation is evident in the inferior leads with reciprocal ST depression anteriorly. (C) Following alteplase and heparin, there is evidence of reperfusion with over 50% reduction in ST elevation in the inferior leads.

{kind=link}
{kind=link}
Stills from invasive coronary angiography in stabilised patient with COVID-19 after thrombolysis for STEMI. Coronary angiography was performed via the right radial artery. (A) the left coronary tree had diffuse disease with moderate to severe disease in a second diagonal artery. A prior stent in the LAD was patent. (B and C) A dominant right coronary artery had a moderate to severe proximal stenosis with a recanalised thrombotic lesion in the midvessel. (D) The proximal and midvessel lesions are stented with 3.5 mm diameter drug-eluting stents that are optimised with 4.0 mm non-compliant balloons. STEMI, ST-elevation myocardial infarction.
Learning points
Thrombolysis should be considered for patients who cannot receive PPCI in a timely manner.
Decisions for thrombolysis should be senior led and made in conjunction with tertiary PPCI centres as a plan for facilitated PCI may be required.
Angiography prior to discharge is desirable and should be performed once the patient has stabilised from COVID-19.
Severe COVID-19 with STEMI-mimic
A 41-year-old man with no prior medical history has a rapidly progressive COVID-19 illness. Following an initial trial of CPAP therapy, he requires intubation and is admitted to intensive care for monitoring. Troponin and BNP levels begin to rise, and his ECG shows widespread significant ST elevation. Haemodynamic parameters are normal, and bedside echocardiography shows ‘low-normal’ function with no clear regional wall motion abnormalities. In light of ST segment changes, the patient undergoes urgent invasive angiography. The coronary vessels are smooth and unobstructed. Conservative measures are instituted, but the patient develops recurrent ventricular tachycardia that is unresponsive to amiodarone and mexiletine. He developed multiorgan failure. He was considered for transfer for advanced supportive therapies but destabilised and passed away.
Learning points
STEMI can occur due to myocarditis and does not equate to coronary occlusion.
The presence of myocarditis is a significant risk. Even those without coronary artery disease remain at high risk of a poor outcome. Consider advanced haemodynamic support with percutaneous ventricular assist devices or extracorporeal membrane oxygenation.
Future perspectives post-COVID-19
The COVID-19 pandemic has driven a rapid configuration of services across hospitals, assisted by reduction in bureaucracy. Acute services have been reconfigured to reduce coronavirus spread with segregation of acute assessment areas, wards and catheter labs into ‘clean’ and ‘dirty’ zones. Patients are stratified by the likelihood of infection. Upstream swabbing and temperature assessment is essential. Unfortunately, maintaining strict clean sites will prove difficult in acute care, in particular for STEMI, and PPE should continue to be used when patients are at risk of being infective. Increasingly rapid swabbing protocols may facilitate more selective use.
Elective work, which was postponed by the pandemic, has been restored by using enhanced preprocedure assessment with comprehensive swabbing and patient self-isolation prior to elective procedures. The length of isolation appears variable across hospitals. Staff swabbing on a fortnightly basis may help identify illness among staff and reduce the chance of services closing or infection of patients. Outpatient elective surgery has been stratified by urgency and, in some places, has moved to different hospital sites to ensure there is no impact to intensive care services. Longer term, normal clinical services must return to minimise a growing inequality of service access.
Outpatient flows have benefited from embracing technology. Clinics become remote to to reduce patient viral exposure. Telephone and video clinics are now fully established and in many cases can replace traditional clinics. Face-to-face appointments can be reserved for specified patients but must include appropriate PPE and social distancing to reduce the exposure risk to cardiology patients who are specifically vulnerable to complications. Postinfarction ‘virtual’ cardiac rehabilitation and heart failure clinics have proven feasible.
Going forward, work is required to anticipate the possibility of further ‘waves’ of the virus. Cardiologists may need novel working models, expanding beyond job plans and may require shift patterns.
Conclusions
The management of ACS remains a key priority and services must be configured in an adaptable manner to respond to the changing demands in the pandemic. The treatment for ACS is well established, and while effort should be made to adhere to standard pathways, the judicious use of pharmacological and diagnostic adjuncts may allow deviation from these pathways to identify and treat those that are not true ACS and those that are simply too unstable to benefit from the standard treatment strategies.
Key points
Prompt and early revascularisation, with appropriate personal protective equipment, remains the default treatment approach for patients with acute coronary syndrome in the COVID-19 era.
The use of risk stratification tools (such as GRACE scores) may aid the prioritisation of cases to minimise their hospital stay.
Critically unwell patients with ST-elevation myocardial infarction, without onsite catheter lab facilities or too unstable for transfer should be considered for thrombolysis and activation of services for facilitated PCI if necessary.
Patients with cardiovascular disease are particularly vulnerable during this period regardless of their infective status. Adaptation of cardiac services to ensure continuity of care for these patients even in the context of a further wave of COVID-19 is essential to minimise preventable cardiovascular death.
CME credits for Education in Heart
Education in Heart articles are accredited for CME by various providers. To answer the accompanying multiple choice questions (MCQs) and obtain your credits, click on the ‘Take the Test’ link on the online version of the article. The MCQs are hosted on BMJ Learning. All users must complete a one-time registration on BMJ Learning and subsequently log in on every visit using their username and password to access modules and their CME record. Accreditation is only valid for 2 years from the date of publication. Printable CME certificates are available to users that achieve the minimum pass mark.
Translated summary
Data availability statement
There are no data in this work.
Ethics statements
Patient consent for publication
References
Footnotes
Twitter @sukhnijjer
Contributors SSN wrote the first draft that was critically appraised by RP and SS leading to subsequent drafts. All three authors have approved the final manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Commissioned; internally peer reviewed.
Author note References which include a * are considered to be key references.