Article Text

Abstract
Objective To evaluate the effect of triglyceride deposit cardiomyovasculopathy (TGCV) on the cardiovascular outcomes in haemodialysis (HD) patients with suspected coronary artery disease (CAD).
Methods This retrospective single-centre observational study included data from the cardiac catheter database of Narita Memorial Hospital between April 2011 and March 2017. Among 654 consecutive patients on HD, the data for 83 patients with suspected CAD who underwent both [123I]-β-methyl-iodophenyl-pentadecanoic acid scintigraphy and coronary angiography were analysed. Patients were divided into three groups: definite TGCV (17 patients), probable TGCV (22 patients) and non-TGCV control group (44 patients). The primary endpoint was a composite of cardiovascular death, non-fatal myocardial infarction and non-fatal stroke assessed for up to 5 years of follow-up.
Results The prevalence of definite TGCV was approximately 20% and 2.6% among consecutive HD patients with suspected CAD and among all HD patients, respectively. At the end of the median follow-up period of 4.7 years, the primary endpoint was achieved in 52.9% of the definite TGCV patients (HR, 7.45; 95% CI: 2.28 to 24.3; p<0.001) and 27.3% of the probable TGCV patients (HR, 3.28; 95% CI: 0.93 to 11.6; p=0.066), compared with that in 9.1% of the non-TGCV control patients. Definite TGCV was significantly and independently associated with cardiovascular mortality and outcomes among HD patients in all multivariate models.
Conclusions TGCV is not uncommon in HD patients and is associated with an increased risk of cardiovascular events including cardiovascular death. Thus, TGCV might be a potential therapeutic target.
- nuclear cardiac imaging
- coronary artery disease
- metabolic heart disease
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Patients on haemodialysis (HD) are at a higher risk of developing cardiovascular disease (CVD), which is a leading cause of death and accounts for approximately 30%–35% of all-cause mortality among patients on HD.1–3 Despite development of therapeutic procedures, such as percutaneous coronary intervention (PCI) and coronary artery bypass grafting (CABG), the mortality rate among patients on HD is still high.4 Although medical therapies have evolved dramatically during the previous three decades, statins have little effect on HD-related lipid abnormalities and the improvement of prognosis among these populations.5 6 Given the poor responses to any invasive revascularisation therapies and medical therapy, cardiovascular mortality is 10–20 times higher in dialysis patients than in the general population.7
Triglyceride deposit cardiomyovasculopathy (TGCV) is a novel disease concept. We initially reported that among Japanese patients requiring cardiac transplantation, defective hydrolysis of intracellular triglyceride (TG) results in diffuse narrowing coronary atherosclerosis with massive accumulation of TG, but not cholesterol in vascular smooth muscle cells (SMCs) and endothelial cells.8 9 Since this discovery, we launched the Japan TGCV study group as a governmental rare disease project to develop diagnostic criteria and specific treatments. TGCV was recently identified as an orphan disease in Europe in 2019 (Orphanet ORPHA Number: 565612).10 The known causes of TGCV thus far are genetic as well as acquired deficiency of adipose triglyceride lipase (ATGL), which is a rate-limiting enzyme of hydrolysis of TG. We reported that SMCs and endothelial cells with ATGL deficiency showed vulnerable and pro-inflammatory phenotypes in vitro.11 12 Our subsequent postmortem and clinical studies showed that some of the patients with TGCV were associated with advanced chronic kidney disease and HD.13 14
Noting the above-mentioned analogies of pathological characteristics of coronary arteries and poor response to currently available therapies, we hypothesised that concurrent TGCV in HD patients with suspected coronary artery disease (CAD) plays a critical role in the cardiovascular outcomes of this population. Therefore, this study aimed to evaluate the effect of TGCV on the prevalence and clinical cardiovascular outcomes in patients on HD at the 5-year follow-up, after the first diagnosis of TGCV.
To the best of our knowledge, this is the first study investigating the prognostic impact and clinical outcomes of TGCV among HD patients.
Methods
Patients and public were not involved in the design, conduct, reporting or dissemination plans of our research.
Patients and study design
This retrospective single-centre observational study included data from the cardiac catheter database of Narita Memorial Hospital between April 2011 and March 2017. Flowchart describing the process of patient selection is shown in figure 1. Among 654 consecutive HD patients during the follow-up period, 118 patients were suspected of CAD based on clinical findings (presence of ischaemic symptoms and/or ischaemic change in the ECG at rest and/or abnormal left ventricular wall motion by ultrasound). After the exclusion of nine patients with missing data and 26 patients because of negative exercise ECG tests and/or non-obstructive CAD findings based on the results of coronary CT angiography, data from 83 patients who underwent both [123I]-β-methyl-iodophenyl-pentadecanoic acid (BMIPP) scintigraphy and coronary angiography (CAG) were analysed. BMIPP scintigraphy and CAG, regardless of BMIPP scintigraphy results, were performed as part of the routine protocol for the diagnosis of CAD. Eighty-three patients were divided into the following groups for subsequent comparative analyses: definite TGCV, probable TGCV or non-TGCV control group. The diagnosis of TGCV was based on the following two chief items (equivalent to two points each): decreased washout rate (WOR) of BMIPP of <10% in [123I]-BMIPP scintigraphy, which is indicative of myocardial TG metabolism,15 16 and diffuse narrowing of the coronary arteries observed on CAG, as well as some other minor items (equivalent to one point each) in the latest diagnostic criteria for TGCV.17–19 Diffuse narrowing of the coronary arteries can be defined as ‘consecutive or longitudinal’ and ‘complete or partial’ obstruction in coronary vessels. To validate the coronary obstruction burden on CAG, we compared 30 randomly selected CAGs. Two interventional specialists (HA and YN), interpreted the CAGs independently. Four points or more indicated a definite diagnosis of TGCV, meanwhile three points indicated probable TGCV.

Flowchart describing the process of patient selection. The latest diagnostic criteria for TGCV was published in 2018 by the Japan TGCV study group which is a governmental rare disease project in Japan. Based on this, a total of 654 consecutive patients with HD, between April 2011 and March 2017, were retrospectively assessed for eligibility. Informed consent was obtained from all patients, of whom, 118 patients were suspected of CAD. Thirty-five patients were excluded mainly due to negative stress ECG and/or non-obstructive CAD findings based on the results of CCTA or missing data. Finally, data from 83 were extracted, and divided into three groups: 17 patients in the definite TGCV, 22 patients in the probable TGCV and 44 patients in the non-TGCV control groups. CAD, coronary artery disease; CCTA, coronary CT angiography; HD, haemodialysis; TGCV, triglyceride deposit cardiomyovasculopathy.
Invasive therapeutic procedures at baseline and during follow-up
Any invasive procedures, including PCI or CABG, at baseline and during the follow-up period, were performed based on the clinical findings of ischaemic chest symptoms with an ischaemic change in electrocardiography and positive functional ischaemia assessment and/or BMIPP scintigraphy findings at baseline.
Clinical endpoints
The primary endpoint was a composite of cardiovascular death, non-fatal myocardial infarction (MI) and non-fatal stroke assessed up to 5 years at follow-up. The key secondary endpoint was a composite of cardiovascular death, non-fatal MI, non-fatal stroke, target vessel revascularisation (TVR), or any hospitalisation for heart failure related to concomitant treatment. TVRs shortly after CAG were not included in the secondary endpoints. The endpoints, including death, MI, stroke, fatal bleeding and any revascularisations during the follow-up period, were defined according to the Academic Research Consortium classification.20
Statistical analyses
Continuous variables with a normal distribution are expressed as means±SD, and three-group comparisons were performed using one-way analysis of variance (ANOVA) analysis. The normality of the variables was assessed with the Shapiro-Wilk test. The number of patients failing the normality tests are expressed as medians with IQRs and were compared using the Kruskal-Wallis H test. Categorical variables are presented as patient numbers (%) and were analysed using the χ2 test. Cohen’s kappa coefficient was used to measure inter-rater reliability for diffuse narrowing of the coronary arteries. Cumulative incidence rates of primary and secondary endpoint were estimated by cumulative incidence functions (CIFs) methods using R V.3.4.1. The differences in incident rates among three groups were compared using the Wilcoxon test. Cox proportional hazards models were used to calculate HRs and 95% CIs for the clinical events after adjustment for confounding factors (age and sex) in Model 1, various variables associated with mortality of HD patients in Model 2 and variables known as classical cardiovascular risks in Model 3. The geriatric nutritional risk index was calculated with serum albumin levels and body weight and height.21 All statistical analyses except for CIFs were performed using SPSS statistical software, V. 25.0 (IBM Corp).
Results
Baseline patient characteristics
The baseline characteristics of patients with or without TGCV are listed in table 1. A total of 83 HD patients were divided into three groups, definite TGCV (17 patients), probable TGCV (22 patients) and non-TGCV control group (44 patients), based on the latest diagnostic criteria.22–24 There were no significant differences concerning the mean age, sex, coronary risk factors, medications, laboratory data and left ventricular ejection fraction among the three groups except for high proportion of diabetes, haemoglobin A1c levels and use of insulin in the probable TGCV group. The WOR value of BMIPP was significantly lower in the definite TGCV group (−5.87±18.6%) than in the probable TGCV group (13.6%±14.8%) and non-TGCV control group (16.3%±9.9%).
Characteristics of the patients at baseline
Coronary morphology and planned revascularisations at baseline
On the CAG, the number of significant stenoses and the proportion of diffuse narrowing coronary arteries were higher in the definite TGCV group (1.5±1.1 and 100%, respectively) and the probable TGCV group (1.7±1.6 and 68.2%, respectively) than in the non-TGCV control group (0.4±0.8 and 20.5%, respectively). Cohen’s kappa coefficient for the diffuse narrowing of the coronary arteries was 0.86. The requirement for PCI or CABG shortly after CAG at baseline was 88.2% (15 out of 17 patients) in the definite TGCV group, 68.2% (15 out of 22 patients) in the probable TGCV group and 25% (11 out of 44 patients) in the non-TGCV control groups.
Cardiovascular outcomes
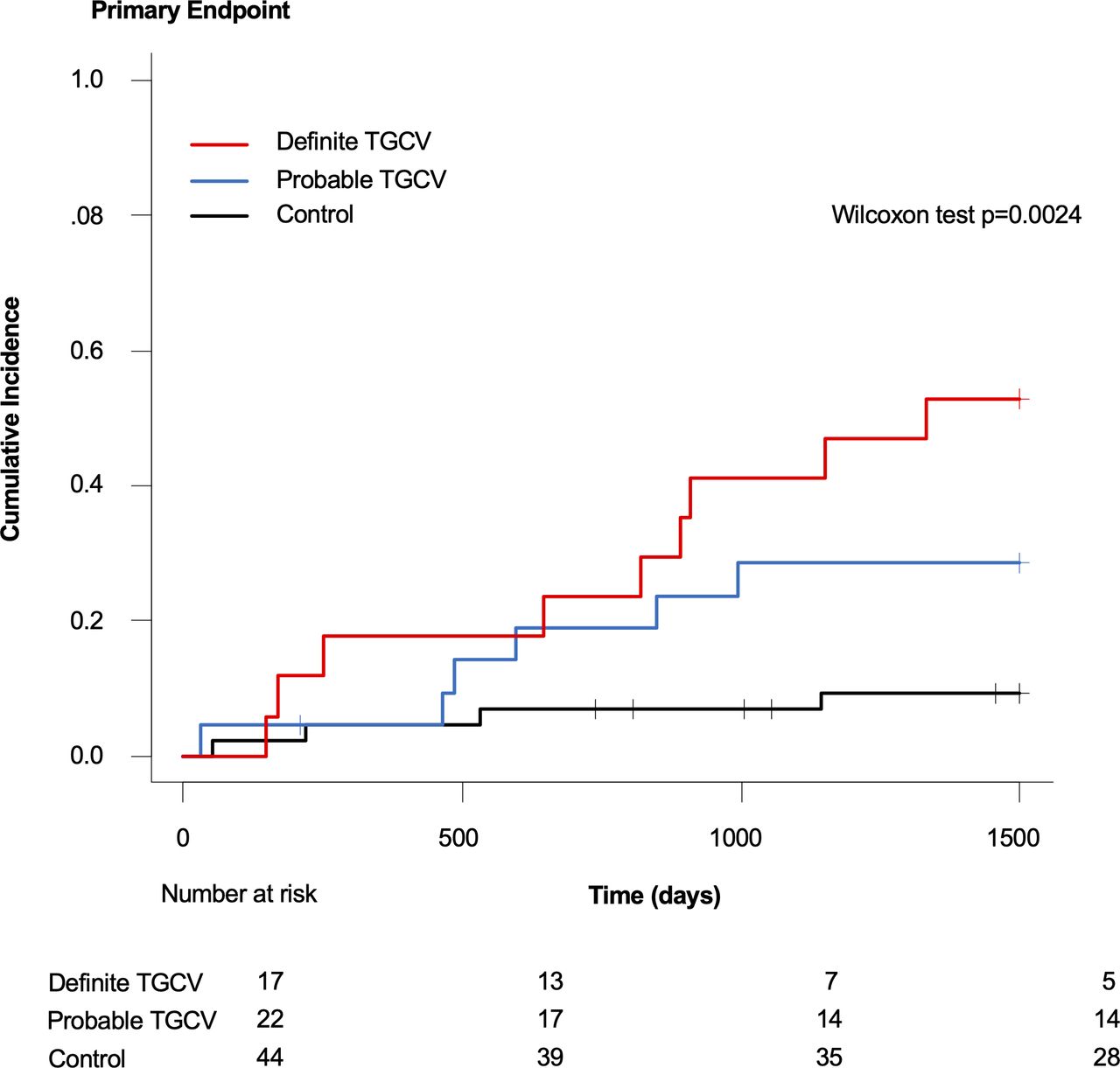
The follow-up period ended in March 2017. The median follow-up duration was 1718 days (4.7 years). Figures 2 and 3 show CIFs for the primary and key secondary endpoints, respectively. figure 4 shows the prespecified hierarchical testing of the endpoints for the definite or probable TGCV. The cumulative incidence of primary endpoints at the 5-year follow-up was 52.9% (9 out of 17 patients) in the definite TGCV group, 27.3% (6 out of 22 patients) in the probable TGCV group and 9.1% (4 out of 44 patients) in the non-TGCV control group. The risk of achieving primary endpoints was significantly higher in the definite TGCV group than in the non-TGCV control group (HR, 7.45; 95% CI: 2.28 to 24.3; p<0.001). The risk of achieving the key secondary endpoint events was also significantly higher in the definite TGCV group (HR, 6.36; 95% CI: 2.89 to 14.0; p<0.001) and the probable TGCV group (HR, 2.67; 95% CI: 1.20 to 5.96; p=0.017) than in the non-TGCV control group. Among the primary composite endpoints, the risk of cardiovascular death and non-fatal MI were higher in the definite TGCV group than in the non-TGCV control group. In contrast, the occurrence of non-fatal stroke was similar between the two groups.
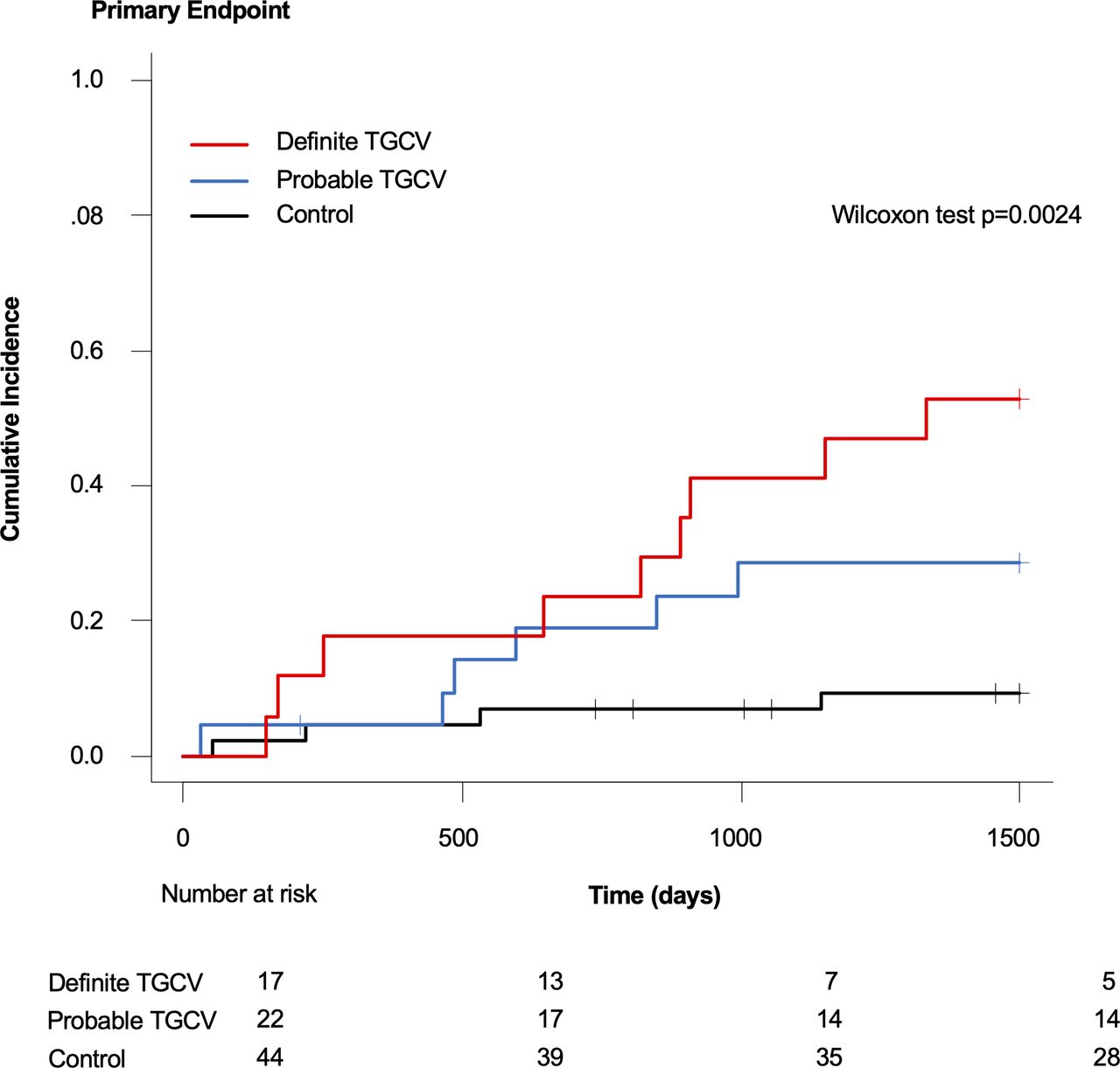
Cumulative incidence functions for the primary composite outcome This figure shows the cumulative incidence of the primary composite outcome of cardiovascular death, non-fatal myocardial infarction and non-fatal stroke in a time-to-event analysis. TGCV, triglyceride deposit cardiomyovasculopathy.

Cumulative incidence functions for the key secondary composite outcome This figure shows the cumulative incidence of cardiovascular death, non-fatal myocardial infarction, non-fatal stroke, target vessel revascularisation, or any hospitalisation for heart failure in a time-to-event analysis. TGCV, triglyceride deposit cardiomyovasculopathy.
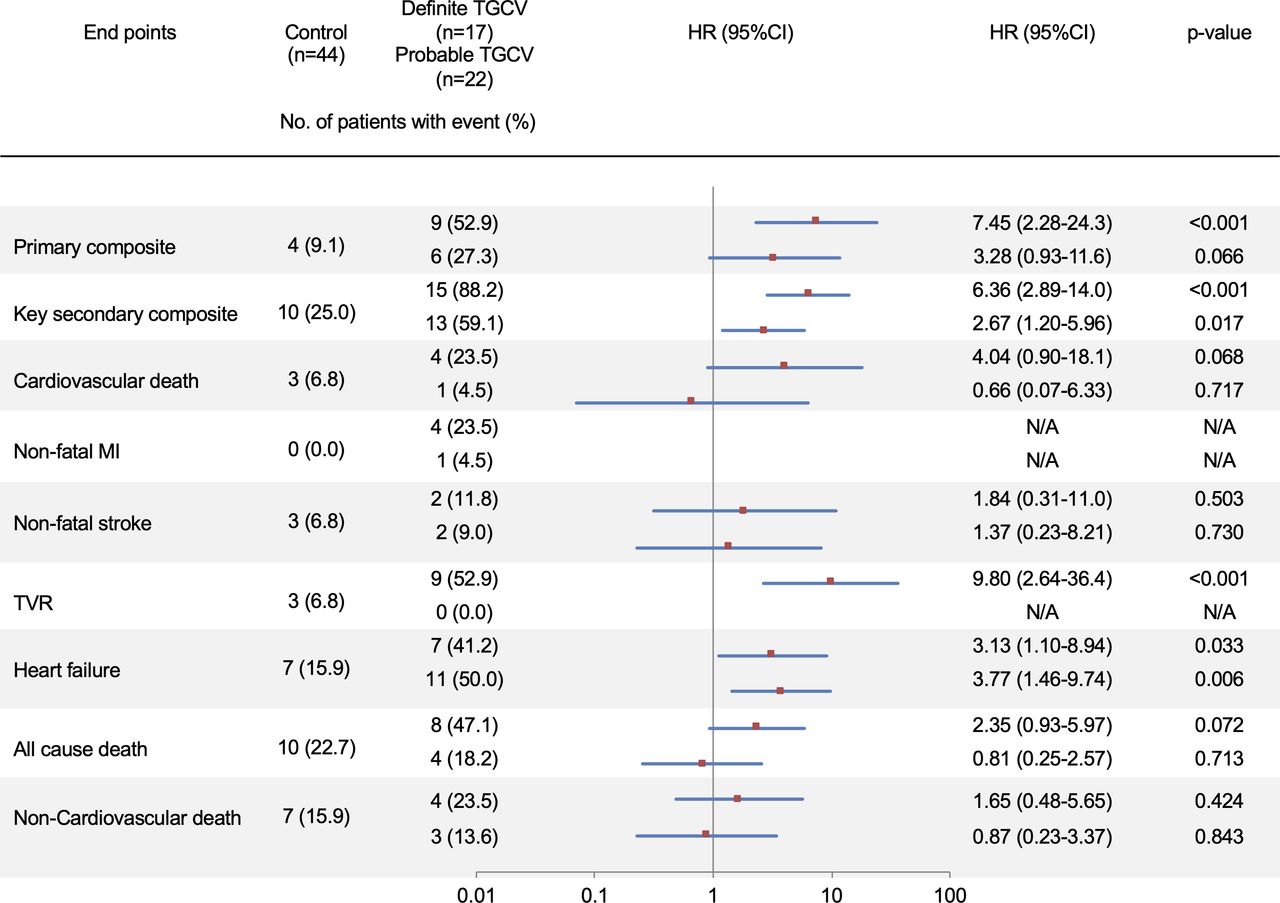
The prespecified hierarchical testing of the endpoints. The prespecified plan for hierarchical testing of the endpoints for the definite TGCV and the probable TGCV is shown. The endpoint (except non-fatal stroke) rates were significantly higher in the definite TGCV group than in the non-TGCV control group. MI, myocardial infarction; TGCV, triglyceride deposit cardiomyovasculopathy; TVR, target vessel revascularisation.
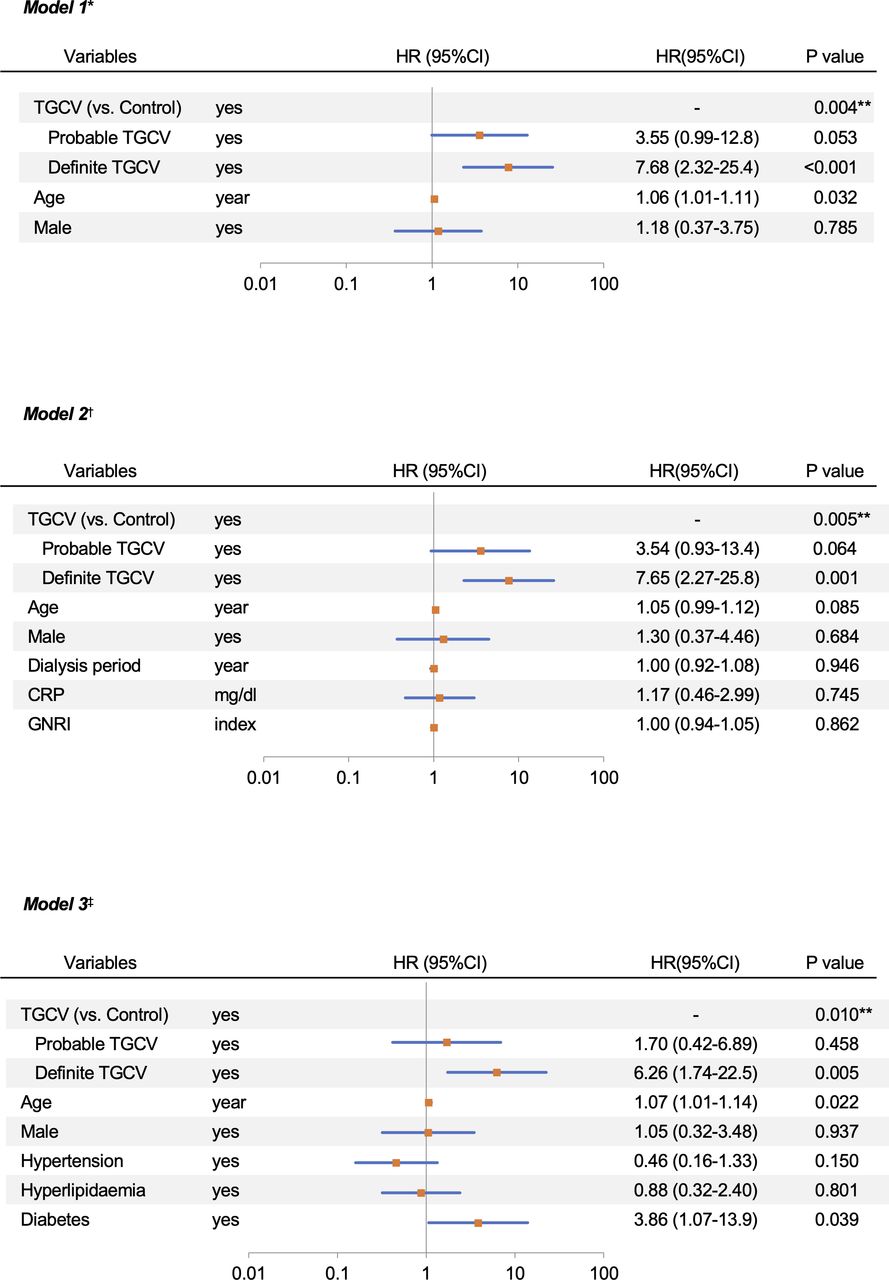
Cox proportional hazard analyses for primary endpoints in patients with the definite or probable TGCV. The primary endpoint was a composite of cardiovascular death, non-fatal myocardial infarction and non-fatal stroke. *Confounding factors (age and sex) were adjusted for in Model 1. †Various variables associated with mortality of HD patients were adjusted for Model 2. ‡Variables known as classical cardiovascular risks were adjusted for Model 3. **P value for trend. CRP, C-reactive protein; GNRI, geriatric nutritional risk index; TGCV, triglyceride deposit cardiomyovasculopathy.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Cox proportional hazard analyses for key secondary endpoints in patients with the definite or probable TGCV. The key secondary endpoint was a composite of death from any cause, non-fatal myocardial infarction, non-fatal stroke, target vessel revascularisation, or any hospitalisation for heart failure related to concomitant treatment. *Confounding factors (age and sex) were adjusted for in Model 1. †Various variables associated with mortality of HD patients were adjusted for Model 2. ‡Variables known as classical cardiovascular risks were adjusted for Model 3. **P value for trend. CRP, C-reactive protein; GNRI, geriatric nutritional risk index; TGCV, triglyceride deposit cardiomyovasculopathy.
All-cause mortality and cause of death
The details of the cause of death during the follow-up period are listed in table 2. Twenty-two of 83 (27%) patients died during the 5-year follow-up. The cumulative all-cause mortality during the 5-year follow-up was 47.1% (8 out of 17 patients) in the definite TGCV group, 18.2% (4 out of 22 patients) in the probable TGCV group and 22.7% (10 out of 44 patients) in the non-TGCV control group. Death from CVDs, including acute MI, heart failure, cerebral haemorrhage and sudden death, was more frequently observed in the definite TGCV group (4 out of 17 patients, 23.5%) than in the non-TGCV control group (3 out of 44 patients, 6.8%). The ratio of cardiovascular mortality to all-cause mortality was 50% (4 out of 8 patients) in the definite TGCV group, 25% (1 out of 4 patients) in the probable TGCV group and 30% (3 out of 10 patients) in the non-TGCV control group.
Cause of deaths
Cox proportional hazard analyses
Figures 5 and 6 show the multivariate Cox proportional hazard models for the primary and key secondary endpoints, respectively, after adjusting for confounding factors (mean age and sex) in Model 1, various variables associated with mortality of HD patients (dialysis period, C-reactive protein and geriatric nutritional risk index) in Model 2, or variables known as classical cardiovascular risks (presence of hypertension, hyperlipidaemia and diabetes) in Model 3. The analysis revealed that definite TGCV was significantly and independently associated with the primary and key secondary endpoints in all three models.
Discussion
In this study, definite TGCV was diagnosed in 20% of the consecutive patients on HD with suspected CAD and 2.6% of all HD participants. We also found that the definite TGCV patients on HD were significantly and independently associated with the incidence and risk of cardiovascular mortality during the 5-year follow-up, even after adjusting for potential confounding factors.
Although cardiovascular mortality has decreased among HD patients in the past decade,1 2 it still accounts for 30%–35% of all-cause mortality events in this patient population. Accordingly, mortality rates of 65%–70% among HD patients are currently associated with non-CVDs, such as infection and cancer.25 In this study, the cumulative mortality from cardiovascular and non-CVDs in the non-TGCV control group was 30% and 70%, respectively. These rates are consistent with the mortality rates associated with cardiovascular and non-CVDs in Japan.2 However, among the definite TGCV patients, 50% of the patients died due to cardiovascular causes, which was nearly two times higher than the cardiovascular mortality rate noted among the non-TGCV control patients. This highlights the greater effect of TGCV on cardiovascular mortality, exclusively in patients with TGCV than in the non-TGCV counterparts.
Another interesting finding of this study was the significantly increased risk of composite of cardiovascular endpoints, including cardiovascular death, non-fatal MI and non-fatal stroke, in the definite TGCV patients compared with the non-TGCV counterparts. Among the three cardiovascular outcomes, the incidences of cardiovascular death, (exclusively caused by sudden cardiac deaths), and non-fatal MI were higher in the definite TGCV group than in the non-TGCV control group. Meanwhile, the incidence of non-fatal stroke was similar between the two groups. Furthermore, the incidence of CAD that require any invasive revascularisations at baseline and during the follow-up period was significantly higher in the TGCV group than in the non-TGCV control group. First reported among Japanese cardiac transplant recipients in 2008, TGCV is a novel disease concept characterised by the ectopic accumulation of TG in vascular SMCs and cardiomyocytes, resulting in CAD and heart failure, and can be at higher risk of fatal arrhythmias as observed in this study.10–12 22 For the current clinical practice, endomyocardial biopsies, cardiac CT angiography and cardiac nuclear magnetic resonance spectroscopy are alternative methods to evaluate myocardial TG deposition directly. These pathophysiological and image findings might contribute to identify the high risk patients with TGCV prone to have fatal arrythmias. Taken together with these findings, the pathological characteristics of TGCV are attributable, in part, to the increased risk of CVD and associated mortality.
HD patients have an extremely high risk of mortality, regardless of the cardiovascular and non-cardiovascular events, compared with non-HD patients. Previous studies have reported the importance of non-cardiovascular causes of death in these patients.23 24 In addition to CVD, malnutrition, inflammation and insulin resistance are all prevalent conditions that likely increase the morbidity and mortality rates among HD patients.23 24 In this study, even after adjustment of the serum C-reactive protein levels, geriatric nutritional risk index and insulin, which were related to worse prognosis in HD patients,26 definite TGCV was significantly and independently associated with an increased risk of cardiovascular outcomes.
Since TGCV is considered an orphan/rare disease, only one report is available regarding the real frequency of TGCV in daily clinical practice.27 In this context, we recently investigated the impact of TGCV on vascular failure after second-generation drug-eluting stent implantation in patients with diabetes mellitus. Among 526 consecutive diabetic patients suspected of CAD, only seven patients (1.3%) were diagnosed with definite TGCV, and proved to be at an increased risk of in-stent restenosis and TVR, compared with the non-TGCV counterparts.27 In this study, the prevalence of definite TGCV was approximately 20% among HD patients with suspected CAD and 2.6% of all HD participants. These findings suggest a relatively higher prevalence of TGCV among HD patients compared with non-HD counterparts, contributing to less effective drugs and therapeutic interventions with respect to the prevention of cardiovascular events in these populations. Further studies will be needed to identify the hypothesis.
The present data showed that patients with TGCV are a high-risk population for cardiovascular events among HD patients and that any kind of plasma lipids assessed (low-density lipoprotein cholesterol, TG and high-density lipoprotein cholesterol) were not associated with an increased risk of cardiovascular outcomes in these patients. Coronary lesions in TGCV are pathologically characterised by the massive and exclusive deposition of TG on SMCs and subsequent formation of diffuse (non-focal) and concentric (negative remodelling) stenosis with or without cholesterol-deposit atherosclerosis10 (online supplemental figure 1). To target this intracellular (but not in plasma) TG deposition, we obtained a preclinical proof of therapeutic concept with tricaprin, a medium-chain TG, in a mouse model of TGCV,28 and have finished investigator-initiated phases I, I/IIa and IIa clinical trials with tricaprin-containing capsules (CNT-01) for patients with TGCV, assigned as a SAKIGAKE designation by the Ministry of Health, Labour and Welfare, Japan, that is a fast track examination for the approval of pioneering drugs. We are also planning the phase IIb trials with CNT-01 for patients with TGCV to identify the safety and efficacy of this drug for the reduction of clinical events. In other countries, because tricaprin is a kind of medium chain TG which has the 50-year-history for clinical use, it could be considered as a medical food or supplement for dietary therapy, depending on the legislation and law in each country. Further studies will be needed to confirm the effectiveness of this therapy among HD patients with TGCV.
Supplemental material
Limitations
There are several limitations to this study. The main limitation is the relatively small number of study subjects, especially control subjects, considering the low frequency of TGCV. However, this is the first study to report that 20% of consecutive HD patients with suspected CAD develop TGCV and are at a higher risk of CVD and all-cause mortality; thus, TGCV may be a therapeutic target for this population. Second, since BMIPP scintigraphy, which is only available in Japan and is well established concerning the risk stratification in HD patients,29 30 is a key tool for the diagnosis of TGCV, simple screening methods are needed in other countries to identify patients with suspected TGCV. Finally, given an orphan/rare nature of TGCV, patient selection is also challenging. Therefore, further improvement of the diagnostic criteria and patient selection of TGCV will be needed for the better classification and selection of patients with suspected TGCV.
Conclusions
TGCV is not uncommon in HD patients and is associated with an increased risk of cardiovascular events including cardiovascular death. Thus, TGCV might be a potential therapeutic target among these populations.
Key messages
What is already known on this subject?
Triglyceride deposit cardiomyovasculopathy (TGCV) was recently identified as an orphan disease in Europe in 2019 (Orphanet ORPHA Number: 565612). However, the degree of association between TGCV and cardiovascular mortality among haemodialysis (HD) patients is unknown.
What might this study add?
In this observational cohort study that included 83 consecutive HD patients with suspected coronary artery disease (CAD), definite TGCV was associated with an increased risk of cardiovascular events, including cardiovascular death, even after adjustment of potential confounding factors.
How might this impact on clinical practice?
The prevalence of definite TGCV was approximately 20% among consecutive HD patients with suspected CAD. Thus, TGCV might serve as a potential therapeutic target for these populations.
Acknowledgments
We thank our colleagues from Osaka University Center for Medical Data Science, Advanced Clinical Epidemiology Investigations Research Project for providing their insight and expertise to our research.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors YN and TA conceived of the presented idea. YN and KH developed the theory and performed the computation. HA and HT devised the project. TN, AT and SS worked out almost all of the technical details. HI and HT verified the analytical methods. TO wrote the manuscript, with help from TA. All authors provided critical feedback and helped shape the research and manuscript. TA and KH are responsible for the overall content as guarantors.
Funding This work was supported by research grants from the Ministry of Health, Labour and Welfare and the Japan Agency of Medical Research and Development [A-MED; grant number 17ek0109092h0003] and Grant-in-Aid for Scientific Research [KAKENHI; grant number 19K11705].
Competing interests KH has a licensed patent (WO2013031729) and has received a research grant from Nihon Medi-Physics Co. YN receives lecture fees from Mitsubishi Tanabe Pharma Co., Eli Lilly Japan KK and Nippon Boehringer Ingelheim Co., Ltd. HI receives lecture fees from Astellas Pharma, AstraZeneca, Bayer Pharmaceutical Co., Ltd., Chugai Pharma Inc., Daiichi-Sankyo Co., Ltd. and MSD KK. TA receives lecture fees from Astellas Pharma, AstraZeneca, Bayer, Daiichi Sankyo and Bristol-Myers Squibb.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Patient consent for publication Not required.
Ethics approval This study was conducted following the guidelines of the Declaration of Helsinki. The Ethics Committee of the Narita Memorial Hospital (R1-23-02) approved the study, and written informed consent was obtained from all patients or their families.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available upon reasonable request.