Article Text

Statistics from Altmetric.com
- advanced heart failure therapies (LV assist devices
- total artificial heart)
- heart failure
- cardiac arrhythmias and resuscitation science
- acute myocardial infarction
- pharmacodynamics
Learning objectives
Review the common cardiovascular aetiologies presenting to intensive care and associated physiology.
Outline a clinical approach to the assessment of the unstable cardiovascular patient and relevant investigations.
Summarise the pharmacological and mechanical management strategies for patients requiring intensive care admission with cardiovascular disease.
Introduction
Despite a decline in mortality related to cardiovascular disease (CVD) over the last three decades, the prevalence of CVD remains high.1 Acute heart failure (AHF) is the most common emergency admission in patients above 65 years old, causing 5% of all emergency admissions with an inpatient mortality of 11%.2 One in five patients hospitalised with heart failure in the USA is admitted to an intensive care unit (ICU),3 and 31.9% of admissions for cardiogenic shock (CS) due to acute myocardial infarction were complicated by multiorgan failure.4 The contemporary ICU therefore has to have the expertise to manage acute cardiovascular care across an increasing breadth and complexity of cardiovascular conditions either as the presenting pathology or as a comorbid condition in critically unwell patients admitted for other reasons.5
This review outlines an approach to the unstable cardiovascular patient on the ICU. We will review the assessment and management of patients requiring intensive care admission with cardiovascular disease, the common aetiologies, associated investigations and the range of support modalities available on the ICU.
Physiology
The underlying processes of AHF and CS are based on four key physiological concepts: contractility, preload, afterload and electrical conductivity.
Contractility
Contractility or inotropy describes the heart’s inherent ability to eject blood for a given preload and afterload. A loss of contractility causes systolic dysfunction. This loss of inotropy results in a decreased stroke volume, increasing the end systolic volume. This in turn prompts a rise in preload. A compensatory increase in end diastolic volume helps to maintain stroke volume by activating the Frank-Starling mechanism, but consequently causes pulmonary congestion and oedema. Measuring contractility at the bedside is complex. Echocardiographic parameters such as ejection fraction and tricuspid annular plane systolic excursion are useful markers of contractility in normal physiological conditions, and they are heavily influenced by changes in preload and afterload, making determination of contractility in isolation difficult.6
Preload
Ventricular preload is cardiomyocyte stretch at the end of diastole. Preload determines the end diastolic volume of the ventricle and is an important factor determining stroke volume. Preload is primarily reliant on passive ventricular filling and ventricular compliance; however, atrial systole contributes significantly to end diastolic volume.
Ventricular compliance is compromised by cardiac disorders such as ventricular hypertrophy, myocardial infarction and the normal ageing process.6 A hypertrophied ventricle is no longer adequately filled passively or with atrial systolic contribution, leading to diastolic heart failure and impaired lusitropy, which is the ability of the myocardium to relax following excitation contraction coupling. Left atrial pressure is therefore augmented by a number of processes, including accumulation of venous blood upstream, increased venous tone and sodium retention. The consequence of this is pulmonary oedema. Diastolic filling is now more reliant on an adequate diastolic duration; therefore, an increase in heart rate (chronotropy) reduces the time for ventricular filling, exacerbating the diastolic dysfunction further.
Afterload
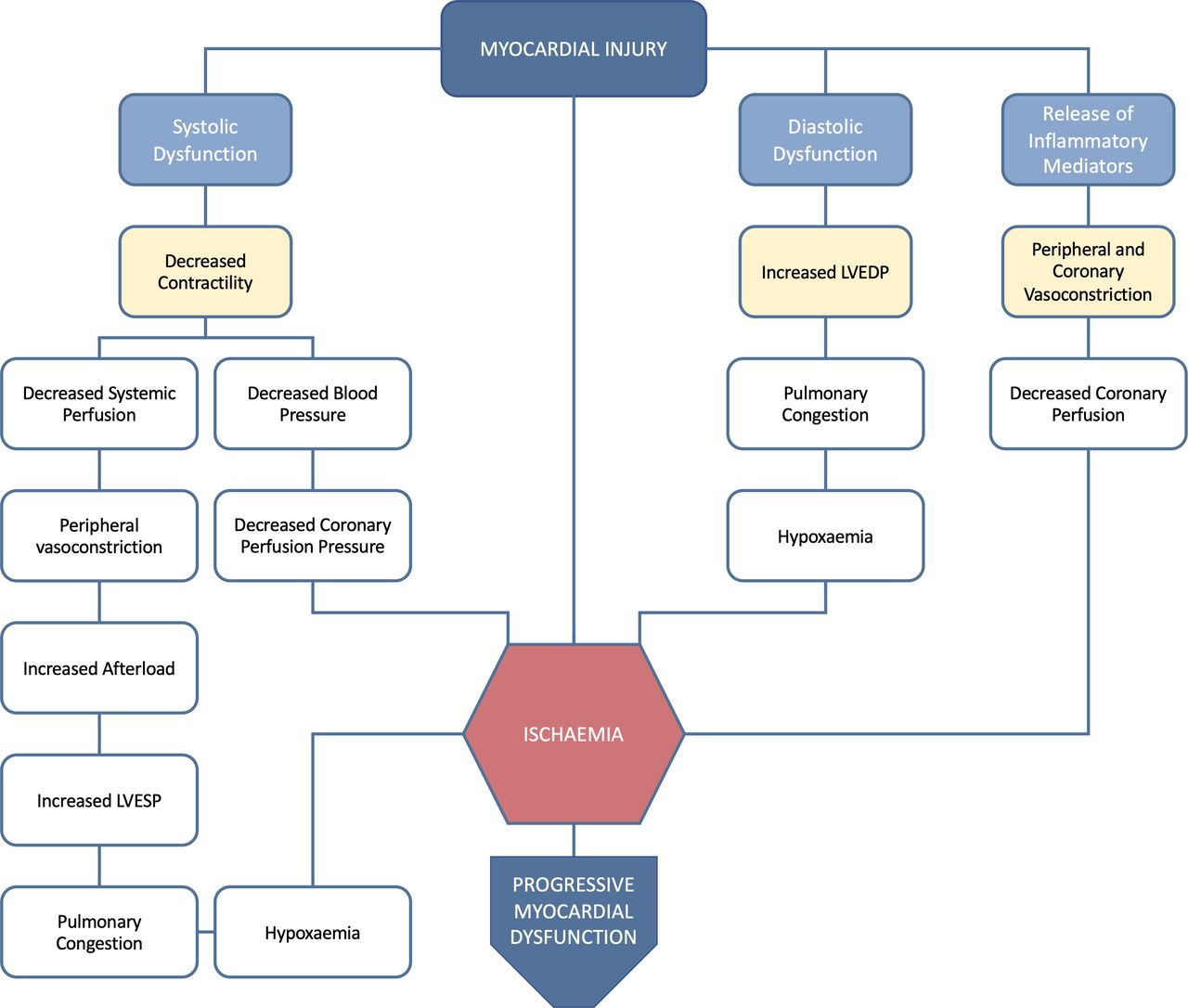
Deleterious circulatory compensation can exacerbate shock. Peripheral vasoconstriction has the benefit of improving coronary and peripheral perfusion, but increases afterload. Afterload is the force opposing ejection of blood from the left ventricle (LV) during systole overcome by LV wall stress. A sudden increase in afterload results in an increased end systolic pressure, a reduced stroke volume and a subsequent reduction in cardiac output (CO). In healthy individuals this is overcome by increasing ventricular diastolic volume and LV contractility. Chronic elevations in afterload in conditions such as aortic stenosis and hypertension lead to compensatory adaptations of the LV. In the context of acute CS, cardiac injury provokes a spiral of physiological events, which in turn propagates cardiac dysfunction (figure 1).

Physiological cascade of cardiac dysfunction following myocardial injury. LVEDP, left ventricular end diastolic pressure; LVESP, left ventricular end systolic pressure.
Electrical conductivity
Cardiac arrhythmias and conduction disturbances are an important cause of morbidity and can be potentially life-threatening due to their profound effects on inotropy, lusitropy and stroke volume particularly in the structurally abnormal or already failing heart. For example, atrial kick is largely redundant in healthy adults, as 80% of the blood flows passively into the ventricles during the rapid filling phase. However, in patients with tachycardia, the time of ventricular diastole is reduced, which leads to dependence of the ventricular filling on the atrial kick. Further, increased ventricular stiffness and diastolic dysfunction reduce the rapid filling phase and early diastasis, creating dependence of atrial kick and loss of CO of up to 30%7 and even more profound effects in right ventricular (RV) dysfunction. Loss of atrial kick occurs in RV infarction, atrial fibrillation (AF), atrial flutter and complete heart block.
Given that the mean arterial pressure equals CO multiplied by systemic vascular resistance, and CO comprised heart rate multiplied by stroke volume, it follows that altered electrical conduction (dromotropy), specifically bradycardia, can significantly worsen heart failure, including valvular heart disease, with risk of progression to CS. Multiple factors may be associated with atrioventricular block, including acute and chronic ischaemia, degenerative disease, acute inflammatory disease (particularly fulminant myocarditis), chronic inflammatory disease (eg, cardiac sarcoidosis), electrolyte disturbance (eg, hyperkalaemia) and medications.
Any tachycardia of atrial or ventricular origin will increase myocardial oxygen demand, while simultaneously decreasing myocardial blood flow due to the shortened diastolic time and reduced ventricular preload which may impact stroke volume and CO, particularly when the ventricular rate is greater than 160 beats per minute. Abnormal ventricular conduction further compromises stroke volume through impaired synchrony and efficiency of ventricular contraction.
General approach
AHF is the most common manifestation of cardiovascular pathology on the ICU and represents a clinical syndrome resulting from any structural or functional cardiac disorder that impairs the ability of the ventricle to fill with or eject blood. AHF may be caused by disease of the myocardium, pericardium, endocardium, heart valves, vessels, or by metabolic disorders including thyroid and growth hormone disorders.8 Initial clinical evaluation should follow international guidance,8–10 adopting an aetiologically directed approach following the CHAMP acronym: acute Coronary syndrome, Hypertension emergency, Arrhythmia, acute Mechanical cause, Pulmonary embolism, in the first instance (table 1). Having excluded aetiologies which require immediate, potentially life-saving intervention, clinicians should proceed with further diagnostic modalities (extended medical and family history, re-examination, comprehensive cardiac (and non-cardiac) imaging, blood tests) and subspecialty input to diagnose less emergent causes of AHF syndromes, which are reviewed elsewhere.10
Aetiologies of acute heart failure syndromes
CS, the most severe manifestation of AHF, is a medical emergency and describes a constellation of clinical signs and physiological perturbations, which may be the result of a de novo acute catastrophic deterioration in ventricular function, most commonly acute myocardial infarction, or decompensation of stable or progressive chronic heart failure. CS presents with signs of systemic tissue hypoperfusion (oliguria, cold peripheries, altered mental status, lactate >2 mmol/L, metabolic acidosis) secondary to inadequate CO despite an adequate circulating volume. Supportive haemodynamic criteria include a sustained (>30 min) systolic blood pressure <90 mm Hg, with a cardiac index <1.8 L/min/m2 without haemodynamic support or <2.2 L/min/m2 with support, and a pulmonary capillary wedge pressure >15 mm Hg.11–14
A systematic approach should be taken when assessing and managing the sick cardiovascular patient, with careful consideration of the likely underlying process(es). In addition to urgent coordination of the multidisciplinary team in order to expedite the optimal interventions, it is imperative to restore adequate tissue perfusion. A thorough clinical examination is essential and should be undertaken with a specific focus on the assessment of peripheral perfusion and volume status. Two-thirds of patients in CS present with the classic ‘cold-wet’ profile. Patients with decompensated chronic heart failure tend to present in euvolaemic or ‘cold-dry’ CS and are generally responsive to diuresis and afterload reduction. Conversely, inflammatory mediators can induce pathological vasodilation, decreasing the afterload associated with a ‘warm-wet’ presentation (figure 2).15
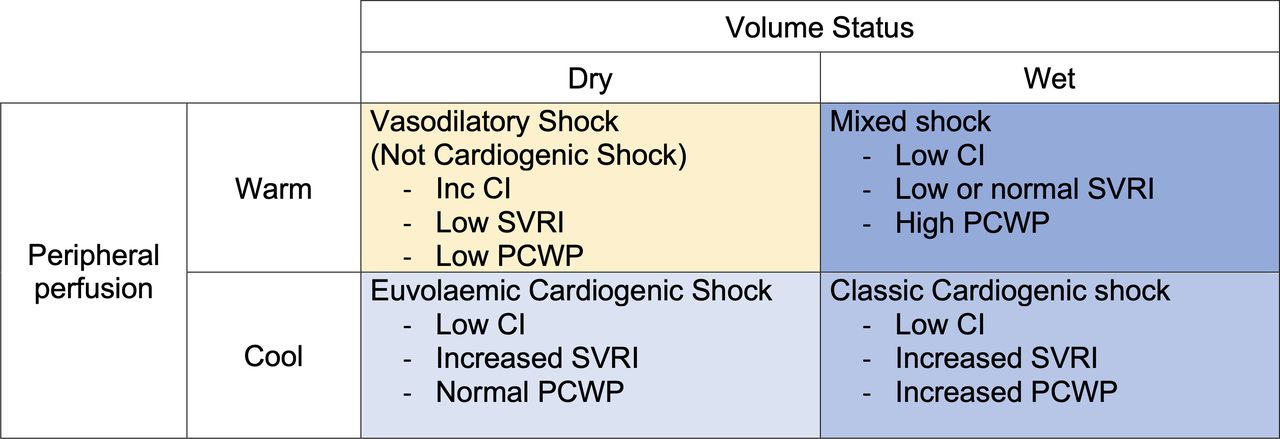
Cardiogenic shock profiles and associated cardiac indices. CI, cardiac index; PCWP, pulmonary capillary wedge pressure; SVRI, systemic vascular resistance index.
Chest X-ray and ECG are essential to identify aetiologies which require immediate and specific management such as tension pneumothorax, arrhythmia or myocardial infarction. Arterial blood gas analysis allows rapid assessment of gas exchange and metabolic derangement, specifically acidosis, which may compound myocardial dysfunction. Lactate measurement may provide an indication of the severity of organ hypoperfusion. Renal and hepatic derangements are common and should be quantified,16 while troponin, although non-specific, may direct clinicians to aetiologies associated with myocardial cellular injury, including ischaemia and myocarditis. Reassessment is imperative to monitor clinical course and response to therapies.
Early and high-quality imaging with echocardiography (with or without lung ultrasound) is essential to identify mechanical and structural issues meriting urgent percutaneous or surgical intervention. Echocardiography also enables the assessment of ventricular (and atrial) size and function, plus quantification of filling pressures, which may have therapeutic and prognostic implications. Additionally, it allows correlation with existing imaging and evaluation and optimisation of response to therapies, for example fluid administration (or removal), vasoactive drugs and support placement of mechanical circulatory support (MCS).
Management of the acutely unwell patient with cardiovascular disease
Management of cardiovascular instability of any aetiology increasingly mirrors the paradigm of acute coronary syndromes, whereby general and specific interventions should occur within the first 60–120 min of presentation to prevent progression to irreversible or lasting non-cardiac organ dysfunction (figure 3).10

{kind=link}
{kind=link}
{kind=link}
Management principles of acute cardiogenic shock. ABG, arterial blood gas; CHAMP, acute Coronary syndrome, Hypertension emergency, Arrhythmia, acute Mechanical cause, Pulmonary embolism; CO, cardiac output; CPAP, continuous positive airway pressure; ; MCS, mechanical circulatory support; MDT, multidisciplinary team; NIPPV, non-invasive positive-pressure ventilation; PPV, positive pressure ventilation; RHC, right heart catheterisation.
Airway and respiratory management
Associated respiratory compromise is common, both as a precipitant of ICU admission and as a sequela of progressive cardiac failure on the ICU. Normalisation of arterial oxygen saturation is critical to facilitate adequate tissue oxygenation. Cardiogenic pulmonary oedema inhibits the transfer of gas across alveolar membranes, contributing to hypoxia and hypercarbia, which can have negative effects of coronary perfusion and pulmonary vascular resistance (PVR). The use of non-invasive positive pressure ventilation (NIPPV) recruits alveoli, redistributes extravascular lung water, and improves compliance and surfactant production, therefore reducing shunt and work of breathing. NIPPV has been associated with a reduction in endotracheal intubation rates and hospital mortality.17
Deteriorating respiratory function despite NIPPV or acute deterioration prior to a trial of NIPPV may necessitate intubation and ventilation. Positive pressure ventilation (PPV) can impart favourable cardiovascular changes in patients with haemodynamic instability. PPV can lower pulmonary wedge pressure, LV afterload, myocardial oxygen demand and work of breathing, and improves cardiac index and oxygenation.18
Conversely, the effects of anaesthetic induction required to initiate PPV can destabilise the failing heart and reduce CO due to impairment of venous return, with consequent reduction in RV preload as well as increases in RV afterload due to increased PVR. This has consequences for LV preload and CO, particularly in those with predominant RV failure. Timing of initiation of PPV and anticipation of complications are therefore essential.
Finally, as patients emerge from sedation and switch from assisted to spontaneous breathing, there can be activation of the sympathoadrenergic system with predictable consequences on heart rate, blood pressure and afterload.
Circulatory management
Any patient in a low CO state should undergo urgent comprehensive assessment including echocardiography,19 with cardiology specialty input depending on the likely aetiology. Where CS complicates acute coronary syndrome, immediate coronary angiography is recommended (within 2 hours from hospital admission) with intent to achieve complete revascularisation.20 This may mandate transfer to a centre with 24/7 angiography capability. Similarly, those patients with an acute mechanical problem (eg, free wall rupture or acute mitral regurgitation) should be discussed with a surgical centre and urgent (within 12 hours) intervention considered.21
Aside from management of specific precipitants, prompt correction of associated metabolic disturbances, optimisation of cardiac preload and afterload, and restoration of organ perfusion are the therapeutic goals. The hypoxaemia and lactic acidosis associated with CS can exacerbate myocardial depression both directly and by limiting responsiveness to vasopressors. Fluid challenge with a balanced solution is recommended as first-line treatment of hypotension without overt fluid overload.10 Ultimately, restoration of adequate CO is essential to prevent a spiral towards multiorgan failure and potential death. This often necessitates the addition of vasoactive drugs and, in the most severe cases, consideration of candidacy for MCS.
Vasoactive drugs
The aim of vasopressors and inotropes is to restore organ perfusion through optimisation of CO and blood pressure. There is currently a paucity of evidence on which a firm recommendation for the choice of the first vasopressor or inotrope in patients with a low CO state can be made.8–10 Regardless of the choice of drug(s), efforts should be made to minimise both the number of agents and their dose; inotropes improve myocardial contractility and performance at the expense of increased myocardial oxygen consumption and arrhythmia risk while vasopressors may increase afterload and cardiac work.
Common among most vasoactive drugs is their influence on the release and utilisation of intracellular calcium. Further classification of these drugs can be achieved by considering how they augment cardiac contractility at a cellular level: by increasing intracellular levels of cyclic adenosine monophosphate (class I); effects on ion channels or pumps (class II); modulation of intracellular calcium regulation (class III); and augmentation through multiple pathways (class IV). Classification is helpful to conceptualise the benefits and limitations of each agent. A summary of the effects of vasoactive drugs is outlined in table 2.
Summary of the effects of commonly used vasoactive drugs on intensive care at the cellular level
Dobutamine is recommended for treatment of moderate hypotension (70–100 mm Hg systolic) following myocardial infarction, without clinical features of shock.22 In CS of any aetiology, the use of dobutamine or milrinone should be considered early. Vasodilatory effects, necessitating coadministration with a vasopressor, often limit their use. Norepinephrine should be regarded as the first-line vasopressor (table 3); it is non-inferior to dopamine, and dopamine has demonstrated worse outcomes in the CS subgroup with the attendant risks of arrhythmias.23 Vasopressin is increasingly deployed as a norepinephrine sparing vasopressor and in the context of right heart failure owing to its pulmonary vasodilatory properties. Epinephrine should be restricted to patients with persistent hypotension despite adequate cardiac filling pressures as it has not been shown to be superior to alternatives and its use has been associated with lactic acidosis, tachyarrhythmias and gastric malperfusion.23
Vasoactive management of cardiogenic shock profiles
Assessment of clinical response to all interventions should occur serially through a combination of clinical assessment, biochemical (lactate, central venous oxygen saturations) and haemodynamic variables (echocardiography, CO, cardiac index and pulmonary capillary wedge pressure). Continuous haemodynamic monitoring is essential to allow early identification of changes in clinical condition and titration of both pharmacological therapies and MCS, which are often used in tandem. Central venous cannulation permits the safe administration of vasoactive drugs and allows monitoring of right atrial pressures and central venous gases, a surrogate assessment of tissue oxygen delivery and utilisation.
Consensus on the optimal method of haemodynamic monitoring in CS is lacking, although invasive monitoring with an arterial line in addition to continuous ECG should be considered at a minimum.10 A range of CO devices exist using either thermodilution or bolus indicator dilution. None has demonstrated superiority or outcome benefit; nonetheless, pulmonary artery catheterisation is advocated in the management of CS to aid diagnosis and monitor response to interventions.16 Use of any CO monitoring should be determined by local availability, safety profile and clinical context of the patient. Where a commensurate physiological response is not being achieved despite escalating pharmacotherapy, discussion with a centre with MCS capability should be considered.
MCS devices
MCS is an umbrella term for a range of devices that include the intra-aortic balloon pump, extracorporeal membrane oxygenation, ventricular assist devices and total artificial hearts. No device is ideal and the choice of device for specific patients is complex and based on the urgency of patient need, institutional capabilities and experience, need for univentricular/biventricular support, likelihood of cardiac recovery, patient comorbidities and lung function. An overview of these devices is covered in the online supplemental material.
Supplemental material
Other haemodynamic interventions
Pulmonary vasodilators
The general principles of RV dysfunction and management are summarised in table 3 and elsewhere.24 25 Reduction of RV afterload can be achieved with correction of hypoxia, hypercarbia (which increase PVR) and acidosis, which may affect RV contractility. If these fail, inhaled pulmonary vasodilators, inhaled nitric oxide and prostacyclin analogues may be trialled. Both appear safe and effective in improving pulmonary haemodynamics in RV failure with no clear comparative data but with prostacyclin analogues offering substantial cost savings. Dose should be titrated to measured mixed venous oxygen saturation, right atrial pressure, PVR and right heart CO.
Management of rhythm disorders
Given the effects on physiology outlined above, severe rhythm disturbances in patients with CS should be corrected urgently.26 27 The choice between medical therapy, electrical cardioversion and temporary pacing will be guided by the specific bradycardia or tachyarrhythmia coupled with patient physiology. In patients with hypotension, that is, those with CS, resuscitation guidelines recommend immediate electrical cardioversion where appropriate.28
Reflecting the consequences on CO through loss of atrial kick, re-establishment of sinus rhythm is desirable, particularly in patients with underlying heart disease. A detailed summary of the management of AF, the most common arrhythmia in ICU, is summarised elsewhere.29 30 Similarly, pharmacological chronotropy, for example, isoprenaline, a non-selective β adrenoreceptor agonist or transvenous pacing, may be indicated in patients with bradycardia and a low CO state.
Cardiac tamponade
Cardiac tamponade is acute circulatory failure secondary to compression of the heart chambers by a pericardial effusion. Pericardial pressures exceed intracardiac pressures, impairing diastolic cardiac filling, and ultimately CO. Presentation is often non-specific and dependent on the rapidity of pericardial fluid accumulation. Accordingly, a high index of suspicion should be maintained, particularly in any patient who has had a recent (within 3 weeks) cardiac surgery or myocardial infarction.
Supportive signs include oliguria, low CO in the presence of elevated filling pressures, ‘pulsus paradoxus’ (an inspiratory decrease in systolic blood pressure >10 mm Hg) and electrical alternans. Tamponade is a clinical diagnosis confirmed by either transthoracic or transoesophageal echocardiography.31 32 Immediate management should include intravascular volume expansion. Vasoactive medications may further temporise physiological decline, but definitive drainage of the pericardial effusion should be sought. The European Society of Cardiology has produced a triage tool to guide the timing of any intervention including referral to a specialist centre.33 Pericardiocentesis may worsen RV dilatation and function in the context of severe pulmonary hypertension and should be undertaken with caution.
Sedation
A full review of sedation options in cardiovascular patients has been published elsewhere.34 Nonetheless, it is important to understand some specific circumstances where sedation may be of benefit in the management of cardiovascular disease.
Usually a combination of opiates (eg, fentanyl, morphine) and hypnotics (eg, propofol, midazolam) are titrated according to established sedation scales.35 The use of opiates appears to be safe in the failing heart. Opiates may have specific benefit in refractory ventricular arrhythmias, where they exert antiarrhythmic effects and may be a therapeutic manoeuvre in ventricular tachycardia storm. Propofol either as a bolus or infusion may lead to hypotension through direct vasodilation and should be used with caution in patients with afterload sensitive conditions, for example hypertrophic cardiomyopathy. The alpha agonists dexmedetomidine and clonidine can cause bradycardia and hypotension at low doses, while at higher doses they may induce hypertension.36 Accordingly, they should be used with caution in patients with heart block or on other rate-limiting drugs. Antipsychotics should be avoided in the arrhythmic heart; they delay myocardial repolarisation, increasing the risk of torsade de pointes, particularly in those receiving other QTc-prolonging medications.37 Sedation in patients who have suffered cardiac arrest is required to manage seizure activity or myoclonic jerk suppression, shivering in temperature-controlled patients, and facilitation of controlled ventilation to optimise cerebral perfusion. Short-acting opioids and hypnotics are usually used to enable more reliable and earlier neurological assessment and prognostication.38
Renal support
In critically ill patients, acute kidney injury (AKI), defined by alterations in serum creatinine and low urine output,39 is common, and one in four patients admitted with heart failure.40 The development of AKI is associated with poor outcomes.41 The cardiovascular aetiologies are a combination of venous congestion caused by right heart failure and neurohormonal activation; aggravation of venous congestion by liberal fluid administration to manage hypotension and hypoperfusion; a low cardiac state with associated reductions in renal perfusion pressure; and the use of nephrotoxic drugs including contrast agents.42–44
Management of AKI is supportive and should be targeted towards managing the inciting pathology as a priority but also any optimisation of cardiac physiology to promote renal recovery. A practical approach to diuretic treatment has been extensively described elsewhere.45 The optimal timing of initiation of renal replacement therapy remains unclear aside from clear indications of severe hyperkalaemia, marked metabolic acidosis or refractory fluid overload. Early ultrafiltration in fluid overload compared with diuretic therapy may allow accelerated fluid removal but confers limited short-term outcome benefit.46–48
The refractory patient
Heart transplantation
Although the gold standard intervention, heart transplantation remains a limited therapeutic option for eligible patients with refractory heart failure. ICU admission is often the defining event that triggers urgent assessment due to acute progression of underlying heart disease or acute, irreversible manifestations of de novo disease. Short-term or durable ventricular assist devices may allow stabilisation and even normalisation of organ failures and pulmonary hypertension. Early discussion with the regional transplant centre is warranted to inform patient management and transfer to establish candidacy for cardiac transplantation.
End of life, palliative care and shared decision-making
Given the high mortality of cardiac patients admitted to ICU, goal-setting, a comprehensive understanding of patient wishes and recognition of futility are essential components of care. Palliative care provides an opportunity for patient-centred management, with shared decision-making on available treatment options, advanced care planning, and attention to physical, emotional, spiritual and psychological needs.49 Integration of palliative care services into the ICU as well as education and training of ICU clinicians are essential to maximise benefits to patients and their families and to minimise harm from unnecessary and potentially futile interventions.50
Conclusion
Owing to the prevalence of heart disease in general and AHF as an admission diagnosis, cardiac presentations are commonplace in ICUs. Exclusion of ischaemic aetiologies and combined decision-making between ICU and cardiology are essential. Tenets of management include rapid diagnostics, alignment of clinical examination with imaging, biochemical and physiological data, and reassessment of these data in response to intervention. Engagement of the multidisciplinary team to explore options for intervention, escalation to MCS, transplantation or palliative care should be undertaken to ensure patient-centred, individualised care.
CME credits for Education in Heart
Education in Heart articles are accredited for CME by various providers. Toanswer the accompanying multiple choice questions (MCQs) and obtain yourcredits, click on the ‘Take the Test’ link on the online version of the article.The MCQs are hosted on BMJ Learning. All users must complete a one-timeregistration on BMJ Learning and subsequently log in on every visit using theirusername and password to access modules and their CME record. Accreditationis only valid for 2 years from the date of publication. Printable CME certificatesare available to users that achieve the minimum pass mark.
Key messages
Contemporary intensive care units (ICUs) deliver acute cardiovascular care to an increasing breadth and complexity of cardiovascular conditions.
The underlying processes of acute heart failure and cardiogenic shock are based on four key physiological concepts: contractility, preload, afterload and electrical conductivity.
Initial clinical evaluation should adopt an aetiologically directed approach following the CHAMP acronym (acute Coronary syndrome, Hypertension emergency, Arrhythmia, acute Mechanical cause, Pulmonary embolism) with multimodal assessment.
A close relationship between the ICU, subspecialties of cardiology and other medical specialties is pivotal to managing all cardiac presentations in the ICU.
Inopressor therapy should target effective tissue perfusion and normalisation of cellular metabolism with regular re-evaluation of response to set physiological and biochemical targets.
Optimisation of ventilation, sedation and renal support can significantly modify cardiovascular physiology.
Options for patients refractory to conventional haemodynamic support include mechanical circulatory support, heart transplantation and end-of-life care.
Ethics statements
Patient consent for publication
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @stephen_t_webb
Contributors DJC, AP: structure, initial drafts, subsequent revisions. SW: revision and final approval.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Commissioned; internally peer reviewed.
Author note References which include a * are considered to be key references.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.