Article Text

Abstract
Objective Waiting time is inevitable during cardiovascular (CV) care. This study examines whether waiting room-based CV education could complement CV care.
Methods A 2:1 randomised clinical trial of patients in waiting rooms of hospital cardiology clinics. Intervention participants received a series of tablet-delivered CV educational videos and were randomised 1:1 to receive another video on cardiopulmonary resuscitation (CPR) or no extra video. Control received usual care. The primary outcome was the proportion of participants reporting high motivation to improve CV risk-modifying behaviours (physical activity, diet and blood pressure monitoring) post-clinic. Secondary outcomes: clinic satisfaction, CV lifestyle risk factors (RFs) and confidence to perform CPR. Assessors were blinded to treatment allocation.
Results Among 514 screened, 330 were randomised (n=220 intervention, n=110 control) between December 2018 and March 2020, mean age 53.8 (SD 15.2), 55.2% male. Post-clinic, more intervention participants reported high motivation to improve CV risk-modifying behaviours: 29.6% (64/216) versus 18.7% (20/107), relative risk (RR) 1.63 (95% CI 1.04 to 2.55). Intervention participants reported higher clinic satisfaction RR: 2.19 (95% CI 1.45 to 3.33). Participants that received the CPR video (n=110) reported greater confidence to perform CPR, RR 1.61 (95% CI 1.20 to 2.16). Overall, the proportion of participants reporting optimal CV RFs increased between baseline and 30-day follow-up (16.1% vs 24.8%, OR=2.44 (95% CI 1.38 to 4.49)), but there was no significant between-group difference at 30 days.
Conclusion CV education delivery in the waiting room is a scalable concept and may be beneficial to CV care. Larger studies could explore its impact on clinical outcomes.
Trial registration number ANZCTR12618001725257.
- education
- delivery of health care
- chest pain
- quality of health care
- health care economics and organizations
Data availability statement
Data are available on reasonable request. Deidentified study data will be made available to researchers who provide a methodologically sound proposal and after the signing of a non-disclosure agreement. To submit a data use proposal, please email the principal investigator at clara.chow@sydney.edu.au.
Statistics from Altmetric.com
- education
- delivery of health care
- chest pain
- quality of health care
- health care economics and organizations
Introduction
Patient education is an integral aspect of disease management and prevention. Among those with cardiovascular disease (CVD), low health literacy is an independent predictor of mortality.1 Furthermore, as poor survival rates from out-of-hospital cardiac arrest (OHCA) gain increased attention,2 community education in cardiopulmonary resuscitation (CPR) is becoming an important focus of OHCA management guidelines.3 Patients with CVD use healthcare more than the general population,4 and for each contact waiting roomtime is often longer than consultation time.5 This time could be used to deliver health information, but delivery of generic information is associated with little effect.6 Digital health technology presents an opportunity to deliver targeted interventions to patients while they wait, providing information on health conditions of interest and their risk factors.
Video-based educational interventions are feasible to deliver in waiting rooms, potentially scalable to large populations, and there is some evidence supporting their potential health benefit.7 One randomised clinical trial (RCT) of video-based education delivered to 327 women prior to their antenatal clinic appointment demonstrated a significant improvement in knowledge, exercise, and diet behaviours compared with control.8 Yet, another RCT of a stroke educational video delivered to 329 waiting non-acute emergency department patients failed to demonstrate any improvement in CVD-related lifestyle metrics at 3 months.9 Another small (n=100) emergency department-based RCT found participants who watched a 1 min CPR educational video performed CPR better than a control.10 To our knowledge, there are no examples of education provision to waiting cardiology patients. This population reports high motivation to make behaviour change,11 demonstrates a strong interest in CPR education,12 and may be more receptive to receiving CVD-focused education than unselected populations from primary care or the emergency department. Motivation is a key precursor to lifestyle change in educational interventions,13 and self-reported confidence to perform CPR is commonly used to describe layperson attitudes towards CPR.14
The While You’re Waiting study aimed to examine in an RCT the effectiveness of a patient-centred, CVD-focused educational intervention in the waiting room of daily-run Rapid Access Cardiology (RAC) clinics15 on motivation to improve CVD-risk modifying behaviours, satisfaction with clinic services and lifestyle behaviours. In a parallel sub-study, we examined the effectiveness of additional CPR-specific education on confidence to perform CPR in the community.
Methods
Study design
While You’re Waiting is a single-centre, single-blind, 2:1 parallel designed RCT of patients in the waiting room of a RAC within a tertiary teaching hospital in Sydney, Australia (figure 1). The methods and intervention are described in detail elsewhere.16 The study was delivered via a REDCap survey tool on a computerised tablet device with the support of trained research staff. This integrated consent, randomisation, baseline data collection, and video delivery if the participant was randomised to intervention.

Enrolment of participants in the While You’re Waiting Randomised Clinical Trial. CPR, cardiopulmonary resuscitation.
Participants
The study population was patients presenting to RAC, Westmead Hospital (Sydney, Australia). The RAC is a cardiologist-led, hospital co-located clinic that provides assessment and management of low-intermediate risk patients with suspected coronary heart disease.15 Many patients presenting to this clinic have multiple CVD risk factors.17 Thus, targeting this patient population with CVD risk factor education presents an opportunity to increase CVD health literacy, lifestyle change, motivation, and ultimately health outcomes.
Patients older than 18 years were eligible. Those too unwell (physically or mentally) to complete surveys and/or watch videos or with insufficient English language competency to provide informed consent were excluded. A log was kept of all participants screened. All participants provided informed consent via an eConsent integrated into the delivery platform.
Patient and public involvement
The intervention was co-designed with patients, consumers, healthcare providers and researchers and is detailed elsewhere.16 Briefly, 21 patients with CVD identified through a consumer organisation contributed to identifying appropriate video content for the intervention programme through rating videos on content utility and likelihood of motivating lifestyle change. Survey data from consumers on CPR confidence informed the sample size calculation for the trial. The 2:1 randomisation design enabled more participants to receive the intervention, and control participants were offered the intervention after the trial. Integration of consent, baseline data collection, intervention delivery and outcome assessment was designed to reduce participant time burden. We plan to disseminate study results to participants following publication.
Randomisation
Participants were randomised 2:1 (intervention:control). The randomisation sequence was developed by the study statistician (SM) using the Randomise R library of R statistical software (V.3.5.1) in blocks of 3. The intervention allocation sequence was incorporated into RedCap such that treating clinic doctors, recruiting staff and outcome assessors were blinded to patient treatment allocation. Due to constraints of the RedCap randomisation stratification module that requires participants to be randomised on a separate device, impacting both study flow and blinding, the decision was taken to not stratify randomisation according to baseline characteristics.
Intervention programme
The intervention programme comprised a curated series of cardiovascular risk modification videos delivered on tablet computer devices in the clinic waiting room. Video selection occurred as previously described.16 All videos were from reputable sources (including the Australian and British Heart foundations, Healthy WA, and the Better Health Channel) and did not contain advertisements.
Intervention participants were initially asked about their: (1) level of health knowledge (low, medium or high) and (2) topics of interest (physical activity, medications, diet, hypertension, heart attack or general education). According to a pre-specified algorithm, this information was used to select a set of videos for the participant to watch. Videos highly rated by staff and consumers were presented first. It was expected the number of videos watched would vary according to participant preference and length of wait. When the patient was called in for their appointment or they had finished the programme, the tablet was returned to clinic administration staff.
Cardiopulmonary education: a random sub-sample of intervention participants received another video on compression-only CPR prior to receiving their customised list of CVD videos.
Control
Following completion of eConsent and baseline surveys on study tablets, control participants proceeded through usual care in the clinic waiting room, which comprised of educational posters/pamphlets and a small central television.
Trial procedures
All participants were assessed on three separate occasions:
Baseline: demographic information, self-reported lifestyle behaviours, CPR confidence (online supplemental appendix 1).
Immediately post-clinic: motivation to improve diet, exercise and blood pressure monitoring, satisfaction with clinic experience, and CPR confidence, willingness and knowledge (online supplemental appendix 2).
Thirty-day follow-up: self-reported levels of CV lifestyle risk factors, motivation to improve diet and exercise, CPR-related items (online supplemental appendix 3).
Supplemental material
Supplemental material
Supplemental material
Baseline clinical and medical history assessment was collected from routine clinical management systems. All other information was collected on study tablets via participant self-report.
Primary outcome (post-clinic)
Highly motivated to improve CVD-health related behaviours
The primary outcome was defined if a participant responded ≥6 on a 7-point Likert scale for ≥2/3 lifestyle behaviours. Participants reported their agreement with three stem statements: ‘Attending the clinic today motivated me to improve my physical activity/diet/regularly measure my blood pressure’.
Secondary outcomes
Post-clinic
Clinic satisfaction: defined if participants reported ≥6 on a 7-point Likert scale for ≥2/3 of three statements on satisfaction: ‘I am satisfied with the waiting time/education/overall clinic today’.
Confidence to perform CPR: defined if participants responded ≥4 on a 5-point Likert scale of agreement to ‘I am confident in my ability to perform CPR’.
Willingness to perform CPR: defined if participants responded ‘yes’ to the question ‘Would you perform CPR on someone you know/a stranger’.
CPR knowledge: true/false question: ‘To perform CPR, you MUST do breaths AND compressions’ (correct answer=false).
Thirty-dayday follow-up
Lifestyle (exercise and diet) behaviours: defined if participants reported meeting thresholds for ≥2/3 measures (>30 min a day for most days of exercise, >4 serves of vegetables per day and >1 serve of fruit per day). Recommended thresholds were defined according to the National Vascular Disease Prevention Alliance 2012 clinical guidelines.18
Motivation to improve physical activity and diet: defined if participants reported ≥6 on a 7-point Likert scale for 2 stem statements on physical activity and diet, that is, ‘I am currently motivated to improve my physical activity/diet’.
CPR confidence, willingness and knowledge as previously defined.
Statistical considerations
Study power and sample size
For the main study, a sample size of 330 had 80% power, allowing for 5% attrition, to detect a relative increase of 41% (RR 1.41) in the proportion of intervention participants reporting high motivation to make lifestyle change. A low attrition rate was assumed as outcomes were collected immediately post-clinic, and a control proportion of 40% was selected based on evidence that patients with chest pain report high motivation for lifestyle change (mean 6 on a 7-point Likert scale).11
For the sub-study, a sample size of 220 (1:1 intervention:control ratio), with 5% attrition, had 80% power to detect a relative increase of 37% (RR 1.37). A control rate of 50% was based on data from a survey of CPR confidence administered to 100 visitors entering Westmead Hospital in September 2018.19
Analytical approach
All analyses were pre-specified in a statistical analysis plan and were conducted according to intention to treat principles. Analyses were performed using R statistical software (V.3.6.1). All tests were two tailed, a p value of <0.05 was considered significant and relative risks are reported with 95% CIs. Normally distributed continuous variables were expressed as mean and SD. Non-normally distributed variables were expressed as median and IQR.
The primary analysis for the main and sub-study used a log binomial model adjusted for age, gender, time spent in clinic and educational level. Binary secondary outcomes followed a similar approach. When relevant baseline measures of outcome variables were available (ie, baseline CPR confidence in the CPR substudy), they were also included in statistical models. Primary analysis was a complete-case analysis. Multiple imputation was not pre-specified and hence not used.
Pre-specified analyses of intervention participants who watched ≥2 videos and participants with no previous CPR training were conducted. Exploratory sub-group analyses assessing treatment effect according to age, sex, educational level, body mass index, blood pressure, diabetic status, ethnicity, referral type and waiting time were undertaken.
Results
Between December 2018 and March 2020, 514 patients attending clinics were screened, 330 randomised (figure 1), 97.8% (323/330) assessed post-clinic and 93.0% (307/330) at 30-day follow-up (figure 1). Recruitment closed when the sample size was achieved. Median time in clinic was 115 min (IQR 90–149). Mean participant age was 53.8 (SD 15.2), 55.2% (182/330) were male and 50.9% (168/330) had previously completed formal CPR training. The intervention arm reviewed a median of 2.0 (IQR 1.0-4.0) videos, 92.7% (204/220) watched at least one video and 63.2% (139/220) watched greater than or equal to two videos. Most baseline characteristics were well matched (table 1). Data completeness is included in online supplemental table 1.
Supplemental material
Baseline demographic characteristics
Motivation, satisfaction and lifestyle behaviours
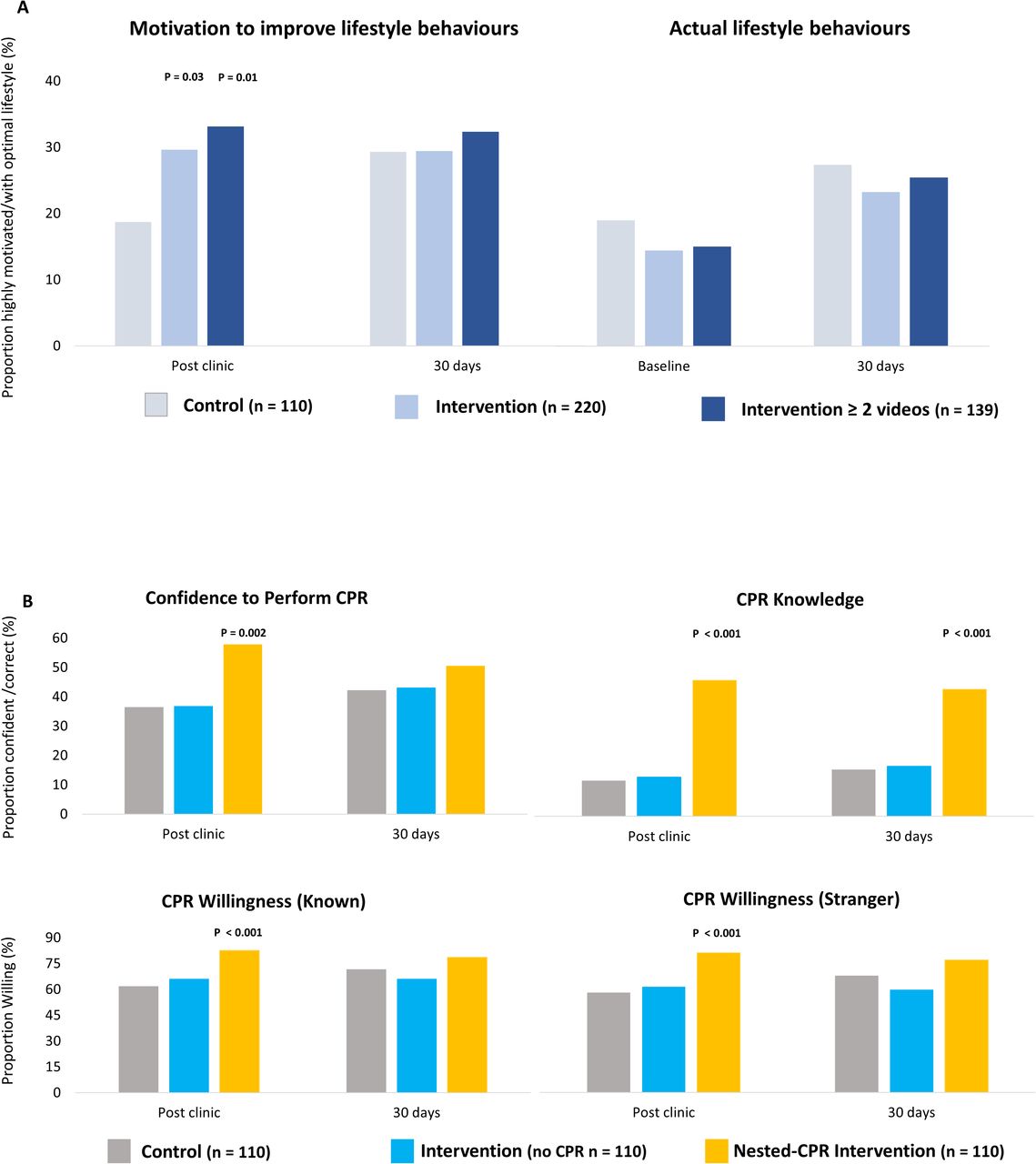
The primary outcome of high motivation to improve CVD risk-modifying behaviours post-clinic occurred in 29.6% (64/216) of intervention participants compared with 18.7% (20/107) of control participants (RR 1.63 (95% CI 1.04 to 2.55), figure 2). This result was robust to a worst-case analysis for missing data. More intervention participants reported high clinic satisfaction than control participants (42.1% (91/216) versus 19.6% (21/107), RR 2.19 (95% CI, 1.45, 3.33)). The 139/220 intervention participants who watched ≥2 videos demonstrated a larger difference (figure 2). Between baseline and 30 days, the proportion of all participants reporting achieving ≥2/3 diet and physical activity thresholds increased (16.1% vs 24.8%, OR=2.44 (95% CI 1.38 to 4.49), see figure 2); however, there was no significant difference between groups at 30 days (figure 2, table 2).
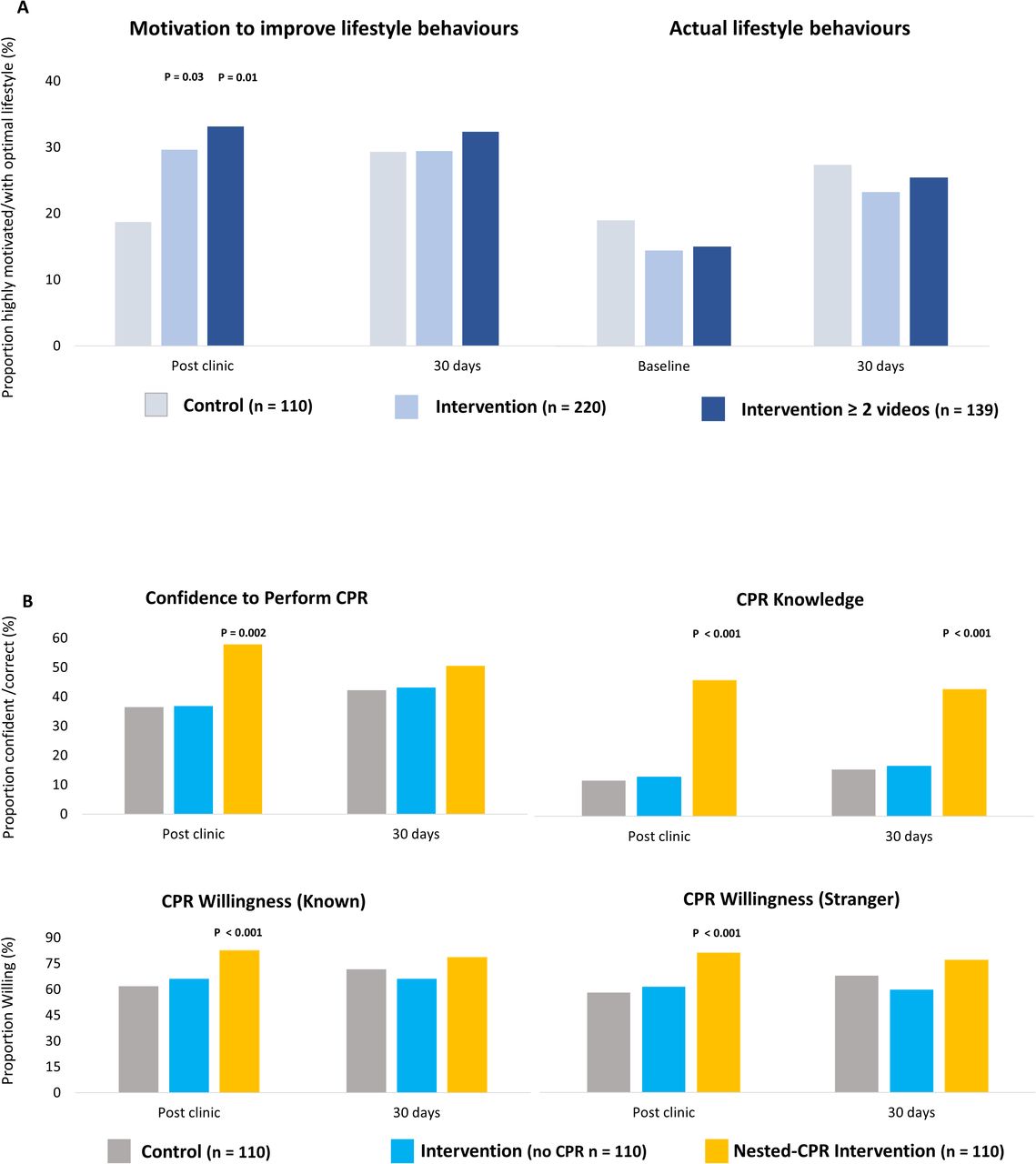
(A) Participant motivation and lifestyle behaviours post-clinic and at 30-day follow-up. (B) CPR confidence, willingness and knowledge post-clinic and 30 days all outcomes adjusted for age, gender, education and total waiting time. *P<0.05, **p<0.01. All p values are relative to control participants unless stated otherwise.
Primary and secondary analyses and sensitivity analysis restricted to participants who watched ≥2 videos
CPR confidence, willingness and knowledge among CPR video recipients
Post-clinic, self-reported confidence to perform CPR was achieved in 57.8% (63/109) of participants that viewed the CPR video compared with 36.4% (39/107) of control participants (RR 1.61 (95% CI 1.20 to 2.16), figure 2). There was a greater difference among the 162/330 participants with no prior CPR training (45.8% (22/49) confident vs control – 16.0% (8/53) confident, RR 2.50 (95% CI 1.24 to 5.04)). Willingness to perform CPR on someone they knew was higher in those that received the CPR video compared with control (RR 1.36 (95% CI 1.15 to 1.62), and willingness to perform CPR on a stranger was also higher (RR 1.43 (95% CI 1.18 to 1.72)). CPR video recipients were more likely to correctly answer the CPR knowledge question (RR 3.80 (95% CI 2.13 to 6.77)).
At 30 days, the difference in CPR knowledge was maintained (39.8% (41/103) vs 14.7% (15/102), RR 2.72 (95% CI 1.60 to 4.64). Differences in confidence and willingness no longer reached significance (RR 1.25 (95% CI 0.97 to 1.60), RR 1.10 (95% CI 0.94 to 1.29) for someone known, RR 1.14 (95% CI 0.95 to 1.35) for a stranger (figure 2)).
Ancillary analyses
Exploratory subgroup analyses are shown in figure 3. Heterogeneity of effect of the study intervention on the primary outcome was suggested according to gender (p=0.012). No other significant subgroup interactions were identified for the primary outcome or the main outcome of the CPR sub-study.

Subgroup analyses of primary outcomes. Based on age, gender, education, ethnicity, referral type, waiting time, blood pressure, body mass index and diabetic status. P value describes whether intervention effect differs between subgroups for the two primary outcomes.
Discussion
It is well-known that positive lifestyle change reduces CVD-related mortality.20 This RCT found a patient-centred, tablet-delivered educational programme on cardiovascular risk significantly increased motivation to improve CVD risk-modifying behaviours and clinic satisfaction (figure 4). Provision of an additional brief CPR video significantly increased confidence, knowledge and willingness to perform CPR post-clinic. Overall, the proportion of participants reporting achieving diet and exercise thresholds was significantly higher at 30-day follow-up than baseline (figure 2), though the difference between groups did not reach statistical significance. Differences in other key outcomes also attenuated and became non-significant at 30-day follow-up. Additional analyses examining intervention participants who watched ≥2 videos suggest the intervention may be more effective in patients who were more engaged with the intervention (figure 2). Ancillary subgroup analysis suggests females were more likely to achieve the primary outcome than males. This may be due to differences in healthcare attitudes, intervention material and delivery, or chance. Further research to explore reasons for intervention effectiveness among different patient populations is needed.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
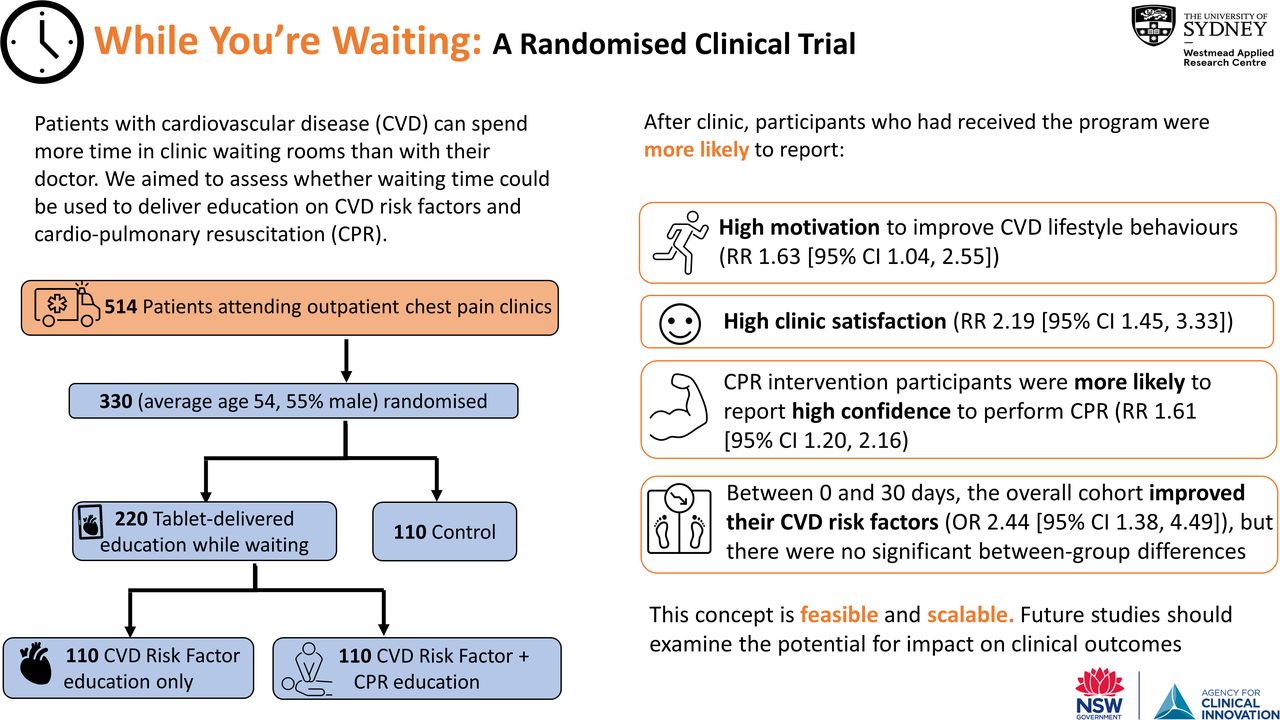
Informational graphic summary of the While You’re Waiting study.
Our literature review identified no similar RCTs of educational interventions in cardiology clinic waiting rooms. However, study results are broadly consistent with non-randomised emergency department-based studies demonstrating waiting room education improved health service satisfaction.21 22
Multiple studies have shown that exposure to CPR videos can improve CPR performance10 23 and confidence to perform CPR.24 A recent systematic review found that community focused CPR interventions improve 30-day survival from OHCA (OR 1.34; 95% CI 1.14 to 1.57).25 Waiting room delivery of CPR education is a novel approach with substantial reach and is likely to be easily scaled. Our study demonstrates delivering CPR education in the clinic waiting room is feasible and effective in improving confidence and willingness to perform CPR. The sub-analysis among participants with no previous CPR training indicated intervention impact may be higher within this group suggesting that this type of intervention may be particularly useful in areas of low health literacy or low knowledge of CPR.
Clinical implications
As pressure on public health systems mounts and patients wait longer,26 interventions of this nature could contribute to patient care in various healthcare settings. Educational interventions such as this are low cost and while their effect sizes on direct health outcomes are likely to be small, they are amenable to provision at scale. As such, the observed effect would need not be large to justify scaled implementation. Using time otherwise not used effectively during patient care makes good clinical sense, and if it empowers patients to understand and self-manage their condition is likely to have additional health and economic benefits.
The large immediate intervention effect on motivation shown in our study could also be harnessed to engage patients in longer term behaviour change interventions. Taking the opportunity of the clinic visit to commence them on this journey is a potentially useful opportunistic intervention. This could be facilitated through extended access to videos and/or the delivery of mobile health strategies that have shown promise in primary and secondary prevention settings.27 28 Delivered at a population level, the intervention may offer a cost-effective approach to provision of CVD and chronic disease preventative programmes.
Limitations
There are several limitations to this study. First, for brevity for participants in a waiting room, we designed a short survey to measure study outcomes we thought relevant from our review of the literature. We piloted this questionnaire among consumers prior to the study but did not carry out formal validity or reliability assessments. The positive wording of some questions may have biased participants to respond positively, though this effect would be experienced equally by intervention and control participants. Second, this is a relatively small, single-centre study and findings may not be generalisable to other patient populations or powered to reach conclusions on small changes to CVD-related lifestyle behaviours. Third, it was not possible to achieve complete blinding in this study. We did take measures to prevent selection biases and blind study staff (eg, by providing tablets initially to both intervention and control participants). However, a Hawthorne effect may have influenced study results post-clinic. Finally, small differences were observed in some baseline characteristics between intervention and control groups. This was likely due to chance in a relatively small sample size study without stratification. Post-hoc analysis of the randomisation algorithm (10 000 iterations with the same sequence of males and females observed in the study) indicated that, without stratification, the likelihood of a ≥12.7% difference in proportion of male participants, as observed, is 4.2%.
Conclusion
Waiting time is increasing, underused and presents an opportunity for the delivery of interventions to improve patient engagement and health outcomes. Our study demonstrated that a simple waiting room-based educational programme had a large immediate impact on motivation to improve CVD risk-modifying behaviours and confidence to perform CPR. The study and concept are scalable and could easily be delivered to larger populations with little risk and the potential for significant population level benefit. Future studies should examine whether sustained intervention deilvery outside the waiting room is feasible. There is also a need for larger, multi-centre waiting room-based studies powered to assess the potential for population level impact on CVD risk and outcomes.
Key messages
What is already known on this subject?
Waiting time is ubiquitous in healthcare but poorly used.
There are no examples of randomised clinical trials assessing the impact of waiting room intervention delivery on cardiology patients.
What might this study add?
In this randomised clinical trial of 330 adults, participants who received waiting room education were 1.6 times more likely to report high motivation to improve cardiovascular lifestyle behaviours than control participants post-clinic.
A sub-set of 110 participants who received education on cardiopulmonary resuscitation (CPR) were 1.6 times more likely to report high confidence to perform CPR than control participants post-clinic.
At 30 days, there was no significant impact on actual lifestyle behaviours, though the study was not powered for this outcome.
How might this impact on clinical practice?
Provision of targeted waiting room education improves patient engagement with cardiovascular disease prevention and could be a feasible and low-cost vehicle for CPR education.
Larger, multi-centre studies are needed to determine the effect on clinical outcomes.
Data availability statement
Data are available on reasonable request. Deidentified study data will be made available to researchers who provide a methodologically sound proposal and after the signing of a non-disclosure agreement. To submit a data use proposal, please email the principal investigator at clara.chow@sydney.edu.au.
Ethics statements
Patient consent for publication
Ethics approval
Ethical approval was obtained from the Western Sydney Local Health District Human Research Ethics Committee (5621) AU RED HREC/18/WMEAD/124.
Acknowledgments
We acknowledge Robert Reid, secretary of the Cardiomyopathy Association of Australia, for his contribution to the development of the intervention. We would also like to thank staff of the Rapid Access Cardiology Clinic, Westmead Hospital and the Westmead Applied Research Centre for their support.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @clara_chow
Contributors Study concept and design: DM, AT and CKC. Acquisition, analysis or interpretation of data: all authors. Drafting of manuscript: DM, AT and CKC. Critical revision of manuscript: all authors. Statistical analysis: DM, AVH, SM and CKC. Obtained funding: DM, AT and CKC. Study supervision: AT and CKC.
Funding This work was supported by the Agency for Clinical Innovation Research Grants Scheme. CKC is supported by a National Health and Medical Research Council of Australia Career Development Fellowship cosponsored by the National Heart Foundation of Australia.
Competing interests None declared.
Provenance and peer review Not commissioned; internally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.