Article Text

Abstract
Background Standard therapy for COVID-19 is continuously evolving. Autopsy studies showed high prevalence of platelet-fibrin-rich microthrombi in several organs. The aim of the study was therefore to evaluate the safety and efficacy of antiplatelet therapy (APT) in hospitalised patients with COVID-19 and its impact on survival.
Methods 7824 consecutive patients with COVID-19 were enrolled in a multicentre international prospective registry (Health Outcome Predictive Evaluation-COVID-19 Registry). Clinical data and in-hospital complications were recorded. Data on APT, including aspirin and other antiplatelet drugs, were obtained for each patient.
Results During hospitalisation, 730 (9%) patients received single APT (93%, n=680) or dual APT (7%, n=50). Patients treated with APT were older (74±12 years vs 63±17 years, p<0.01), more frequently male (68% vs 57%, p<0.01) and had higher prevalence of diabetes (39% vs 16%, p<0.01). Patients treated with APT showed no differences in terms of in-hospital mortality (18% vs 19%, p=0.64), need for invasive ventilation (8.7% vs 8.5%, p=0.88), embolic events (2.9% vs 2.5% p=0.34) and bleeding (2.1% vs 2.4%, p=0.43), but had shorter duration of mechanical ventilation (8±5 days vs 11±7 days, p=0.01); however, when comparing patients with APT versus no APT and no anticoagulation therapy, APT was associated with lower mortality rates (log-rank p<0.01, relative risk 0.79, 95% CI 0.70 to 0.94). On multivariable analysis, in-hospital APT was associated with lower mortality risk (relative risk 0.39, 95% CI 0.32 to 0.48, p<0.01).
Conclusions APT during hospitalisation for COVID-19 could be associated with lower mortality risk and shorter duration of mechanical ventilation, without increased risk of bleeding.
Trial registration number NCT04334291.
- COVID-19
- pharmacology
- clinical
Data availability statement
Data are available upon reasonable request.
This article is made freely available for use in accordance with BMJ’s website terms and conditions for the duration of the covid-19 pandemic or until otherwise determined by BMJ. You may use, download and print the article for any lawful, non-commercial purpose (including text and data mining) provided that all copyright notices and trade marks are retained.
https://bmj.com/coronavirus/usageStatistics from Altmetric.com
Introduction
COVID-19 is an infectious illness, first reported in China in December 2019, presenting mainly with fever and cough, which frequently leads to lower respiratory tract disease.1 It has quickly spread all over the world, becoming a pandemic in a few months. According to current literature, only therapy with dexamethasone and inhibitors of interleukin (IL) 6 (tocilizumab) showed potential benefit in terms of mortality reduction among patients with COVID-19 and severe respiratory failure. Data on antiviral therapy are controversial, with remdesivir having potential benefit in critically ill patients.2 Antibiotic therapy with azithromycin, whether combined or not with hydroxychloroquine, an antimalarial drug, did not show any significant benefit.2
Data from autopsies suggested a potential role of coagulopathy in the outcome of patients with COVID-19,3 which is associated with a higher incidence of both venous and arterial thrombosis and localised pulmonary thrombotic microangiopathy.4
Clinical deterioration in COVID-19 seems mainly due to a combination of hyperinflammation, endotheliitis and coagulopathy. In this context aspirin may have antiviral, anti-inflammatory and pleiotropic effects on the endothelium.5 Moreover, P2Y12 receptor antagonists inhibit platelet activation and neutrophil–platelet aggregates, reducing pulmonary neutrophil recruitment and platelet-derived proinflammatory cytokine release from α-granules.6
Data on anticoagulation therapy are still controversial. Randomised trials showed therapeutic anticoagulation has no benefit in critically ill patients,7 8 while heparin at therapeutic doses, compared with thromboprophylaxis doses, in non-critically ill patients with COVID-19 could be associated with slightly increased survival rates.9
On the other side antiplatelet therapy (APT) in patients with COVID-19 could provide some benefit in terms of mortality reduction; a randomised trial (RECOVERY) showed that aspirin therapy is associated with a 1.2% absolute increase in survival.10
The aim of this study was therefore to evaluate the potential benefit and safety of APT in patients with COVID-19.
Methods
Study design and population
There were 7824 consecutive patients with COVID-19 enrolled and followed up in the multicentre international registry (Health Outcome Predictive Evaluation Registry (HOPE-COVID-19); https://hopeprojectmd.com; NCT04334291). The protocol was established by a scientific board from Italy, Spain, Ecuador and Germany. Patients were enrolled from seven countries (Spain, Italy, Ecuador, Cuba, Germany, China, Canada). Detailed information on the participating countries and hospitals is reported on the website of the registry. All patients were diagnosed with COVID-19 through PCR testing, according to the WHO interim guidance. In this analysis, hospital data and patients were included from 16 January 2020 until 30 May 2020. All patients discharged (deceased or alive) from any hospital centre were included in the registry.
All local principal investigators reviewed the draft and checked for the accuracy and veracity of data. A list of participating hospitals, investigators, collaborators and the protocol is available in the appendix and on the website of the project (https://hopeprojectmd.com).
Data extraction
Epidemiological, clinical and outcome data were manually extracted from electronic medical records and evaluated by medical researchers. Each definition of clinical outcomes was recorded and checked by at least two medical doctors in each hospital. Patients’ data were anonymised, and the electronic data were stored and/or filled in an encrypted, password-protected computer/website.
Throat swab samples were obtained from all patients at admission and tested using real-time reverse transcriptase PCR assays according to the WHO recommendation. Additionally, patients’ clinical and laboratory data and imaging test were extracted. All drugs at admission and previous to hospitalisation were recorded. Additional information on data records has been provided in a previous article from this research group.11
Anticoagulation therapy was recorded if patients were treated during hospitalisation with therapeutic or prophylactic dose, including oral, subcutaneous or intravenous forms. Therapeutic dose included oral anticoagulants and unfractionated or low molecular weight heparin (LMWH) (1 mg/kg daily). Prophylactic dose included patients receiving LMWH 40 mg daily.
Antiplatelet therapy
Patients were included in the antiplatelet group if treated during all hospitalisation days, since admission, with aspirin (either oral or intravenous), clopidogrel, ticlopidine, prasugrel and ticagrelor, either with single or dual APT. Patients who started APT more than 24 hours after admission were excluded from analysis.
Major bleeding was defined as (1) overt bleeding associated with haemoglobin less than 70 g/L or any red blood cell transfusion; or (2) overt bleeding associated with at least 2 units of red blood cell transfusion within 48 hours.
Outcome and endpoint
We considered as primary endpoint all-cause mortality during hospitalisation. Other events were recorded, such as invasive mechanical ventilation, non-invasive mechanical ventilation, respiratory insufficiency, heart failure, renal failure, bleeding, sepsis and embolic events. Events were allocated following the Guidelines on the Management of Critically Ill Adults with Coronavirus Disease 2019 (COVID-19).12
Statistical analysis
Data are presented as mean±SD for continuous variables with a normal distribution and as frequency (%) for categorical variables. The Kolmogorov-Smirnov test was used to assess normal distribution. Student’s t-test and Mann-Whitney U test were used to compare continuous variables with normal and non-normal distributions, respectively. The χ2 test or Fisher’s exact test was used to compare categorical variables. Survival was plotted on Kaplan-Meier curves and assessed with log-rank test. Relative risk with 95% CI was calculated. Factors statistically significant on univariable analysis with p<0.0001 were entered into Cox multivariable regression analysis to define the independent risk factors for the outcome. A model including gender, age, hypertension, diabetes, renal failure, respiratory failure, heart failure, invasive ventilation, prior APT, in-hospital anticoagulation therapy and in-hospital APT was used for multiple Cox regression analysis. Variables statistically significant on univariable analysis but not included in the Cox analysis were initial setting of care (intensive care unit (ICU) vs non-ICU), dyslipidaemia, atrial fibrillation and lung disease.
Given the sample size of patients included in the analysis, the death rates in the control group (patients receiving neither anticoagulation therapy nor APT), a power of 80% and α of 0.05, a relative risk reduction of at least 22.5% could be detected as statistically significant. The proportional hazard assumption was tested using Schoenfeld residual analysis with a threshold of p<0.05 for non-proportionality and confirmed for in-hospital APT variable.
Statistical analysis was performed with SPSS Statistics V.26.0. P<0.05 was considered statistically significant and all tests were two-sided.
Patient and public involvement statement
The public were involved in the study by registering to the HOPE-COVID-19 Registry and publishing on a website.
Results
Baseline features
The mean age of the patients admitted was 64±17 years, and 58% (n=4578) were male. The mean hospital stay was 11±9 days and follow-up duration was 19±17 days. Several comorbidities were prevalent, such as hypertension (48%), diabetes (19%) and obesity with a body mass index >30 (19%). Moreover, about 20% of patients had a history of heart disease (22%) and/or lung disease (18%). History of cancer had a prevalence of 13%.
Of the patients 9% (n=768) were admitted to the ICU. All demographic features are reported in table 1.
Baseline clinical features of the overall COVID-19 population and patients treated with and without antiplatelet therapy
APT during hospitalisation
Of the patients 730 (9%) received APT during hospitalisation; 680 patients (93%) received single APT (645 patients with aspirin, 33 patients with clopidogrel, and 1 with ticlopidine and ticagrelor, respectively) and 50 patients (7%) received dual APT (DAPT) (35 patients with aspirin and clopidogrel, 10 patients with aspirin and ticagrelor, and 5 patients with aspirin and prasugrel) (figure 1).

Study flow chart: patients on APT during COVID-19 hospitalisation. APT, antiplatelet therapy; HOPE, Health Outcome Predictive Evaluation; pts, patients.
DAPT was started during hospitalisation due to acute coronary syndrome associated with COVID-19 in 29 patients, while DAPT was continued in 21 patients due to history of cerebrovascular or cardiovascular events.
Patients who received APT were older (74±12 years vs 63±17 years, p<0.01), more frequently male (68% vs 57%, p<0.01), had higher prevalence of diabetes (39% vs 16%, p<0.01) and had higher prevalence of concomitant anticoagulation therapy (66% vs 56%, p<0.01) (table 1). In both groups, APT versus no APT, anticoagulation therapy was mainly administrated subcutaneously at a prophylactic dose (77% vs 73%).
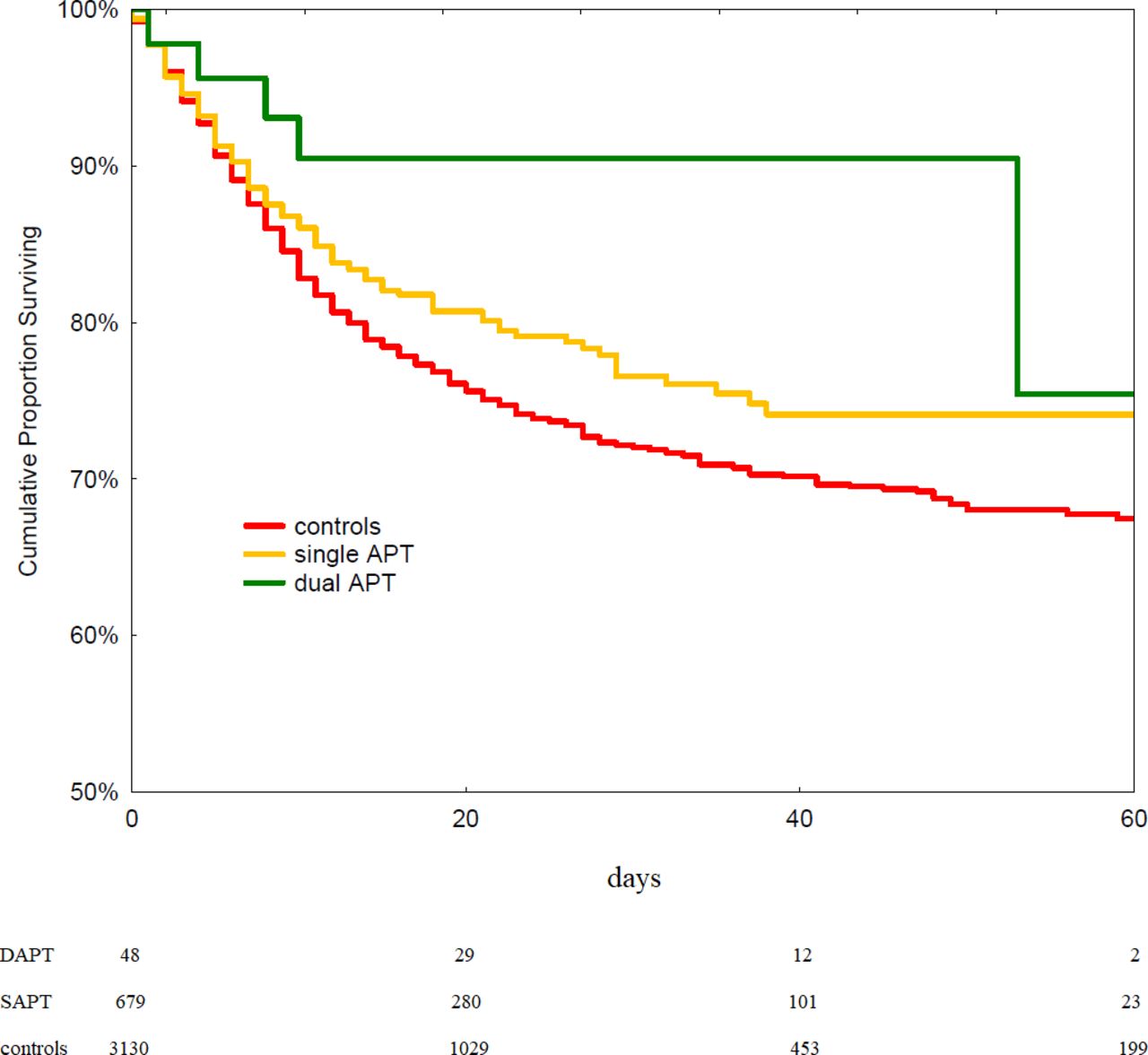
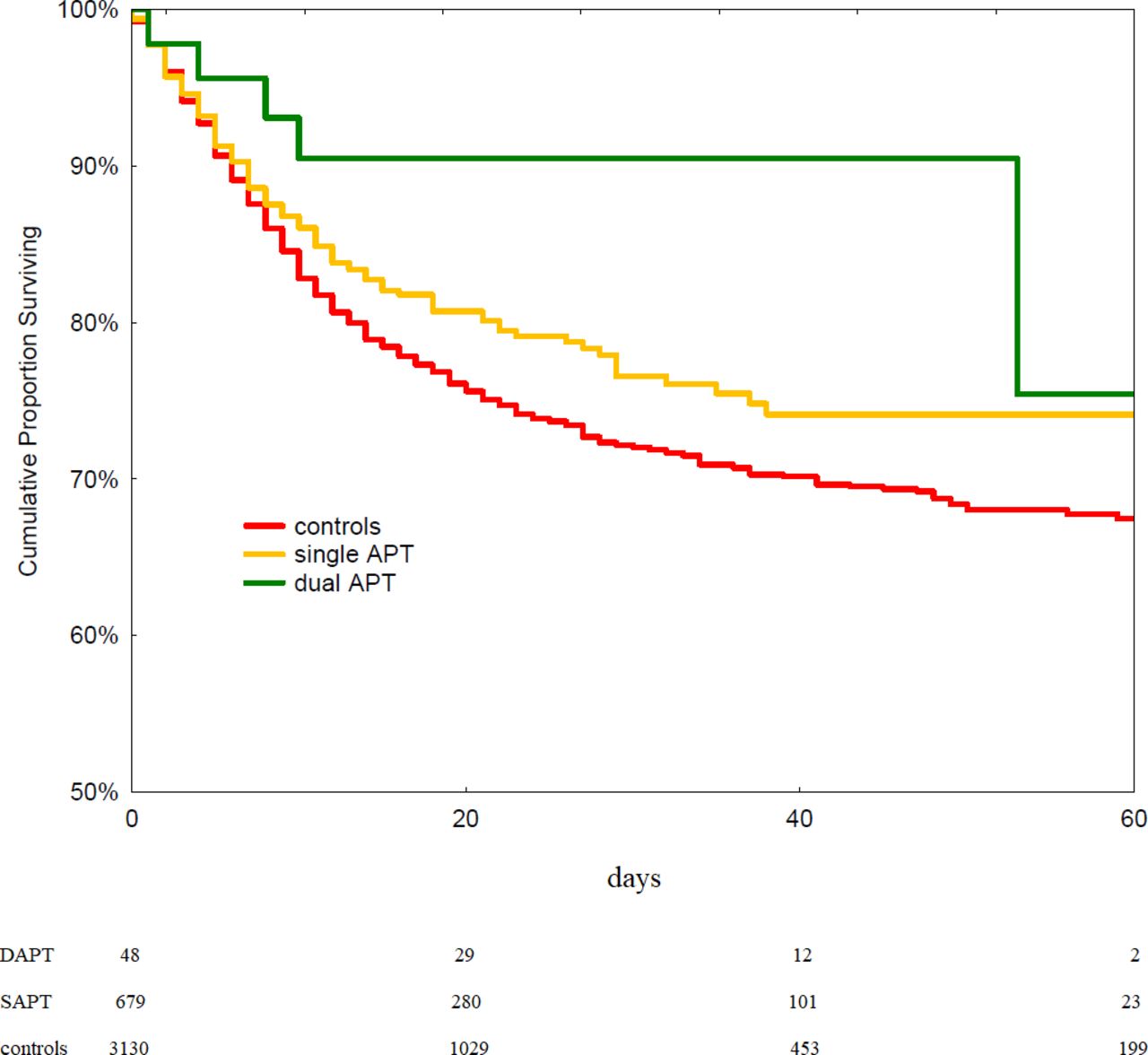
On univariable analysis, patients treated with APT during hospitalisation (including those also receiving anticoagulation) showed no differences in terms of in-hospital mortality (18% vs 19% p=0.64, log-rank p=0.23), need for invasive ventilation (8.7% vs 8.5% p=0.88), bleeding (2.1% vs 2.4%, p=0.43) and embolic events (2.9% vs 2.5% p=0.34), but had shorter duration of mechanical ventilation (8±5 days vs 11±7 days, p=0.01), compared with those not treated. Among patients requiring invasive ventilation, there were no differences in terms of risk of bleeding between patients on APT and those who were not (8.7% vs 8.9%, p=0.83). However, when comparing patients with APT versus no APT and no anticoagulation therapy, APT was associated with lower mortality rates (log-rank p<0.01, relative risk 0.79, 95% CI 0.70 to 0.94; figure 2). In this subset of patients, when comparing patients with single APT, double APT and controls during hospitalisation, mortality rates were not statistically significant (20% in controls, 18.5% in single APT group, 10% in DAPT group, log-rank p=0.11; figure 3).

Survival curves according to in-hospital antiplatelet therapy (log-rank p<0.01, relative risk 0.79, 95% CI 0.70 to 0.94).
{kind=link}
{kind=link}
{kind=link}
Kaplan-Meier survival curves: patients treated with and without dual and single antiplatelet therapy (log-rank p=n.s.). APT, antiplatelet therapy; DAPT, dual APT; SAPT, single APT.
In the multivariable Cox regression analysis model including age, gender, diabetes, hypertension, renal failure, respiratory failure, heart failure, history of cancer, need for invasive ventilation, prehospital use of antiplatelet drugs and in-hospital anticoagulation therapy, in-hospital APT was associated with a lower mortality risk (risk ratio (RR) 0.39, 95% CI 0.32 to 0.48, p<0.01) (table 2). APT was associated with a lower risk of mortality even in the subgroups of patients in the ICU (RR 0.42, 95% CI 0.26 to 0.67, p<0.001) and with history of cancer (RR 0.66, 95% CI 0.44 to 1.01, p=0.0565).
Predictors of all-cause death on multivariable Cox regression analysis in the general population of patients with COVID-19
In 556 (45%) out of 1256 patients receiving APT before hospital admission, APT was withdrawn after hospital admission. Death rate was 18% in those with APT before and after and 57% in those where APT was withdrawn after hospital admission.
Discussion
We report the safety and efficacy of APT from a large multicentre international registry on COVID-19. We found that about 9.3% of patients received APT during hospitalisation; APT was not associated with higher risk of in-hospital bleeding; and APT was associated with lower in-hospital mortality risk in a multivariable analysis including cardiovascular risk factors, anticoagulation therapy and severe clinical presentation.
COVID-19 is a multisystem disorder characterised by respiratory insufficiency, endothelial cell dysfunction and hypercoagulability.13 Indeed, coronavirus enters the human cells mainly by binding to ACE2, which is expressed in lung alveolar cells, vascular endothelial cells, cardiac myocytes and other cells.14
COVID-19 is associated with several haemostatic abnormalities as increased D-dimer levels and mild thrombocytopaenia.15 In a meta-analysis study, Malas et al 16 found in patients with COVID-19 an overall rate of venous thromboembolism of 21% (31% and 5% among ICU and non-ICU patients, respectively) and arterial thromboembolism of 2% (5% and 1% among ICU and non-ICU patients, respectively). The rates of arterial thromboembolic events were as follows: myocardial infarction 0.5%, cerebrovascular accident 1% and acute limb ischaemia 0.5%.
The higher rate of thromboembolic events among patients with COVID-19 admitted to the ICU can be explained by increased concentrations of proinflammatory cytokines, such as tumour necrosis factor-α and IL, including IL-1 and IL-6.17 IL-6 can induce tissue factor expression on mononuclear cells, which subsequently initiates coagulation activation and thrombin generation. Although tissue-type plasminogen activator is upregulated by the kinin-bradykinin pathway in coronavirus infections (SARS-CoV-1),18 severe COVID-19 is associated with suppressed fibrinolytic system due to the counterbalancing effect of increased plasminogen activator inhibitor-1 induced by an excess of uncleaved angiotensin-II.19
Autopsy studies showed that thromboembolic lesions can be found in several organs with platelet-fibrin-rich thrombi in the pulmonary, hepatic, renal and cardiac microvasculature.20 Thrombi were located in veins, pulmonary arteries and arterioles, and microvessels, but not in systemic arteries. Pellegrini et al 21 found on a heart autopsy examination that myocyte necrosis was mainly due to microthrombi with higher prevalence of fibrin and c5b-9 complement. Moreover, circulating megakaryocytes were seen in all cases in the microvasculature of the heart, renal glomeruli and lungs.22
Platelet activation, including aggregation, α-granule secretion and dense granule release, was found to be a major driver of thrombosis in COVID-19.22 Zhang et al 22 found that SARS-CoV-2 and its spike protein directly stimulated platelets, resulting in the release of coagulation factors and inflammatory cytokines and enhancing leucocyte–platelet aggregates, which can promote thrombosis and thrombus stability.
Extensive platelet-fibrin microthrombi combined with megakaryocytes within the heart microvasculature suggests a deep platelet response in COVID-19, which may be one of the mechanisms involved in multiorgan failure. Therefore, drugs able to reduce platelet aggregation may also be helpful in the treatment of microthrombi in patients with COVID-19. In this context, aspirin may have several potential actions; it irreversibly inhibits cyclo-oxygenase, has antiviral properties and attenuates the proinflammatory effects of nuclear transcription kappa B, which has been implicated as having a critical role in the cytokine storm that occurs with COVID-19.23 It may also have pleiotropic effects on the endothelium which could target potential development of endotheliitis, a potential complication of severe COVID-19.24
The antiviral properties of APT are mainly related to their potential activity of suppressing platelet activation. Indeed, in several models of tissue injury during virus infection (influenza A virus, dengue, HIV-1, severe acute respiratory syndrome), severe inflammation is driven by unsuppressed platelet activation.25
In animal models, treatment with glycoprotein IIb/IIIa antagonists, protease-activated receptor 4 antagonists and clopidogrel showed protective effects against severe lung injury (inhibition of neutrophil recruitment into inflamed lungs) and lethal infections induced by several influenza strains.26 Similar data on reduction of platelet and immune activation have been shown in clinical studies on patients with HIV-1.27
In a multicentre observational cohort study of 412 patients with COVID-19, Chow et al 28 found that in-hospital aspirin use was associated with a significant reduction in risk of ICU admission, mechanical ventilation and in-hospital death, and there were no differences in terms of major bleeding or thrombosis between aspirin users and non-users.
Meizlish et al 29 have shown similar data in a retrospective study of 2785 hospitalised patients with COVID-19 that aspirin therapy (n=638) was associated with lower incidence of in-hospital death. Moreover, a randomised trial (RECOVERY) evaluated the efficacy of aspirin in COVID-19, enrolling 7351 patients, and the authors found that aspirin therapy was associated with a 1.2% increase in survival, a 0.6% reduction in thrombotic events, and an increase in major bleeding events of 0.6%.10
These data are in line with the present study, where APT was associated with lower in-hospital mortality. In this study patients receiving APT other than aspirin, such as as clopidogrel, ticlopidine, ticagrelor and prasugrel, were also included. Fifty patients received DAPT and of these 29 were due to acute coronary syndrome and as previous treatment for the remaining patients.
Patients receiving APT in the present study were a subset of more critical patients, with higher prevalence of male sex and diabetes. Interestingly APT therapy was associated with a shorter duration of mechanical ventilation. These data suggest that APT may have a role in modulating the cytokine storm. APT also showed benefits in a subset of frail patients, such as those in the ICU and with history of cancer.
Noteworthy, the role of APT could be independent from anticoagulation therapy, which was included in the multivariable analysis model for mortality prediction. In the present study, 66% of patients treated with APT also received anticoagulation therapy (77% and 23% at a prophylactic or therapeutic dose, respectively). A low dose of antiplatelet drugs and a prophylactic dose of anticoagulants could therefore represent another potential therapeutic approach to be investigated in patients with COVID-19.
Apparent discrepancy between worse outcome with APT prior to hospital admission and better outcome with APT after admission could presumably be explained by higher rates of APT withdrawal in subjects with presumably worse clinical conditions.
Anticoagulants may have several potential benefits in patients with COVID-19, reducing the risk of thrombotic disease, and could also have some anti-inflammatory effects against sepsis and the development of acute respiratory distress syndrome. Heparins block P-selectin, the cross-talk of platelets and neutrophils, inhibit neutrophil response, and reduce the release of IL-1β, IL-6, E-selectin and intercellular adhesion molecule 1.30 However, the role of anticoagulants in COVID-19 is still debatable. Among critically ill patients, no differences in terms of survival between therapeutic and prophylactic anticoagulation have been found in randomised trials.7 8 In non-critically ill patients, heparin at therapeutic doses compared with thromboprophylaxis doses could be associated with slightly increased survival rates.9
The present study showed that APT could be a potential additional tool for COVID-19 treatment; randomised, double-blinded, adequately powered trials evaluating a combination of antiplatelet and anticoagulation therapy are definitely warranted.
Limitations
Some limitations to the present investigation have to be considered. The study is a large multicentre international prospective registry; however, this is not a randomised trial and no patient was randomised to different alternative therapies. APT was left to the operator’s choice and therefore evaluation of potential benefit was performed with a retrospective analysis. Data on the median dose of APT provided during hospitalisation were not available for all patients. Most of the patients have 28 days of follow-up and no conclusion can be done on long-term benefit. The study relies on patient data entered by individual principal investigators at each participating institution and the accuracy of data relies on this factor.
Conclusions
APT during hospitalisation for COVID-19 could be associated with lower mortality risk and shorter duration of mechanical ventilation, without increased risk of bleeding.
Key messages
What is already known on this subject?
Thrombosis may complicate COVID-19.
What might this study add?
Antiplatelet therapy is associated with lower mortality in hospitalised patients with COVID-19.
How might this impact on clinical practice?
This observational study could represent a proof of concept for future randomised trials.
Data availability statement
Data are available upon reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
The local ethics committee approved this study and was consistent with the guidelines of Helsinki.
References
Footnotes
FS and IJN-G are joint first authors.
Twitter @FraSantoroMD, @ibnsky, @Auribarri, @S_Raposeiras, @GuerraCardio, @natalebrunetti
FS and IJN-G contributed equally.
Contributors FS and IJN-G designed the study. EV, MV, BR-M, RR-P, GFG, IFR, AU, VMB-M, EA-R, MG-A, JH, MEO-A, JFG-P, ECR, FU, MB, AM, SR-R, JJ, CE, ARA, FM, FG, IA, BC, HR, CM and AF-O collected data. FS wrote the paper. NDB performed the statistical analysis. NDB and IJN-G supervised the study. FS, IJN-G and NDB were responsible for the data.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were involved in the design, or conduct, or reporting, or dissemination plans of this research. Refer to the Methods section for further details.
Provenance and peer review Not commissioned; externally peer reviewed.