Article Text

Abstract
The purpose of this document is to update the existing joint British Societies recommendations on multidisciplinary meetings (MDMs) published in 2015 to reflect changes in practice. We aim to provide guidance on the structure and function of MDMs which should be taking place in every cardiac surgical centre. Out of scope are MDMs that do not require the routine presence of a cardiac surgeon such as electrophysiology MDMs and those which are not provided in every centre, such as complex aortic surgery.
Statistics from Altmetric.com
Introduction
The way in which care for cardiac patients is provided has changed considerably in the last 20 years. At the turn of the century, patients were mostly under the care of a single cardiologist, who assessed the patient, made the diagnosis and initiated treatment. In addition, the cardiologist decided if surgery was indicated. At this point, the patient was referred to a cardiac surgeon who was responsible for counselling the patient about the risks of surgery and for the surgery itself. The anaesthetist would administer the anaesthetic and provide additional input if there were issues with ventilation or if the patient was returned to theatre.
Step forward to today and the patient pathway has evolved due to increased subspecialisation in both cardiology and in cardiac surgery, advances in cardiac imaging and the use of new technologies. Patients are looked after by multiple specialists, including nurse practitioners and cardiac scientists, through their journey which may involve cardiac assessment, anaesthesia, surgery and intensive care. There are more diagnostic tools with greater expertise required to interpret the results. Furthermore, there are more therapeutic options available including percutaneous coronary intervention (PCI) using calcium modification technologies, arrhythmia ablation, transcatheter aortic valve implantation (TAVI), percutaneous closure of paraprosthetic leaks and emerging mitral and tricuspid valve interventions. The majority of myocardial revascularisation procedures are now performed on an urgent basis for acute coronary syndromes (ACS). There is a ‘mitral surgeon’ and a surgeon for the aorta. Intensivists play a key role in supporting critically unwell patients and guide more comorbid patients through the pre-assessment, intra-operative and postoperative period, often using advanced tools for haemodynamic assessment such as transoesophageal echocardiography (TOE) in surgery and on the intensive therapy unit.
These changes have made multidisciplinary team (MDT) working a key component of contemporary patient care. MDT working, however, has been adopted at different rates by different individuals and units. The Getting It Right First Time (GIRFT) reports in cardiology and cardiothoracic surgery demonstrated unwarranted variation in these aspects of practice.1 2 The units which have been able to implement change achieved these improvements in the delivery of care for their patients by functioning as a team across disciplines. An independent review into mortality rates at a UK cardiac surgical centre made 12 recommendations which are applicable to most units.3 In broad terms, the report recommended protocols for patient pathways with functioning multidisciplinary meetings (MDMs), effective clinical governance and, critically, professionalism in all interactions with colleagues.
MDMs have become the common ground of our practice. They bring specialists together who have the knowledge, skills and experience to interpret investigation results, discuss therapeutic options and make recommendations aimed at helping the patient decide on their preferred management strategy. The MDM requires high professional standards, administrative support in order to coordinate cases and execute the decisions in a timely way and processes which facilitate audit and quality assurance. Subspecialisation and increasing complexity of cases have expanded the range of MDMs in cardiac surgical centres which should now include the following:
Myocardial revascularisation.
Aortic valve disease.
Mitral and tricuspid valve disease.
Endocarditis.
These MDMs need to encompass the full breadth of patients from those who are stable in the outpatient setting to patients who present acutely with haemodynamic instability.
The purpose of this document is to update the existing joint British Societies recommendations published in 20154 to reflect these changes in practice. We aim to provide guidance on the structure and function of MDMs which should be taking place in every cardiac surgical centre (box 1 and figure 1). Out of scope are MDMs that do not require the routine presence of a cardiac surgeon such as electrophysiology MDMs and those which are not provided in every centre, such as complex aortic surgery. Members of the Cardiovascular Care Partnership UK reviewed drafts of this document to provide a patient perspective.
Key messages
MDMs are a key part of the patient pathway for myocardial revascularisation, aortic valve disease, mitral and tricuspid valve disease and endocarditis.
MDMs should function as a single, disease-specific, point of access to interventional pathways.
Many patients can be rapidly triaged by the relevant MDM but those where the optimal management is unclear require detailed review.
MDMs should incorporate the principles of patient-centred care and shared decision making.
MDMs should be virtual (or hybrid) by default and accessible to all referring clinicians within a network.
Each surgical centre should convene a daily MDM for consideration and prioritisation of urgent inpatient referrals involving, as a minimum, the on call cardiologist and cardiac surgeon.
MDMs must have a coordinator and a chair and should be job planned for all core attendees.
All MDM discussions must be documented and the decisions made subject to regular audit.

The evolution of the Heart Team.
The multidisciplinary team and the multidisciplinary meeting
This document draws a distinction between the MDT and the MDM. The MDT (or ‘Heart Team’) is the group of healthcare professionals responsible for the management of a patient on a disease-specific pathway, which may extend from primary to tertiary care. The MDM is a meeting of members of the MDT convened for the purpose of reaching a consensus on the optimal management of a particular patient. The traditional model of care, in which the cardiologist’s responsibility for a patient effectively ended following acceptance for surgery, or in which the surgeon’s responsibility ended with acceptance for TAVI does not reflect the reality of modern practice. We propose a re-focusing of the MDM as part of an approach which promotes collective decision-making and fosters collective ownership of the decision and of the outcomes associated with it.5 A poor outcome from TAVI should cause as much concern for the surgical and intensivist members of the team as for the cardiologist(s), while a poor surgical outcome should be of equal concern to the cardiology specialists as to the surgeon(s).
The MDM requires patients referred for possible intervention to be routed through a single, disease-specific, point of entry rather than to an individual surgeon or cardiologist. Proposals for how this could work in practice are outlined in the disease-specific sections of this document. There are obvious challenges to the process, particularly for patients on an ACS pathway where the default procedural listing is for coronary angiography±PCI if indicated. MDM review of all such patients is unrealistic and unnecessary. There should, however, be clear protocols for which patients should be reviewed in an MDM. Failure to follow these protocols risks disenfranchising patients from the shared decision-making process, a key concept which must be maintained throughout the patient pathway. Nor should assumptions be made about which management strategy the patient will favour when more than one treatment option is available. Collective ownership of decisions means that the Heart Team needs to know the consequences of its recommendations for all patients and this requires regular audit of outcomes.
Cardiac MDMs have often been seen as the remit of tertiary centres, with variable access for referring cardiologists from other institutions. If the MDM is to function effectively as the disease-specific point of entry to the cardiac centre, participation must be open to all referring cardiologists and the MDM owned by the cardiac network rather than by the tertiary centre. All MDMs require a minimum dataset which must be completed for patients who are referred for discussion. This has been a problem in the past, either because of incomplete investigations or due to delays arising from serial appointments. Referrals should be made by a standardised electronic form which facilitates real-time tracking of the patient’s clinical journey and audit of timelines and outcomes.
The rapid evolution of virtual technology has facilitated network involvement in the MDM and potentially also allows the involvement of patients and relatives in the discussion, either ‘live’ or in the form of a recording of a video consultation.6 In many instances, clinical decision-making is relatively straightforward without the need for detailed discussion, particularly when patients have been assessed in the relevant specialist clinic and the characteristics of the case can be recognised in the major practice guidelines. In other cases, in which specific patient factors add complexity or when there is equipoise between treatment options, detailed discussion is essential and must be prioritised.
The role of the multidisciplinary meeting chair
The MDM chair is critically important to the effective functioning of the meeting and for the MDT pathway as a whole. As such, the role must be recognised by hospital management teams in job plans and included in formal appraisal. The chair is responsible for determining if the MDM is quorate. He/She should be a senior clinician who is responsible for ensuring that all views are heard in a constructive dialogue which facilitates decision-making by consensus. The chair is responsible for ensuring that decisions are recorded accurately and impartially. The MDM summary should include sufficient detail of the discussion to allow the decision-making process to be reconstructed; unresolved differences of opinion should be recorded. If no consensus was reached, this should be stated. This is particularly important for complex cases and when differences of opinion were expressed. The chair should review the MDM outcome records during or after the meeting.
The chair, in conjunction with the MDM coordinator, is responsible for ensuring that the decisions made in the MDM and the resulting MDM records are formally communicated back to referring teams in a timely fashion. Communications should be electronic and should be entered into the medical records. In cases in which there is a transfer of care between centres, for example, for patients accepted for transfer to a surgical centre, or between clinicians when a patient is accepted for surgery within a centre, the chair should ensure that a named consultant is responsible for the ongoing management of each patient.
The role of the multidisciplinary meeting coordinator
No MDM can function effectively without a dedicated coordinator. Roles should be constructed so that there is always cover for planned or unplanned leave. The responsibilities of the coordinator include the following:
To ensure that completed referral forms and all investigation results are available prior to the MDM.
To agree with referring teams when specific patients will be discussed.
To agree, in conjunction with the chair, a record of the MDM discussions and ensure that decisions are conveyed to referring teams in a timely fashion.
To ensure that MDM outcomes are enacted, for example, by making referrals to surgeons or liaising with the interhospital transfer coordinator.
To liaise with the on-call cardiologist and cardiac surgeon to ensure that the results of ad hoc urgent MDMs are recorded.
Participation in multidisciplinary meetings
All cardiologists in the network should attend the MDM relevant to their field. Advanced nurse practitioners and other members of heart teams should also attend. Larger networks may need more than one MDM arranged on a subnetwork basis, especially for myocardial revascularisation, but the same principles of participation apply.1 2 Participation in MDMs should be agreed during job planning, and recorded and audited for all ‘core’ participants. While clinical and other commitments will dictate that attendance of an individual consultant is not always possible, it is not acceptable for core members to attend only when they have a patient to discuss. Participation in daily urgent MDMs will be more restricted but should be job planned for the on-call cardiologist and cardiac surgeon at the surgical centre. MDM attendance is an important part of specialty and undergraduate training. Training rotas should be organised to enable attendance at MDMs by trainees, who should be encouraged to participate actively in the discussions.
The patient in the multidisciplinary process
Patients, and their partners and carers, play little or no part in most MDMs. Important decisions are being made by clinicians, most of whom have no direct knowledge of the patient. This risks detracting from patient-centred care and shared decision-making. It is therefore vital that the consultant who is responsible for the patient, or a nominated deputy who knows the details of the case, is in attendance to present. Notwithstanding these issues, it is important to view MDMs for elective patients as an integral part of their clinical pathway rather than as stand-alone events. Outpatients who are discussed at an MDM should have a clear understanding of the nature, purpose and possible outcomes of the MDM, and be asked in advance for their views on potential treatment options so that these may form part of the discussion. A simple additional step which might help the MDT to familiarise itself with the patient in order to individualise its recommendation is the inclusion of a photograph of the patient in the MDM case presentation, while the move towards virtual MDMs means that it is now possible to review videos of consultations or of a patient mobilising. The more widespread use of virtual technologies also means that patients and their carers could be directly involved in the MDM. The outcome of the MDM must be conveyed to the patient by a member of the MDT responsible for their care in terms that they can understand.
Multidisciplinary meetings for elective and non-elective patients
The arrangements for MDMs need to reflect the pattern and volume of patient referrals such that discussions and recommendations can be made in response to the urgency of clinical presentations. There are three broad categories of patients: outpatients, urgent inpatient referrals and emergency cases.
Outpatients
Specialty MDMs should be convened on a regular basis to discuss outpatient cases. The frequency for most MDMs should be at least weekly.
Urgent inpatient referrals
While urgent cases can be discussed in the elective patient MDM, a weekly meeting is not sufficiently frequent to ensure discussion of all urgent referrals without some patients incurring a significant delay in their care pathway. Surgical centres should convene daily virtual MDMs at a fixed time for the consideration of urgent in-house and network referrals. This requires the availability of the MDM coordinator and, as a minimum, the on-call cardiac surgeon and cardiologist. This will only be possible if they are free of other timetabled commitments and is greatly facilitated by a cardiologist and surgeon of the week system as this allows for continuity of decision-making. There should also be an identified cardiac anaesthetist/intensivist available to join discussions as required. The on-call cardiologist and cardiac surgeon should be readily available to discuss potential referrals with colleagues from around the network. The on-call consultants, assisted by the MDM coordinator, are responsible for engaging with other colleagues as required for discussion of an individual case and should ensure that decisions taken are acted on and that there is clear ownership of the ongoing management of the patient by a named consultant at the surgical centre. This model will require reorganisation in the way that cardiology, surgical and anaesthetic teams operate in some centres, but is essential for optimal decision-making.
Ad hoc or ‘mini-MDMs’ for emergency cases
This applies predominantly to patients with ACS in high-risk or very high-risk categories, where there is a need for urgent revascularisation and the optimal strategy is uncertain. In these instances, an ad hoc or ‘mini-MDM’ can be held with the patient still in the catheter laboratory. This allows PCI to be undertaken as a follow-on procedure if it is concluded by the MDM that this is the preferred treatment. If the patient is in a non-surgical centre there should be arrangements for access to the on-call cardiology and surgical teams at the surgical centre and the capability for image sharing. Anaesthetic input may also be required. Discussions in a mini-MDM must be recorded in the patient’s record and forwarded to the MDM coordinator. These principles also apply to endocarditis and other situations where rapid decisions about timing of surgery need to be made in unstable patients.
The role of cardiac anaesthesia/intensive care in the multidisciplinary pathway
The majority of patients discussed at MDMs will not require specific anaesthetic/intensive care input at this point in their management. Access to anaesthetic advice is essential, however, for some complex and high-risk patients, for example, those who are being considered for cardiac surgery who have comorbidities and patients who have severely impaired systolic left ventricular function. Anaesthetic assessment clinics should be available as part of the MDT pathway for elective outpatients, the outcome of which can be fed into the MDM if the assessment was undertaken a priori, or the patient can be referred for formal anaesthetic assessment from the MDM, depending on the prior pathway. Critical care support will also be required for (non-elective) patients who are haemodynamically unstable. Arrangements should include the ability to involve the on-call cardiac anaesthetist/intensivist for these patients. Anaesthetist/Intensivist input into these discussions must form part of the MDM record. There should also be cardiac anaesthetist/intensivist involvement in feedback and audit (see Feedback and Audit below).
The role of joint clinics
Joint cardiology/cardiac surgery clinics may be required after the MDM if there is clinical equipoise or when there are outstanding issues to resolve.
Output of the multidisciplinary meeting
The output of the MDM must include a record of the key decisions made and the reasons behind these decisions. The output should be incorporated into the patient’s electronic hospital records (for in-house cases), and conveyed electronically to the referring consultant, to the general practitioner and to the patient. The nature of the information included in the output form will vary according to the type of MDM, but essential information includes the following:
The named consultant responsible for ongoing care.
Treatment recommendations.
Key reasons for treatment recommendations.
Timing of treatment—elective outpatient treatment, discharge for outpatient treatment, urgent inpatient treatment.
Arrangements for interhospital transfer, if required.
Nature of any additional investigations required.
Process for review of any additional investigations.
Recommendations for specific aspects of care such as antiplatelet therapy, antibiotic therapy for endocarditis and assessment for implantable cardioverter defibrillator/cardiac synchronisation therapy.
MDM outcome forms are naturally suited to standardised electronic design.
Feedback and audit
Collective ownership of the outcomes of the MDM requires that MDM processes and their outcomes are subject to regular audit. In addition, each specialist MDT should schedule review of serious adverse outcomes as part of regular morbidity and mortality reviews. Considerable time is required to collect and analyse the relevant data. Named individuals should be appointed to lead this process for each MDM. These contributions to clinical governance should be recognised in job planning. Review meetings require their own dedicated sessions, which could be aligned with audit and education days or morbidity and mortality sessions. Areas for regular audit and review should include the following:
Number and breakdown of cases discussed at MDM in relation to unit procedural volumes.
Review of cases discussed at ad hoc/mini-MDMs.
Breakdown of MDM treatment recommendations (eg, medical treatment, PCI, coronary artery bypass graft (CABG) or no consensus, for coronary artery disease).
Number (proportion) of MDM treatment recommendations which were/were not followed through.
Reasons why MDM treatment recommendations were not followed through (eg, patient choice, operator choice, acute admission, administration failure, death on waiting list).
Timeframes to interventions.
Feedback regarding specific cases for shared learning.
Conclusions
It is recognised that the recommendations made in this document will require changes in the way that many cardiac units operate. Some of the recommendations are aspirational and many of them are included in the recently published GIRFT reports relevant to cardiac patients.1 2 They are all aimed at improving the quality of service that we provide to the patients under our care.
Myocardial revascularisation multidisciplinary meetings
Introduction
The cardiology GIRFT report recommends that there should be a default strategy of listing patients for coronary angiography with follow-on PCI, if indicated, for both stable and unstable chest pain pathways.2 Adoption of this strategy places a renewed emphasis on the importance of consent and a careful explanation of the potential outcomes of the diagnostic procedure. Some stable patients may choose to undergo a diagnostic procedure only irrespective of the results of the angiogram, with a plan for further discussion prior to any intervention. Whichever pathway is followed, it is essential that cases are referred appropriately to the revascularisation MDM in order to ensure that treatment decisions are consistent with guidelines.7 Referral to the MDM should be based on agreed network protocols which align with the recommendations of the cardiology and cardiac surgery GIRFT reports1 2 and apply equally to surgical and non-surgical centres.
Coronary angiography should be performed in a catheter laboratory which is equipped for invasive coronary artery physiology assessment and intracoronary imaging by an operator who is experienced in the use of these technologies. This strategy encourages the use of coronary physiology and anatomical assessments which are of crucial importance in guiding MDM discussions.
In patients on the stable chest pain pathway and in those with stabilised ACS, PCI should be performed immediately following diagnostic angiography±invasive physiology/anatomical assessment when the coronary anatomy, Syntax score and clinical considerations including comorbidities and patient preference, all support follow-on PCI as the optimal treatment strategy.7 All other patients who may require revascularisation should be discussed at an MDM. The consent discussion should be informed by the patient’s presentation and the results of any prior non-invasive investigations. All patients should be made aware of the possible need for MDM discussion after the completion of the coronary angiogram.
In the smaller group of patients who present with ongoing myocardial ischaemia or haemodynamic instability where there is a clinical indication for urgent revascularisation but the optimal strategy is uncertain, an ad hoc MDM discussion can take place within the catheter laboratory. The outcome must be recorded within the patient’s record and should be notified to the MDM coordinator. Ideally, non-surgical centres should have immediate access to the on-call surgeon at the surgical centre and the ability to transfer images for urgent review as part of the ad hoc MDM. When a surgeon is not immediately available, the case management should be discussed among at least two interventional cardiologists.
Proposed process
Regular MDMs, at least once per week, for discussion of elective and urgent coronary artery disease cases.
Daily MDMs for urgent cases which can be accessed virtually as required by all cardiologists within the network. Surgical centres must ensure that a consultant surgeon and a consultant interventional cardiologist are available to attend these meetings.
Ad hoc MDMs within the catheter laboratory for urgent decision-making. These should be documented to the same standard as formal MDMs.
All interventional cardiologists who perform PCI within the network and all cardiac surgeons who perform CABG surgery should attend at least one MDM per week.
Patients for discussion*
Patients in whom the optimal management strategy (medical vs PCI vs CABG) is not clear.
Patients in whom the optimal revascularisation strategy (PCI vs CABG) is not clear.
Patients who have left main stem disease irrespective of Syntax score.
Patients who have two-vessel or three-vessel coronary artery disease, which involves the proximal segment of the left anterior descending artery.
Patients who have ostial disease of the left anterior descending artery.
Patients with perceived high procedural risk for PCI or CABG due to comorbidities or left ventricular systolic dysfunction.
Patients with complex coronary anatomy which causes technical issues for PCI or CABG.
Patients who have arterial access issues.
*There is potential overlap between categories.
Minimum dataset
History—nature of presentation, symptoms, details of any previous cardiac interventions, comorbidities including diabetes mellitus, cerebrovascular disease, peripheral arterial disease and contraindications to antiplatelet therapy.
Blood test results—estimated glomerular filtration rate, haemoglobin concentration.
Coronary angiography and results of invasive physiology/anatomy assessments, if undertaken.
Cardiac imaging results indicating left ventricular function, valve function and myocardial viability and ischaemia, as appropriate to the case.
Special patient circumstances and treatment preference.
Core attendees
MDM coordinator.
Interventional cardiologist—at least one (the norm should be two or more).
Cardiac surgical consultant—at least one (the norm should be two or more).
Additional attendees
General cardiology consultant.
Cardiology imaging consultant(s) (CT/MRI/echo).
Cardiac anaesthetist/intensivist.
Cardiology and surgical trainees.
Cardiac physiologists.
Cardiology and surgical specialist nurses.
Medical students.
Aortic valve multidisciplinary meetings
Introduction
Degenerative, calcific aortic stenosis is the most prevalent significant valve lesion in the UK. There is a long asymptomatic phase during which the adverse cardiovascular event rate is low. The disease trajectory accelerates, however, after symptoms develop. Aortic regurgitation may be well tolerated for years, but the added stroke volume it places on the left ventricle may ultimately cause it to fail. The aim of the MDM is to provide a streamlined, consistent pathway which ensures that the right patients receive the right procedure at the right time. The timing of intervention, in asymptomatic patients in particular, requires a careful assessment by the MDT of lesion severity, ventricular function and procedural risk. Both surgical aortic valve replacement (sAVR) and TAVI are effective interventions for severe aortic stenosis and selection of the optimal intervention is a key and nuanced part of decision-making.8 It is also the case that data from clinical trials may not reflect contemporary outcomes in UK practice. The pathway for all patients being referred for aortic valve intervention should therefore include review at an aortic valve MDM. Factors that need to be taken into account are the risk of sAVR and TAVI, technical suitability for each procedure, comorbidities or frailty that could delay or impair functional improvement after intervention and patient preference. This is essential to shared decision-making.
This section is complementary to the recommendations made by the British Heart Valve Society about aortic MDMs in its consensus service framework document, Networked-Based care for Heart Valve Disease.9
Proposed process
The presenting clinician should ensure that all data are available prior to MDM listing. Echocardiography and other cross-sectional imaging must be available for review by relevant specialists in the meeting.
All patients should be reviewed by the MDM. It is important, however, that proportionately more time in the MDM is allocated for the review of complex patients, without delaying those patients for whom decision-making is straightforward. In order to facilitate this, patients should be triaged ahead of the MDM according to an agreed network-wide protocol. Triaging should be performed by one or more designated senior clinicians including the MDM chair, supported by the MDM coordinator and/or a specialist nurse. Patients should be triaged into groups based on comorbidities and frailty as indicative markers for the most likely preferred intervention. An example of triage into risk categories is provided below. The triaging process must be part of the MDM record and a list of patients triaged into groups 1 and 2 along with a brief case summary should be made available at the MDM. If, following clinic review, the optimal treatment option for these patients is called into question for any reason, they should be referred back for full MDM discussion (see figure 2 for flow chart and box 2 for patient examples).

Patient flow through the aortic MDM. *CTCA or invasive, †as required. CTCA, CT coronary angiography; MDM, multidisciplinary meeting; PFT, pulmonary function testing; sAVR, surgical aortic valve replacement; TAVI, transcatheter aortic valve implantation; TOE, transoesophageal echocardiography.
Examples of possible triage to illustrate the aortic MDM pathway
Scenario 1: a man aged 68 years with severe bicuspid AS and 5 cm aortic root
Triaged to group 1. Summary to MDM, review in specialist aortic surgical clinic. Listed for sAVR and root replacement.
Scenario 2: a woman aged 88 years, CKD stage 3, suffering from diabetes
Triaged to group 2. Summary to MDM, review in TAVI clinic. Accepted for TAVI. Review in TAVI technical MDM to confirm access, valve size and choice of prosthesis.
Scenario 3: a man aged 75 years, limited mobility, Parkinson’s disease
Triaged to group 3. MDM review. Predicted slow/difficult recovery from sAVR. Review in TAVI clinic. Accepted for TAVI. Review in TAVI technical MDM to confirm access, valve size and choice of prosthesis.
Scenario 4: a man aged 78 years, severe AS, severely symptomatic, myelodysplasia, platelet count 25, transfusion dependent
Triaged to group 4. Poor non-cardiac prognosis and high procedural risk. Not appropriate for intervention. Discharged back to referring team.
Scenario 5: a man aged 82 years, severe tricuspid AS, 70% mid-LAD stenosis, otherwise fit and active
Triaged to group 3. MDM review. Good candidate for both sAVR and TAVI. Joint review by surgeon and TAVI operator. Patient opted for sAVR and CABG. Listed for sAVR and LIMA.
Scenario 6: a woman aged 78 years, severe AS
Triaged to group 1. Summary to MDM. Review in surgical clinic. Recently widowed and now sole carer for disabled daughter. Referred back to MDM. TAVI likely better option in view of recovery time. Reviewed in TAVI clinic. Accepted for TAVI. Review in TAVI technical MDM to confirm access, valve size and choice of prosthesis.
Scenario 7: a man aged 81 years, severe AS, recent reduced mobility
Triaged to group 2. Summary to MDM. Review in TAVI clinic. In clinic found to be limited solely by symptoms from severe AS, otherwise very fit and independent. Wishes to consider sAVR. Referred back to MDM. Seen in sAVR clinic. Accepted for sAVR.
Group 1: patients for whom surgery appears the best option
Patients in group 1 should, in general, be triaged towards sAVR as the preferred treatment option and seen in a surgical clinic. Patients will typically be at low risk for complications and/or prolonged recovery following sAVR. MDM recommendations can be made by protocol unless there are concerns about technical feasibility, severe individual organ dysfunction or multiple comorbidities. Examples of such concerns include the following:
Uncertain severity of aortic valve disease/indication for intervention.
Significant ascending aortic calcification/porcelain aorta.
Increased surgical risk due to comorbidities.
Increased risk of prolonged postoperative recovery due to frailty, restricted mobility or other conditions that may affect rehabilitation after the procedure.
Group 2: patients for whom TAVI appears the best option
Patients in group 2 should, in general, be triaged towards TAVI as the preferred treatment option and seen in a TAVI clinic. These patients are likely to be at high risk for complications and/or prolonged recovery time following sAVR. The MDM recommendation can be made by protocol unless there are concerns about appropriateness or feasibility of TAVI or, after clinic review, they are felt to be good, low-risk, candidates for sAVR, in which case a full MDM discussion is required. Examples of concerns about suitability for TAVI include the following:
Uncertain severity of aortic valve disease/indication for intervention.
Unsuitable for transfemoral access.
Severe, complex coronary artery disease.
Significant mitral or tricuspid valve disease.
Dilated ascending aorta.
Aortic regurgitation—all patients with severe aortic regurgitation require full discussion.
Aortic/Arterial features identified by CT scanning which confer high risk for complications with TAVI.
Where comorbidities raise doubt regarding whether or not intervention is likely to be beneficial.
Group 3: patients where both sAVR and TAVI are potential options
Patients in group 3 require a detailed review of the pros and cons of each intervention, with a full MDM discussion to determine the preferred treatment strategy. The MDM discussion should consider the surgical risk profile of the patient, as well as factors which influence recovery such as frailty, liver disease and cognitive impairment.8 Decision-making should take account of local surgical experience, outcome data from the national adult cardiac surgical audit and local TAVI experience and outcomes.10 11
When both TAVI and sAVR are technically feasible and the optimal strategy is unclear, it may be appropriate for patients to be assessed jointly in clinic by the cardiac surgery team and the TAVI team to discuss the merits of each intervention and to enable fully informed joint decision-making.
Group 4: patients where the role of intervention is uncertain
Some of the most difficult decisions concern those patients where the benefit of intervention is uncertain due either to uncertainty about the true severity of the aortic stenosis or concerns about the suitability of the patient for any form of intervention. All such patients require full MDM review.
Minimal dataset for initial triage
Current symptoms and trajectory.
Medical history and comorbidities.
Up-to-date blood test results (full blood count and renal function as a minimum).
Up-to-date echocardiogram—images and report.
Up-to-date invasive coronary angiogram or CT coronary angiogram images and report.
Frailty score or comment on frailty.
Information on prognosis from other conditions.
Additional dataset for multidisciplinary meeting review
A TAVI CT (gated cardiac study, non-gated contrast aortogram from lung apices to femoral arteries) should be available for any patient where TAVI is considered as an option.
12-lead ECG.
N-terminal pro-brain natriuretic peptide, where there are concerns about left ventricular function or symptomatic heart failure.
Lung function tests±arterial blood gases if history of lung disease.
Six-minute walk where there are concerns about functional status or frailty.
Formal assessment of cognitive function such as the Montreal Cognitive Assessment (MoCA), if there are concerns regarding cognitive function.
Patient’s and referrer’s treatment preferences.
Core attendees
MDM coordinator.
Cardiologist with expertise in echocardiography and valve disease.
Cardiologist or radiologist with expertise in cardiac structural CT.
Surgeon with expertise in aortic valve surgery±TAVI.
Interventional cardiologist with expertise in TAVI.
Additional attendees
Specialist nurses—cardiac surgical and structural.
Cardiac anaesthetist/intensivist.
Elderly care physician.
Cardiology and surgical trainees.
Cardiac physiologists.
Medical students.
Mitral and tricuspid valve multidisciplinary meetings
Introduction
Mitral and tricuspid valve disease predispose to increases in pulmonary venous pressure and systemic venous pressure, respectively. This can lead to breathlessness, fatigue and peripheral oedema. Atrial dilation and atrial arrhythmia are common consequences of mitral and tricuspid valve disease. Ensuring that patients who develop atrial fibrillation or atrial flutter are treated with oral anticoagulation is an important part of their management. Diagnosis of mitral and tricuspid valve disease is usually straightforward. Assessment of lesion severity is more difficult, while differentiating primary from secondary regurgitation, and assessment of biventricular function and pulmonary artery pressure are other important considerations in management. The GIRFT report for cardiothoracic surgery identified the need to increase the rate of mitral valve repair for patients with degenerative mitral valve disease nationally.1 It is essential that patients who require surgical intervention for mitral regurgitation have access to dedicated mitral valve surgeons who have high rates of valve repair for degenerative valve disease in order to improve patient outcomes and ensure equitable care. The emergence of percutaneous technologies for mitral and tricuspid valve pathologies has increased the treatment options for patients whose surgical risk is prohibitive.
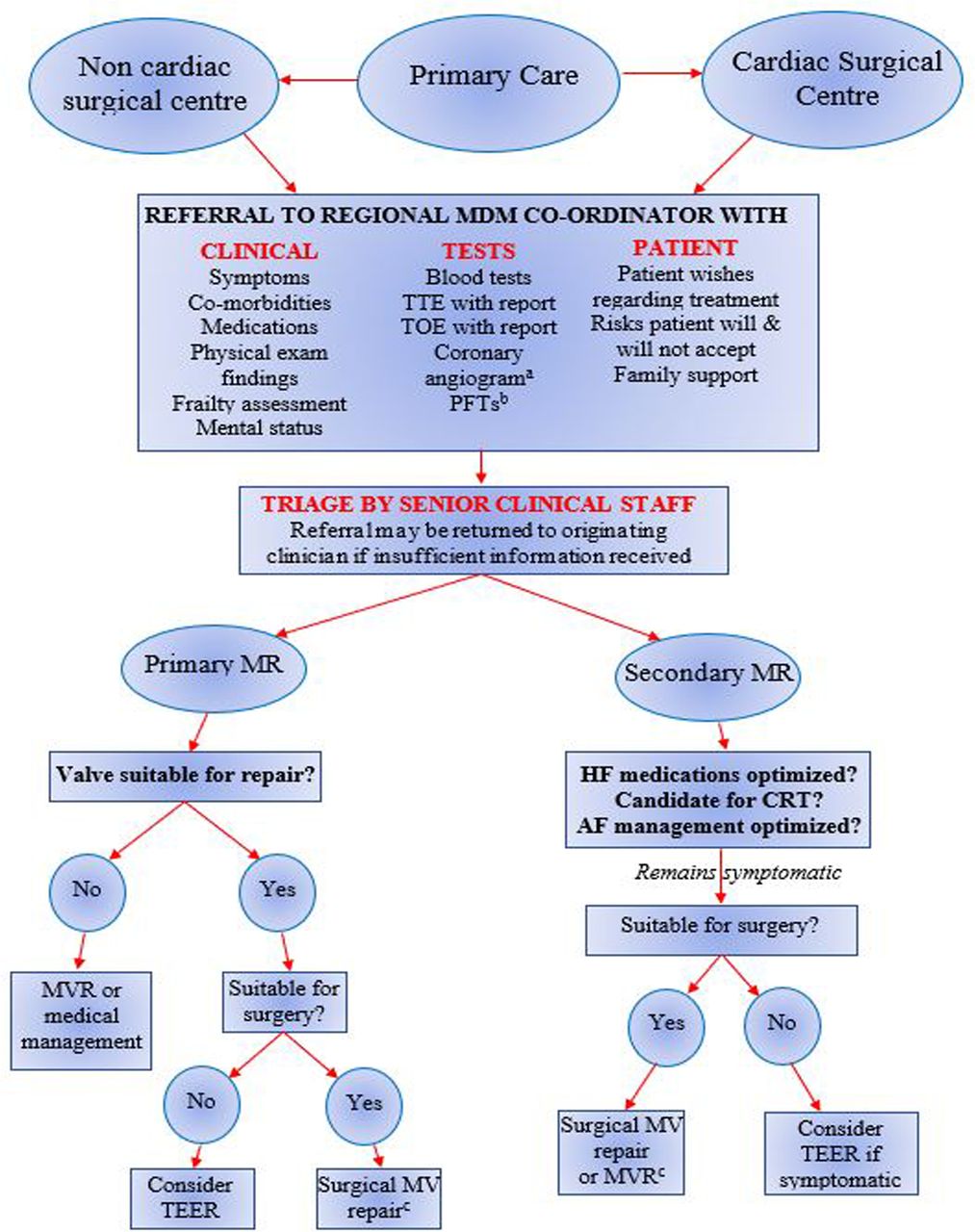
The main objective of the mitral and tricuspid valve MDM is to ensure that patients undergo a team-based evaluation, which identifies the patients who are most likely to benefit from valve intervention. The MDM should function as the single point of entry for all patients under consideration for intervention to the mitral valve and/or the tricuspid valve (figure 3). The mitral regurgitation pathway is differentiated into primary and secondary regurgitation. For patients who have secondary mitral regurgitation, the involvement of a heart failure specialist is essential, either as the referrer or as part of the MDM attendees.

{kind=link}
{kind=link}
{kind=link}
Patient flow through the mitral/tricuspid MDM. *CTCA or invasive, †as required, c+/− TV repair and AF surgery. AF, atrial fibrillation; CRT, cardiac resynchronisation therapy; MDM, multidisciplinary meeting; MR, mitral regurgitation; MVR, mitral valve replacement; PFT, pulmonary function testing; TEER, transcatheter edge-to-edge repair; TOE, transoesophageal echocardiography; TTE, transthoracic echocardiography; TV, tricuspid valve.
This section is complementary to the section on mitral and tricuspid valve MDMs in the British Heart Valve Society consensus service framework document, Networked-Based Care for Heart Valve Disease.9
Proposed process
The referring clinician should ensure that all data are available for the MDM. Echocardiography and other cross-sectional imaging such as cardiac MRI scans (if performed) should be available for review in advance of the MDM by a cardiologist with appropriate expertise, who will be present at the meeting. The valve lesion(s) and severity, intervention and surgeon or operator should be identified by the MDM. For patients with mitral regurgitation, the MDM should advise whether or not the mitral valve is amenable to repair. Patients who have degenerative mitral valve disease which is amenable to surgical repair should be operated on by a surgeon with appropriate expertise and procedural results in line with best contemporary practice in published guidelines.8 10 This may require referral to another centre. When patients are deemed potentially best managed by percutaneous valve interventions which are not available locally, they should be referred to another centre for assessment.
Recommendations about the management of concomitant atrial fibrillation, optimisation of heart failure medication and the need for cardiac resynchronisation therapy should be made where applicable.
Minimum dataset
Current symptoms and symptom trajectory.
Medical history/comorbidities.
Up-to-date transthoracic echocardiogram—images and report.
Up-to-date TOE images (needed for most elective cases).
Up-to-date invasive coronary angiogram or CT coronary angiogram—images and report.
Additional dataset
Lung function tests±arterial blood gases if history of significant lung disease.
Information on prognosis for other potentially life-limiting conditions.
MoCA or other assessment of cognitive function if history of confusion/dementia.
Comment on frailty.
Opinion from referrer and patient regarding preferred treatment.
Core attendees
MDM coordinator.
Surgeon with expertise in mitral valve/tricuspid valve repair.
Cardiologist with expertise in echocardiography and valve disease.
Additional attendees
Specialist nurses—cardiology and surgical.
Cardiologist with expertise in percutaneous treatment of mitral valve and tricuspid valve for discussion of cases where percutaneous intervention is under consideration.
Heart failure specialist (for discussion of patents with secondary mitral regurgitation).
Consultant cardiologist with expertise in cross-sectional imaging.
Cardiac anaesthetist/intensivist.
Cardiac physiologists.
Cardiology and surgical trainees.
Medical students.
Endocarditis multidisciplinary meetings
Introduction
Endocarditis is associated with a mortality of 10%–30%. Its incidence appears to be increasing. It can present challenges in both diagnosis and management. Endocarditis affecting prosthetic valves and cardiac rhythm management devices poses particular problems. The aims of the endocarditis MDM are to provide a pathway which ensures that all patients with suspected or confirmed endocarditis are discussed, treated and prioritised for surgery when necessary, with an appropriate degree of urgency by an expert team in an equitable way, irrespective of the hospital to which they were first admitted.12 Patients with endocarditis may present with haemodynamic instability and require urgent assessment by a clinical team which includes cardiologists, cardiac surgeons, infectious disease/microbiology experts and cardiac anaesthesia/intensive care specialists. The MDM pathway therefore needs to encompass mechanisms to deal with emergency out-of-hours referrals. The MDM also provides a forum for the ongoing review of inpatients, for discharge planning and for arranging long-term follow-up. This section is complementary to the recommendations regarding endocarditis which were made in the British Heart Valve Society consensus service framework document, Networked-Based Care for Heart Valve Disease.9
Proposed process
The MDM should be held at least weekly with the potential to discuss emergency cases in ad hoc MDMs between the main meetings. Referrals to the MDM should be made to the MDM coordinator and MDM chair using a standardised form. All available imaging and ancillary data should be provided at the time of referral.
Urgent advice regarding patients who are admitted as an emergency or for inpatients who deteriorate out of hours should be sought from the on-call consultant cardiologist at the network cardiac surgery centre and referred to the MDM as soon as possible for ad hoc review. All cardiac surgical centres should provide the capability for ad hoc MDMs for endocarditis on a daily basis.
The MDM chair should be the cardiology lead for the endocarditis service. There should also be a designated lead cardiac surgeon.
Minimum dataset
Nature of presentation, symptoms, medical history, details of any previous cardiac surgery, risk factors for endocarditis (eg, known valve disease, congenital heart disease, cardiac rhythm management device, intravenous drug use or previous endocarditis).
Blood test results: inflammatory markers, estimated glomerular filtration rate, albumin, full blood count and trend since admission.
Microbiology results—blood cultures, sensitivities, minimum inhibitory concentrations if available.
Antimicrobial therapy.
Echocardiographic images (transthoracic±transoesophageal).
Other imaging, for example, CT imaging for embolic events/abscess formation, brain MR for suspected cerebral embolisation.
Complications: ongoing fever, new-onset heart failure, embolisation, valve dysfunction, abscess formation.
Core attendees (for both formal and ad hoc multidisciplinary meetings)
MDM coordinator.
Consultant cardiologist with expertise in valve disease and/or echocardiography.
Consultant microbiologist and/or consultant in infectious diseases.
Consultant cardiac surgeon.
Additional attendees
Consultant in general cardiology.
Consultant cardiologist with expertise in cardiac cross-sectional imaging.
Consultant in cardiac anaesthesia/intensive care.
Pharmacist.
Cardiac physiologist.
Specialist nurse.
Trainees in cardiology/cardiac surgery/microbiology/infectious diseases.
Medical students.
Ethics statements
Patient consent for publication
Ethics approval
This study does not involve human participants.
Acknowledgments
We are grateful to members of the Cardiovascular Care Partnership UK (CCPUK) for reviewing drafts of this document to provide a patient perspective.
Footnotes
Contributors All authors contributed to the discussion, drafting, review and approval of the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests APB: unrestricted educational grant from Boston Scientific, speaker fees from Boston Scientific, Abbott Vascular, Medtronic, Miracor and Shockwave. AB: research support from Abbott Vascular, speaker fees from Microport, AstraZeneca, Sinomed, Medtronic, Terumo, Pi-cardia. GC: payment for expert testimony, Cambridgeshire Coroner, Trustee, The Aortic Dissection Charitable Trust. PMacC: speaker fees and expert testimony, Edwards Life Sciences. SR: fee for chairing advisory board and speaker fee paid to Manchester University Hospitals, Novartis; reimbursement of travel expenses as speaker (no fee), Abbott. Trustee, Heart Valve Voice.
Patient and public involvement Patients and/or the public were involved in the design, or conduct, or reporting, or dissemination plans of this research. Refer to the 'Methods' section for further details.
Provenance and peer review Commissioned; externally peer reviewed.