Article Text

Abstract
Objective This study aims to examine the incidence of pregnancy-related cardiometabolic conditions and severe cardiovascular outcomes, and their relationship in US Medicaid-funded women.
Methods Medicaid is a government-sponsored health insurance programme for low-income families in the USA. We report the incidence of pregnancy-related cardiometabolic conditions (hypertensive disorders and diabetes in, or complicated by, pregnancy) and severe cardiovascular outcomes (myocardial infarction, stroke, acute heart failure, cardiomyopathy, cardiac arrest, ventricular fibrillation, ventricular tachycardia, aortic dissection/aneurysm and peripheral vascular disease) among Medicaid-funded women with a birth (International Classification of Diseases, Tenth Revision, Clinical Modification (ICD-10-CM) diagnosis code O80 or O82) over the period January 2015–June 2019, from the states of Georgia, Ohio and Indiana. In this cross-sectional cohort, we examined the relationship between pregnancy-related cardiometabolic conditions and severe cardiovascular outcomes from pregnancy through to 60 days after birth using multivariable models.
Results Among 74 510 women, mean age 26.4 years (SD 5.5), the incidence per 1000 births of pregnancy-related cardiometabolic conditions was 224.3 (95% CI 221.3 to 227.3). The incidence per 1000 births of severe cardiovascular conditions was 10.8 (95% CI 10.1 to 11.6). Women with pregnancy-related cardiometabolic conditions were at greater risk of having a severe cardiovascular condition with an age-adjusted OR of 3.1 (95% CI 2.7 to 3.5).
Conclusion This US cohort of Medicaid-funded women have a high incidence of severe cardiovascular conditions during pregnancy. Cardiometabolic conditions of pregnancy conferred threefold higher odds of severe cardiovascular outcomes.
- Pregnancy
- Heart Failure, Systolic
- Diabetes Mellitus
- Hypertension
- Stroke
Data availability statement
Data may be obtained from a third party and are not publicly available. This is a post-hoc analysis of pre-existing de-identified administrative data, which were obtained from the third party upon request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Approximately 700 women die from pregnancy-related complications in the USA every year with cardiovascular conditions being responsible for over 33% of pregnancy-related deaths.1 Despite goals to reduce it, maternal mortality has concerningly increased by 26.6% in the USA, from 18.8 per 100 000 live births in 2000 to 23.8 per 100 000 live births in 2014.2 Pregnancy-related cardiometabolic conditions can result in more severe cardiovascular outcomes. For example, pre-eclampsia is one of the major causes of maternal and neonatal morbidity and mortality globally affecting 5% of all deliveries in the USA and worldwide.3 Globally, 1 in 2000 deliveries results in maternal death from hypertensive disorders of pregnancy4 and the risk of death among women with pre-eclampsia is close to four times higher.4 In the USA, there is an increasing number of women with chronic health conditions, such as hypertension, diabetes and chronic heart disease, going into pregnancy. Using the 1998–2006 Nationwide Inpatient Sample of the Healthcare Cost and Utilization Project data, Kuklina et al 5 reported an increase in overall prevalence of hypertensive disorders among delivery hospitalisation and an increase of hospitalisation with eclampsia/severe pre-eclampsia, and Albrecht et al 6 and Correa et al 7 published data on an increase of gestational diabetes over a similar time period.
Medicaid is a government-sponsored health insurance programme for low-income families who have no medical insurance or inadequate insurance and finances more than 4 in 10 births in the USA.8 It provides insurance coverage to pregnant women up to 60 days post-delivery. This results in a comprehensive database of conditions encountered during pregnancy and for the 60 days post-delivery through Medicaid claims. Federal law requires that all states extend eligibility for pregnant women with incomes up to 138% of the federal poverty level (FPL), however, most states go beyond this minimum threshold, ranging from 138% to 380% FPL. For Indiana, Ohio and Georgia, the eligibility is 218%, 205% and 225%, respectively. In Ohio and Indiana, 23%–25% are eligible for Medicaid and 18%–23% in Georgia.9 With cardiometabolic conditions on the rise, it is important to understand the rates within more vulnerable parts of society, including the Medicaid population. We aim to estimate the rates of clinically important pregnancy-related cardiometabolic conditions and their effect on severe cardiovascular outcomes in pregnancy, in a large cohort of Medicaid-insured women in the USA.
Methods
Study cohort
In this retrospective cross-sectional cohort study, we analysed Medicaid claims data for the states of Georgia, Indiana and Ohio. The Medicaid insurance company that provided the data for this study, US Health Management Systems, receives all the claims from the CareSource managed care company. Choice of managed care company is influenced by patient choice, and in Indiana there are four managed care companies with one being CareSource which processes 9% of the people eligible for Medicaid. Ohio has five managed care programmes with the CareSource managed care programme processing claims for 53% of people eligible for Medicaid. CareSource Georgia collects claims from 12% of the Medicaid-eligible population in Georgia. Our study used data extracted from January 2017 to June 2019 for Georgia and Indiana and from January 2015 to June 2019 for Ohio, which is when CareSource began in the respective states. These three states were selected because they had higher data coverage compared with the other states.
The Medicaid population does not necessarily translate to the general population as it represents a lower socioeconomic group as a direct reflection of who is eligible and skews towards non-white people with 65% of black women being covered by Medicaid.10 There is coverage across urban and rural parts of each state. Patients have a choice of Medicaid providers so this cohort will reflect those that chose CareSource. CareSource processes all the claims submitted by their patients from services within their network and some approved external providers.
All Medicaid-eligible pregnant women were included. The ICD-10-CM O80 or O82 diagnosis codes (full-term delivery or delivery with caesarean) were used to identify women with pregnancy that had at least one delivery during the data study period. If women had more than one delivery, then the first delivery in that study period was included and all subsequent episodes of care excluded. A pregnant woman’s pre-existing conditions collected at first prenatal visit, any additional diagnoses, medical procedures, hospitalisation throughout pregnancy, delivery, and up to 2 months post-delivery were all claimed and collected through the Medicaid data. This is a post-hoc analysis of pre-existing de-identified administrative data so there was no public or patient involvement.
Exposure definition
Pregnancy-related cardiometabolic conditions were defined by the presence of at least one ICD-10-CM diagnosis code (see online supplemental appendix) indicative of pre-existing hypertension-complicating pregnancy, gestational hypertension, mild to severe pre-eclampsia, pre-existing diabetes mellitus in pregnancy or gestational diabetes, in the time frame of first prenatal visit to 2 months post-delivery. We applied the following in our approach. The type of pregnancy-related cardiometabolic conditions was defined as the most severe outcome of pre-existing hypertension-complicating pregnancy, mild to moderate pre-eclampsia, severe pre-eclampsia/eclampsia and gestational hypertension. If the woman had pre-existing hypertension, then they could not have gestational hypertension and the diagnosis of gestational diabetes excluded patients with pre-existing diabetes. Women who had hypertension before pregnancy can be diagnosed with ‘hypertension complicated in pregnancy’.
Supplemental material
Outcome definition
Severe cardiovascular outcome that occurred from the time of the first prenatal visit to 2 months post-delivery was defined as the presence of at least one ICD-10-CM diagnosis code (see online supplemental appendix) indicative of myocardial infarction, heart failure, cardiac arrest, ventricular tachycardia and re-entry ventricular arrhythmia, ventricular fibrillation, stroke, aortic dissection or rupture, aortic aneurysm and pulmonary embolism. Death was not an outcome because this is not routinely reported through the Medicaid claims process.
Statistical analysis
The incidence of pregnancy-related cardiometabolic conditions and severe cardiovascular outcomes in women from their first prenatal visit to 2 months post-delivery were calculated as the rate per 1000 births with the associated 95% CI. The incidence was also estimated within three age groups, the youngest being under 20 years, a middle group of ages 20–34 years and the oldest being over 34 years old. These categories were used because advanced maternal age (>35 years) and teenage pregnancy (<20 years) are associated with increased risk of some complications. The ORs, with 95% CIs, of any severe cardiovascular outcome with each pregnancy-related cardiometabolic condition were estimated using logistic regression adjusting for the mother’s age at delivery and all the components of the pregnancy-related cardiometabolic conditions. In addition, the ORs, with 95% CIs, of each component of severe cardiovascular outcome with any pregnancy-related cardiometabolic condition were estimated using logistic regression adjusting for the mother’s age at delivery.
Results
There were 74 510 women with at least one delivery during the observation period, with 80.6% from Ohio, 12.1% from Georgia and 7.3% from Indiana, which reflects the coverage of Health Management Systems in these states. The mean age was 26.4 years with an SD of 5.5 years. The overall incidence of pregnancy-related cardiometabolic conditions per 1000 births was 224.3 (95% CI 221.3 to 227.3). The most common conditions were gestational diabetes with an incidence of 64.9 per 1000 births (95% CI 63.1 to 66.7), gestational hypertension at 61.0 per 1000 births (95% CI 59.3 to 62.8), followed by mild to moderate pre-eclampsia at 35.9 per 1000 births (95% CI 34.5 to 37.2) and severe pre-eclampsia at 31.7 per 1000 births (95% CI 30.4 to 33.0), with the remaining breakdown shown in table 1.
Pregnancy-related cardiometabolic conditions by age group
The incidence of severe cardiovascular outcomes per 1000 births was 10.8 (95% CI 10.1 to 11.6). The most common severe cardiovascular outcome was heart failure with 5.3 per 1000 births (95% CI 4.8 to 5.8), followed by pulmonary embolism, 3.3 per 1000 births (95% CI 2.9 to 3.8). Severe cardiovascular outcomes increased with age, as shown in table 2.
Incidence of components of severe cardiovascular outcomes by age group
For those with a pregnancy-related cardiometabolic condition during pregnancy, the incidence of severe cardiovascular outcomes was 23.2 per 1000 births (95% CI 21.0 to 25.6), compared with 7.2 per 1000 births (95% CI 6.5 to 7.9) for those with no reported pregnancy-related cardiometabolic conditions, with an OR of 2.9 (95% CI 2.5 to 3.3) and a similar OR of 3.1 (95% CI 2.7 to 3.5) after adjusting for age. When stratifying by age groups, the OR of severe cardiovascular outcomes by whether the women had a pregnancy-related cardiometabolic condition during pregnancy was 4.0 (95% CI 2.2 to 7.1) for the under 20 years age group, 3.2 (95% CI 2.8 to 3.8) for the 20–34 years age group and 2.7 (95% CI 1.9 to 3.8) for the 35 and older age group. There was no evidence of heterogeneity of these ORs across age groups (interaction p=0.45).
The final model for subsequent severe cardiovascular outcomes, adjusted for age and each component of the pregnancy-related cardiometabolic conditions, estimated that severe pre-eclampsia has the highest association with severe cardiovascular outcomes with an OR of 7.0 (95% CI 5.7 to 8.6). The odds of a severe cardiovascular outcome increased by 4% for every year of maternal age as shown in figure 1. Few women in the dataset had no claims before delivery (4%). A sensitivity analysis adjusting for number of months prior to delivery with health service claims had little effect on the results. For example, OR of severe pre-eclampsia with severe cardiovascular outcomes dropped to 6.8 (95% CI 5.5 to 8.3).

ORs from final model of subsequent severe cardiovascular (CV) outcomes, age-adjusted and adjusted for each component of the pregnancy-related cardiometabolic conditions. DM, diabetes mellitus.
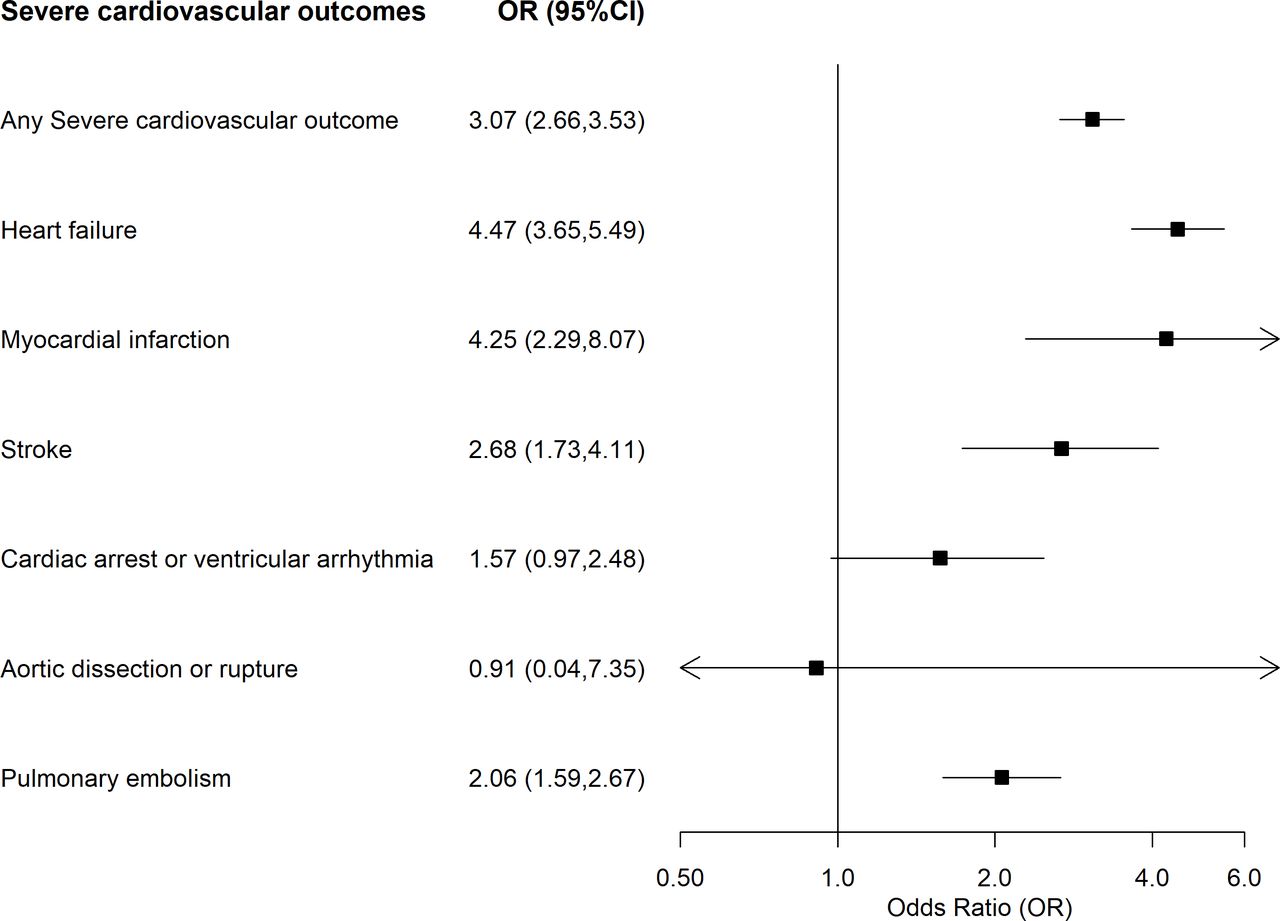
Examining overall and components of severe cardiovascular outcomes, figure 2 shows the outcomes having a higher association with pregnancy-related cardiometabolic conditions were heart failure, with an OR of 4.5 (95% CI 3.7 to 5.5) and myocardial infarction, with an OR of 4.3 (95% CI 2.3 to 8.1), both adjusted for age.

ORs of overall and components of severe cardiovascular outcomes (during pregnancy up to 60 days post-delivery) with any pregnancy-related cardiometabolic condition adjusted for age.
There were no missing data as by definition a claim was made or not. However, there were 13 women with missing age information, so all the models had a total sample size of 74 497 births. A visual graphic of the design and key findings is shown in figure 3.

{kind=link}
{kind=link}
{kind=link}
A visual display of the key findings.
Discussion
In this study of 74 510 Medicaid-funded recently pregnant women, 22% of births were associated with cardiometabolic conditions in the mother. In 1% of births, mothers had severe cardiovascular outcomes during pregnancy or up to 2 months post-delivery. Patients with any pregnancy-related cardiometabolic conditions (pre-eclampsia, gestational diabetes or hypertension or diabetes associated with pregnancy) had over threefold higher odds of severe cardiovascular outcomes, and for severe pre-eclampsia this was about sevenfold.
There is an increasing body of evidence that pregnancy-related cardiometabolic conditions including pre-eclampsia, hypertensive disorders of pregnancy and gestational diabetes portend a higher subsequent cardiovascular disease (CVD) risk for women.11 ,12 Most of these studies examine the association with long-term CVD risk in cohort studies, linkage studies and case–control studies finding that these pregnancy-related cardiometabolic abnormalities are associated with about a doubling of odds of developing CVD later in life. For example, in one systematic review and meta-analysis of CVD risk in women with pre-eclampsia, 18 studies (5 case–control and 13 cohort studies) reported CVD outcomes. Among the 14 studies included in the meta-analysis, women with pre-eclampsia had increased OR of CVD later in life of 2.28 (95% CI 1.87 to 2.77).13
There are fewer studies that examine the association of pregnancy-related cardiometabolic conditions and immediate or early cardiovascular outcomes. In one analysis of linked data for 849 639 births between 1995 and 2004 in New York City to hospital discharge diagnoses in the year after delivery, the cumulative incidence rates per 100 000 live births were 30 for heart failure, 14.8 for stroke/transient ischaemic attack (TIA) and 9.5 for coronary heart disease (CHD). Pre-eclampsia was associated with fourfold, threefold and threefold increased odds of heart failure, stroke/TIA and CHD, respectively.14 Our literature review identified only one similar study to the current study that examined the relationship of pregnancy-related cardiometabolic conditions to severe cardiovascular outcomes during the delivery hospitalisation. This retrospective cohort study was also from New York City and examined 569 900 women 15–55 years old with a singleton gestation between 2008 and 2012, finding 6.9% with a hypertensive disorder of pregnancy among whom about one-third (2.8%) had severe pre-eclampsia. Severe pre-eclampsia was associated with a 3.5-fold increase in odds of severe cardiovascular morbidity (OR 3.46, 95% CI 2.99 to 4.00), which was lower than the current study.
The rate of severe cardiovascular outcomes was high in our study. In comparison with the above New York study, it was over double the rate (3.9 per 1000 in New York study vs 10.8 per 1000 in the current study). Some of this difference may be due to differing definitions, including cardiovascular outcomes up to 2 months post-delivery and the higher overall risk of the current study’s population. Also, it is important to note that the New York study had 60% Medicaid-funded women in their cohort and excluded patients with pre-existing medical conditions including hypertension, diabetes and any CVD and hence does not represent a real-world setting. Other older US studies have reported the rate of acute myocardial infarction (AMI) in pregnancy. For example, Smilowitz et al 15 estimated the rate of AMI from the US National Inpatient Sample database from 2002 to 2014 during pregnancy and the puerperium at 8.1 (95% CI 7.5 to 8.6) per 100 000 hospitalisation admissions. Ladner et al 16 reported AMI rates of 2.8 per 100 000 births that used hospital records from 1991 to 2000 that included 98% of deliveries in California. Elgendy et al 17 estimated the rate of stroke from the National Inpatient Sample from 2007 to 2015 to be 0.4 per 1000 hospitalisation admissions. The current study also had slightly higher absolute rates of severe pre-eclampsia at 3.2%, compared with severe pre-eclampsia rates of 2.1% in the New York study above,18 and rates reported in 2014 by the Agency for Healthcare Research and Quality (AHRQ)19: 2% in the Midwest USA and 4% in the south USA. Again, the higher rates could be due to the higher risk population and differing definitions, but also may suggest increases in rates of hypertensive pregnancy disorders over time. Increasing cardiometabolic risks of childbearing women in the USA are consistent with other studies showing higher rates of hypertension and diabetes in the young general population.20 21 The current analyses suggest that such changing trends have implications both in occurrence of higher rates of pregnancy-related cardiometabolic conditions and of severe cardiovascular outcomes in the peripartum period to which they are related. Such findings should further encourage policy to focus on cardiovascular primary prevention for women of childbearing age.
The current analyses do suggest the Medicaid population is at much higher risk. AHRQ reported higher pre-eclampsia/eclampsia rates in the Medicaid population at 49.0 per 1000 deliveries vs 45.1 among those privately insured. Higher risk of gestational diabetes has been reported in older studies, such as in the Health Care Cost and Utilization project from 1993 to 2009 US national sample hospitalisation study, which found Medicaid/Medicare versus privately funded patients had higher odds of gestational diabetes (OR 1.7, 95% CI 1.6 to 2.0). This study also showed an increasing trend in gestational diabetes mellitus per 100 deliveries of 3.09–5.57 from 1993 to 2009 (trend p<0.001).
Our study has some limitations. Use of Medicaid claims data for reporting rates of health outcomes has limitations by its nature as a claims database rather than a research database. Palmsten et al 22 examined pre-eclampsia in the US Medicaid Analytic eXtract, a nationwide healthcare utilisation database, finding a positive predictive value of 67% (95% CI 54% to 77%) for pre-eclampsia when cross-checking with hospital records. This probably underestimated the validity of the data as they only used one hospital’s data records for cross-checking. There is also recent research suggesting that the ICD-10 codes for pre-eclampsia without severe features had low sensitivity.23 Other studies have demonstrated high validity of Medicaid data in research.24 In this analysis, we have no data to validate diagnoses and rely on the accuracy of the claims. Other limitations of this study include the lack of covariate data, such as ethnicity, socioeconomic factors, smoker status or body mass index and hence the inability to adjust for these potential confounders. Similarly, we have no data on pre-existing conditions so we could not adjust for this in our models, thus we are unable to rule out the possibility of bias due to reverse causality. We did, however, account for each of the pregnancy-related cardiometabolic conditions in our models of severe cardiovascular outcomes. Patients have a choice of Medicaid providers, but we have no data to compare the type of patients subscribed to each provider. US Health Management Systems does have representation geographically across the states and a patient is offered a list of doctors who offer Medicaid for inpatient and outpatient services across a range of hospitals and healthcare facilities. Eligibility of a patient to receive Medicaid may change over time so a woman’s data may be lost when their family exceeds income thresholds for Medicaid. Medicaid data for research can also lose follow-up data if patients move between states but this is less likely to be important due to the short time frame and focus on pregnancy and the puerperium. Our data are also limited to three states, which is another potential limitation.
In conclusion, the current study has found a high burden of pregnancy-related cardiometabolic conditions and severe cardiovascular outcomes in the perinatal and postnatal period in this Medicaid-funded cohort of US women, and a strong association between the two. This implies that trends towards increasing rates of cardiometabolic conditions of pregnancy, aligned with increasing age of pregnant women and worsening cardiometabolic health of younger people, could lead to more severe cardiovascular outcomes in the perinatal and postnatal period and calls for a greater focus on cardiometabolic health in women of childbearing age.
Key messages
What is already known on this subject?
There is a growing body of evidence that pregnancy-related cardiometabolic conditions including pre-eclampsia, hypertensive disorders of pregnancy and gestational diabetes portend a higher subsequent cardiovascular disease risk for women.
What might this study add?
There are fewer studies focusing on early cardiovascular outcomes during the pregnancy and the postnatal period of 60 days post-delivery. Medicaid supports low-income Americans. In this analysis of a cohort of Medicaid-insured women from Indiana, Ohio and Georgia, USA, the estimated incidence of pregnancy-related cardiometabolic conditions was 224.3 per 1000 births (95% CI 221.3 to 227.3), and the incidence of severe cardiovascular conditions was 10.8 per 1000 births (95% CI 10.1 to 11.6). Women with cardiometabolic conditions of pregnancy had threefold higher odds of having a severe cardiovascular outcome during the pregnancy and early post-delivery period.
How might this impact on clinical practice?
The analysis indicates pregnancy-related cardiometabolic conditions are common, are associated with higher risk of early and more severe cardiovascular outcomes, and highlight the need for a greater focus on cardiometabolic health in women of childbearing age.
Data availability statement
Data may be obtained from a third party and are not publicly available. This is a post-hoc analysis of pre-existing de-identified administrative data, which were obtained from the third party upon request.
Ethics statements
Patient consent for publication
Ethics approval
This analysis was submitted to the Human Research Ethics Committee of The University of Sydney that exempted this from ethics approval.
Acknowledgments
The data were provided by Health Management Systems. Dr Tim Shaw and Emma Charlston facilitated the relationship with this organisation. CKC is supported by an NHMRC investigator fellowship (GNT1195326).
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @simoneMarschne1, @clara_chow
Correction notice Figure 3 has been corrected since this article was first published. The following sentence was incorrectly written as 10% but has now been corrected to 1%: 'Between pregnancy to 60 days post delivery over 1% of women had severe cardiovascular outcome'.
Contributors Study concept and design—SM, AvH and CKC. Statistical analysis—SM and AvH. Data analysis and interpretation—SM, AvH, CKC and SZ. Drafting of the manuscript—SM. Critical revision of the manuscript and intellectual input—SM, AvH, CKC, VL, HRR, PC and SZ. Guarantor—CKC.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.