Article Text

Abstract
Objectives Cardiovascular disease is one of the leading causes of mortality and morbidity in women. Despite this, even in contemporary research, female patients are poorly represented in trials. This study aimed to explore reasons behind the sex disparity in heart failure (HF) trials.
Methods HF trials published in seven high-impact clinical journals (impact factor >20), between 2000 and 2020, were identified. Trials with over 300 participants of both sexes were included. Large HF registries, as well as population statistics, were also identified using the same criteria.
Results We identified 146 HF trials, which included 248 620 patients in total. The median proportion of female patients was 25.8%, with the lowest proportions seen in trials enrolling patients with ischaemic cardiomyopathy (17.9%), severe systolic dysfunction (left ventricular ejection fraction (LVEF) <35%) (21.4%) and those involving an invasive procedure (21.1%). The highest proportion of women was seen in trials assessing HF with preserved LVEF (51.6%), as well as trials including older participants (40.5%). Significant differences were seen between prevalence of female trial participants and population prevalence in all LVEF categories (25.8% vs 49.0%, p<0.01).
Conclusions A significant sex disparity was identified in HF trials, most visible in trials assessing patients with severely reduced LVEF and ischaemic aetiology. This is likely due to a complex interplay between enrolment bias and biological variation. Furthermore, the degree of both these aspects may vary according to trial type. Going forward, we should encourage all HF trials to appraise their recruitment log and suggest reasons for any reported sex disparity.
- GENDER
- Heart failure
- Research Design
- Coronary Artery Disease
Data availability statement
Data are available upon reasonable request. All data relevant to the study are included in the article.
This is an open access article distributed in accordance with the Creative Commons Attribution 4.0 Unported (CC BY 4.0) license, which permits others to copy, redistribute, remix, transform and build upon this work for any purpose, provided the original work is properly cited, a link to the licence is given, and indication of whether changes were made. See: https://creativecommons.org/licenses/by/4.0/.
Statistics from Altmetric.com
Introduction
Cardiovascular (CV) disease is the leading cause of mortality in women, accounting for 43%–49% of all deaths.1 Within CV disease, heart failure (HF) is the only category for which the incidence, prevalence, hospitalisation rate and mortality continues to rise, attributed to the increasing burden of CV risk factors as well as improved survival from acute myocardial infarction.1 2 However, patients enrolled in CV clinical trials have been predominantly male, which contrasts with much more balanced proportions encountered in clinical practice and population statistics.3 4 Certainly, while female representation in CV trials has more than doubled in the last 40 years, this varies significantly according to diagnosis.5 6 A review of 740 CV trials found that women accounted for only 29% in HF, which, after adjustment for population prevalence, accounted for the lowest representation compared with all other CV pathologies.5 In a systematic review of 317 trials investigating HF with reduced ejection fraction (HFrEF), 25.5% of participants were woman, with sex-related eligibility criteria, recruitment in ambulatory settings and male chief investigators all being associated with underenrolment of women.6 Furthermore, while women are now equally represented in hypertension trials, the sex distribution in HF trials has been found to be static over a 30-year period.5 7
As such, policies and programmes have been introduced in an attempt to address this, on the assumption that this reflects selection bias.8 9 Several journals have released statements prompting investigators that women should be routinely included in trials and that sex-specific analyses should be reported.10 However, this assertion has not been directly assessed before and an alternative explanation may be that sex-specific differences may lead to different HF phenotypes in men and women. The aim of our study was to explore the relative impact of these factors on differential proportions of women being enrolled in HF trials. In brief, we compared proportions of patients in clinical trials, registries and population data as an indicator of enrolment bias and compared prevalence of women by aetiology and disease characteristics as an indicator of biological variation between men and women.
Methods
HF trials published in high-impact general medical or CV journals between 2000 and 2020 were identified using the search terms ‘heart failure’ (MeSH Major Topic) AND ‘clinical trial’ (Filter). Trials were included if they met the following criteria: published in the English language, >300 participants enrolled, both sexes enrolled and sexes of participants reported. In the case of serial publications, only the headline trial paper was included, with articles reporting post hoc or subgroup analyses excluded. The prevalence of female participants, trial design, study population as well as inclusion and exclusion criteria were recorded. Indicative journals were selected by an impact factor >20 (in 2021) and included four of the most widely read general medical journals (New England Journal of Medicine, The Lancet, The British Medical Journal, Journal of the American Medical Association) and three specialist CV journals (European Heart Journal, Journal of the American College of Cardiology, Circulation).
Trials were subdivided into different clinically relevant criteria, including diagnostic investigations leading to recruitment, HF aetiology and left ventricular ejection fraction (LVEF).
HF registries were identified using a PubMed search encompassing the same terms in the above journals (online supplemental material). Population statistics were derived from publications in the same journals, which reported national healthcare datasets and primary and secondary care electronic healthcare records (online supplemental material). Ethical approval was not required as this is a retrospective analysis of published data.
Supplemental material
Statistical analysis was performed using SPSS software (V.24.0; IBM Corp). Normally distributed data are expressed as mean and compared using the Student’s t-test. Non-normal data are expressed as median (IQR) and compared using the Mann-Whitney U test. Study level prevalence data by sex was extracted from each trial; medians for each LVEF/aetiology subcategory were then calculated. All p values are two‐sided with a significance threshold of p<0.05.
Patient and public involvement
The initial motivation behind this work came from a Trial Steering Committee meeting for the ongoing trial REVIVED-BCIS2, which includes two patient representatives. It had been identified that very few female patients had been enrolled and the potential reasons behind this, as well as possible actions to address the issue, including this work, were discussed at length.
Results
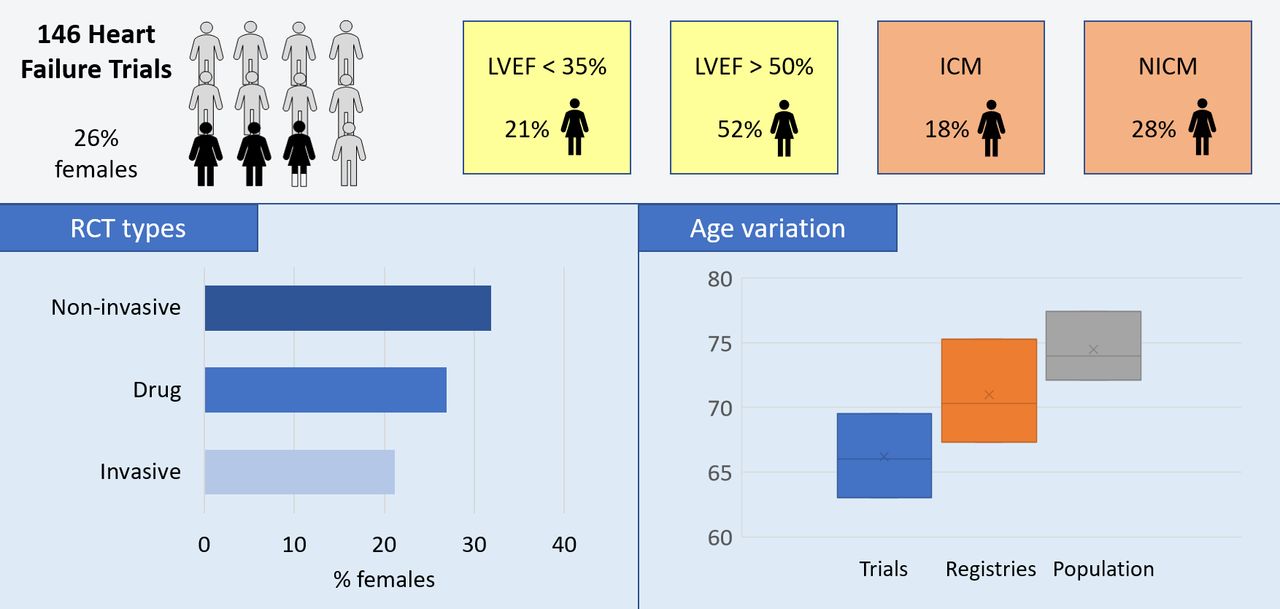
The PubMed search yielded 905 trials, which were further screened as above (figure 1) and resulted in 146 randomised controlled trials (RCTs) being included in our analysis (table 1). This encompassed 238 813 patients. The overall proportion of women in RCTs was 25.8% (21.3%–36.0%) (figure 2).
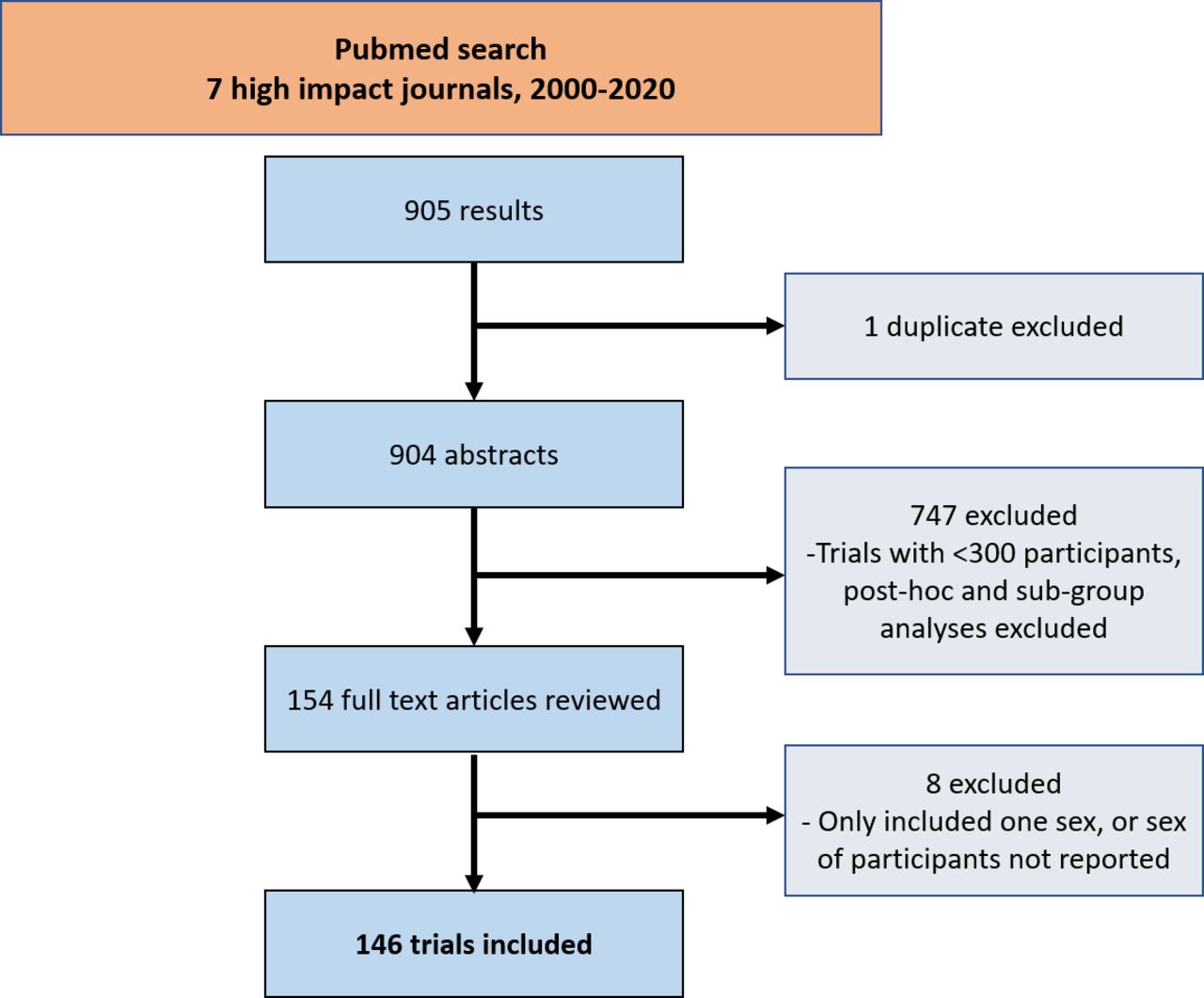
Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) diagram. Outline of inclusion and exclusion pathway.
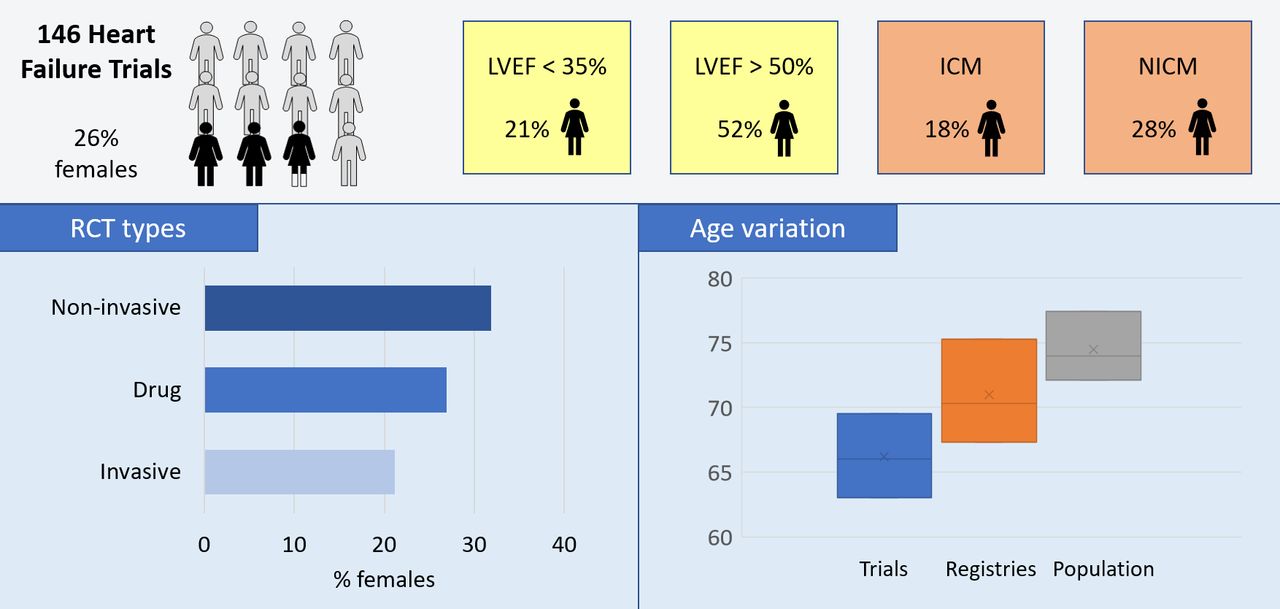
Across all trials, the median proportion of women was 26%, with the lowest proportions seen in trials assessing patients with severely impaired left ventricular function and ischaemic cardiomyopathy. ICM, ischaemic cardiomyopathy; LVEF, left ventricular ejection fraction; NICM, non-ischaemic cardiomyopathy; non-invasive, outpatient care and diagnostic trials; RCTs, randomised controlled trials.
Summary of trials, by design characteristics
Nineteen registries were identified, encompassing 583 742 patients (online supplemental table 2). The female prevalence in RCTs was markedly lower than that in registries (26% vs 40%, p<0.01) (figure 3). Significant differences were also seen between prevalence of female trial participants and population prevalence (table 2). Of the different classifications of HF, the largest difference in sex-based representation was in all-comer HF trials (RCTs vs registries 8.4%, p=0.08; RCTs vs population 13.6%, p<0.01) (table 2).

Female representation in research. Proportion of women in trials, registries and the population. HF, heart failure; LVEF, left ventricular ejection fraction.
Proportion of women in trials, registries and population statistics (median (IQR))
Trial populations had a lower median age compared with registries and population statistics (RCTs 66 years (63–69.5), registries 70.3 years (67.3–75.3), population 74 years (72.1–77.4)) (figure 2).
The lowest proportion of women was seen in trials exclusively enrolling patients with ischaemic cardiomyopathy (ICM vs NICM: 17.9% (11.7%–21.2%) vs 27.5% (25.8%–29.4%); p=<0.01, online supplemental table 4) and with severe LV systolic dysfunction (LVEF <35%) only (table 2). The highest proportion of women was seen in trials recruiting patients with HF with preserved ejection fraction (HFpEF) (figure 4), as well as trials assessing only older patients (table 1).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Sex prevalence in HF trials. Male and female prevalence in different HF trial categories; largest four trials from each subgroup shown. HF, heart failure; LVEF, left ventricular ejection fraction; trial acronyms*: I-PRESERVE, PARAGON-HF, TOPCAT, CHARM-preserved, CHARM, EPHESUS, Victoria, PARADIGM-HF, ATMOSTPHERE, OVERTURE, comet, STICH, *see online supplemental material.
Trials involving an invasive procedure or surgical treatment had the lowest prevalence of women (cumulative prevalence 21.2%, figure 2). Conversely, there was a higher proportion of women in studies investigating HF presentation including the use of risk scores (39.4%); these trials also had a higher median age (table 1).
Multiple trials reported outcomes by participant sex; two trials from either end of the female proportion spectrum are shown (online supplemental table 5). In all sex-specific analyses, women were older and had lower rates of smoking. Furthermore, some trials were identified to have an upper age limit, including GALATIC-HF, SCD-HEFT, PROTECT-2 and IABP-SHOCK-2. It was also identified that STICH and PARR-2 excluded women of childbearing age.
Among the registries that reported at least one sex-specific outcome (n=16), four did not find differences between sexes in the use of guideline-directed medical therapy, while four reported lower rates in women. Three registries specifically discussed investigations, one reporting lower use of echocardiography in women, one reporting lower use of coronary angiography and one reporting lower use of all procedure-orientated therapy (including angiography, percutaneous coronary intervention, haemodynamic support, coronary artery bypass grafting and device implantation). Female patients were less likely to receive an implantable device, even after controlling for LVEF in two registries. Three registries reported that female patients were less likely to be followed up in specialised services. Five reported sex-specific mortality outcomes; three reported no significant differences (OPTIMIZE-HF, ADHERE-HFpEF, REPORT-HF) and two reported women had a higher mortality rate (ESC-HF-LT,GARFIELD-AF).
Discussion
We have found a major disparity in sex representation in HF trials, with a median female proportion of 26% across 146 randomised control trials. The novel findings of this study are: (1) a negative correlation between the proportion of women recruited and the degree of LV systolic dysfunction, with women less frequently recruited into HFrEF than HEpEF trials and (2) variation in proportion of women enrolled by HF aetiology, being least often represented in ischaemic cardiomyopathy; (3) marked variation in the proportions of women included in trials compared with registries or population series.
Although other authors have previously reported a sex disparity in individual HF trials and meta-analyses, an appraisal of the underlying reasons behind this has been missing. Furthermore, previous reports have regarded HF trials as a single entity, but as we have shown, HF is a broad description that encompasses heterogenous conditions, each of which may be affected differentially by enrolment bias (encompassing physician-related selection bias and patient-related participation bias) and biological variation. The findings of our study show that the relative contribution of each determinant varies with the type of condition resulting in HF as well as the nature of the intervention being assessed in each trial. To this extent and the entry criteria into these trials are equally varied; therefore, there is a significant disparity in the types of patients that are recruited into these studies.
Sex disparity in ICM
Trials for patients with ICM have the highest sex disparity, with only 26% of the participants being women. Furthermore, among trial of ICM itself, those designed to evaluate an invasive treatment (such as coronary artery bypass surgery) have the lowest prevalence of women. It has been previously reported that female patients are more likely to prefer lifestyle-based interventions as opposed to procedure-based interventions,5 representing patient-related bias. Sex-based diagnostic and therapeutic biases have previously been demonstrated in clinical practice.11 We identified that even after hospitalisation, female patients are less likely to be followed up in specialised cardiac services.12 13 This may result in fewer opportunities for consideration of entering these patients into clinical trials.
While these represent enrolment bias, there is evidence to suggest that biological variation may also play a significant role in accounting for the sex disparity in ICM trials. Women have smaller epicardial coronary artery diameter, and yet, similar coronary flow reserve compared with men; this is achieved by higher baseline and hyperaemic coronary blood flow.14 This has been hypothesised to reduce lipid accumulation and delay development of coronary plaques through enhanced wall shear stress.12 Women, when presenting with an acute coronary syndrome, are less likely to have extensive coronary disease or functionally significant coronary artery stenoses15 16; therefore, making them less likely to develop ICM. Furthermore, oestradiol has been hypothesised to play a crucial role in preventing, or delaying the onset of, obstructive coronary artery disease in women. There is evidence that oestrogen increases myocyte resistance to ischaemia, with rodent studies finding superior post-ischaemic recovery of LV function and reduced infarct size in female rats, hypothesised to occur via oestrogen-mediated protein kinase C signalling.17 Indeed, in an HF registry of 9428 patients with HF, ischaemic heart disease was the aetiology in 49% of men and 28% of women18; this very closely mirrors our findings of 26% female prevalence in ICM trials. These provide a case in support for biological variation playing a significant contributory role in the sex disparity in trials investigating patients with ICM.
Sex disparity in HFrEF versus HFpEF trials
After ICM, trials recruiting only patients with HFrEF have the highest sex disparity. Studies have consistently reported that women with HF have a higher mean LVEF, which may put them beyond the threshold for trial recruitment in HFrEF trials. They may also not tolerate target HF medication doses. The PARADIGM-HF inclusion criteria included LVEF ≤35%, raised natriuretic peptide plasma concentration, a systolic blood pressure ≥95 mm Hg, estimated glomerular filtration rate ≥30 mL/min and a tolerated period of enalapril 20 mg daily (or equivalent). Norberg et al19 applied these inclusion criteria to their real-life patient cohort and found that only 16% of their female patients would have been eligible to partake in the study, largely due to female patients not meeting target medication doses. Other work has identified that lower doses of prognostic medications are required in female patients to achieve similar benefits20 21; therefore, suitable female patients may be excluded. This represents physician-related enrolment bias but also highlights the potential for oversight in trial design.
On the contrary, women are more susceptible to certain coronary vasomotor disorders due to sex-specific risk factors, such as systemic inflammation and endocrine changes. Oestradiol is generally protective against inflammation and reduced oestrogen levels post-menopause are associated with altered vascular function, heightened systemic inflammation and upregulation of the renin–angiotensin–aldosterone and sympathetic nervous systems.22 These have all been implicated in the pathogenesis of HFpEF and serve as the reasons for why women may be biologically more likely to develop HFpEF than HFrEF.23
Influence of patient and physician on likelihood of enrolment
Patient-related enrolment bias
It has been demonstrated that women perceive higher personal harm from involvement in research and have been found to be less willing to partake in trials than their male counterparts.24 This has been hypothesised to be related to cultural differences, greater childcare responsibilities and even related to the sex of researchers recruiting patients.5 25 26
Physician-related enrolment bias
RCTs included a younger population than registries, and both RCTs and registries had a lower median age when compared with population statistics. Older patients are under-represented in trials,5 with RCT patient cohorts being consistently younger compared with registry populations.27 As female patients presenting with HF are more likely to have significant comorbidities and be of older age, they are more likely to meet exclusion criteria in such trials.6 27 28 As identified here, some trials set an upper age limit or excluded women of childbearing age, both of which would disproportionally impact recruitment of female patients.6 Other work has found that higher numbers of women are excluded during trial screening.7 Van Spall et al27 reported that common medical conditions and older age were the reason for trial exclusion in 81.3% and 38.5% of trials, respectively.
Putting our findings into wider context
The sex disparity in HF trials may have implications on the management of female patients with HF. The majority of evidence-based pharmacotherapy, device and intervention strategies in HF management are currently based on populations comprised largely of male patients. Therefore, if the women are truly under-represented, then this represents a significant void that needs to be urgently addressed. However, and as is clearly evidenced by the arguments pertaining to biological variations between the sexes, we must be cautious when trying to achieve preconceived parity in sex representation in HF trials. There is certainly growing evidence that biological variation plays a significant role in the sex disparity seen in certain HF trials. It is probable that the interplay between enrolment bias and biological variation is complex and varies according to each study; for example, in trials enrolling patients with ICM, it may be that biological variation plays a more dominant role, while enrolment bias may play a dominant role in trials mandating invasive procedures before recruitment. Rather than striving to always achieve 50% female representation, researchers should make efforts to ascertain population prevalence, which in turn should influence trial design and eligibility criteria on the one hand and equitable recruitment strategies on the other hand. In this context, true equality may be best served by ensuring that every eligible patient has the same chance of being included in the appropriate trial and initiatives, such as ‘WIN-her’, by Boston Scientific may go some way to achieving this.
Limitations
The limitations of this study include that it is a retrospective analysis of published work, and therefore, reasons for individual patient exclusion cannot be explored in detail. Furthermore, we were unable to compare characteristics between men and women within trial cohorts unless this was reported by the original authors. Ideally, trial and registry recruitment would be followed prospectively and this should be an area for future work.
Conclusions
Sex disparity exists in HF trials and across all subgroups, but most visible in trials assessing patients with severely reduced LVEF and ICM. This is likely due to a complex interplay between enrolment bias and biological variation. Furthermore, the degree of enrolment bias and biological variation may vary according to the study type. Going forward, we should encourage all trials recruiting patient with HF to appraise their recruitment log and suggest reasons for any reported sex-specific disparity.
Key messages
What is already known on this subject?
Female participation in cardiovascular clinical trials has consistently been lower than that of men. Compared with all other cardiovascular pathologies, this is most marked in heart failure (HF) trials. Although this sex disparity in HF research has been previously reported, reasons for this remain unclear, and until they are identified we cannot effectively address this issue.
What might this study add?
This study identified a significant sex disparity in HF trials, with a negative correlation between the proportion of women recruited and the degree of left ventricular systolic dysfunction, with women less likely to be recruited into HF with reduced ejection fraction than HF with preserved ejection fraction trials and furthermore significant variation by HF aetiology with women less likely to be represented in ischaemic cardiomyopathy. While differential biology may account for some of the disparity, enrolment bias is also an important contributing factor, which must be addressed.
How might this impact on clinical practice?
Given the sex disparity in HF trials, it may be argued that the guideline recommendations, based on the aforementioned trials, may not necessarily be generalisable to female patients with HF. In this work, we have described a number of recommendations for future HF research. Clinicians must be aware of unconscious biases in their management and investigation of female HF patients. Trial paperwork and design should encourage and support female participation. Inclusion and exclusion criteria should be reviewed to ensure female patients are not unwittingly penalised. There must be clear documentation of those screened but excluded, with consideration of simultaneous registries.
Data availability statement
Data are available upon reasonable request. All data relevant to the study are included in the article.
Ethics statements
Patient consent for publication
Ethics approval
Not applicable.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Correction notice This article has been corrected since it was first published. The open access licence has been updated to CC BY.
Contributors HM conceived the idea, conducted the search, analysed the results and drafted the manuscript. AS conducted the search, repeated all analyses and drafted the manuscript. MM and SMH supervised the work, reviewed and edited the manuscript. DP conceived the idea, reviewed and edited the manuscript and is responsible for the overall content as the guarantor.
Funding This work was supported by the British Heart Foundation (Fellowship FS/CRTF/21/24190 to HM), the Medical Research Council (Fellowship MR/T029390/1 to AS) and the National Institute for Health Research (Biomedical Research Centre Award to Guy’s and St Thomas’ NHSFT and King’s College London).
Competing interests None declared.
Patient and public involvement Patients and/or the public were involved in the design, or conduct, or reporting, or dissemination plans of this research. Refer to the Methods section for further details.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.