Article Text

Abstract
Objective Type 2 myocardial infarction (MI) and myocardial injury are common conditions associated with an adverse prognosis. Physicians experience uncertainty how to distinguish these conditions, as well as how to manage and treat them. Therefore, the objective of this study was to compare treatment and prognosis in patients with an adjudicated diagnosis of type 2 MI and myocardial injury, who were discharged with and without a clinical diagnosis of MI.
Design The study consisted of two cohorts, 964 and 281 consecutive patients with elevated cardiac troponin, discharged with and without a clinical diagnosis of MI, respectively. All cases were adjudicated into MI type 1–5 or myocardial injury and followed regarding all-cause death.
Results The adjudication identified 138 and 37 cases of type 2 MI, and 86 and 185 of myocardial injury, with and without a clinical MI diagnosis, respectively. In patients with type 2 MI, a clinical MI diagnosis was associated with more coronary angiography investigations (39.1% vs 5.4%, p<0.001) and an increased use of secondary prevention medications (all p<0.001). However, no difference was observed in adjusted 5-year mortality between patients with and without a clinical MI diagnosis (HR: 0.77 with 95% CI 0.43 to 1.38). The results were similar for adjudicated myocardial injury.
Conclusion In both type 2 MI and myocardial injury, a clinical diagnosis of MI at discharge was associated with more investigations and treatments. However, no prognostic effect of receiving a clinical MI diagnosis was observed.
- myocardial infarction
Data availability statement
Data are available upon reasonable request. Due to Swedish laws on personal integrity and health data, as well as the Ethics Committee, we are not allowed to make any data including health variables open to the public even if made anonymous. The data could be shared with other researchers after a request to the head of our department (es.uu.icsdem@grebdnil.ave).
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Type 2 myocardial infarction (MI) and myocardial injury are heterogeneous conditions that are difficult to distinguish in clinical practice. The therapeutic and prognostic effects of assessing either of these serious conditions as MI or not are unknown.
WHAT THIS STUDY ADDS
Receiving a clinical diagnosis of MI was associated with more cardiology care including an increased use of coronary assessments and secondary preventive therapies both in patients adjudicated as having type 2 MI and myocardial injury, respectively. However, no long-term prognostic effect of receiving a clinical diagnosis of MI was observed for either of these conditions.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
The use of the term MI among patients currently defined as type 2 MI and myocardial injury, as well as the current distinction between these conditions, may not be clinically relevant. Further studies are needed to identify patients for whom specific and prognostically relevant recommendations could be applied.
Introduction
Measurement of cardiac troponin (cTn) levels in blood is recommended in patients presenting with a suspected acute coronary syndrome and levels above the 99th percentile with a significant rising and/or falling pattern is an obligatory criterion for a diagnosis of myocardial infarction (MI).1 However, elevated levels of cTn are a common finding also in the absence of the coronary atherothrombotic event that currently defines type 1 MI. Among patients with elevated cTn at emergency departments, 19%–35% have been reported to have type 2 MI and 35%–56% to have non-ischaemic myocardial injury (later referred to as myocardial injury).2–4 These are two different conditions according to the current classification of MI, where type 2 MI is caused by ischaemia due to myocardial oxygen supply/demand mismatch, while myocardial injury is thought to be caused by non-ischaemic mechanisms and therefore not classified as MI.1 However, type 2 MI and myocardial injury are resembling each other in many aspects. They are both provoked by or associated with other underlying disease, often occur in older, multi-morbid individuals and are both associated with a poor short-term and long-term prognosis.5 Due to the difficulty to distinguish type 2 MI from myocardial injury, misclassification is common and there is a large variation in the use of an MI diagnosis in both these conditions in clinical practice.6 7 However, the effects on therapeutic strategies and prognosis of receiving a clinical diagnosis of MI in these conditions are unknown. In the light of this, the aims of this study were (1) to describe patients with elevated cTn that were not clinically diagnosed as having MI, and (2) to compare treatment strategies and prognosis among patients with an adjudicated diagnosis of type 2 MI and myocardial injury with and without a clinical diagnosis of MI at discharge.
Methods
Clinical diagnosis of MI
During the study period, clinicians recorded diagnoses according to the 10th revision of International Statistical Classification of Diseases and Related Health Problems (ICD-10). The ICD-10 code I.21 was used to identify patients with a clinical diagnosis of MI regardless of ST-elevation myocardial infarction or non-ST elevation myocardial infarction. ICD-10 does not include specific codes for MI subtypes.
Study population
Two patient cohorts were used in this observational study, one which included patients with elevated cTn but without a clinical MI diagnosis (no ICD-10 code: I.21) and one which included patients with a clinical MI diagnosis (with ICD-10 code: I.21).
All 17 122 patients with a cTn measurement at Uppsala University Hospital in 2011 were identified using the local laboratory records. After exclusion of patients without elevated cTn values and patients with a clinical MI diagnosis, 3218 with at least one cTn measurement above the 99th percentile upper reference limit remained. From these, the first 300 patients with at least one additional cTn measurement within 24 hours were selected for inclusion.
The second cohort consisted of 964 consecutive patients with a clinical MI diagnosis at discharge from eight Swedish hospitals of different size and geographical location in 2011 (figure 1 and online supplemental figure S1).
Supplemental material

Patient selection and diagnosis adjudication for(A) patients with elevated troponins without a clinical MI diagnosis and for (B) patients with a clinical MI diagnosis. cTn, cardiac troponin; MI, myocardial infarction; URL, upper reference limit.
Data collection
Data were collected from the local electronic patient records in a similar way for the two patient cohorts, using a pre-specified case report form (including dates, demographical information, clinical parameters, laboratory results, results from invasive and non-invasive investigations and treatment). Copies of ECGs and relevant medical notes were also collected from the electronic patient records.
Date of death was provided by the Swedish Tax Agency.
Diagnosis adjudication
Based on the collected information, all patients in both cohorts were adjudicated and classified into MI subtypes 1–5 or myocardial injury by two independent reviewers (online supplemental table S1 and S2). In case of disagreement, a third independent reviewer decided the final diagnosis. The classification was done using a pre-specified form based on the Third Universal Definition of MI and the reviewers were physicians (cardiologists or cardiology residents) or physicians in training, specially trained in the MI classification presented in the Third Universal Definition of MI (online supplemental file—definition of MI and myocardial injury subtypes).8 In addition to the diagnosis adjudication, reviewers also assessed the underlying condition triggering the ischaemic (in case of type 2 MI) or non-ischaemic myocardial injury.
Supplemental material
Supplemental material
Troponin assay
Several different cTn assays, conventional and high-sensitive, were used in the participating hospitals. Therefore, all cTn values presented on a group level were standardised by division with the 99th percentile upper reference limit of the assay used.8
Uppsala University Hospital mainly used Abbott Architect STAT troponin I during the study period.
Outcomes and follow-up
The analysed outcome was all-cause mortality. Follow-up started from hospital arrival and continued until the 1 February 2017.
Statistics
For all statistical analyses, a p value <0.05 was considered to indicate statistical significance. Groups were compared using Mann-Whitney U test for non-normally distributed continuous variables, Student’s t-test for normally distributed continuous variables and Pearson’s χ2 test for categorical variables. Related samples were compared with McNemar’s test.
Agreement between the reviewers in the MI classification was analysed with Cohen’s kappa.
To compare time to all-cause mortality in patients with and without a clinical MI diagnosis at 1 year and 5 years of follow-up, Kaplan-Meier survival estimates and multivariable Cox regression models were created. The proportional hazards assumption was tested by analysing the correlation between Schoenfeld residuals and survival time and was met in survival analyses starting at 30 days after hospital admission.9 In addition to crude analysis, the following models were used:
Model 1: Adjustment for age, sex, active smoking and modified Charlson comorbidity index (1 p for MI, congestive heart failure, peripheral vascular disease, dementia, cerebrovascular disease, chronic lung disease and history of bleeding; 1.5 p for diabetes mellitus; 2 p for kidney disease and liver disease; 6 p for metastatic tumour).
Model 2: As per model 1 plus heart rate at admission, systolic blood pressure at admission, reaction level scale (RLS) >1 at admission (yes or no), creatinine level at admission, maximal troponin level, maximal C reactive protein (CRP) level and invasive or non-invasive ventilation during hospital stay (yes or no).
In addition, frailty models with random effect were used to account for the clustering by hospital.10
Multiple imputation of missing values of current smoking, heart rate, blood pressure, RLS level, troponin level (one patient with type 2 MI and two with myocardial injury) CRP level and creatinine level was performed (using the SAS function PROC MI and arbitrary missing pattern) with all variables in the covariate section used to produce the values for imputation. Fifty imputed datasets were used to ensure that the effect estimates were not overly inaccurate due to Monte Carlo variability. The results for each imputation were combined (using SAS function PROC MIANALYZE). In total, the proportion of missing data was 17.0% and 16.4% for current smoking and 12.8% and 0.4% for RLS level among patients with and without a clinical MI diagnosis, respectively. For the other covariates, less than 5% of the data were missing in both groups.
Patient and public involvement
Patients or the public were not involved in the design, conduct, reporting or dissemination plans of this study.
Results
Description of patients without a clinical MI diagnosis
During the data collection process, 19 patients were excluded due to receiving an ICD-10 code I.21 after transfer to a new department or due to insufficient data. Consequently, 281 patients with elevated cTn between 1 January and 5 February 2011 but without a clinical MI diagnosis was included in further analyses (figure 1).
Clinical features among the 281 patients with elevated cTn but without a clinical MI diagnosis are presented in table 1 as well as in online supplemental table S3 and online supplemental figure S2. In 49 cases, the main reason for hospital admission was elective or subacute cardiac surgery. These patients are described in detail in online supplemental tables S4 and S5 and since they had a very distinctive clinical and prognostic profile, they were not included in the comparative analyses below.
Supplemental material
Characteristics of patients with elevated cardiac troponins
Adjudicated diagnoses
Among the 281 patients with elevated cTn but without a clinical MI diagnosis, 47 (16.7%) met the MI criteria with 9 (3.2%) adjudicated as type 1 MI, 37 (13.2%) as type 2 MI and 1 (0.4%) as type 4a MI. The remaining 234 patients (83.3%), including all patients admitted for cardiac surgery, were adjudicated as myocardial injury (figure 1).
Among the 964 patients with a clinical MI diagnosis, 878 (91.1%) met the MI criteria with 722 (74.9%) adjudicated as type 1 MI, 138 (14.3%) as type 2 MI and 18 (1.9%) as type 3 or 4 MI. In 86 (8.9%) patients, the MI diagnosis was considered as incorrect, and hence adjudicated as having myocardial injury.
Comparison of adjudicated type 2 MI and myocardial injury patients with and without a clinical MI diagnosis
Comparisons of clinical characteristics between patients with and without a clinical MI diagnosis, among adjudicated type 2 MI and myocardial injury respectively, are presented in table 2. In adjudicated type 2 MI with a clinical MI diagnosis, a majority had been treated at a cardiology department (68.1%). On the contrary, treatment at a cardiology department was rare among those without a clinical MI diagnosis (10.8%, p<0.01 for treatment at a cardiology department vs any other department) (online supplemental figure S3). In adjudicated myocardial injury, care was given at a cardiology department in 48.8% and 13.5% of those with and without a clinical MI diagnosis, respectively (p<0.01) (online supplemental figure S4).
Supplemental material
Supplemental material
Characteristics and in-hospital treatment
Triggering mechanisms
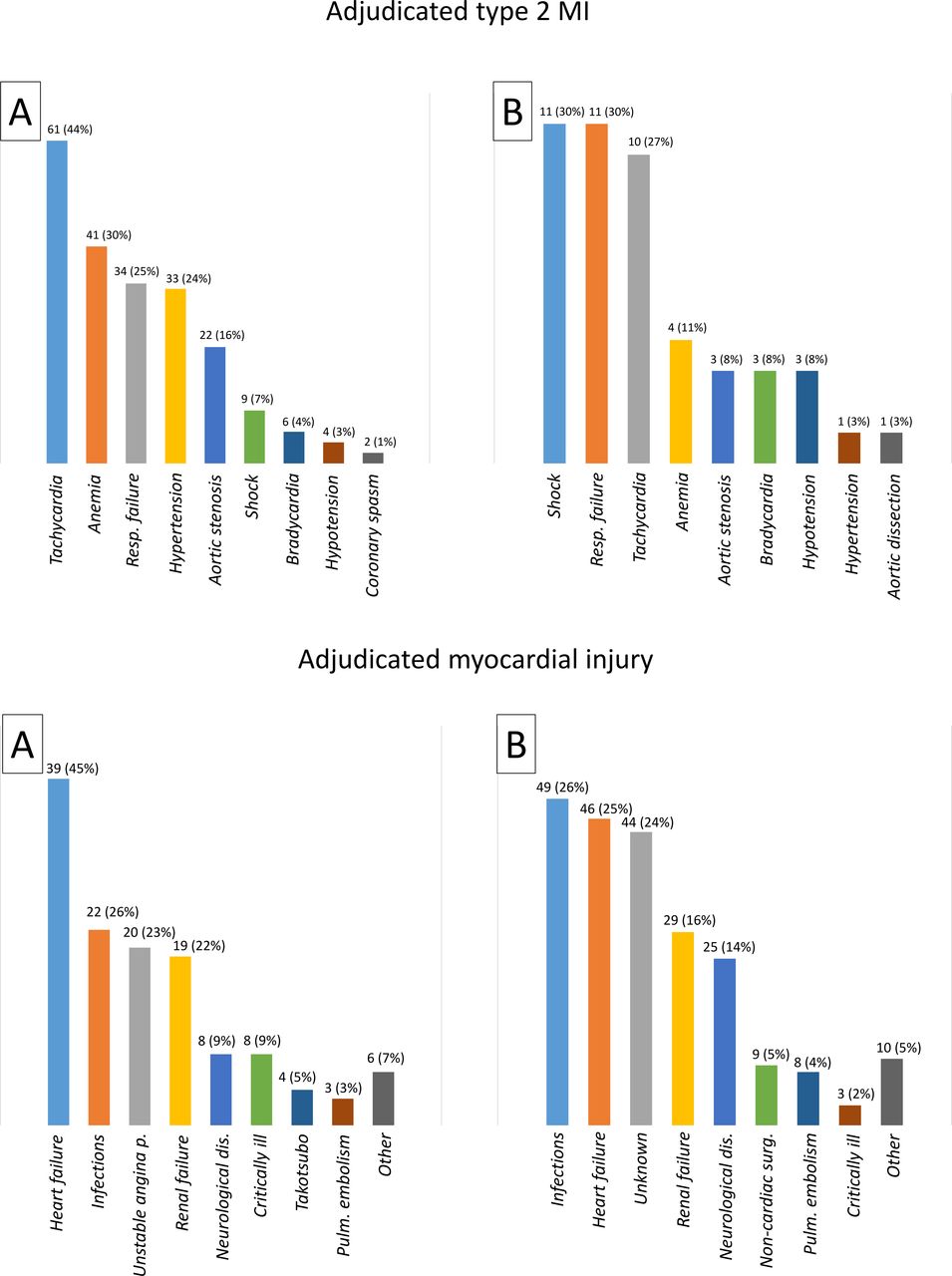
In adjudicated type 2 MI, tachycardia, anaemia and respiratory failure were common triggering mechanisms regardless of the clinical diagnosis (figure 2). However, shock was less often the triggering cause among patients with a clinical MI diagnosis when compared with patients without a clinical MI diagnosis (7% vs 30%, p<0.01). In adjudicated myocardial injury, heart failure and infections were the most common underlying conditions contributing to the myocardial injury in both groups.

Adjudicated triggering mechanisms of type 2 MI and conditions contributing to a myocardial injury among (A) patients with a clinical MI diagnosis and among (B) patients without a clinical MI diagnosis. Several were possible in each case. In patients with a clinical MI diagnosis, ‘Other’ include rhabdomyolysis, non-cardiac surgery, dehydration or other unknown causes. In patients without a clinical MI diagnosis, ‘Other’ include cardiac ablation, unstable angina pectoris, pancreatitis, rhabdomyolysis, ileus and hypertrophic cardiomyopathy. MI, myocardial infarction.
Investigations and treatment
Regardless of the adjudicated diagnosis, the frequency of coronary angiography investigations as well as treatment with Fondaparinux were higher in patients with a clinical MI diagnosis (table 2). As regards both adjudicated type 2 MI and myocardial injury patients, a clinical MI diagnosis was associated with an increased use of Aspirin, P2Y12 inhibitors, statins, renin-angiotensin-aldosterone system blockers and beta-blockers. On the contrary, the use of secondary preventive pharmacological treatments remained essentially unchanged in patients without a clinical MI diagnosis (figure 3). In adjudicated cases of myocardial injury, this difference in treatment was most prominent among cases with a <20% rise or fall in troponin levels (online supplemental table S6).

Pharmacological treatment at admission (red) and at discharge (blue) among patients alive at discharge. MI, myocardial infarction; M. injury, myocardial injury. *p<0.05; **p<0.01; ***p<0.001.
Survival
The mean follow-up was 6.0 years. Information on date of death could not be retrieved from the Swedish Tax Agency in seven patients with a clinical MI diagnosis (four adjudicated type 2 MI and three adjudicated myocardial injury). In adjudicated type 2 MI, 95 (68.8%) patients with and 29 (78.4%) without a clinical MI diagnosis died during follow-up. In adjudicated myocardial injury, the corresponding numbers of deceased patients were 54 (62.8%) and 123 (66.5%).
As presented in figure 4, a high rate of early deaths was observed among adjudicated type 2 MI patients without a clinical MI diagnosis and among adjudicated myocardial injury patients with a clinical MI diagnosis. However, regardless of the adjudicated diagnosis, no clear difference in survival could be observed between patients with and without a clinical MI diagnosis after the first 30 days of follow-up.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Crude zero days to 30 days and 30 days to 5 years survival curves for adjudicated type 2 MI and myocardial injury patients with and without a clinical myocardial infarction diagnosis (ICD-10 code I.21). MI, myocardial infarction.
As regards both adjudicated type 2 MI and adjudicated myocardial injury, no significant difference in all-cause mortality was observed between patients with and without a clinical MI diagnosis between 30 days and 1 year or 5 years of follow-up, neither in crude nor in adjusted models (table 3). Online supplemental table S7 presents the proportion of patients discharged with each secondary preventive treatment among patients alive and diseased after 5 years of follow-up.
All-cause mortality with time zero at 30 days after hospital admission
With follow-up starting at hospital admission, no significant difference in all-cause mortality was observed between patients with and without a clinical MI diagnosis, regardless of an adjudicated type 2 MI (fully adjusted 5-year HR: 0.70 with 95% CI 0.42 to 1.17) or myocardial injury (fully adjusted 5-year HR: 1.38 with 95% CI 0.56 to 3.39) diagnosis (online supplemental figure S5 and table S8).
Supplemental material
After merging adjudicated type 2 MI and myocardial injury patients into one group, no significant difference in all-cause mortality was observed between patients with and without a clinical MI diagnosis, neither with follow-up starting at 30 days after hospital admission (fully adjusted 5-year HR: 0.97 with 95% CI 0.54 to 1.75) nor with follow-up starting at hospital admission (fully adjusted 5-year HR: 1.03 with 95% CI 0.59 to 1.80) (online supplemental table S9).
Discussion
In this study, comparing consecutive patients with cTn elevation, discharged with and without a clinical MI diagnosis, type 2 MI was observed to be a commonly unrecognised condition. A clinical MI diagnosis was associated with more cardiac care, including more coronary investigations and an increased use of secondary preventive treatment in both adjudicated type 2 MI and myocardial injury patients. However, no difference in long-term prognosis between patients with and without a clinical MI diagnosis could be observed in either of these conditions.
A clear majority (82.3%) of the patients with elevated cTn at Uppsala University Hospital in 2011 did not receive a clinical MI diagnosis. After adjudication, this was judged to be incorrect in 16.7% of the cases with predominantly missed cases of type 2 MI, which suggests that a high number of patients with type 2 MI are not being diagnosed and treated as MI in clinical routine.
It has previously been reported that approximately half of the patients with type 2 MI are found outside cardiology departments.11 In the present study, receiving care at cardiology departments was rare among both type 2 MI and myocardial injury patients, who were not diagnosed clinically with MI. Treatment of MI outside cardiology departments has been reported to be associated with an adverse prognosis.12
Elevated cTn in patients without a type 1 MI has been observed to increase cardiology care and coronary angiography investigations, without altering the use of MI therapies or the prognosis.13 A clinical MI diagnosis was associated with an increased use of MI-specific therapies in the present study. Still, no significant difference in 5-year all-cause mortality could be observed, neither in type 2 MI nor in myocardial injury. This questions the clinical relevance of an MI diagnosis in either of these conditions. Further, the clinical importance of distinguishing type 2 MI from myocardial injury is yet to be demonstrated. Given the ischaemic aetiology of a type 2 MI, it is theoretically appealing to expect a high proportion of patients with underlying CAD which would benefit from pharmacological and possibly also invasive MI treatment. In a recently published study, the prevalence of non-obstructive and obstructive CAD was 38% and 30%, respectively, among patients with type 2 MI.14 Further, it has been observed that CAD is an important risk factor for future cardiovascular events in type 2 MI.15 16 These findings suggest that there is an important subgroup of patients with type 2 MI with CAD in which the MI diagnosis would be clinically relevant. Therefore, it is important to note that the present study only attempts to evaluate the use of an MI diagnosis and associated treatment in the whole population of what is currently defined as patients with type 2 MI. Unfortunately, corresponding studies of CAD and its importance in myocardial injury are lacking.
Limitations
During the study period, the laboratory in Uppsala recommended a decision limit for MI (0.3 µg/L) with Abbott Architect troponin I, which was higher than the 99th percentile (0.022 µg/L) (personal communication). This may have contributed to the large number of clinically unrecognised type 2 MI cases. Another possible cause is that adjudicators classified patients according to the 2012 universal definition of myocardial infarction which was released after the study period.17 However, the reported prevalence of type 2 MI in the national SWEDEHEART registry has been stable since the study period, arguing against any significant changes in the tendency to diagnose type 2 MI.18 19
It is important to note that, among patients with a clinical MI diagnosis, the clinical assessment of MI type may have been different from the adjudicated MI type. Hence, some patients adjudicated as either type 2 MI or myocardial injury may have been assessed as type 1 MI by the attending physician. This could for example explain the increased use of Fondaparinux and P2Y12 inhibitors for which the rationale is doubtful in MI in the absence of an atherothrombotic event. Consequently, some patients may have received MI treatment that would be considered, by most, to be unreasonably aggressive in these conditions. Further, it may be suspected that patients with a clinical profile indicative of an underlying coronary artery disease were more likely to receive a clinical MI diagnosis and that these patients therefore had a higher rate of cardiovascular death compared with patients not receiving a clinical MI diagnosis. Unfortunately, however, this study lacks data on causes of death.
There was a relatively small number of patients in the assigned groups, especially among type 2 MI without a clinical MI diagnosis. This gives an increased risk of type 2 errors. However, when merging type 2 MI and myocardial injury patients into one group as a sub analysis, still, the results were essentially neutral, suggesting that a possible effect of a clinical MI diagnosis on survival would be small.
Potential residual confounding in the survival analyses most probably include unrecognised factors, for example, frailty, negatively associated with both a clinical MI diagnosis and survival. In accordance with prior studies, tachycardia and respiratory failure were common adjudicated triggering mechanisms of a type 2 MI3 4 11 regardless of the clinical diagnosis. However, the much higher prevalence of shock as an underlying trigger among adjudicated type 2 MI patients without a clinical MI diagnosis may be important since shock has been reported as the only triggering mechanism independently predicting all-cause mortality.20 The multivariable survival analyses in the present study included systolic blood pressure as an attempt to adjust for this difference.
Finally, a minor selection bias may be present since a higher proportion of patients without a clinical MI diagnosis declined participation and since only patients alive were asked for informed consent (in accordance with the decision from the ethical committee). The best approximation of the magnitude of this bias is that the informed consent inquiry may have led to a 1 and 2.3 percentage points higher mortality among patients with and without a clinical MI diagnosis at 2 and 4.6 years of follow-up, respectively. Hence, the observed HRs in the present study may be slightly underestimated.
Conclusion
This study demonstrates that the currently defined type 2 MI often is not recognised as MI in clinical practice. In both adjudicated type 2 MI and myocardial injury, a clinical diagnosis of MI at discharge was associated with increased cardiology care, including a greater use of coronary angiography and secondary preventive therapies. However, no prognostic effect of receiving a clinical diagnosis of MI could be observed for either of these conditions. This questions the clinical relevance of the term MI outside type 1 MI and highlights the need for further studies in both these heterogeneous conditions.
Data availability statement
Data are available upon reasonable request. Due to Swedish laws on personal integrity and health data, as well as the Ethics Committee, we are not allowed to make any data including health variables open to the public even if made anonymous. The data could be shared with other researchers after a request to the head of our department (es.uu.icsdem@grebdnil.ave).
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by the Regional Ethical Review Board Uppsala, reference number 2012/208. Participants gave informed consent to participate in the study before taking part.
Acknowledgments
This paper is based on a thesis.21 A special thanks to Gorav Batra, MD, PhD; Marcus Hjort, MD, PhD; and Karolina Szummer, MD, PhD, for participation in the diagnosis adjudication process. A special thanks also to Nermin Hadziosmanovic, MSc, who performed multiple imputation for missing data. Further, a special thanks also to everyone who has contributed by collecting data at Mälarsjukhuset Hospital in Eskilstuna, Falun Central Hospital, Gävle County Hospital, Ryhov County Hospital in Jönköping, Karlstad Central Hospital, Danderyd University Hospital Corp, Örebro University Hospital and Uppsala University Hospital.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors AG, BL and TB has contributed to the planning, conduct and reporting of the study. BL also contributed as the guarantor of the study.
Funding This study was supported by grant from the Swedish Foundation for Strategic Research (grant number KF10-0024). The Swedish Foundation for Strategic Research had no role in the design of the study; collection, management, analysis and interpretation of the data; preparation, review or decision to submit the manuscript for publication.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.